
Abstract
Objective:
The association of coffee consumption with cardiovascular disease remains controversial. Endothelial function is associated with cardiovascular risk. We examined the association between chronic coffee consumption and endothelium function in elderly inhabitants of the island of Ikaria.
Methods:
The analysis was conducted on 142 elderly subjects (aged 66–91 years) of the Ikaria Study. Endothelial function was evaluated by ultrasound measurement of flow-mediated dilation (FMD). Coffee consumption was evaluated based on a food frequency questionnaire and was categorized as ‘low’ (< 200 ml/day), ‘moderate’ (200–450 ml/day), or ‘high’ (> 450 ml/day).
Results:
From the subjects included in the study, 87% consumed a boiled Greek type of coffee. Moreover, 40% had a ‘low’, 48% a ‘moderate’ and 13% a ‘high’ daily coffee consumption. There was a linear increase in FMD according to coffee consumption (‘low’: 4.33 ± 2.51% vs ‘moderate’: 5.39 ± 3.09% vs ‘high’: 6.47 ± 2.72%; p = 0.032). Moreover, subjects consuming mainly a boiled Greek type of coffee had a significantly higher FMD compared with those consuming other types of coffee beverages (p = 0.035).
Conclusions:
Chronic coffee consumption is associated with improved endothelial function in elderly subjects, providing a new connection between nutrition and vascular health.
Keywords
Introduction
Coffee is one of the most frequently consumed beverages and several studies have evaluated the association between chronic or acute coffee consumption and cardiovascular disease risk.1–5 Recent studies suggest a slight risk reduction for coronary heart disease mortality with moderate coffee consumption.6,7 Moreover, favorable effects of chronic caffeine administration on endothelial cell migration, on re-endothelialization and on the expression of nitric oxide synthase enzyme have also been reported.8,9
It is known that endothelium plays a key role in vascular function and parameters of vascular function and structure show important clinical impact and are associated with cardiovascular risk.10–12 Endothelial function, which is usually quantified by flow-mediated dilatation (FMD) in the brachial artery, 13 reflects the ‘health’ of the vessel wall and is affected by various lifestyle habits (e.g. smoking) and aging.14,15
Ikaria island inhabitants have been recognised as having one of the highest longevity rates universally and a high percentage of healthy aging.16,17 Indeed, in Europe, only 0.1% of the population lives over 90 years, while in Ikaria the percentage is roughly 1%. As Ikaria’s elderly population consists of an isolated rural group with established lifestyle conditions, the study of the factors related to cardiovascular risk seems interesting.
To our knowledge, there are no clinical studies evaluating the effects of chronic coffee consumption on endothelial function, especially in subjects with established cardiovascular risk factors such as elderly individuals. Therefore, under the context of the Ikaria Study,17,18 we examined the association between habitual coffee intake and endothelial function.
Materials and methods
Study sample
The Ikaria epidemiological study17,19,20 has been carried out in the Province of Ikaria, in Greece. In brief, during 2009, a volunteering-based, multistage sampling method was used to enroll 673 permanent elderly inhabitants of Ikaria above the age of 65 years old. The participation rate was 95%. Of the aforementioned sample, we randomly selected one of every fifth participant entering the study in order to evaluate his/her endothelial function; thus, 71 men (75 ± 6 years) and 71 women (75 ± 6 years) were studied in this project. All participants were interviewed by trained personnel (cardiologists, general practitioners and nurses) who used a standard questionnaire developed for the purposes of the study.
Bioethics
The study was approved by the Medical Research Ethics Committee of our institution and was carried out in accordance with the Declaration of Helsinki (1989) of the World Medical Association. All subjects were informed about the aims of the study, agreed to participate and signed an informed consent.
Anthropometric, clinical and biochemical characteristics
Weight and height were measured using standard procedures and body mass index (BMI) scores were calculated as weight divided by height squared (kg/m2). Resting arterial blood pressure was measured three times in the right arm at the end of the physical examination with the subject in a sitting position. Patients whose average blood pressure levels were greater or equal to 140/90 mmHg or were under anti-hypertensive medication were classified as hypertensive subjects. Fasting blood samples were collected between 08.00 and 10:00 hours. Blood lipid examinations (serum total cholesterol, high-density lipoprotein (HDL) cholesterol and triglycerides) were measured using a chromatographic enzymic method in an automatic analyzer (RA-1000). Low-density lipoprotein (LDL) cholesterol was calculated using the Friedewald formula: (total cholesterol) – (HDL cholesterol) – 1/5 (triglycerides). The intra- and inter-assay coefficients of variation of cholesterol levels did not exceed 3%, of triglycerides 4% and of HDL-cholesterol 4%. Hypercholesterolemia was defined as total serum cholesterol levels greater than 200 mg/dl or the use of lipid-lowering agents. All biochemical evaluations were carried out in the same laboratory that followed the criteria of the World Health Organization Reference Laboratories. Diabetes mellitus type 2 was determined by fasting plasma glucose tests and was analyzed in accordance with the American Diabetes Association diagnostic criteria (fasting blood glucose levels > 125 mg/dl (7 mmol/l) or use of special medication, indicating the presence of diabetes).
