
Abstract
The objective was to compare the efficacy of treatment options for right heart thrombi (RHT) in transit. All published reports between 1992 and 2013 were identified and pooled. We analyzed 328 patients with RHT and pulmonary embolism (PE). The treatments administered were none in 11 patients (3.4%), anticoagulation (AC) with heparin in 70 patients (21.3%), thrombolytics in 122 patients (37.2%), catheter-related treatments in five patients (1.5%) and surgical embolectomy in 120 patients (36.6%). The overall short-term mortality for the entire cohort was 23.2%. The mortality rate associated with no therapy was highest at 90.9%. The mortality associated with AC alone was significantly higher than surgical embolectomy or thrombolysis (37.1% vs 18.3% vs 13.7%, respectively). In univariate analysis, any therapy was better than no therapy with a favorable odds of 16.92 (95% CI 2.05–139.87) for AC, 61.76 (95% CI 7.42–513.81) for thrombolysis and 44.54 (95% CI 5.42–366.32) for surgical embolectomy. In multivariate analysis with age and hemodynamic status entered as covariates, thrombolytic therapy was better than AC with favorable odds of 4.83 (95% CI 1.52–15.36). Similarly, there was a trend in favor of surgical embolectomy with an odds of 2.61 (95% CI 0.90–7.58). The estimated probability of survival in hemodynamically unstable patients with AC, surgical embolectomy and thrombolysis was 47.7%, 70.45% and 81.5%, respectively. There was no significantly increased risk of complications with thrombolytic therapy. In conclusion, left untreated, patients with RHT and PE have very high mortality. Aggressive management with thrombolysis or surgical thrombectomy may be more effective than AC alone in the management of these patients.
Keywords
Introduction
Right heart thrombi (RHT) in transit represent emboli from the deep veins that are temporarily lodged in the right atrium or ventricle in patients with pulmonary embolism (PE). They tend to be large and free floating masses (type A thrombi) with a high propensity for distal embolization unlike in situ right atrial clots (type B thrombi) that are small and immobile. 1 Despite the high prevalence of pulmonary thromboembolism, RHT are uncommon but are associated with a catastrophically higher mortality (80–100%)2,3 than seen in untreated or missed pulmonary embolus alone (26–30%). 4 There is, however, little if any consensus for the optimal management of RHT. To date, there are no randomized controlled trials comparing the three widely used management strategies (anticoagulation therapy versus systemic thrombolysis versus surgical embolectomy) and the three (>50 patients) meta-analyses performed thus far have differing recommendations.1,3,4 Also, most published reports on RHT are uncontrolled retrospective case series5 –8 or individual case reports.9 –12 Furthermore, patients treated with anticoagulation, thrombolytics or surgical embolectomy differ in their baseline characteristics or severity of illness, making direct comparisons between the therapeutic strategies difficult. We therefore undertook this pooled analysis of available data to identify a larger series and provide a proposal for the optimal therapeutic approach in patients with RHT.
Methods
Study selection
We conducted a systematic search for published literature on RHT in transit from January 1992 to 22 February 2013. Two authors (GA and PS) performed data collection from three online databases: MEDLINE (PubMed), Cochrane Collaboration of Clinical Trials and Google Scholar. The search terms used were “cardiac thrombus”, “atrial thrombus” and “ventricular thrombus”. Limiting the search parameters to the English Language was applied subsequently. Citations were screened at the title and abstract level and retrieved as full report if they reported on the outcome of patients with RHT. The full texts of all potential articles were reviewed in detail. The bibliographies of retained studies were used to seek additional relevant studies.
Inclusion criteria
Studies were included if the following criteria were all met: (a) presence of clinically (high probability) or diagnostically proven acute PE; (b) presence of right atrial or right ventricular (RV) thrombus; (c) reported on the therapeutic strategy; and (d) reported on the outcome. When there was an overlap of reported cases from the same institution or author, the most recent publication was included in the analysis.
Exclusion criteria
Studies were excluded if any of the following criteria applied: (a) right heart thrombus due to an indwelling catheter, implantable cardioverter defibrillator (ICD) or pacemaker lead, or a foreign device in the heart (atrial septal defect (ASD) closure device or mechanical valves); (b) tumor thrombus; (c) diagnostic dilemma (thrombus versus tumor); (d) systemic inflammatory diseases such as Bechet’s disease, etc; (e) if choice of therapy was narrowed by the primary authors due to a contraindication to either anticoagulation, surgical embolectomy or thrombolysis; and (f) if an English translation of a foreign language paper was not available.
