
Abstract
It is unknown how endothelial-dependent flow-mediated dilation (FMD) stimulated by a sustained, exercise-induced increase in shear stress (EX-FMD) is affected by a simultaneous sympathoexcitatory painful stimulus. The purpose of this study was to examine the impact of a cold pressor test (CPT) on brachial artery EX-FMD elicited by a handgrip exercise-induced increase in shear stress. Participants were healthy males (age 21±2 years) (n=28; 16 Experimental group, 12 Control). Brachial artery diameter and blood velocity were measured using echo and Doppler ultrasound, respectively. Shear stress was estimated by shear rate (shear rate = blood velocity / diameter) and targeted to reach 75 s–1 in each of two EX-FMD trials in all subjects. In the Experimental group, the second EX-FMD trial was accompanied by simultaneous foot immersion in ice water (simultaneous CPT). The shear rate stimulus did not differ between groups (p=0.823) or trials (p=0.726) (group × trial interaction: p=0.646) (average exercise shear rate (mean ± SD): 67.6±6.2 s–1). The CPT (experienced during EX-FMD trial 2 in the Experimental group) increased mean arterial pressure (p<0.001) and heart rate (p=0.002) relative to the Control group. %EX-FMD was not different between groups (p=0.508) or trials (p=0.592) (group × trial interaction: p=0.879) (EX-FMD: Experimental group trial 1: 5.4±3.4%, trial 2: 5.6±2.6%; Control group trial 1: 6.0±3.7%, trial 2: 6.4±2.2%). In conclusion, the CPT did not impact concurrent EX-FMD, and this indicates that an acute painful stimulus does not interfere with conduit artery FMD responses during exercise in young healthy men.
Keywords
Introduction
The proper function of the endothelial cells lining the arteries is critical for maintaining vascular health. 1 In addition to exerting an antiatherogenic, vasoprotective influence, healthy endothelial cells secrete vasodilators and influence perfusion.2,3 A key stimulus for endothelial vasodilator release is blood flow-associated shear stress. Indeed, endothelial function is typically assessed in humans by quantifying the magnitude of dilation in response to an experimenter-imposed increase in shear stress (flow-mediated vasodilation, FMD). The standard non-invasive FMD assessment protocol creates a transient shear stress stimulus via the release of temporary limb occlusion (reactive hyperemia, RH).4,5 Acute stimuli (e.g. a single meal or stressful event) can transiently impair RH-FMD in healthy individuals6,7 and this may have important implications if it occurs frequently and endothelially mediated vasoprotection is similarly attenuated.
The nature of the shear stress stimulus profile is a key determinant of the FMD response characteristics.8,9 FMD stimulated by RH versus more prolonged increases in shear stress may be mechanistically distinct. In contrast with the brief RH stimulus profile, exercise induces a sustained, intensity-dependent increase in conduit artery shear stress.10–12 Importantly, FMD in daily living occurs during exercise (EX-FMD) and may play an important role in muscle perfusion (i.e. perfusion may be compromised if EX-FMD is impaired).2,13,14 Existing evidence indicates that RH-FMD and EX-FMD may have differing vulnerabilities to impairment,15–18 although similar vulnerability has also been found.19,20 As a whole, findings suggest that the impact of a stimulus or condition on RH-FMD cannot be generalized to EX-FMD. Although connections between EX-FMD and future cardiovascular disease have not been established, due to its physiological relevance and potential functional involvement in perfusion during exercise, it is important that the factors influencing EX-FMD are fully understood.
Understanding the interaction of multiple vasoactive stimuli is key to understanding in vivo vascular function. Submersion of a limb in an ice-water slurry (cold pressor test, CPT) acutely increases sympathetic nervous activity, is perceived as painful and results in a robust increase in mean arterial pressure.21,22 Superimposition of a CPT with RH has consistently been shown to impair brachial artery RH-FMD;23,24 however, the impact of a CPT on FMD performed in conjunction with a sustained increase in shear stress is unknown. The purpose of this study was to determine whether brachial artery EX-FMD is impaired when a CPT is performed during the period of exercise-induced shear stress elevation. We hypothesized that the CPT would result in an attenuated EX-FMD response.
Methods
Participants
Twenty-eight young, healthy, male non-smokers from the Queen’s University (Kingston, Ontario) community participated in the study. Subject characteristics are summarized in Table 1. Sixteen participants were recruited for the Experimental group and 12 participants were recruited for the Control group. The study protocol was approved by the Health Sciences Research Ethics Board at Queen’s University and all subjects signed a consent form approved by the same board. A medical screening questionnaire was used to exclude subjects with known symptoms of or a diagnosis of cardiovascular disease. All subjects fasted for 4 hours and abstained from caffeine, alcohol and exercise for 12 hours prior to the study. Following a familiarization visit, during which informed consent was provided, subjects visited the laboratory on one occasion in the afternoon for participation in the experiment. All experiments were performed in a quiet and temperature-controlled room (~20–23°C).