Sociodemographic and lifestyle variables
The age and sex of the participants were recorded. As regards smoking habits, current smokers were defined as those who smoked at least one cigarette per day or had stopped smoking for less than a year, while non-current smokers were defined as those who had stopped smoking for at least 1 year or reported never smokers.
Assessment of coffee consumption
All participants were asked about their usual frequency and type of coffee consumption (i.e. never, < 1 cup per week, 1–2 cups/day, 3–5 cups/day and > 5 cups/day) over the previous year. Brewed coffee is the richest in caffeine content (135 mg/8 oz (227 g) of coffee), while percolated-roasted ground coffee contains 74 mg of caffeine per 5 oz (142 g), and drip-roasted ground coffee 112 mg per 5 oz (142 g). 21 Furthermore, Greek coffee contains 0.3–6.7 mg/100 ml cafestol and 0.1–7.1 mg/100 ml kahweol, in contrast with filtered coffee, which contains these diterpenes at 0–0.1 mg/100 ml. 22 For the analysis, all types of coffee reported (instant, boiled coffee, ‘cappuccino’ or filtered) were adjusted for one cup of 150 ml coffee and a concentration of 28 mg of caffeine per 100 ml. One cup of coffee was equivalent to 450 ml of brewed coffee or 300 ml of instant coffee. 23 According to the distribution of coffee consumption, we categorized usual coffee consumption as ‘low’ (< 200 ml/day), ‘moderate’ (200–450 ml/day), or ‘high’ (> 450 ml/day). As only 11% of the participants consumed less than one cup of coffee daily, this group was merged with the group who consumed less than 200 ml/day.
Evaluation of vascular function
Endothelial function was evaluated by estimating the FMD in the brachial artery, as previously described.24,25 Endothelium-independent dilation (EID) was defined as the percentage change of vessel diameter from rest to the maximum diameter post-nitrate administration. Briefly, all subjects were instructed to refrain from smoking at least 6 hours before the examination time, and after 10 minutes’ rest the right brachial artery was scanned in longitudinal section 5 cm above the antecubital fossa using a Vivid e PRO ultrasound imager (General Electric, Milwaukee, WI, USA) equipped with a linear array (4–13 MHz) U/S transducer. A pneumatic cuff placed distal to the ultrasound probe was then inflated to supra-systolic pressure on the forearm for 5 minutes to induce reactive hyperemia. After the release of the ischemia cuff, the brachial artery diameter was measured every 15 seconds for 2 minutes, and FMD was defined as the percentage change of vessel diameter from rest (baseline brachial artery diameter) to the diameter 60 seconds after cuff release. After 10 minutes’ rest, a further arterial diameter measurement was made between 2 and 5 minutes after a single sublingual spray of glyceryl trinitrate (400 μg). EID was defined as the percentage change of vessel diameter from rest to the maximum diameter post nitrate administration.
Statistical analysis
All variables were tested for normal distribution using the P-P plots. The values of triglyceride levels were skewed; thus they were log-transformed to improve normality. Normally distributed variables were expressed as mean ± SD and not normally distributed variables were expressed as median with first and third quartile. Student’s t-test or analysis of variance (ANOVA) were used to compare the mean values of normally distributed variables (i.e. age, BMI, FMD) between different categories of qualitative variables (i.e. coffee consumption). Post hoc analysis after Bonferroni correction was applied to test for pairwise differences between study subgroups. The chi-squared test was used to evaluate dependency between categorical variables (i.e. diabetes mellitus, smoking status and coffee consumption category). Multiple linear regression analysis was used to test for the association between FMD and coffee consumption categories, after adjustment for several covariates known to affect endothelial function. Statistical significance was indicated by p-values < 0.05. Plots of standardized residuals against predicted values were used to evaluate models’ assumption of homoscedacity, while the Durbin–Watson statistic was used to test for serial dependency. Collinearity between independent variables was tested using the VIF criterion. Cook’s distances were used to check for influential points in the regression analyses. All statistical analyses were performed using SPSS software (version 18.0; SPSS Inc., Chicago, IL, USA).
Power analysis with a type I error of 0.05 and a standardized difference of 0.30 in FMD between the three coffee consumption groups revealed that the number of enrolled individuals has a power of > 80% to reveal statistical significance differences.
Results
Basic characteristics of the participants
From the study participants, 80% were characterized as hypertensive, 23% suffer from diabetes mellitus, 73% had hypercholesterolemia, 17% were active smokers and 22% had a history of cardiovascular disease. Concerning coffee consumption, 89% consumed every day at least one cup of coffee while 87% consumed a boiled Greek type of coffee, 6% instant coffee or cappuccino, and 8% filter coffee. The basic characteristics of the participants according to coffee consumption are shown in Table 1. From the elderly participants included in the study, 40% had a ‘low’ daily coffee consumption, 48% a ‘moderate’ consumption and 13% consumed more than 450 ml of coffee daily. As shown in Table 1, there was no difference in the presence of diabetes mellitus, hypertension, hypercholesterolemia and hyperlipidemia between the three groups of coffee consumption.