Data extraction
Information collected included first author, year and journal of publication, the number of subjects included, presenting symptoms, underlying etiology, baseline clinical characteristics (heart rate, blood pressure, respiratory rate), electrocardiogram (ECG) evidence of RV strain, echocardiographic data (site, size and description of the thrombus, presence of paradoxical embolism, concomitant left ventricular (LV) thrombus, RV dilation, RV systolic function), initial and final treatment strategy, outcome and complications. The few disagreements between the two reviewers (GA and PC) were settled by consensus.
Study end points and definitions
The study end point was inhospital survival or death. Tachycardia was defined as a heart rate >100 beats per minute. Tachypnea was defined as a respirator rate >25/minute. Hemodynamic instability was identified in patients with shock (systolic BP <90 mm despite fluid resuscitation and requiring inotropic support) or when noted by the primary authors. When two therapies were employed, patients were categorized based on the final therapeutic strategy. Treatment was coded as the treatment actually received and not based on the intention to treat. Patients in the treatment arm were grouped according to the highest intensity of the therapy received because many patients who underwent thrombolysis as well as surgery probably received heparin too as the initial step in management; however, they were not categorized as receiving heparin. All patients in the thrombolysis group received systemic thrombolysis.
Statistical analysis
Categorical variables are reported as n (%) and compared among subgroups using the chi-squared test. Continuous variables are reported as mean ± standard deviation (SD) and compared among groups using one-way ANOVA. The results were considered significant with p-values ≤0.05. Univariate and multivariate binary logistic regression analysis was performed for the association between mortality and independent predictor variables (age, sex, clinical