Subject characteristics.
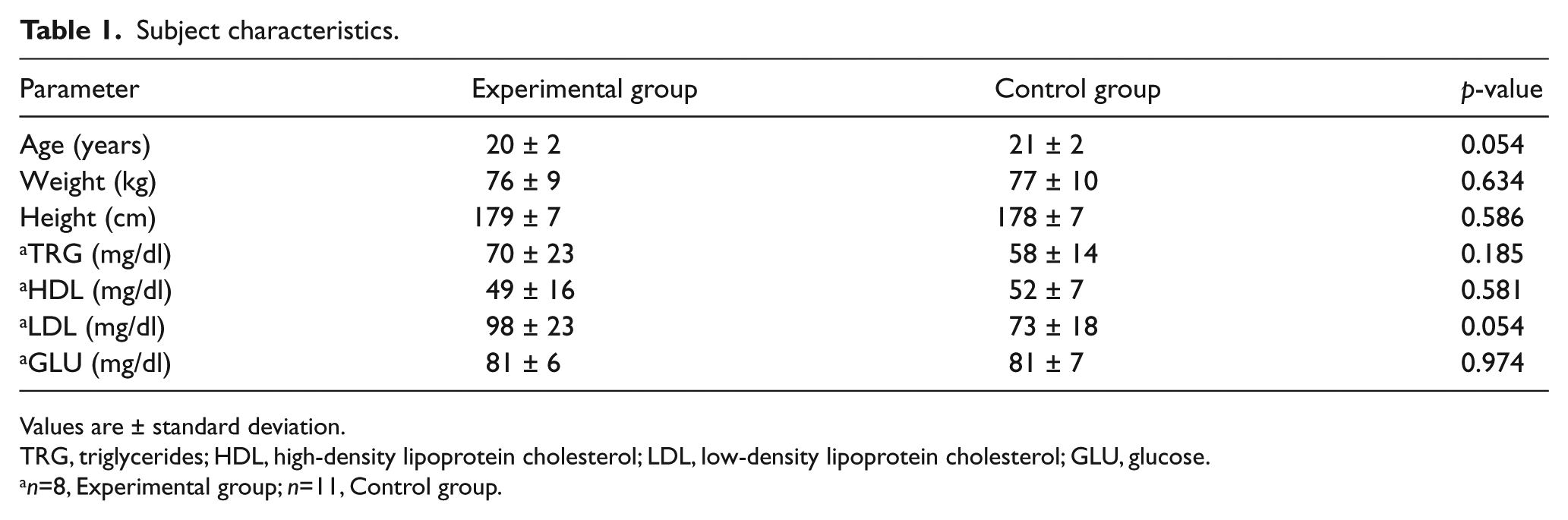
Values are ± standard deviation.
TRG, triglycerides; HDL, high-density lipoprotein cholesterol; LDL, low-density lipoprotein cholesterol; GLU, glucose.
n=8, Experimental group; n=11, Control group.
Subject monitoring
Heart rate was measured using a three-lead electrocardiogram. Blood pressure was measured continuously with finger photoplethysmography (Finometer; Finapres Medical Systems, Amsterdam, The Netherlands). BeatScope Easy software v.01 (Finapres Medical Systems) was used to record an estimate of stroke volume derived from the finger blood pressure wave. Cardiac output was calculated as: cardiac output = heart rate * stroke volume. Total peripheral resistance was calculated as: total peripheral resistance = mean arterial pressure / cardiac output. Due to technical difficulties we were unable to obtain BeatScope recordings in four subjects; therefore, for total peripheral resistance, n=13 in the Experimental group and n=11 in the Control group.
Brachial artery blood velocity and diameter
Blood velocity in the brachial artery was measured continuously using Doppler ultrasound operating at 4 MHz (Vivid i2; GE Medical Systems, London, ON, Canada). The probe was placed approximately 5 cm proximal to the antecubital fossa, and a guide was adhered to the skin to ensure the same probe placement between trials. Doppler ultrasound measurements were taken at a 68° insonation angle for reasons previously described. 25 A Multigon 500P TCD spectral analyzer (Multigon Industries, Yonkers, NY, USA) was used to analyze the Doppler shift frequency spectrum, where mean velocity was determined as a weighted mean of the spectrum of Doppler-shift frequencies. The voltage output was sampled continuously (PowerLab; ADInstruments, Colorado Springs, CO, USA) and stored for later analysis (LabChart; ADInstruments).