Characteristic of the study’s sample according to coffee consumption.
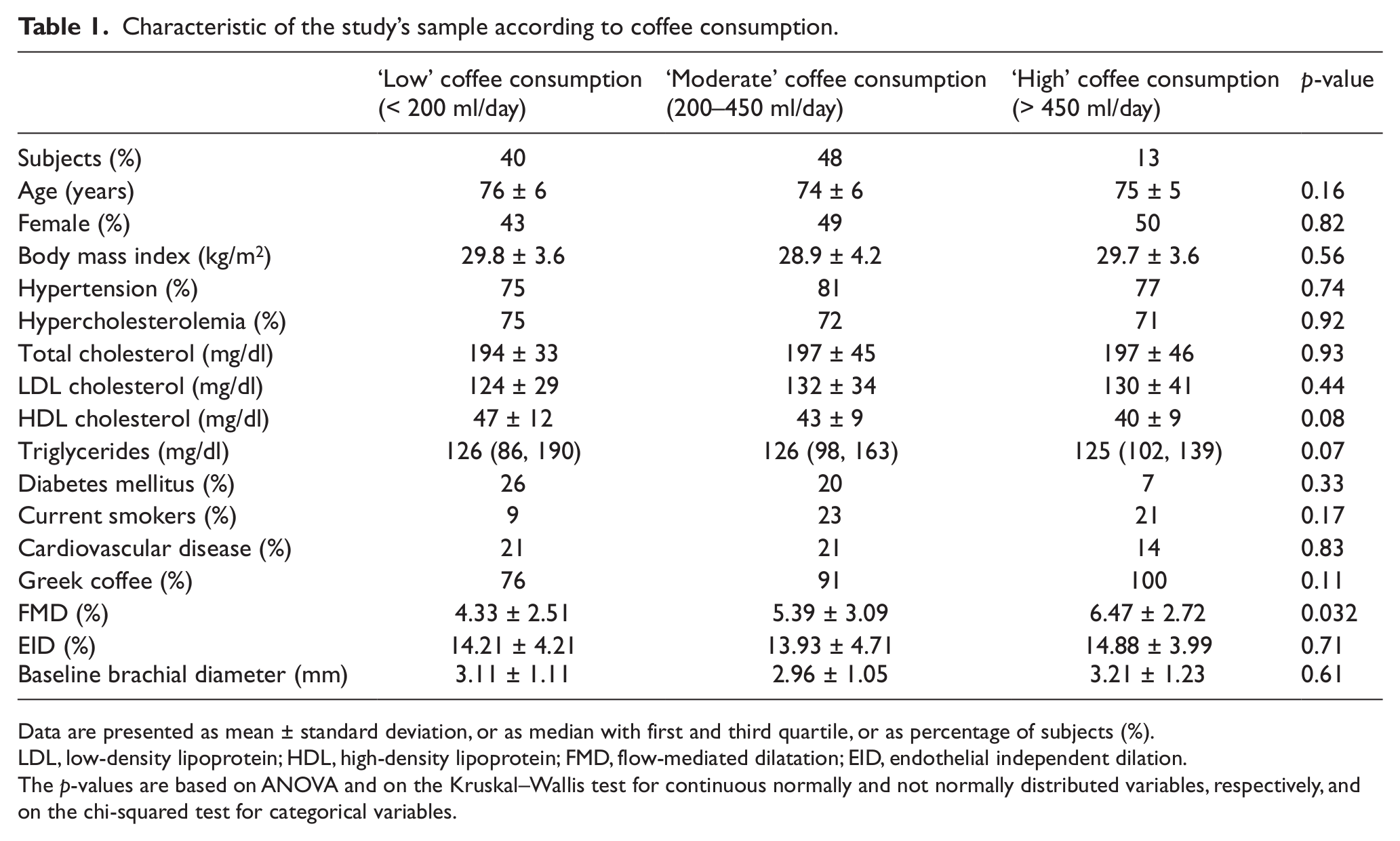
Data are presented as mean ± standard deviation, or as median with first and third quartile, or as percentage of subjects (%).
LDL, low-density lipoprotein; HDL, high-density lipoprotein; FMD, flow-mediated dilatation; EID, endothelial independent dilation.
The p-values are based on ANOVA and on the Kruskal–Wallis test for continuous normally and not normally distributed variables, respectively, and on the chi-squared test for categorical variables.