and echocardiographic variables and primary treatment). The results are reported as odds ratios (ORs) and their 95% confidence intervals (CIs). The effect of each variable on the multivariate model was assessed by the likelihood ratio test. Data analysis was performed using IBM SPSS software version 21 (Armonk, NY: IBM Corp.). In Table 3, statistical analysis was limited to only those with available data.
Results
Between January 1992 and February 2013, we identified 166 reports (Figure 1) describing a total of 328 patients with RHT. Most of the studies were single case reports (141 reports) (Supplemental references e1–e138).9 –11 There were 25 case series with a minimum of two and a maximum of 45 reported cases of RHT (e139–e160).5,6,12 The baseline characteristics of the individual patients were not available in most reports. The clinical and echocardiographic characteristics were variably reported (Supplemental Table 1). The locations, type of thrombus, treatment and inhospital outcomes of all 328 patients were available. Long-term (post-hospitalization) follow-up data were available for only 17 patients.
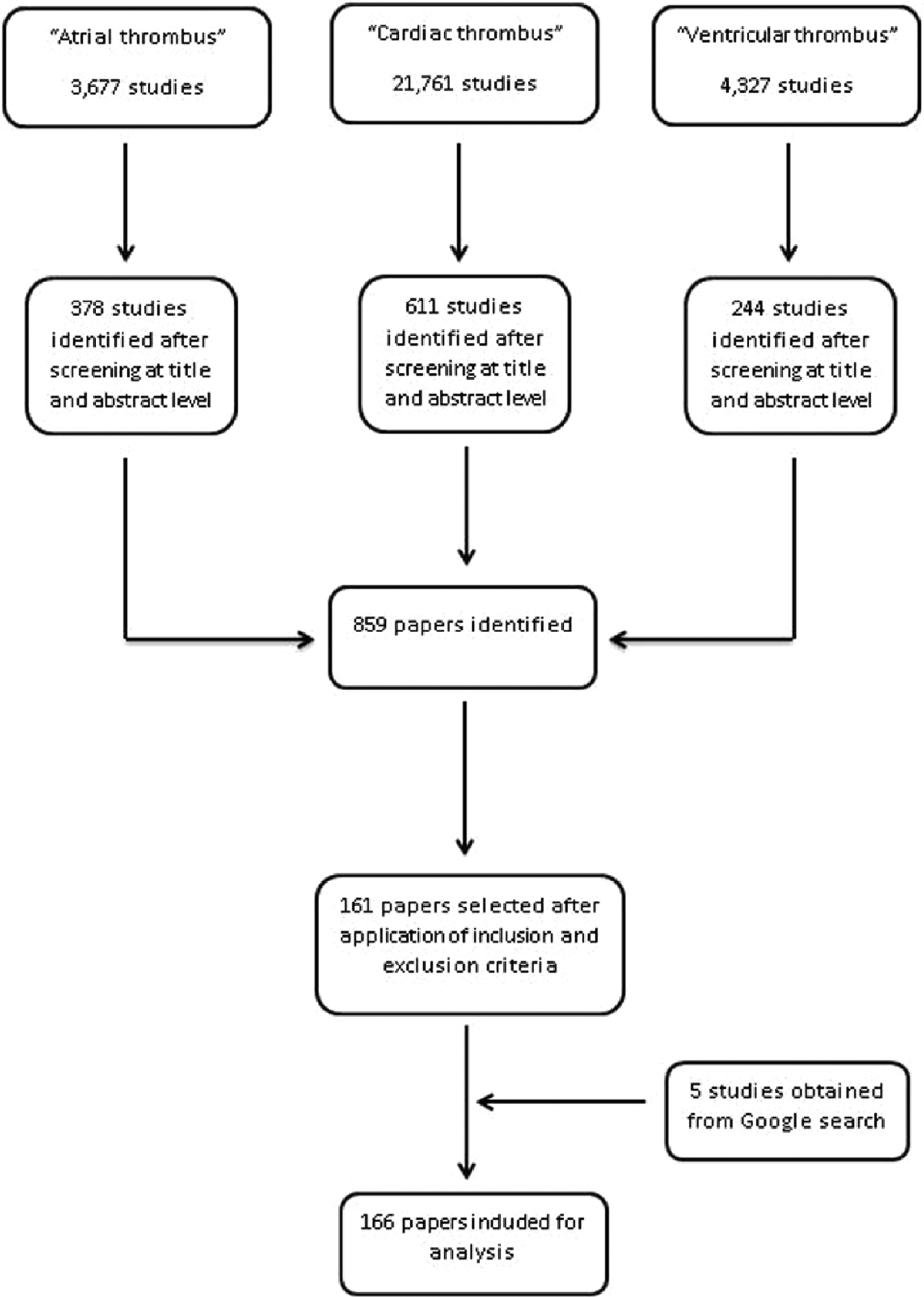
Flow diagram of study selection process.
The main clinical, diagnostic and treatment characteristics of the patients stratified by the three major treatment arms (anticoagulation, thrombolysis and surgical embolectomy) are shown in Table 1. The mean age of the study population was 57.9±16.52 years (range 19 to 87), with an equal distribution of men (47.1%) and women (52.9%). The most common presenting symptom was shortness of breath (69.2%) followed by chest pain (29.2%) and syncope/light-headedness (20.4%). There was no identifiable precipitating factor in most patients (53.7%). In those with a known cause, immobilization/post-surgical stresses (23.9%) and known coagulopathies (9.5%) were the most common precipitating factors.
Characteristics of patients stratified by treatment arm.
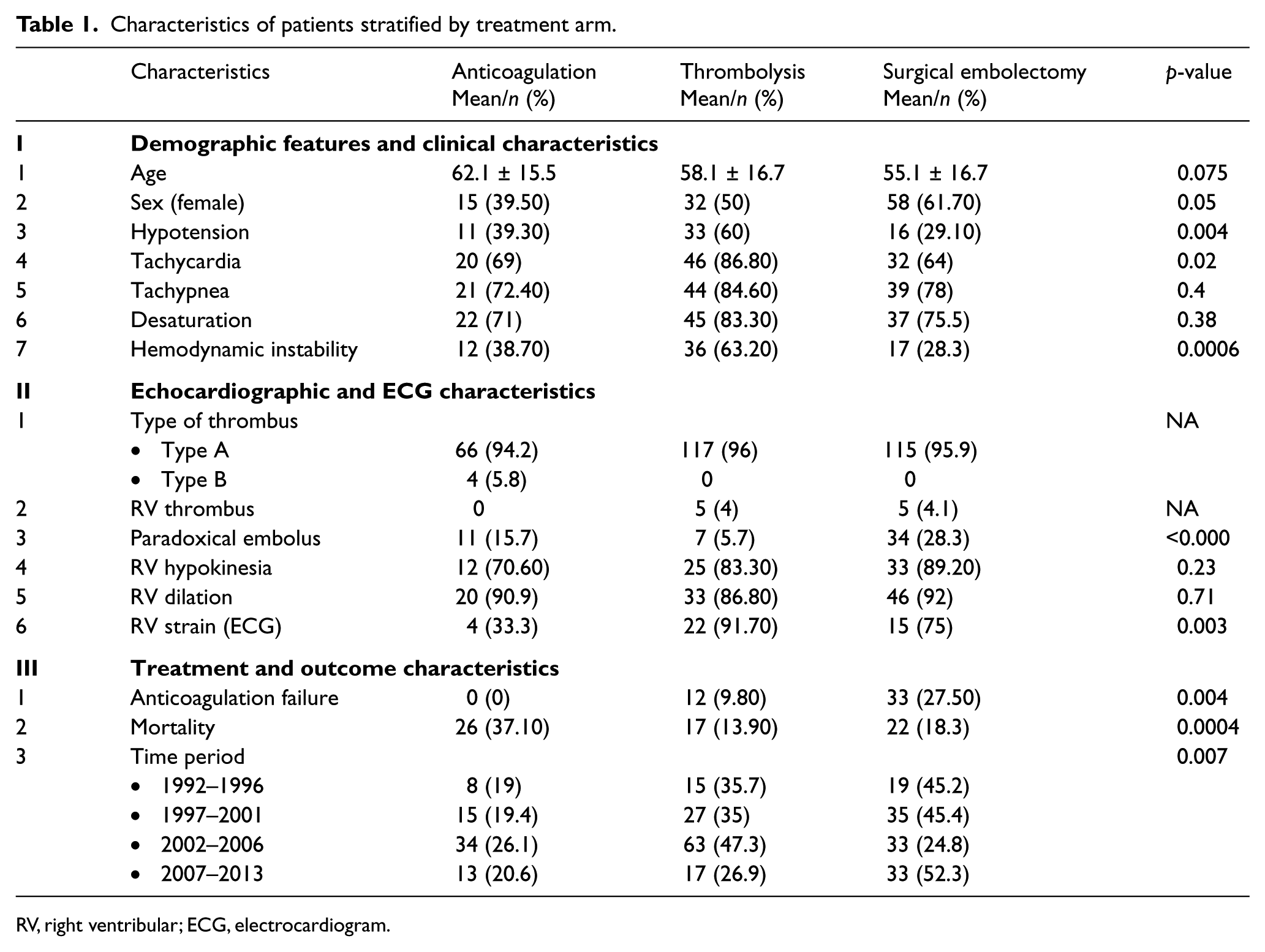
RV, right ventribular; ECG, electrocardiogram.
