
Abstract

Keywords
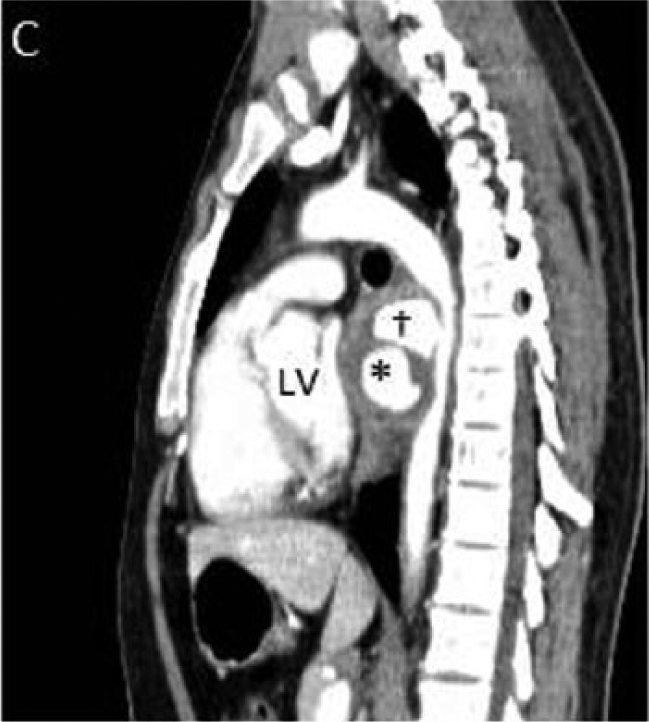
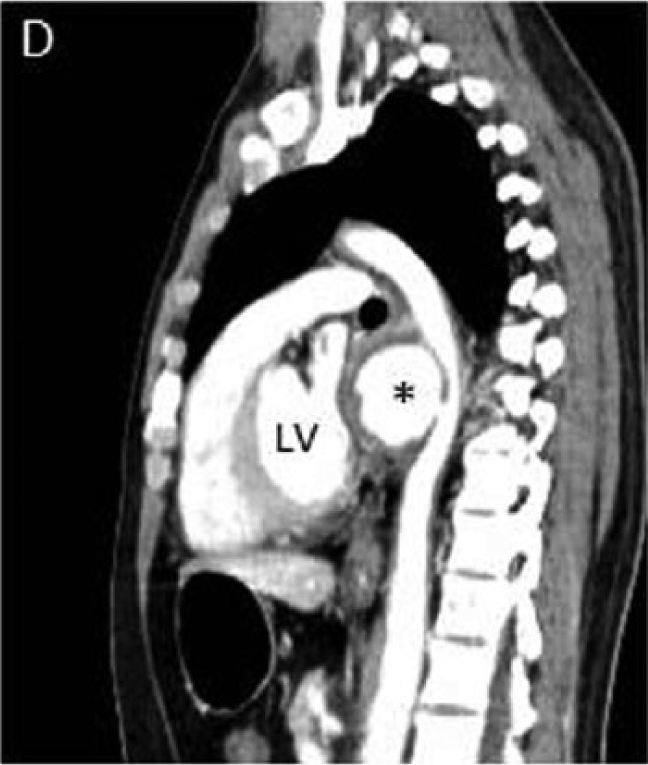
A 29-year-old man with no significant past medical history presented with progressive dysphagia for several weeks duration. The patient did not report any chest pain or shortness of breath. His physical examination was unremarkable. Upper endoscopy revealed a large extrinsic mass compressing the mid-esophagus. An electrocardiogram showed normal sinus rhythm, inferolateral Q waves and voltage criteria for left ventricular hypertrophy. Transthoracic echocardiogram revealed normal left ventricular function with a large mass compressing the left atrium (Panel A and B; indicated by arrow). Computed tomography (CT) of the chest and abdomen with iodinated contrast demonstrated two sequential descending thoracic aortic pseudoaneurysms (PSAs) with intramural thrombi (Panel C and D; indicated by cross and asterisk) compressing the left atrium (Panel E, arrow) and esophagus (Panel F, arrow). The patient underwent urgent aneurysmectomy with descending thoracic interposition graft placement. Aortic histopathology was suggestive of a non-specific chronic inflammatory process. The patient had an uneventful post-operative course and was discharged in good condition after a short hospital stay.