Vascular function and coffee consumption
In the overall study population, ANOVA revealed a linear increase in FMD according to coffee consumption, while there was no difference in EID and in the baseline brachial artery diameter (Table 1). Furthermore, concerning the association of FMD with coffee intake in hypertensive subjects, the same pattern as in the total study population was also evident (coffee consumption: ‘low’: 4.14 ± 2.83% vs ‘moderate’: 5.01 ± 2.60% vs ‘high’: 6.57 ± 2.64%; p = 0.048), while there was no difference in EID (coffee consumption: ‘low’: 14.35 ± 4.55% vs ‘moderate’: 14.55 ± 4.61% vs ‘high’: 13.78 ± 4.65%; p = 0.87) and in the baseline brachial artery diameter (coffee consumption: ‘low’: 3.21 ± 1.07 mm vs ‘moderate’: 3.06 ± 1.17 mm vs ‘high’: 3.61 ± 1.22 mm; p = 0.30).
Interestingly, regression analysis revealed that, in the whole study population, subjects consuming mainly the boiled Greek type of coffee had significantly higher FMD compared to those consuming other types of coffee beverages independently of the daily coffee consumption in ml/day (5.26%, 95% CI (4.73, 5.80) vs 3.65%, 95% CI (2.27, 5.04); p = 0.035) (Figure 1).
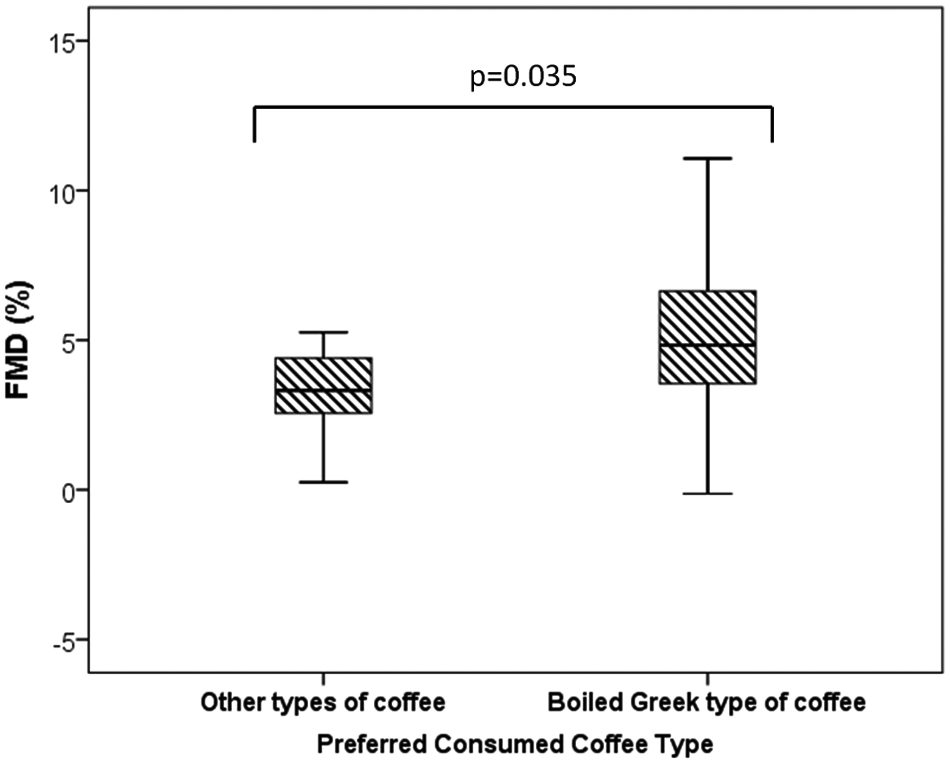
Box-plots of FMD values according to preferred consumed coffee type. (FMD, flow-mediated dilatation.)
However, residual confounding may exist; thus, multiple linear regression analysis, after adjusting for age, sex, BMI, smoking habits, the presence of hypertension, diabetes mellitus, hypercholesterolemia and cardiovascular disease, revealed that subjects who consumed daily less than 200 ml of coffee had significantly lower FMD compared to those who consumed daily more than 450 ml of coffee independently of confounders affecting endothelial function and the general health of the participants (Table 2) (Figure 2, panel A).
Results from multiple linear regression analysis that evaluated the association between FMD (dependent outcome), coffee consumption (main effect) and various other covariates in the total sample population.