A right atrial type A thrombus was identified in 314 patients (95.7%) and a RV thrombus in 10 patients (3%). Type B thrombus was identified in only four patients (1.2%). The initial strategy of anticoagulation alone was used in 115 patients. However, in 45 patients (39.4%) the initial strategy of anticoagulation was unsuccessful, 12 (26.6%) of whom were subsequently treated with thrombolysis and 33 (73.3%) with surgical embolectomy. The final treatment offered was none in 11 patients (4%), anticoagulation in 70 patients (21.3%), thrombolysis in 122 patients (37.2%), catheter-directed therapies in five patients (1.5%), and surgical embolectomy in 120 patients (36.6%).
The overall inhospital mortality was 23.2%. The clinical and echocardiographic characteristics of the survivors and non-survivors are shown in Table 2. The highest mortality was seen in untreated patients (90.9%). The mortality rate in patients who received anticoagulation, thrombolysis and surgical embolectomy were 37.1%, 18.3% and 13.9%, respectively. Owing to the small number of patients treated with catheter-directed therapies, this subgroup was not compared to the other three groups
Characteristics of the patients stratified by outcome.
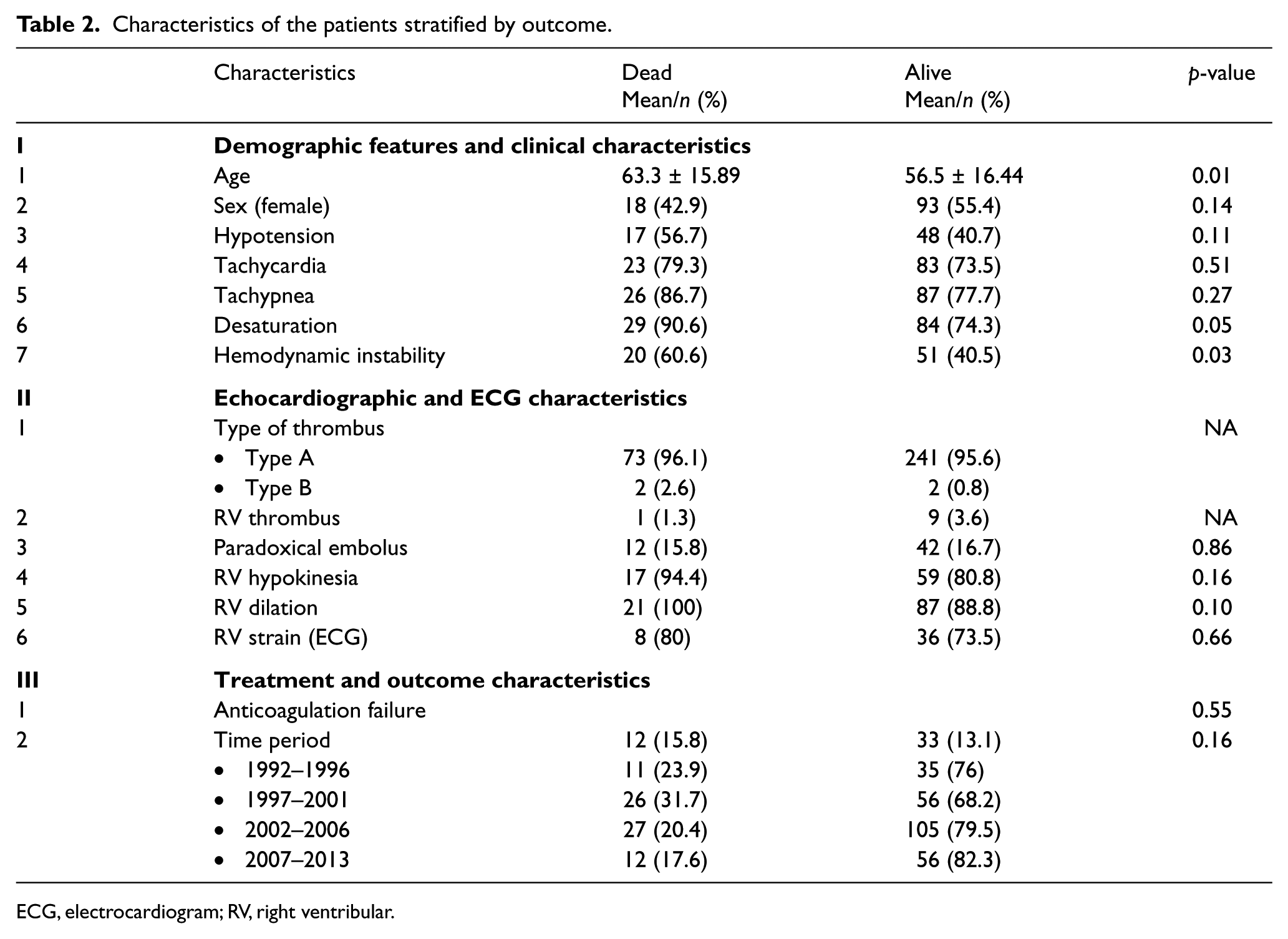
ECG, electrocardiogram; RV, right ventribular.
In univariate binary logistic regression, age, hemodynamic status and type of treatment were significantly associated with the outcome of patients with RHT (Table 3). In multivariate modeling, hemodynamic status and type of treatment were the only variables that significantly affected the outcome of patients with RHT (Table 3). Using anticoagulation as reference and after adjusting for age and