Brachial artery images were obtained with the same probe using echo ultrasound at 12 MHz in B-mode (Vivid i2). Parameters on the ultrasound machine were set to optimize longitudinal B-mode images of the lumen–arterial wall interface. The image data were recorded as .avi files on an independent computer (Camtasia Studio; TechSmith Corp., Okemos, MI, USA) with a VGA to USB frame grabber (Epiphan Systems Inc., Ottawa, ON, Canada).
Experimental procedure
Participants lay supine, and their left arm was extended to the side for ultrasound measurements. Blood pressure measurements were made on the right arm. After approximately 30 minutes of supine rest, participants performed the first EX-FMD trial. Following a minimum 10-minute rest (waiting until the brachial artery diameter had returned to baseline), a second EX-FMD trial was performed. This was identical to the first trial in the Control group. In the Experimental group, the second trial was performed with submersion of one foot in ice water (CPT) for the duration of the exercise period (Figure 1).
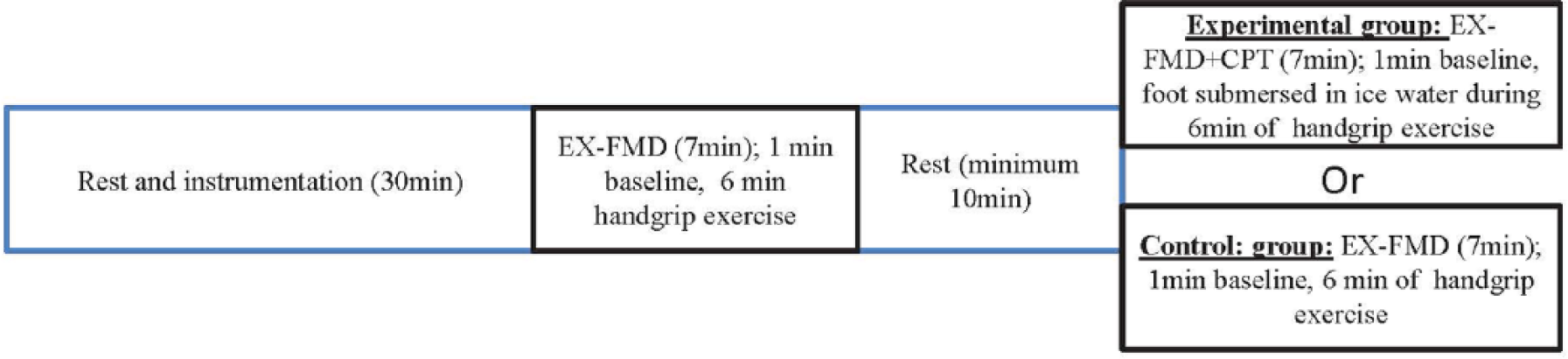
The experimental protocol. A minimum of 10 minutes, or the time until the brachial artery diameter returned to baseline, was allowed between EX-FMD trials. The CPT involved placing the right foot in an ice bath for 3 minutes, followed by removal of the right foot and simultaneous submersion of the left foot for 3 minutes. (EX-FMD: handgrip exercise-induced flow-mediated vasodilation; EX-FMD+CPT: EX-FMD with a CPT performed during the handgrip exercise bout.)
EX-FMD
In each EX-FMD trial, brachial artery blood velocity and diameter were recorded for 1 minute at baseline and then during 6 minutes of handgrip exercise. During the handgrip exercise, isometric handgrip force feedback (percent maximal voluntary contraction) was displayed continuously (PowerLab). Subjects achieved the required force and duration for each contraction by displacing the force readout line to the desired level in time with a 1-second contraction / 5-second relaxation duty cycle metronome. 26 In both trials the goal was to reach and maintain a target brachial artery shear rate of 75 s–1 during exercise. Shear rate (an estimate of shear stress without blood viscosity) was calculated as: shear rate = mean blood velocity / vessel diameter. This target was selected because it has previously been shown to result in a robust FMD response and because it requires an exercise intensity that can be comfortably maintained for 6 minutes. 15 The blood velocity required to achieve the target shear rate was calculated for each subject as follows: required blood velocity = 75 s–1 * brachial artery diameter. To estimate the exercise intensity necessary to achieve the required blood velocity, subjects performed a series of contractions at various % maximal voluntary contractions during the familiarization visit. During the EX-FMD trial the intensity was adjusted by an experimenter who coached the subject to maintain the desired blood velocity.