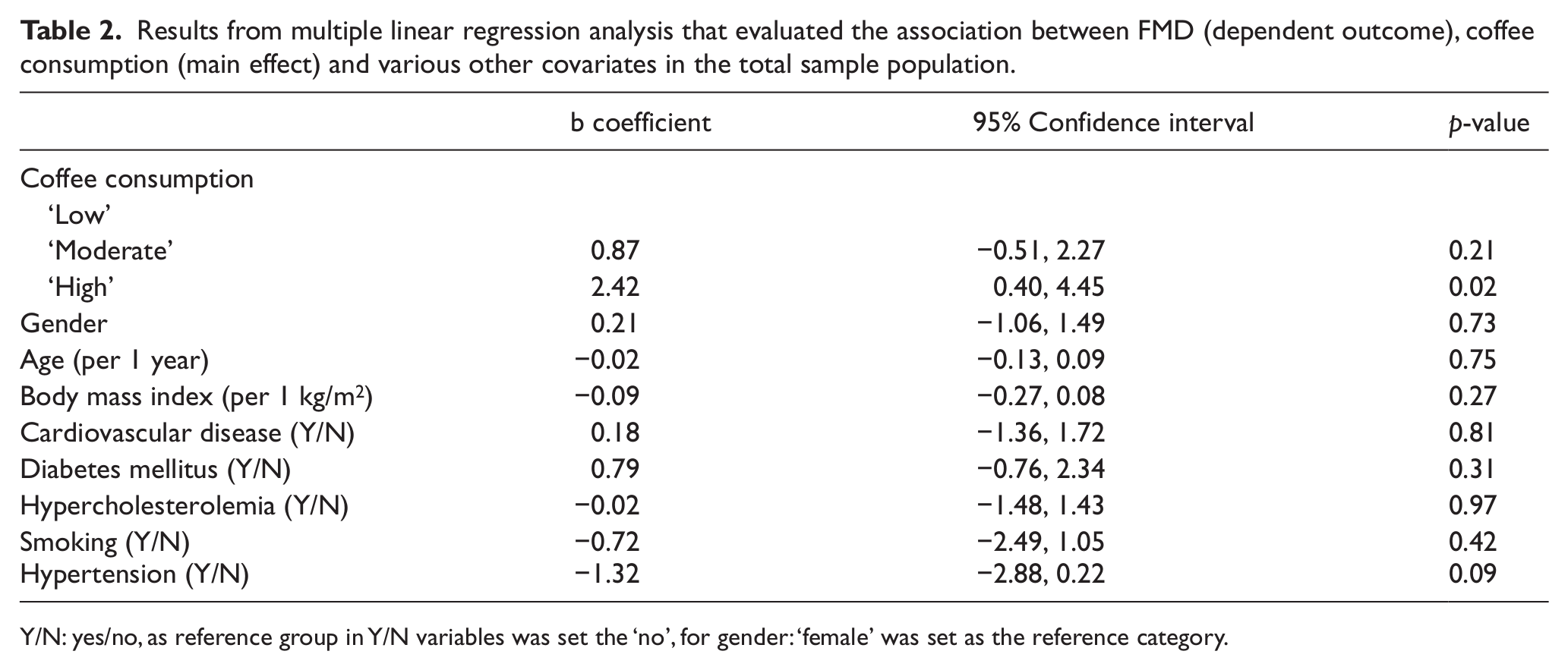
Y/N: yes/no, as reference group in Y/N variables was set the ‘no’, for gender: ‘female’ was set as the reference category.
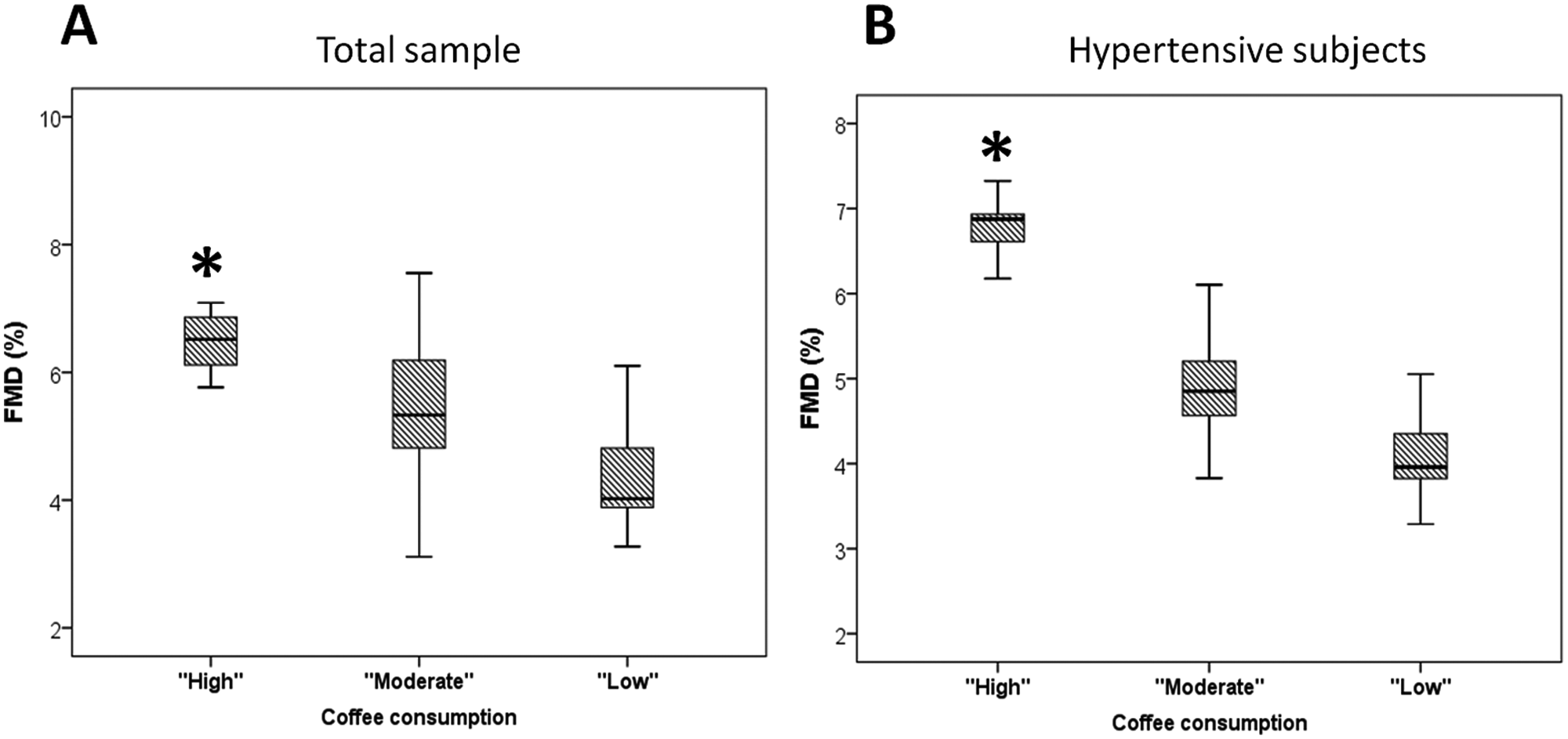
Box-plots of adjusted FMD values for several confounders according to coffee consumption. Panel A: Whole study population; Panel B: Hypertensive subjects. (FMD, flow-mediated dilatation. *p < 0.05 compared to ‘low’ coffee consumption category.)
Interestingly, in hypertensive participants, multiple linear regression analysis, after adjustment for the aforementioned confounders, reveals that subjects who consumed