hemodynamic status, the OR for survival was 4.83 (95% CI 1.51–15.36) with thrombolysis and 2.61 (95% CI 0.90–7.58) with surgical embolectomy. The estimated probability of survival (Figure 2) in hemodynamically stable and unstable patients was better with thrombolysis (92.4% and 81.5%, respectively) than with surgery (86.9% and 70.4%, respectively) or anticoagulation (71.8% and 47.7%, respectively).
Univariate and multivariate logistic regression models of survival.
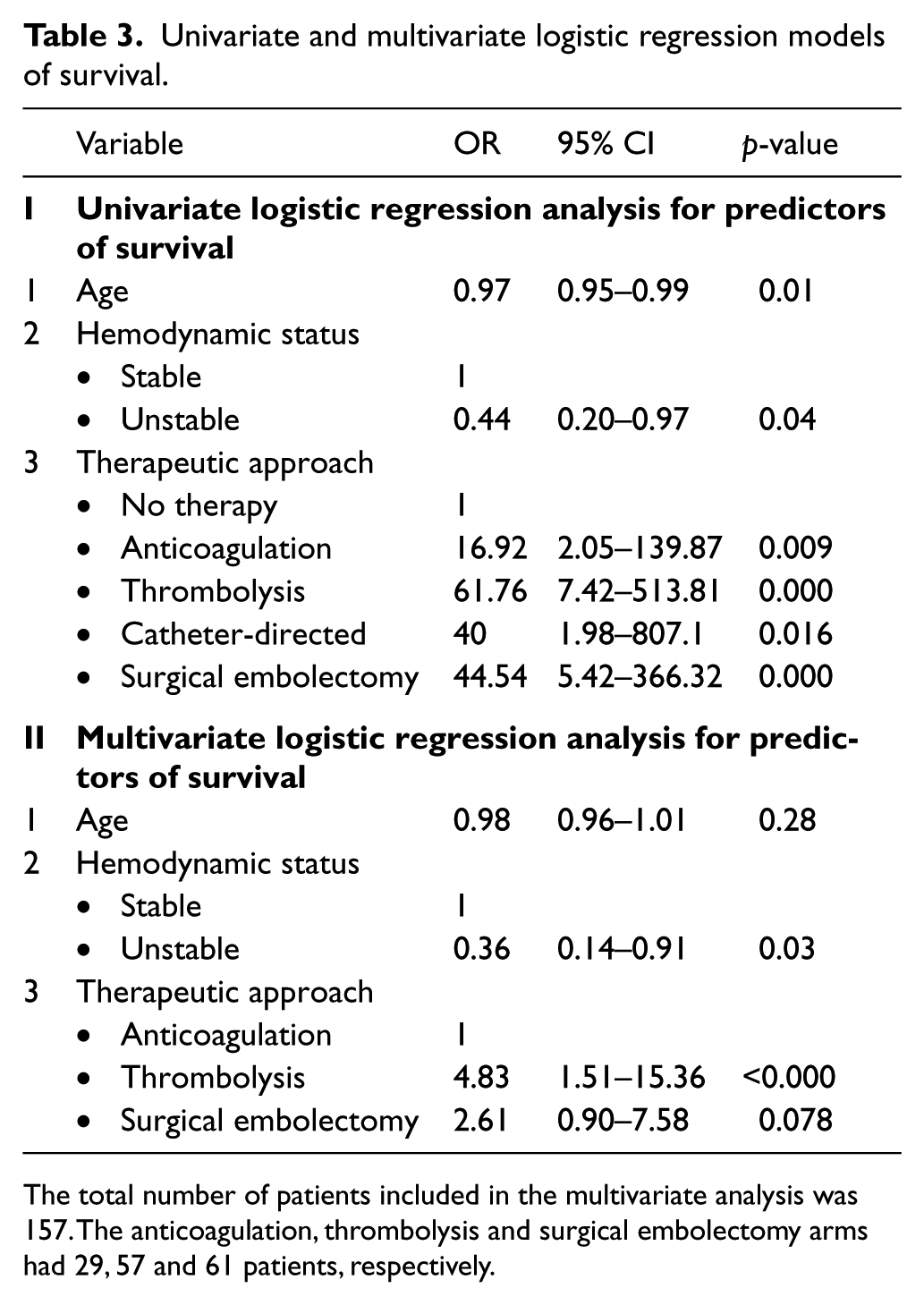
The total number of patients included in the multivariate analysis was 157. The anticoagulation, thrombolysis and surgical embolectomy arms had 29, 57 and 61 patients, respectively.
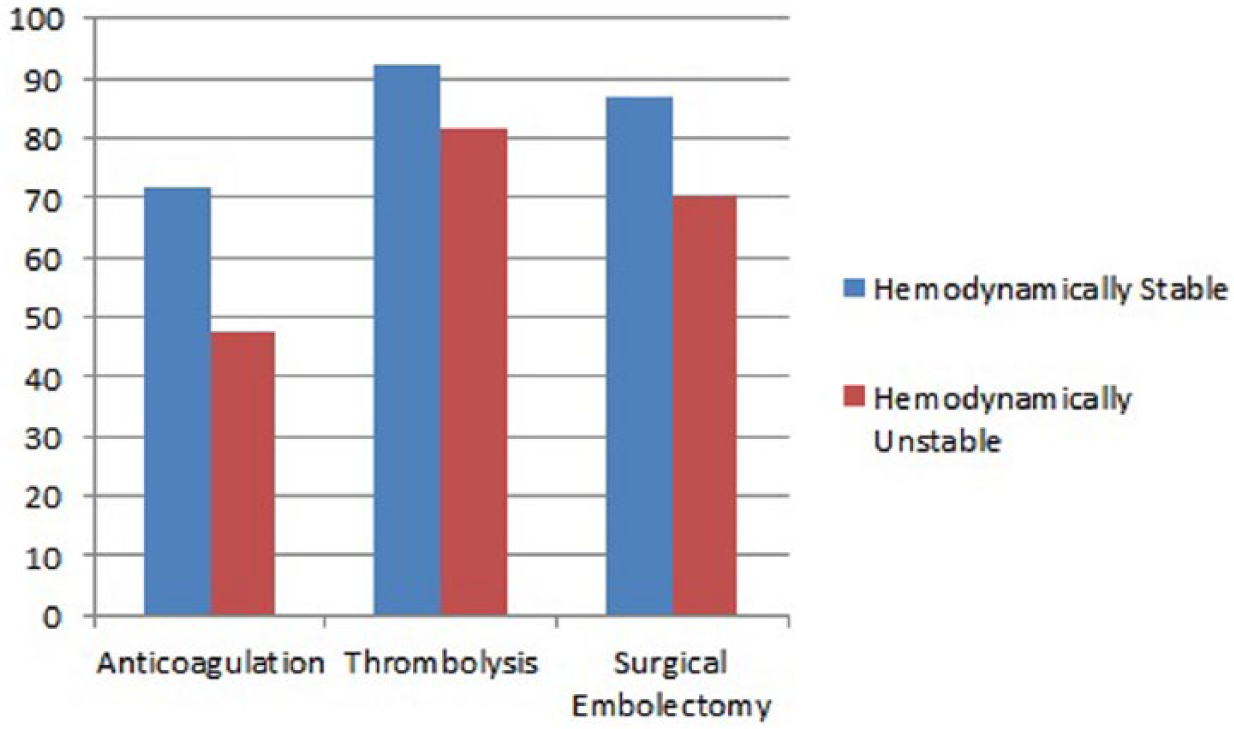
Probability of survival for each treatment type with and without hemodynamic instability using the logistic regression model.