CPT
The CPT was performed concurrently with the handgrip exercise during the second EX-FMD trial in the Experimental group. After the 1-minute baseline period, participants began the handgrip exercise. At this point, lab personnel immersed one of the participant’s feet in the ice-water bath, which was maintained at a constant temperature (4.5 ± 0.5°C). This foot was kept in the bath for 3 minutes and then was removed as the opposite foot was submerged for 3 minutes. The CPT therefore totaled 6 minutes in duration, aligned with the 6 minutes of handgrip exercise. All participants completed the full 6 minute CPT.
Blood lipids and glucose
At the end of the ultrasound data collection, a small sample of blood was taken by finger prick for analysis of blood lipid and glucose levels using a Cholestech LDX system (Alere Inc., Ottawa, ON, Canada). Due to technical difficulties, this sampling and analysis was only completed in eight subjects in the Experimental group and 11 subjects in the Control group.
Data analysis
Hemodynamic variables
Heart rate, mean arterial pressure and total peripheral resistance data were analyzed offline and compiled into 3-second average time bins (LabChart). For each variable, a 1-minute average baseline value and a peak 1-minute average during exercise were reported.
Brachial artery diameter
Brachial artery image files were analyzed using automated edge detection software (FMD/Blood Flow Acquisition and Analysis; Reed Electronics, Perth, WA, Australia) as previously described. 10 The diameter data were compiled into 3-second time bins for alignment with blood velocity and calculation of shear rate (see below). EX-FMD was calculated as the percent change in diameter from baseline to the peak 1-minute average during exercise.
Brachial artery blood velocity
Blood velocity was analyzed offline in 3-second average time bins (LabChart). The blood velocity data were assembled into 1-minute averages, and the blood velocity for each trial is reported as an average of the steady-state period (last 5 minutes of exercise).
Shear rate
The following equation was used to calculate shear rate: shear rate = mean blood velocity / vessel diameter. This was achieved using aligned 3-second average diameter and blood velocity time bins. The shear rate data were assembled into 1-minute averages and the shear rate for each trial is reported as an average of the steady-state period (last 5 minutes of exercise).
Statistical analysis
The data are reported as means ± standard deviation. To compare subject characteristics between groups, t-tests were used. ANOVA analysis (factors group (between-subjects; Experimental and Control) and trial (within-subjects; trials 1 and 2)) was used to compare all other variables. Post hoc analysis to explore significant interactions was done via pairwise comparisons (t-tests and paired t-tests as appropriate). The level of significance was set at p < 0.05 for all tests. All statistics were calculated using SPSS (SPSS Inc., Chicago, IL, USA) or Sigma Plot (Systat Software Inc., San Jose, CA, USA).
Results
Subject characteristics
The average age, height, weight, and blood lipid profiles of the participants are shown in Table 1. Group differences approached significance for age (higher in the Control group; p=0.054) and LDL (lower in the Control group; p=0.054) only.