daily less than 200 ml of coffee had significantly lower FMD compared to those who consumed daily more than 450 ml of coffee independently of confounders affecting endothelial function and the general health of the participants (Table 3) (Figure 2, panel B).
Results from multiple linear regression analysis that evaluated the association between FMD (dependent outcome), coffee consumption (main effect) and various other covariates in hypertensive subjects.
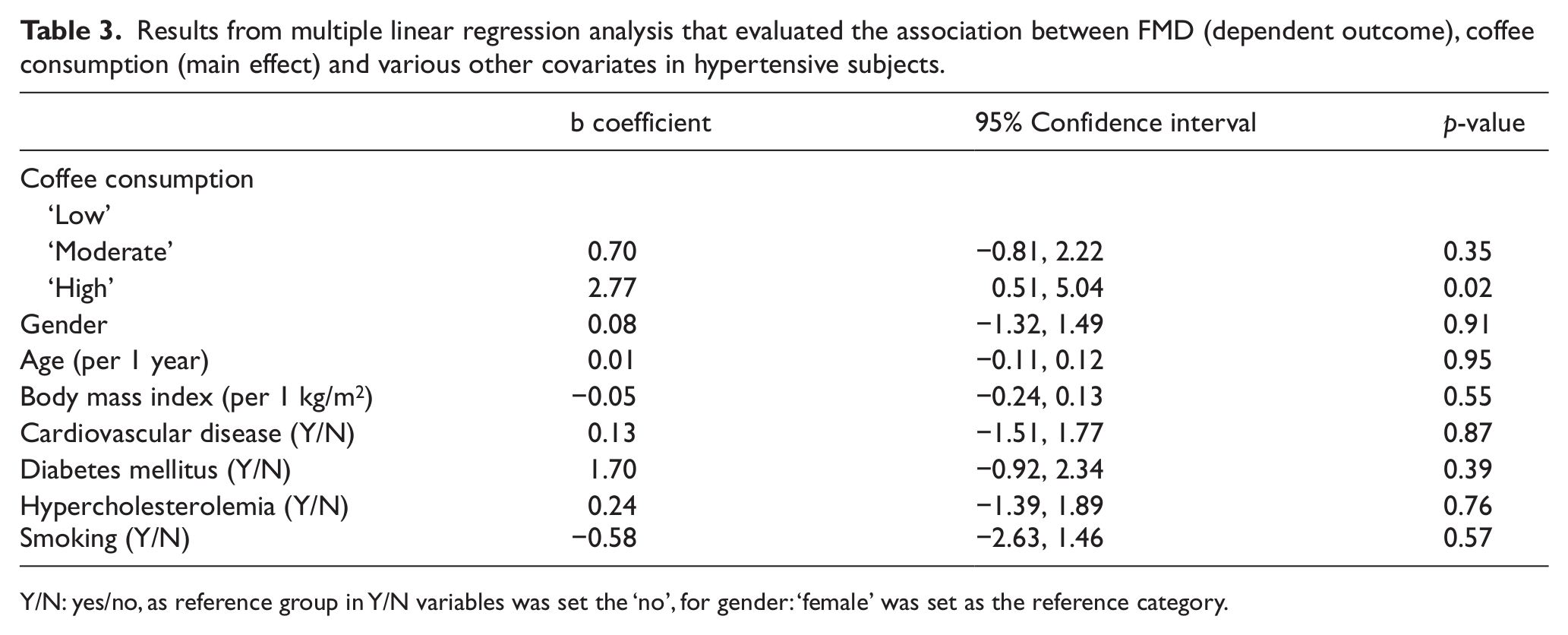
Y/N: yes/no, as reference group in Y/N variables was set the ‘no’, for gender: ‘female’ was set as the reference category.