To compare thrombolysis with surgical embolectomy we performed a subgroup analysis of patients who underwent surgical embolectomy or thrombolysis and had available data on age and hemodynamic status. This analysis was performed in 116 patients. The OR for survival in the thrombolytic arm was not significantly higher than that in the surgical arm: 1.78 (95% CI 0.55–5.64). The complications that were observed in the 242 patients treated by either strategy (thrombolysis or surgical embolectomy) are shown in Supplemental Table 2. In patients treated with thrombolysis, major bleeding requiring blood transfusion and intracranial bleed occurred in one patient each. Transient episodes of hypotension, hypoxia and hemodynamic deterioration during thrombolytic infusion occurred in five patients. One of these patients required brief cardiopulmonary resuscitation, while the others improved with continuation of the thrombolytic agent without cessation of thrombolytic therapy. Minor bleeding occurred in three patients, requiring no specific therapy. In patients undergoing surgical embolectomy, the notable complications were difficulty to wean from cardiopulmonary bypass in four patients, three of whom did not survive, stroke in two patients, recurrent PE in three patients, pulseless electric activity in one patient and acute respiratory distress syndrome in one patient. The occurrence of any complication (major or minor) was 10% with use of thrombolytics and 13.2% with surgical embolectomy. The complication rate from either procedure was less that the mortality observed when treated with anticoagulation alone (37.1%).
We compared the treatment trends over four time periods (1992–1996, 1997–2001, 2002–2006 and 2007–2013). There was a steady rise in the use of thrombolysis, with no increased short-term mortality from 1992 to 2006. However, during the period 2007 to 2013 thrombolysis was less frequently used than surgical embolectomy, again with no difference in mortality.
Discussion
Our study was conceived with the intention to address the gap in knowledge concerning the treatment of RHT. To date, this is the largest sampling of data given that the presence of RHT is an uncommon association in the setting of the frequent presentation of pulmonary embolus. Our analysis of 328 patients demonstrates that patients with RHT have a very high mortality if left untreated. The treatment strategy and hemodynamic status of the patient are the only major predictors of survival in this group. Similar to no treatment, anticoagulation has a high failure rate, delaying appropriate therapies and with increased mortality when compared to thrombolysis or surgical embolectomy. Thrombolysis and surgical embolectomy are both effective strategies, with a slightly increased probability of survival with thrombolysis.
Multiple earlier reports on consecutive cases have indicated that any one of the treatment choices (anticoagulation or thrombolysis or surgical embolectomy) may be effective in patients with RHT.5,6,12 –14 They have, however, been plagued by selection bias, small numbers and a lack of comparable groups. To compound the situation further, the only three prior meta-analyses of over 50 patients have also suggested differing treatment recommendations.1 –3 In an analysis of 119 patients from 1966 to 1989, Kinney and Wright 2 demonstrated a slightly increased survival with anticoagulation (70%) when compared to surgical embolectomy or thrombolysis (62%). However, in this group not all patients had PE and the representation of each therapy was unclear. The authors noted that for all treatments prognosis was worse if pulmonary emboli were present. In the same year (1989), the European Working Group on Echocardiography reported their experience in a total of 119 patients across 30 European centers from 10 countries. 1 Information was collected by a mailed questionnaire. They reported a lower observed mortality with surgical embolectomy (27%) when compared to anticoagulation (>60%). Thrombolysis was not evaluated in their report because only a few cases received it. In 2002, Rose et al. 3 performed the first pooled analysis of over 50 patients with RHT. They analyzed 177 patients with RHT from 1966 to 2000 in whom age, sex, therapy and outcome were reported. They demonstrated a superiority of thrombolytic therapy over surgical embolectomy (OR for mortality: 2.83, 95% CI 1.04–7.69) and anticoagulation (OR for mortality: 3.03, 95% CI 1.02–3.125). They were, however, unable to adjust for other important confounding factors (clinical and echocardiographic variables) and reasons for treatment choice. In our analysis of 328 patients, we included only patients with RHT, we did not include patients who had contraindications to either therapy and all three treatments were uniformly represented. To achieve a more accurate comparison of efficacy we performed a multivariate logistic regression analyses to account for baseline clinical and echocardiographic confounding variables. We therefore believe that our findings are more reliable and widely applicable to the management of these complex patients.