Hemodynamic variables
The average heart rate, mean arterial pressure and total peripheral resistance at baseline and during handgrip exercise are shown in Table 2.
Hemodynamic, arterial and force parameters.
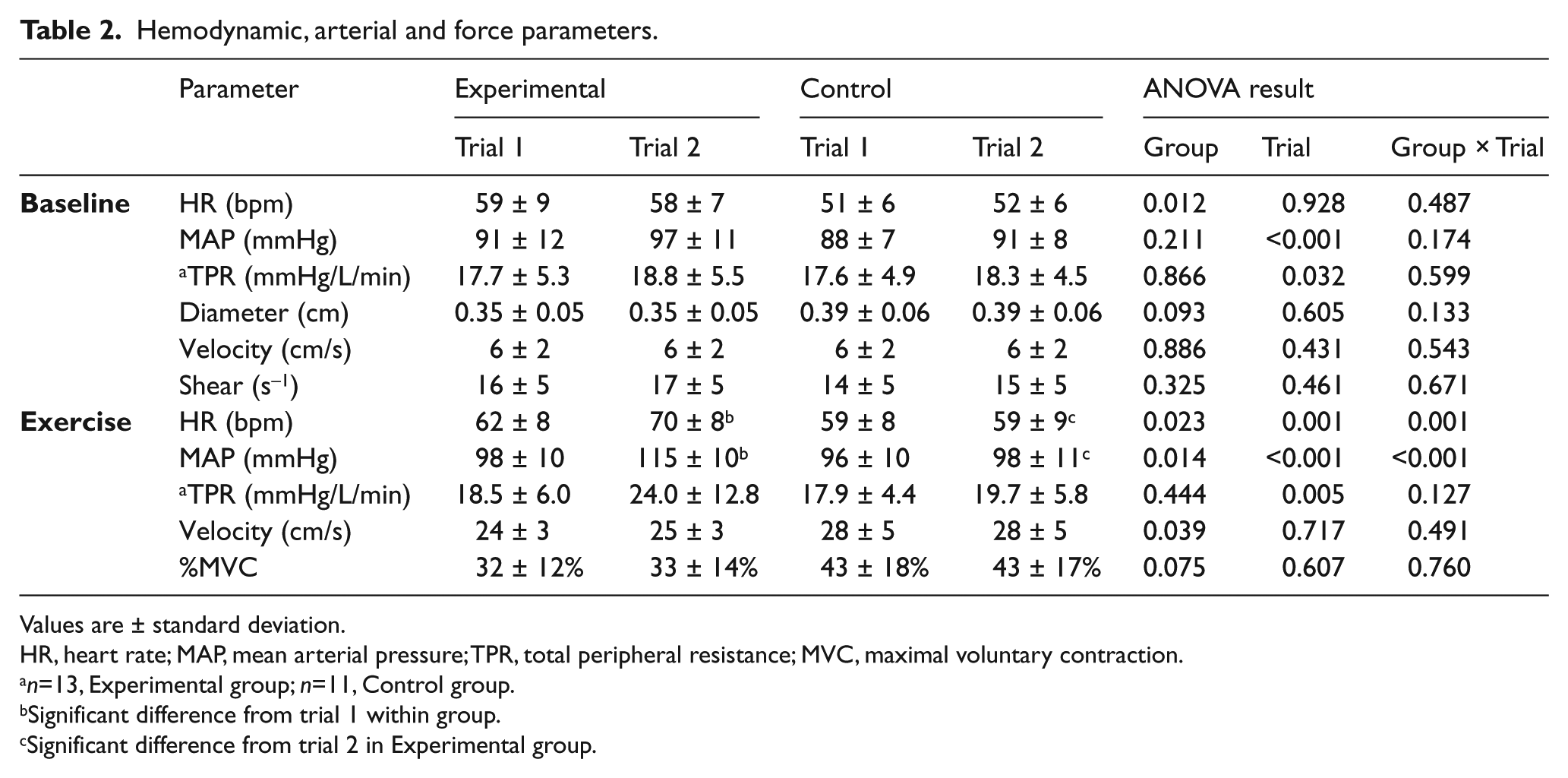
Values are ± standard deviation.
HR, heart rate; MAP, mean arterial pressure; TPR, total peripheral resistance; MVC, maximal voluntary contraction.
n=13, Experimental group; n=11, Control group.
Significant difference from trial 1 within group.
Significant difference from trial 2 in Experimental group.
Heart rate
Baseline heart rate did not differ between trials (main effect of trial p=0.928); however, heart rate was higher in the Experimental group versus the Control group (main effect of group p=0.012) (group × trial interaction p=0.487). During handgrip exercise, there was a significant main effect of group (p=0.023) and trial (p=0.001), and a significant interaction between group and trial (p=0.001). Post hoc analysis revealed that heart rate was significantly greater in trial 2 versus trial 1 in the Experimental group (p<0.001) but not in the Control group (p=0.868). In addition, heart rate was not significantly different between groups in trial 1 (p=0.262), but it was significantly greater in the Experimental group in trial 2 (p=0.002).
Mean arterial pressure
Baseline mean arterial pressure did not differ between groups (main effect of group p=0.211); however, it was significantly greater in trial 2 versus trial 1 (main effect of trial p<0.001) (group × trial interaction p=0.174). During exercise, there was a main effect of group (p=0.014) and trial (p<0.001), and a significant interaction between group and trial (p<0.001). Post hoc analysis revealed that mean arterial pressure during exercise was significantly greater during trial 2 versus trial 1 in the Experimental group (p<0.001) but not in the Control group (p=0.095). In addition, exercise mean arterial pressure was not different between groups in trial 1 (p=0.480), but it was significantly greater in the Experimental group versus the Control group in trial 2 (p<0.001).
Total peripheral resistance
Baseline total peripheral resistance was not significantly different between groups (main effect of group p=0.866); however, trial 2 total peripheral resistance was significantly greater than trial 1 total peripheral resistance (main effect of trial p=0.032) (group × trial interaction p=0.599). Similarly, during exercise total peripheral resistance was not significantly different between groups (main effect of group p=0.444); however, total peripheral resistance in trial 2 was significantly greater than total peripheral resistance in trial 1 (main effect of trial p=0.005) (group × trial interaction p=0.127).
Shear rate
Baseline shear rate was not different between groups (main effect of group p=0.325) or trials (main effect of trial p=0.461) (group × trial interaction p=0.671). As expected with targeting of shear rate, there was no effect of group (main effect of group p=0.823) or trial (main effect of trial p=0.726) (group × trial interaction p=0.646) on the shear rate stimulus during exercise (Figure 2). The velocity reached to achieve the shear rate was slightly higher in the Control group (p=0.039) (Table 2).
