
Abstract
The aim of the present study was to investigate the association of physical activity with small artery elasticity in the early stage of hypertension. We examined 366 young-to-middle-age stage 1 hypertensives (mean blood pressure 145.6±10.3/92.5±5.8 mmHg), divided into two categories of physical activity, sedentary (n=264) and non-sedentary (n=102) subjects. The augmentation index was measured using the Specaway DAT System. Small artery compliance (C2) was measured by applanation tonometry, at the radial artery, with an HDI CR2000 device. After 6 years of follow-up, arterial distensibility assessment was repeated in 151 subjects. Heart rate was lower in active than in sedentary subjects (71.2±8.9 vs 76.6±9.7 bpm, p<0.001). After adjusting for age, sex, heart rate, smoking, and blood pressure, C2 was higher (8.0±2.6 vs 6.4±3.0 ml/mmHg × 100, p=0.008) in non-sedentary than in sedentary patients. The augmentation index was smaller in the former (8.8±20.1 vs 16.8±26.5%, p=0.044) but the difference lost statistical significance after further adjustment for blood pressure. After 6 years, C2 was still higher in the non-sedentary than sedentary subjects. In addition, an improvement in the augmentation index accompanied by a decline in total peripheral resistance was found in the former. These data show that regular physical activity is associated with improved small artery elasticity in the early phase of hypertension. This association persists over time and is independent of blood pressure and heart rate.
Introduction
Assessment of arterial distensibility by means of pulse wave velocity has been included among the markers of subclinical organ damage by the 2007 ESC/ESH guidelines. 1 In the last few years, other distensibility parameters acquired importance in clinical practice as they proved to be predictive of increased risk of cardiovascular morbidity and mortality.2–5 Among these, parameters determined by diastolic pulse contour wave analysis have attracted the interest of the investigators because they provide information on the characteristics not only of large capacitance arteries but also of smaller conduit arteries.
The importance of lifestyle changes for preventing or retarding the development of hypertension and of its complications has long been known. 1 The ESC/ESH guidelines stress the importance of improving lifestyle habits before starting anti-hypertensive treatment in subjects with stage 1 hypertension and particular emphasis is put on physical activity. Regular physical activity has a beneficial effect not only on blood pressure (BP), 6 but also on body fat, waist circumference, and the metabolic profile by increasing insulin sensitivity and high-density lipoprotein (HDL)-cholesterol level. 7 Thus, exercise has the potential for retarding the stiffening process related to aging 8 and for improving arterial compliance.9–12 Among the putative beneficial effects of exercise on arterial distensibility, a decrease of sympathetic nervous system activity has also been advocated. Physical activity decreases BP, heart rate, plasma and urinary norepinephrine and the responsiveness to daily life stressors.13,14 However, it is still debated whether the sympathetically mediated beneficial effect of physical activity on arterial compliance, particularly small artery compliance, is merely due to the reduction of heart rate and BP or to a direct effect on the arterial wall.9,15–19 Regular physical activity, through a reduction of sympathetic activity, may lead to a reduction of smooth muscle tone thereby decreasing the stiffness of the muscular arteries. Increased sympathetic tone is frequently associated with hypertension in young-to-middle-age adults 20 and thus a non-pharmacological measure that reduces the sympathetic tone could have beneficial effects on the small artery elasticity of these subjects.
The aim of the present study was to investigate whether regular physical activity is associated with parameters of small artery distensibility at baseline and after a follow-up of 6 years in young-to-middle-age stage 1 hypertensive subjects.
Methods
The study participants took part in the HARVEST (Hypertension and Ambulatory Recording VEnetia STudy), a long-term prospective observational study involving 17 centers in the north east of Italy. The study was approved by the HARVEST Ethics Committee and by the Ethics Committee of the University of Padova. A written informed consent was given by the participants. The 366 subjects taking part in this subproject were all those recruited and followed up in the four HARVEST centers which agreed to participate in the arterial distensibility study: Padova (two centers), Vittorio Veneto, and San Daniele del Friuli. Patients’ recruitment was obtained with the collaboration of the local general practitioners who were instructed during local meetings. Subjects were screened for stage 1 hypertension and had never been treated for hypertension. Patients with diabetes, renal impairment, cardiac failure or coronary heart disease were excluded. Secondary forms of hypertension were excluded on the basis of complete history, physical examination and routine diagnostic procedures.