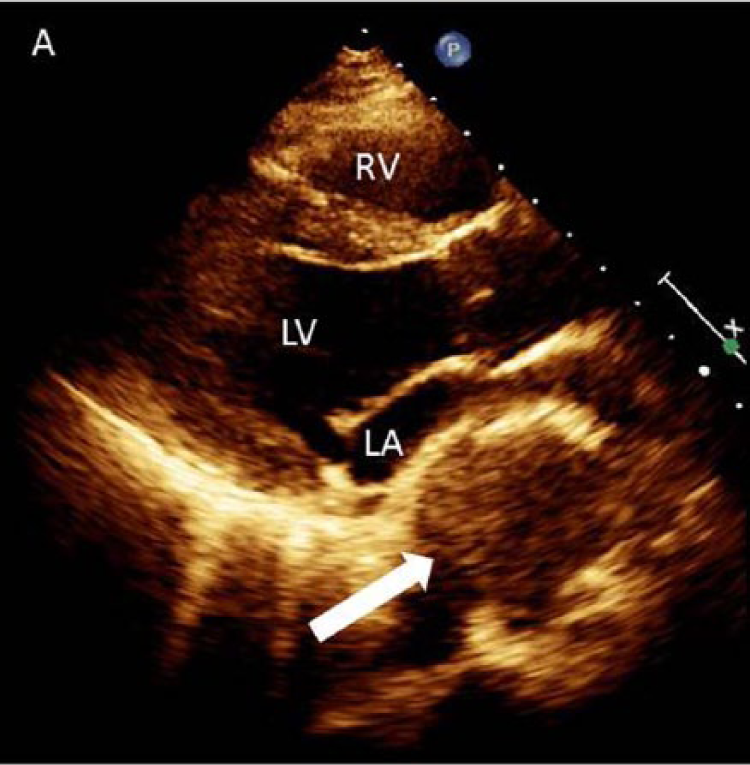
RV, right ventricle; LV, left ventricle; LA, indicates left atrium.
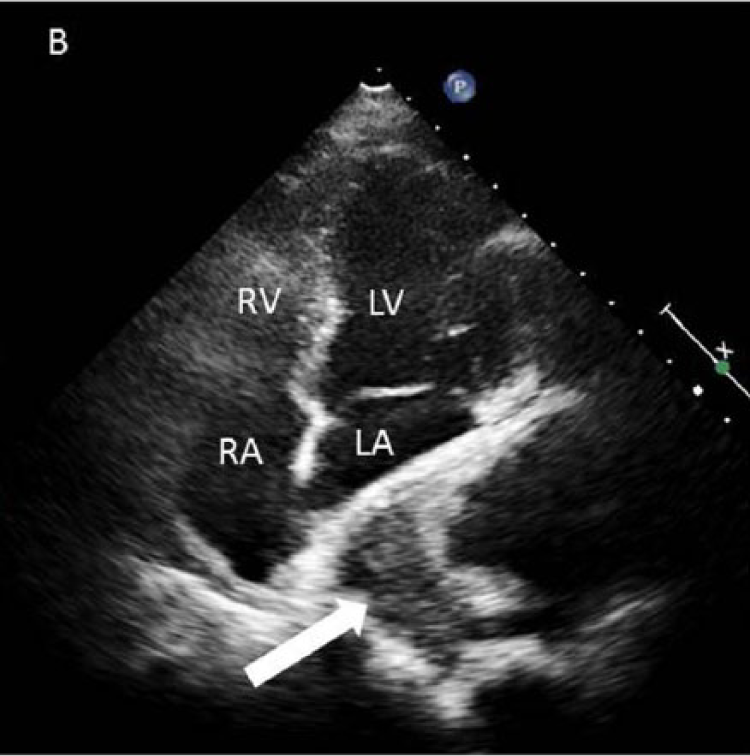
LA, indicates left atrium; LV, left ventricle; RA, right atrium; and RV, right ventricle.


Thoracic aortic PSAs are a rare manifestations of aortic disease. The majority of aortic PSAs are asymptomatic. Rarely, extrinsic compression of the esophagus from an aneurysmal segment of the aorta can cause difficult swallowing and is termed dysphagia aortica. A rare and late presentation of aortic aneurysmal disease, dysphagia aortica heralds the development of an aortoesophageal fistula, aortic rupture, and death. To our knowledge, this is the first report in the literature of multiple descending thoracic aortic pseudoaneurysms causing both symptomatic compression of the esophagus and asymptomatic compression of the left atrium.
‘Images in vascular medicine’ is a regular feature of Vascular Medicine. Readers may submit original, unpublished images related to clinical vascular medicine. Submissions may be sent to: Heather L Gornik, Editor in Chief, Vascular Medicine, via the web-based submission system at http://mc.manuscriptcentral.com/vascular-medicine
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.