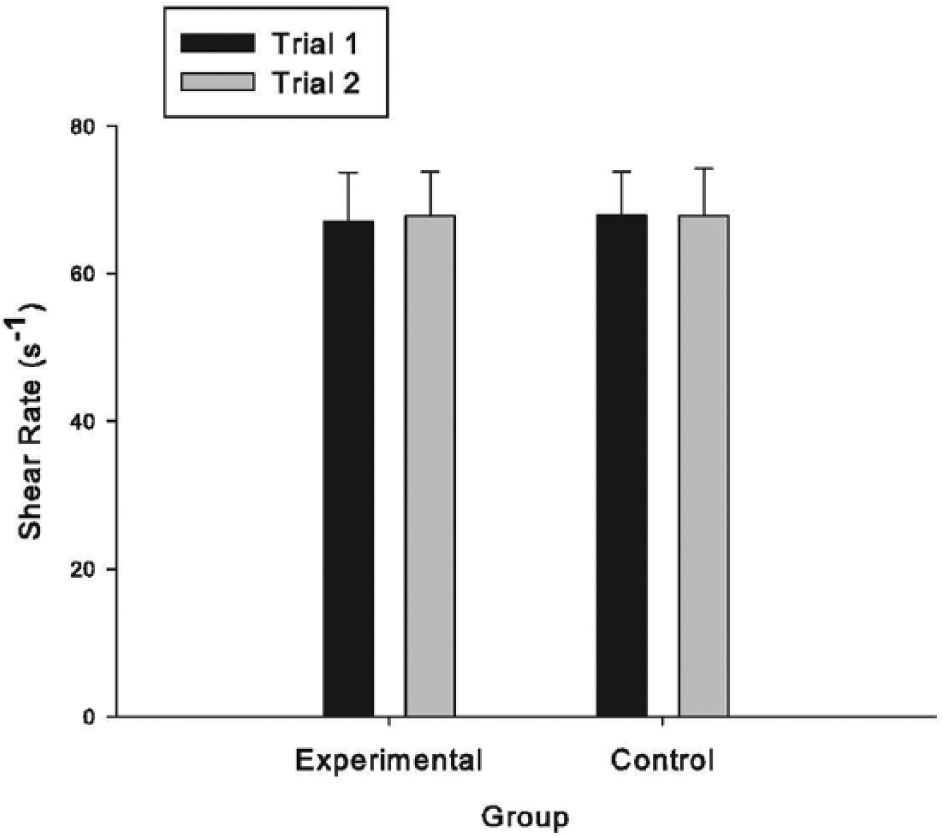
The average shear rate stimulus during the last 5 minutes of the handgrip exercise (steady-state period). (Error bars are ± standard deviation.)
Baseline diameter and %EX-FMD
There was no significant effect of group (main effect of group p=0.093) or trial (main effect of trial p=0.605) (group × trial interaction p=0.133) on baseline diameter (Table 2). There was also no significant effect of group (main effect of group p=0.508) or trial (main effect of trial p=0.592) (group × trial interaction p=0.879) on %EX-FMD (Figure 3).
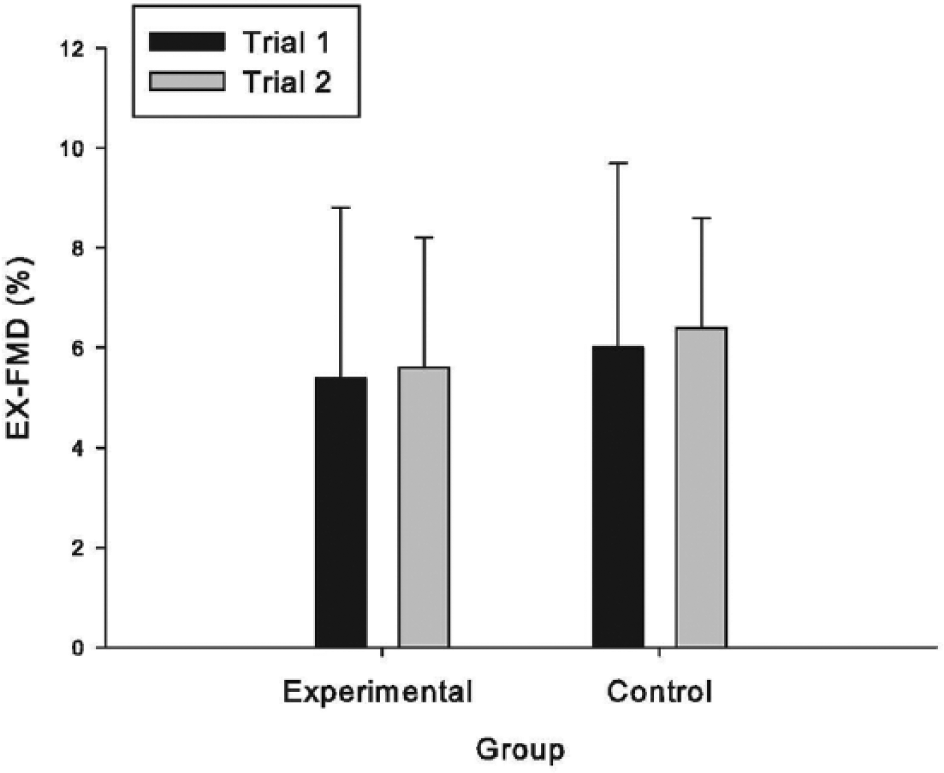
Percent exercise-induced flow-mediated dilation (%EX-FMD). (Error bars are ± standard deviation.)