Patients with RHT present a therapeutic emergency even if hemodynamically stable because of their possible risk of circulatory collapse from further embolization into the pulmonary bed. 15 Therefore, similar to patients with massive and submassive PEs, these patients are more likely to benefit from rapid dissolution of the clot using thrombolytics than anticoagulation as the initial treatment strategy. Wan et al. 16 performed a meta-analysis of trials comparing thrombolysis to anticoagulation as the initial treatment of patients with PE. The pooled estimate showed no difference between the two treatments for recurrence of PE or mortality (OR 0.67, 95% CI 0.40–1.12). However, on subgroup analysis, thrombolysis was found to decrease recurrent PE or mortality compared with anticoagulation (9.4% vs 19.0%) in the trials that included patients with major pulmonary emboli (OR 0.45, 95% CI 0.22–0.92). The number needed to prevent one recurrent PE or death was 10. They also showed no benefit of thrombolysis over heparin in trials that excluded patients with major PE.
Similarly, Stein and Matta 17 demonstrated the benefit of thrombolysis in over 20,000 unstable patients with PE. Inhospital mortality was 15% in the thrombolysis arm as opposed to 47% in those that did not receive thrombolytics. This reduction in mortality persisted in the elderly and in patients with comorbidities. In our analysis, thrombolytics increased the probability of survival compared to anticoagulation (92.4% vs 71.8%). Also of note, 40% of patients initially started on anticoagulation had to be switched to either thrombolysis or surgical embolectomy because of clinical deterioration. We therefore recommend against anticoagulation as the initial treatment in patients with RHT.
Theoretically, surgical embolectomy is the most definitive therapy for patients with PE or RHT as it rapidly clears the clot from the right atrium, right ventricle and central pulmonary artery and restores pulmonary patency. However, it is also the most invasive with a limited availability of surgeons with expertise in this procedure. The procedure is associated with substantial mortality ranging from 11% to 64% in older literature.18,19
Current guidelines therefore recommend surgical embolectomy in patients with massive and submassive PE, with contraindications to thrombolysis. 20 Surgical embolectomy has nonetheless never been compared directly to thrombolysis and recent reports suggest a much lower mortality (<30% the mortality of untreated PE 4 ) with appropriate patient selection and timing. 21 Thrombolytic agents dissolve organized clot by targeting fibrin bonds and restore pulmonary patency. Their wide availability, ease of use and efficacy make them an ideal choice in most situations. Perhaps the greatest concern with use of thrombolytic agents in patients with RHT is the risk of dislodgement of the thrombus into the pulmonary artery with resulting massive PE and circulatory collapse and the risk of major bleeding. The risk of clot dislodgement and distal embolization with cardiovascular collapse appears to be unsubstantiated at this time. In our analysis, in 122 patients treated with thrombolysis no such complications were reported. The risk of bleeding with thrombolytics in published reports ranges from 6% to 20% and that of intracerebral hemorrhage from 0.6% to 3%.22,23 Nevertheless, in our analysis, major bleeding was seen in only one patient (intracranial hemorrhage). There is emerging evidence to suggest against withholding thrombolytic therapy in fear of complications irrespective of age or comorbid conditions. 17 In an analysis of the Nationwide Inpatient Sample database, Stein and Matta showed that among elderly (>80 years) unstable patients with PE and unstable patients with comorbidities only 53% (490/910) and 19.4% (11,670/60,100) received thrombolytic therapy, respectively. However, withholding thrombolytic therapy was not associated with improved survival. On the contrary, irrespective of age and comorbidities, mortality was lower in those who received thrombolytic therapy (18.4% versus 50% in the elderly and 6.4% versus 34% in patients with comorbidities).
The initiation of the Right Heart Thrombi European Registry (RiHTER) is currently underway and will hopefully provide prospective data on the management of this subset of patients. 24
Limitations
There are several limitations of our analysis, with few notable ones. (1) The size of our study was only 328 patients. (2) Our analysis included case series and individual case reports with no prospective studies. (3) There was incomplete reporting of important clinical and echocardiographic variables by the primary authors, limiting our analysis and comparisons between the different treatments, so we were not able to account for the missing variables in the final statistical analysis. Patients had to be moved from one treatment strategy to the other due to the need for escalating care, so some patients received two treatment strategies; for example, anticoagulation and surgical thrombectomy.
Summary
Right heart thrombi in transit are rare in patients with PE but when present identify a group with very high short-term mortality. Therapy for RHT should be individualized weighing the risks and benefits of surgery and thrombolysis. In most patients with no contraindications to thrombolytic agents, a trial of thrombolytics may be attempted prior to surgery. However, in centers with expertise in surgical embolectomy, hemodynamically unstable patients requiring inotropic support may benefit from early surgery without a trial of thrombolysis. In either case delays in treatment or an initial treatment with anticoagulation should be avoided to reduce mortality. Future well-designed randomized trials would be ideal but are unlikely because of the rarity of RHT.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.