At enrollment, patients underwent physical examination, blood chemistry and urine analysis. Baseline data also included medical and family history and a questionnaire about physical activity, current use of cigarettes, alcoholic beverages and coffee use.18,21,22 The physical activity level was determined using the previously published criteria. 18 Briefly, activities were classified on the basis of relative intensity, adapting the activity intensity codes established and validated by the Minnesota Heart Survey. 23 Subjects were defined as sedentary if they did not regularly perform any physical activity; they were defined as mild exercisers if they performed leisure-time physical activities, such as walking, gardening, yard working, etc; and as exercisers if they performed sports such as running, jogging, cycling, swimming, soccer, tennis, etc, at least once a week during the previous 2 months. Within the exercisers, the subjects performing competitive sports (competitive athletes) were separated from those not involved in competition (amateurs). However, as we had only a few subjects in the sports categories, for the present analysis all active subjects were grouped into one category (non-sedentary, n=102) and were compared with the sedentary subjects (n=264).
Baseline BP was the mean of six readings obtained during two visits performed 2 weeks apart. At the enrollment, patients also underwent 24-hour BP monitoring using the A&D TM2420 model 7 (A&D, Tokyo, Japan) or ICR Spacelabs 90207 monitor (Spacelabs, Redmond, WA, USA) devices. Both of these devices were previously validated and were shown to provide comparable results. 24
Arterial distensibility assessment
The augmentation index (AIx) was recorded with applanation tonometry of the carotid and radial arteries, using the DAT System (SN1002-960604-12; Specaway, Sydney, Australia). After acquiring 30 sequential waveforms, a software system, which incorporated a validated transfer function, was used to generate an average peripheral and corresponding ascending aortic pressure waveform. 25 The device provides the AIx as the ratio of the difference between the pressure at the second systolic shoulder and diastolic blood pressure (DBP) to that between DBP and pressure at the first inflection point: AIx=100*(P2 – DBP)/(P1 – DBP). Although numerically different values are obtained, a one-to-one mapping occurs between the two definitions (carotid and radial) of AIx and both provide a quantitative expression of the pressure wave contour, 26 giving equivalent information. 27 For the present analysis, AIx derived from the radial artery was considered.
Arterial compliance was measured by arterial pulse waveform analysis using the HDI/Pulse WaveTM CR2000 (Hypertension Diagnostics, Inc., Eagan, NY, USA). 28 This technique involves a 30-second non-invasive recording of radial artery waveforms by applanation tonometry. The tonometry unit contained an array of pressure transducers capable of measuring the relative intra-arterial pulse-amplitude with high accuracy. The tonometer was centered over the radial artery obtaining the optimal waveform by pneumatical stabilization. Brachial BP was oscillometrically measured in the opposite arm. A beat-marking algorithm determined the beginning of the systole, peak systole, onset of diastole and end-diastole for each beat during the measurement period. To obtain arterial compliance, a model was used that divides the total systemic arterial compliance into large artery (or capacitive, C1) and small artery (or oscillatory, C2) compliance. 28 Cardiac output (CO) and stroke volume (SV) were determined from the arterial pressure waveforms using a specific algorithm validated with invasive studies. 28 Total peripheral resistance was expressed as the ratio of mean arterial pressure to CO. The reproducibility of these indexes during the same session and after 4 months was assessed in 72 subjects, as previously described. 29
Follow-up
Follow-up data were available in 151 subjects for C1 and C2 measurement (111 males and 40 females) and in 138 subjects for AIx (99 males and 39 females). Follow-up visits were scheduled after 1, 2, 3 and 6 months and thereafter at 6-month intervals. Subjects were followed until they developed sustained hypertension requiring anti-hypertensive treatment, according to the criteria for young subjects at low cardiovascular risk available at the time of patients’ assessment. 22 If at follow-up visits, occurring at least after ≥6 months of implementation of non-pharmacological measures, the BP level was above the operational threshold level, the patient was rescheduled for a visit within 2–4 weeks and the average BP was calculated. If BP was still above the limit, the patient reached the end-point and was given anti-hypertensive treatment; otherwise he or she was checked at monthly intervals. Thus, only patients whose BP remained permanently elevated during the observation period were finally treated. The second arterial distensibility assessment was scheduled for after 6.0 ± 1.0 years from baseline evaluation, irrespective of whether the patient was treated or remained untreated. The median follow-up time for the 151 subjects who completed the follow-up was 6.0 years (interquartile range: 4.7–6.6 years). Other details on follow-up procedures in the HARVEST were reported elsewhere.18,21,22
Data analysis
Data are presented as mean ± standard deviation (SD) unless specified. Correlations were tested with Pearson’s correlation test. Independent predictors of arterial distensibility indexes were included in multiple regression analyses with the distensibility index as the dependent variable and risk factors measured at baseline as the independent variables. Between-group differences were assessed by one-way ANCOVA analysis, adjusting for age and sex. When comparing elasticity indices, systolic and diastolic BPs, heart rate and smoking were also included in the ANCOVA models because these clinical variables have been shown to affect arterial distensibility.25,28,29 The significance of differences in categorical variables was assessed with the χ2 test. Longitudinal changes in arterial distensibility parameters were examined by a one-way repeated measure ANCOVA analysis, adjusting for the above confounders and also for parental hypertension, body mass index (BMI), presence/absence of anti-hypertensive treatment, and time elapsed between first and second measurement. A two-tailed probability value <0.05 was considered significant. All analyses were performed using SYSTAT version 12 (SPAA Inc., Evanston, IL, USA).