Handgrip exercise intensity
The average % maximal voluntary contraction throughout the 6 minutes of exercise was not significantly different between groups (main effect of group p=0.075) or trials (main effect of trial p=0.607) (group × trial interaction p=0.760) (Table 2).
Discussion
The purpose of this study was to perform the first examination of the impact of a CPT on concurrent handgrip EX-FMD. A robust response to the CPT was indicated by increases in heart rate and mean arterial pressure; however, brachial artery EX-FMD measured simultaneously was not different from the Control condition. These results indicate that the physiological response evoked by the CPT did not impact the ability of the brachial artery endothelium to respond to exercise-induced increases in shear stress and suggests that in this population, an acute, sympathoexcitatory stimulus does not interfere with conduit artery FMD responses during exercise. This is in contrast to previous observations of impaired FMD responses to a brief shear stress stimulus during a CPT,23,24 and suggests that the impact of CPT-stimulated signals may be shear stress profile-specific. An intact response to an exercise-induced shear stress stimulus would tend to support active muscle perfusion in the presence of painful/stressful stimuli.
CPT–FMD interaction
Several studies have examined the impact of a CPT and other acutely stressful and painful stimuli on endothelial function.23,24,27 Sympathetic nervous activity, epinephrine, and hemodynamic responses increase shortly after the onset of a stressor 28 and begin to return to baseline immediately post-stressor, while other responses are significantly delayed (e.g. peak cortisol concentrations occur 20–40 minutes following stressor onset 28 ). Therefore, the ‘stress-associated’ physiological signals present to interact with FMD differ depending on the timing of FMD evaluation to stressor application. 29 We have previously observed that the EX-FMD response is modestly enhanced 15 but not 35 minutes following a CPT in young healthy men. 22 To our knowledge, this is the only previous study examining EX-FMD in relation to a CPT. In the present study, EX-FMD was measured concurrently with the CPT experience, and we found no significant difference from Control conditions (Figure 3). Taken together, these data suggest that EX-FMD is unaffected by the signals present during a CPT, and is modestly enhanced by the signals that shortly follow CPT cessation. This is in contrast to observations that a CPT performed concurrently with RH-induced increases in shear stress impairs brachial artery RH-FMD by ~35–70%.23,24 These studies also used foot immersion, with a 5-minute 23 or 10-minute 24 duration.
Reactive hyperemia and handgrip exercise elicit very distinct shear stress profiles in the brachial artery, which likely influence the transduction pathways, and potentially the vasodilators, that are involved in the respective FMD responses.8,12,30–33 Differing vulnerabilities of RH-FMD and EX-FMD to acute stimuli have previously been reported by our group 16 and others. 17 Given the contrast of our findings with the previous work indicating impaired RH-FMD during a CPT, our findings suggest that the impact of CPT signals on FMD may be non-uniform and specific to the nature of the shear stress stimulus. These data add to the evidence indicating that an observed impact of a given stimulus on RH-FMD should not be generalized to EX-FMD.
Although not measured directly here, the CPT has been demonstrated to raise sympathetic nervous activity, indicated by an increase in the rate of peroneal nerve bursts 21 and an increase in circulating norepinephrine. 24 In addition, cold exposure stimulates nociceptors 34 and is perceived as both painful and stressful. 22 Interventions that acutely elevate sympathetic nervous activity have been shown to impair RH-FMD in some, 35 but not all, 24 cases, and sympathetic nervous activity may have been involved in impairing endothelial function in previous CPT studies.23,24 It is thought that impairment could be due to a blunting of dilation due to a superimposed vasoconstrictor signal or neural interactions with endothelial function. 36
The hemodynamic responses to the CPT are secondary to sympathetic activation, and the magnitude of the increase in mean arterial pressure (~18 mmHg) observed in the present study is similar to previous reports in which RH-FMD was observed to be impaired.23,24 However, we did not detect a significantly higher total peripheral resistance during trial 2 in the Experimental group (EX-FMD test + CPT) versus trial 2 in the Control group (EX-FMD test alone) (no interaction between group and trial, p=0.127) (Table 2). This suggests a lack of a pronounced peripheral vasoconstriction response to the CPT. It is therefore possible that in individuals with a more profound constrictor response EX-FMD may be adversely affected by the CPT. However, exploratory analysis indicated no relationship between the change in total peripheral resistance with the CPT and the change in EX-FMD in the Experimental group (data not shown).