Coffee consumption and arterial hypertension
In the whole study population, there was no difference in systolic (‘low’: 140 ± 20 mmHg vs ‘moderate’: 146 ± 17 mmHg vs ‘high’: 136 ± 17 mmHg; p = 0.17) and diastolic (‘low’: 79 ± 12 mmHg vs ‘moderate’: 80 ± 12 mmHg vs ‘high’: 77 ± 4 mmHg; p = 0.66) blood pressure according to coffee consumption.
In hypertensive subjects, there was also no association of coffee consumption with systolic (‘low’: 146 ± 19 mmHg vs ‘moderate’: 150 ± 16 mmHg vs ‘high’: 144 ± 6 mmHg; p = 0.49) and diastolic (‘low’: 81 ± 12 mmHg vs ‘moderate’: 82 ± 13 mmHg vs ‘high’: 78 ± 4 mmHg; p = 0.64) blood pressure.
Discussion
The present study, based on the elderly inhabitants of the island of Ikaria, highlighted the correlation of the boiled Greek type of coffee with improved endothelial function. Inhabitants of Ikaria consume at a rate of more than 87% mainly the boiled Greek coffee and there is a linear association of endothelial function with daily coffee consumption. More importantly, subjects consuming mainly Greek coffee had better endothelial function than those consuming other types of coffee beverages. Interestingly, the association of Greek coffee consumption with endothelial function was also evident in hypertensive subjects while there was no difference on arterial blood pressure, EID and baseline brachial artery diameter according to daily coffee consumption.
Coffee is one of the most consumed beverages worldwide, composed mainly by compounds such as caffeine, chlorogenic acid, diterpenes, purinic alkaloids such as theobromine, theophylline, polyphenols, and various lipid-soluble substances, which may have either beneficial or harmful effects on the cardiovascular system.26,27 Coffee has been identified as a major source of antioxidants, but on the other hand it is supposed to have adverse effects on blood cholesterol and homocysteine levels and hypertension.28–31 Caffeine (1,3,7-trimethylxanthine) is the most important and well-known pharmacologic compound of it, acting as a competitive inhibitor of cyclic nucleotide phosphodiesterase isoenzymes and exerting various functions including the modulation of glucose metabolism, alterations in apoptotic processes, immunomodulatory effects, and stimulation of muscle contraction. 9
Acute and chronic coffee intake is associated with increased arterial stiffness and wave reflections in healthy subjects and in hypertensive ones.32,33 Moreover, caffeine intake acutely increases blood pressure 34 and postprandial glucose levels in diabetics subjects – probably due to the increase of catecholamine released. 35 However, data from epidemiological studies concerning the association of coffee consumption with cardiovascular disease risk are conflicting. Some studies have shown a positive association 36 while other studies report no relationship 37 or even a negative association. 21
Endothelial function represents the health of the vessel wall and is associated with nitric oxide (NO) production in response to shear stress. Moreover, endothelial dysfunction is an important early step in the atherosclerotic process 38 and is associated with resistant hypertension 39 and with adverse cardiovascular events.11,40 There is convincing evidence that coffee consumption acutely impairs endothelial function. 6 Nevertheless the impact of chronic coffee intake on endothelial function is largely unknown. Data from epidemiological studies have not confirmed a detrimental effect of chronic coffee consumption 41 on endothelial function, while coffee beverages without caffeine have shown a beneficial effect. These observations imply that other substances of coffee beverages, beyond caffeine, can affect endothelium. 5
The present study revealed an association between habitual coffee consumption, especially the boiled Greek type of coffee, and improved endothelial function in elderly subjects with several comorbidities. Importantly, there was no association between coffee consumption, EID and baseline brachial artery diameter, highlighting the association of coffee consumption with endothelial-dependent dilation. Interestingly, this correlation of daily Greek coffee consumption with endothelial function was also constant in hypertensive subjects and was not affected by other parameters related with general health.