Results
Participants were 366 subjects (72.9% men and 27.1% women) with a mean age of 31.7±8.5 years and a BMI of 24.9±3.4 kg/m2. Their screening mean office BP was 145.6±10.3/92.5±5.8 mmHg.
The baseline characteristics of the study population, divided according to physical activity status are reported in Table 1. Non-sedentary patients were younger, more frequently male and had a better metabolic profile compared to sedentary ones. Baseline office and ambulatory BP values in the two groups are reported in Table 2. No significant difference was observed between the two groups for both office and ambulatory BPs, while office and ambulatory heart rates were significantly lower in the non-sedentary than in the sedentary patients. In ANCOVA models, including age, sex, and smoking, non-sedentary participants presented higher stroke volume and C2, and lower AIx compared to sedentary ones (Table 3). After inclusion of heart rate in the models, the differences in C1 and total peripheral resistance attained the level of statistical significance. However, when systolic blood pressure (SBP) and DBP were accounted for, only the between-group difference in C2 remained statistically significant.
Baseline characteristics of the study group divided into two subgroups of sedentary and non-sedentary individuals.
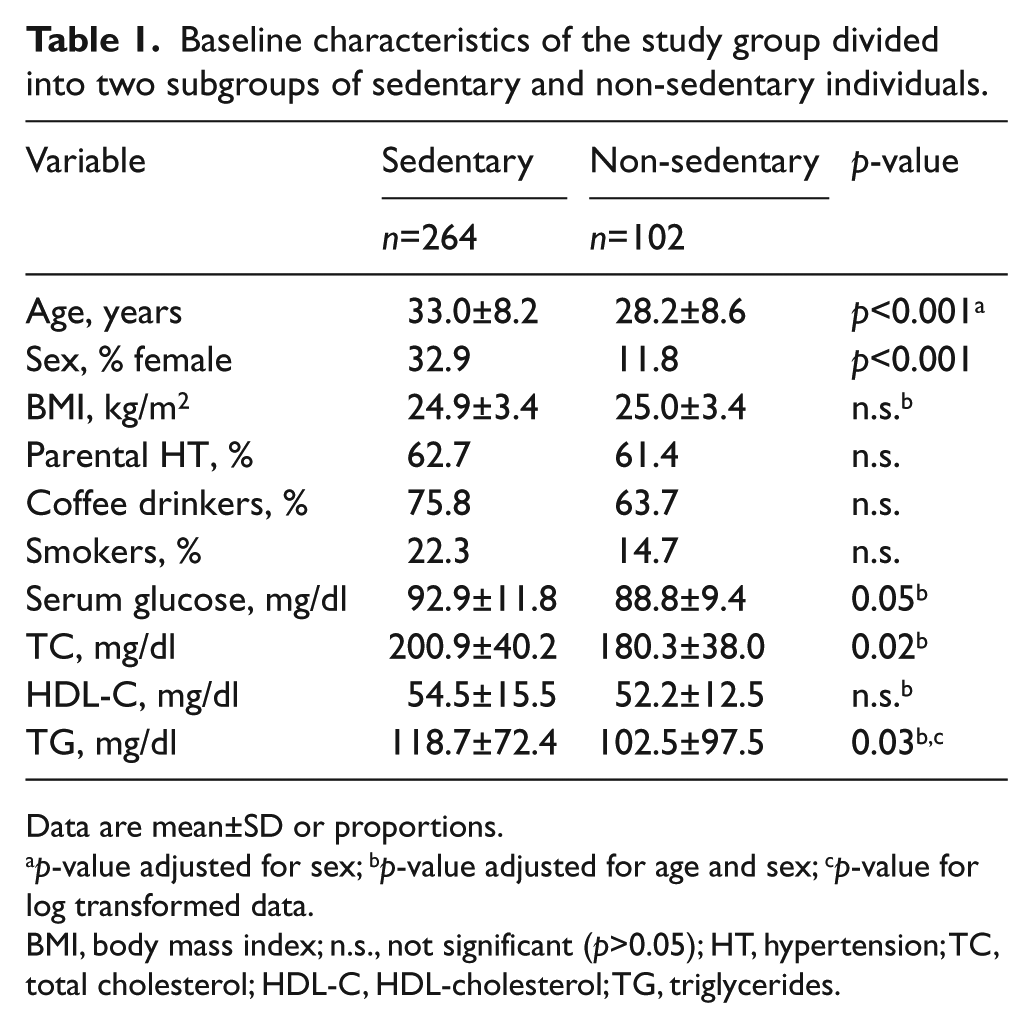
Data are mean±SD or proportions.
p-value adjusted for sex; bp-value adjusted for age and sex; cp-value for log transformed data.
BMI, body mass index; n.s., not significant (p>0.05); HT, hypertension; TC, total cholesterol; HDL-C, HDL-cholesterol; TG, triglycerides.
Baseline blood pressures and heart rates in sedentary and non-sedentary individuals.
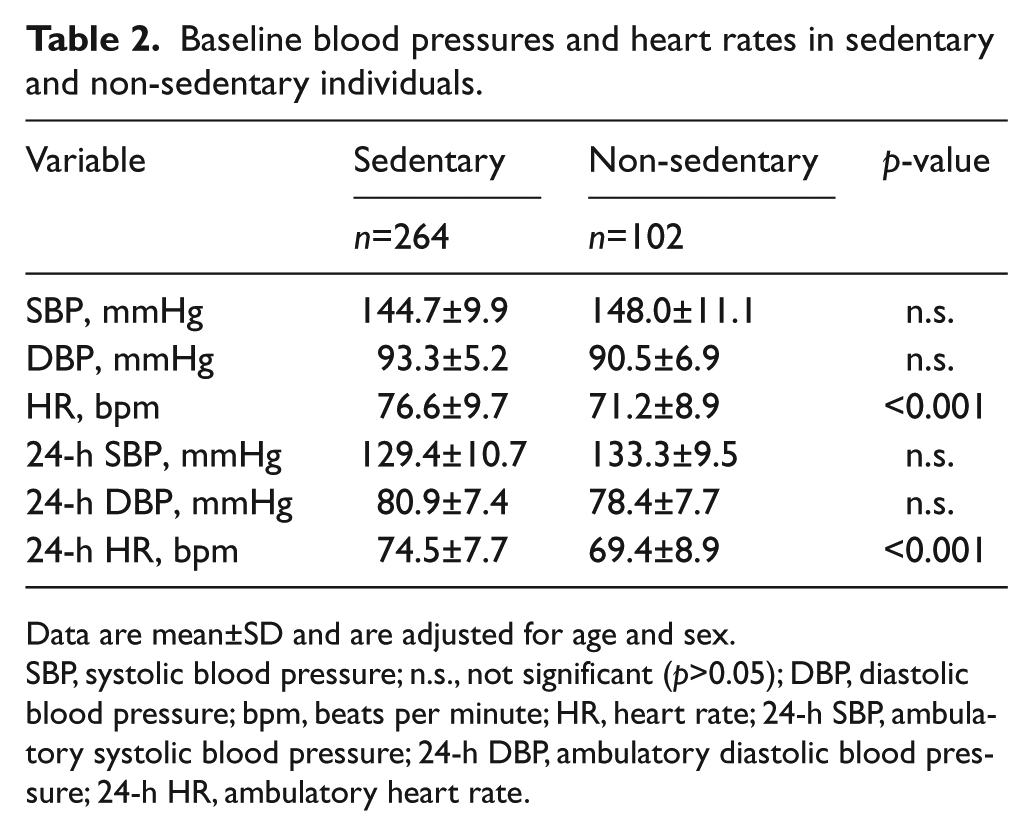
Data are mean±SD and are adjusted for age and sex.