Significance of EX-FMD responses
The use of exercise-induced increases in shear stress for investigating conduit artery FMD has been validated previously. Specifically, it was demonstrated that brachial and radial artery dilation during a brief (6-minute) bout of handgrip exercise is due to increases in shear stress (i.e. it is FMD) and not a vasodilatory signal that is conducted upwards from the active muscle vascular bed.10,11 EX-FMD is understudied; however, a small body of evidence indicates that it provides information that is relevant to arterial health. First, FMD in response to exercise or other sustained, modest increases in shear stress has been shown to be impaired in some populations at increased risk for cardiovascular disease (patients with type 1 diabetes 18 and smokers15,19). However, this has not always been found (patients with hypercholesterolemia 8 ). Future research is required to determine if, like RH-FMD, 37 EX-FMD has some disease prediction value.
EX-FMD can play a role in tissue perfusion, and if this dilatory contribution were compromised in vulnerable populations and vascular beds (e.g. in the heart in a coronary artery disease population or in the leg in a peripheral artery disease population), it might contribute to clinically important ischemia.2,13,14,38 If EX-FMD were vulnerable to impairment by elevated sympathetic nervous activity (elevated in the present study with the CPT, but also elevated by mental stress and certain disease states), this might result in compromised perfusion, and this could contribute to the relationship between sympathetic activity and mortality. 39 While the present results do not support an impact of acute sympathetic activation on EX-FMD, this may differ in other populations. Further research is required to establish the precise circumstances and populations in which EX-FMD impairment is present and clinically/functionally relevant.
Limitations
This study was performed in young, healthy males, and the results cannot be extended to other populations. Also, muscle sympathetic nervous activity, epinephrine and norepinephrine were not assessed, and changes in these variables might have provided further insight regarding the response to the CPT and its potential to influence EX-FMD responses. However, the observed hemodynamic response to the CPT was similar to that of other studies in which the CPT impaired RH-FMD. This suggests that our participants responded typically and to a degree that could influence some aspects of endothelial function.
Given the potential for a lasting impact of a CPT on EX-FMD, 22 we could not counterbalance the order of the presentation of the CPT in the Experimental group (the CPT was always experienced in trial 2). It is possible that the impact of the CPT on EX-FMD might have been different if it had been experienced during the first EX-FMD trial; however, this seems unlikely given that multiple, closely spaced handgrip exercise trials result in a stable EX-FMD response (demonstrated in the Control group and in Pyke and Jazuli 40 ). Although it did not reach significance (group × trial interaction p=0.174), the rise in baseline mean arterial pressure from trial 1 to trial 2 was larger in the Experimental group (6 mmHg vs 3 mmHg; Table 2). It is possible that this indicates some anticipation of the impending CPT in the Experimental group, but this is unlikely to have impacted the results given that the much more robust elevation in blood pressure during the CPT did not significantly impair the EX-FMD response. Finally, we did not perform a CPT to characterize the hemodynamic reactivity without simultaneous handgrip exercise, although previous work suggests that handgrip exercise does not alter heart rate and blood pressure responses to a CPT. 41 If the exercise did modulate reactivity to the CPT, this would not alter our primary conclusion that the simultaneous CPT did not have a deleterious impact on the EX-FMD response.
Conclusions
In a population of young, healthy males we found that, when performed concomitantly with handgrip exercise, a CPT achieved with foot immersion in ice water did not result in an impaired brachial artery EX-FMD response. This suggests that, in this population, an acute painful stimulus associated with an increase in sympathetic nervous activity does not interfere with peripheral conduit artery endothelial responses to exercise. Future research is required to examine responses in a range of populations and to identify the impact of chronically elevated sympathetic nervous activity on EX-FMD.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was funded by a Natural Sciences and Engineering Research Council of Canada (NSERC) Discovery Grant and by Canada Foundation for Innovation and Ontario Ministry of Research and Innovation Leaders Opportunity Funding to KE Pyke. TJR Stuckless was supported by a Ministry of Research Innovation Early Researcher Award to KE Pyke.