The design of the present study does not permit etiologic association. Based on the results of previous studies, we can attribute the association of coffee consumption with endothelial function to better glucose tolerance, 42 to its phenolic antioxidant properties 43 and to its high-sensitivity C-reactive protein (hsCRP) lowering effect. 44 Moreover, coffee can ameliorate atherosclerosis progression through the prevention of LDL-cholesterol oxidation 45 and by inhibiting platelet aggregation. 46 Caffeine has a direct effect on endothelial function, stimulating the production of NO 47 and the release of Ca2+ from the reticulum, favoring the activation of endothelial NO synthase. 8 Furthermore, caffeine enhances endothelial cell migration and re-endothelialization, partly through an AMP protein kinase-dependent mechanism, suggesting a beneficial role of caffeine on endothelial repair. 9
Interestingly, chlorogenic acid, a polyphenol found in coffee, with its metabolites (caffeic and ferulic acids) have beneficial antihypertensive effects.48,49 The antihypertensive effect of chlorogenic acid is reported to be associated with NO, as caffeic and ferulic acids appear to improve vascular function by reducing reactive oxygen species production and enhancing the bioavailability of NO.49,50 Moreover, other micronutrients, including flavonoids, magnesium, potassium, niacin, and vitamin E, contribute to the observed health effects of coffee consumption, mainly because of their antioxidant properties. 51 Concerning boiled Greek coffee, this seems to offer further anti-inflammatory and antioxidant benefits as it contains 0.3–6.7 mg/100 ml cafestol and 0.1–7.1 mg/100 ml kahweol, in contrast with filtered coffee which contains 0–0.1 mg/100 ml of these diterpenes.21,22 At last, coffee consumption not only exhibits inherent antioxidant properties, but also activates the endogenous antioxidant defense system by increasing plasma levels of glutathione.21,22,51
We note the discrepancy between studies concerning the association of coffee consumption and cardiovascular health. These differences can be attributed to the differences in study design (acute versus chronic coffee intake), in study population (healthy subjects, subjects suffering from arterial hypertension, diabetes mellitus or acute cardiovascular events) and to differences in studied endpoints or surrogate markers of cardiovascular disease. Moreover, part of the discrepancy can be attributed to the different coffee types studied with different contents of caffeine, lipids, polyphenols and other antioxidant substances. Indeed, the boiled Greek type of coffee, which is rich in polyphenols and antioxidants and contains only a moderate amount of caffeine, seems to gather benefits compared to other coffee beverages.
This study, as a cross-sectional study, has some inherent limitations. The relative small sample size in this cross-sectional study cannot provide causative associations. Moreover, the lack of randomization and control group make this study inherent to biases. Especially, recall biases may have happened, particularly in the assessment of dietary habits. Coffee drinking was evaluated on the basis of the subjects’ self-reports. Thus, the real amount of coffee consumed may have been over- or underestimated. Moreover, people living in the Mediterranean islands are not a representative sample of the total Greek or European population. They could be considered a ‘closed’ population for a long time and, therefore, unaffected by the influence of westernized habits. Furthermore, increased consumption of coffee is associated with unhealthy behaviors, such as physical inactivity, unhealthy dietary habits and smoking or, in contrary, decreased coffee consumption can reflect a poor general feeling of health. Although, these potential confounders were statistically controlled, residual confounding may still exist. Finally, the majority of the participants consumed Greek coffee, which meant that the association of other coffee types could not be evaluated in our study. Despite the above-mentioned limitations, the sample size of our study has an adequate power to reveal differences between the three study groups. We can also note that this study examined the habitual coffee consumption and lifestyle characteristic of a population with a high percentage of healthy aging, highlighting the association of coffee consumption with endothelial function throughout aging.
Conclusion
The present study provides evidence that chronic consumption of the boiled Greek type of coffee is associated with improved endothelial function in elderly individuals with an increased burden of cardiovascular risk factors. This evidence provides a further explanation about how chronic coffee consumption can favorably affect cardiovascular risk, providing a new connection between nutritional habits and cardiovascular health. Importantly, given the widespread use of coffee beverages across the world and the fact that even small health effects of coffee could have a large impact on public health, further studies are needed to document the exact beneficial mechanisms of coffee in vascular integrity.
Footnotes
Acknowledgements
We are particularly grateful to the men and women from the island of Ikaria who participated in and collaborated on this survey. We would like to thank especially Konstantinos Chronakis for his technical support. We also wish to express our gratitude to the following: Mr Karoutsos (Mayor of Raches), Mr Stamoulos (Mayor of Evdilos), Mr Teskos (Mayor of St Kyrikos), Dr K Katte, Dr B Mylonakis, Mrs S Spanou (Health Center of Eudilos), Dr S Mamatas, Mr Skaros (General Hospital of St Kyrikos), and the following field investigators: I Andreou, D Aragiannis, S Athanassopoulou, E Christoforatou, K Dimitriadis, J Felekos, N Galiatsatos, E Giakoumi, M Kambaxis, C Kosifa, P Kourkouti, S Kyvelou, S Lagoudakou, G Lazaros, D Maragiannis, A Margazas, C Masoura, V Metaxa, A Patialiakas, S Plytaria, E Poulidakis, B Psaroudaki, D Roussos, J Skoumas, M Striggou, C Sykaras, G Triantafyllou, D Tsiachris, G Tsitsinakis, A Valatsou, D Vasiliou, G Vogiatzi, S Vogiatzoglou, M Xynogala, and V Zoulia.
Author note
The preliminary results of this study have been presented at the Annual Scientific Sessions of the American College of Cardiology, Chicago, Illinois, USA, April 2012.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.