SBP, systolic blood pressure; n.s., not significant (p>0.05); DBP, diastolic blood pressure; bpm, beats per minute; HR, heart rate; 24-h SBP, ambulatory systolic blood pressure; 24-h DBP, ambulatory diastolic blood pressure; 24-h HR, ambulatory heart rate.
Hemodynamic and distensibility parameters in sedentary and non-sedentary individuals.

Data are mean±SD.
n. s., not significant (p>0.05); C1, large artery compliance; C2, small artery compliance.
Adjusted for age, sex, and smoking.
Adjusted for age, sex, smoking, and heart rate.
Adjusted for age, sex, smoking, heart rate, and systolic and diastolic blood pressures.
AIx was negatively correlated with C2 (r=−0.51, p<0.001) and C1 (r=−0.29, p<0.001). In a multivariable linear regression analysis including age, sex, SBP, DBP, heart rate and smoking, the AIx was a negative independent predictor of C2 (p<0.001) and to a smaller extent of C1 (p=0.045)
Follow-up
The 151 subjects with follow-up data were slightly older (32.7±8.4 versus 30.9±8.6 years, p=0.051) and leaner (24.5±3.2 versus 25.2±3.4 kg/m2, p=0.048) than the rest of the group. No differences in sex distribution, parental hypertension, lifestyle factors, metabolic data, and clinic and 24-hour BPs and heart rates were found between the two groups (data not shown). Also, baseline SV, CO, total peripheral resistance, C1, C2, and AIx were similar in the two groups (data not shown).
Among the patients who had follow-up data, we observed a higher incidence of hypertension needing treatment among the sedentary patients (59.1%) compared to the non-sedentary ones (42.2%) (χ2=8.5, p=0.003). In addition, 24-hour DBP at study end was significantly lower in the non-sedentary than the sedentary individuals (81.2±7.0 versus 83.8±7.5 mmHg, age- and sex-adjusted, p=0.017). Ambulatory SBP did not differ between the two groups (131.9±10.6 versus 132.5±9.4 mmHg, p=n.s.).
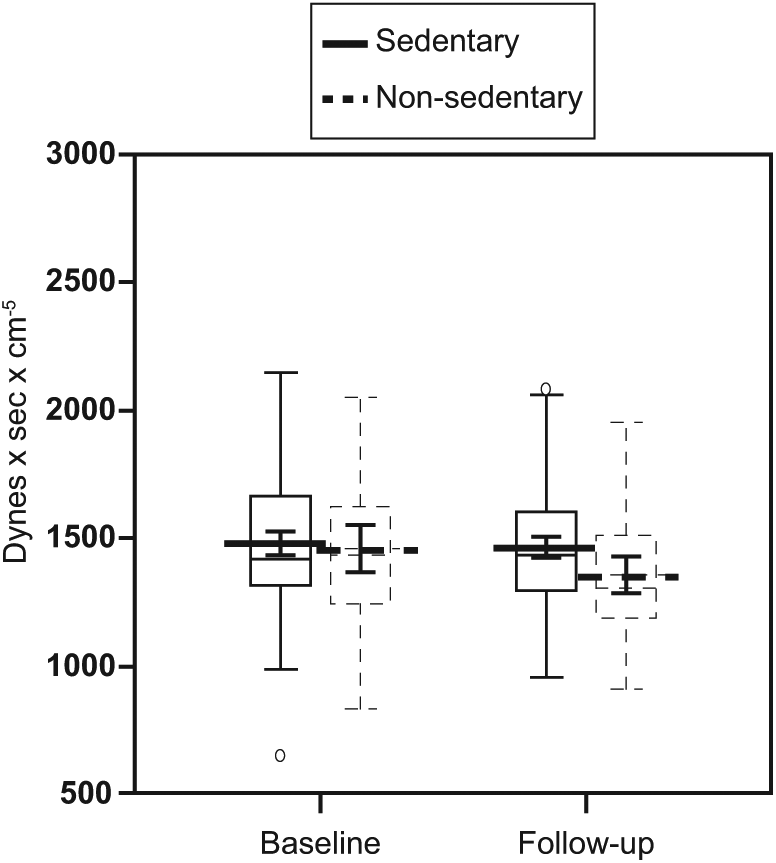
C2 and AIx showed a divergent trend in the two groups during the follow-up. C2 increased by 0.69±0.39 ml/mmHg × 100 (mean±SEM) in the non-sedentary subjects and decreased by 0.28±0.23 ml/mmHg × 100 in the sedentary ones (adjusted p=0.040). In a linear regression model including age, sex, smoking, BMI, SBP, DBP, lifestyle factors, parental hypertension, follow-up time, anti-hypertensive treatment, and baseline C2, physical activity status was a significant predictor of follow-up changes in C2 (p=0.034). The follow-up changes in AIx were −2.04±2.95% and 5.16±1.73%, respectively, for the non-sedentary and the sedentary subjects (adjusted p=0.019). Changes in arterial distensibility parameters in the non-sedentary and sedentary groups were also analyzed with a one-way repeated measure ANCOVA. The difference in C2 present at baseline increased at the end of the study (Figure 1), though there was no significant group × time interaction. For AIx, a group × time interaction reflecting the opposite changes in the two groups during the follow-up was found (Figure 2). No significant between-group differences were observed for the follow-up changes in C1 (data not shown). An inverse correlation with AIx was found for both C2 (r=−0.48, p<0.001) and C1 (r=−041, p<0.001) at follow-up measurements. These relationships remained significant also in multiple regression models (p<0.001 for both).
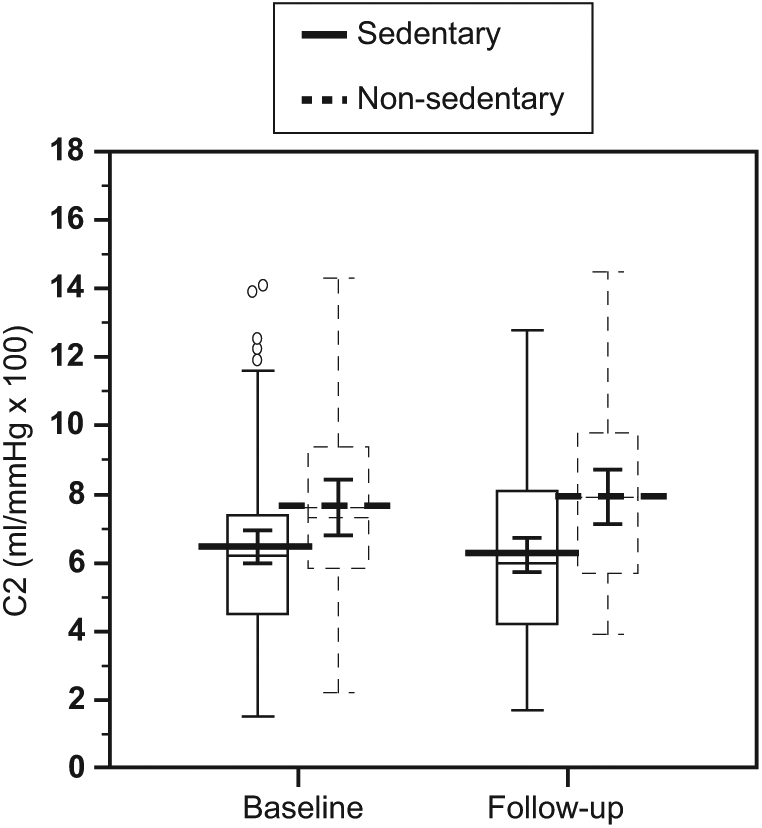
Box-and-whisker plots for small artery compliance at baseline and after 6 years of follow-up in 151 subjects. Results of one-way repeated measure ANCOVA analysis. The central box represents the values from the lower to upper quartile (25 to 75 percentile). The middle line represents the median. The horizontal line extends from the minimum to the maximum value, excluding ‘far out’ values which are displayed as separate points. The p-value for sedentary versus non-sedentary subjects = 0.011; p-value for baseline versus follow-up = n.s.; p-value for interaction = n.s. The p-values are adjusted for age, sex, BMI, SBP, DBP, lifestyle habits, parental hypertension, presence/absence of anti-hypertensive therapy, and time elapsed from first to second measurement. C2, small artery compliance.
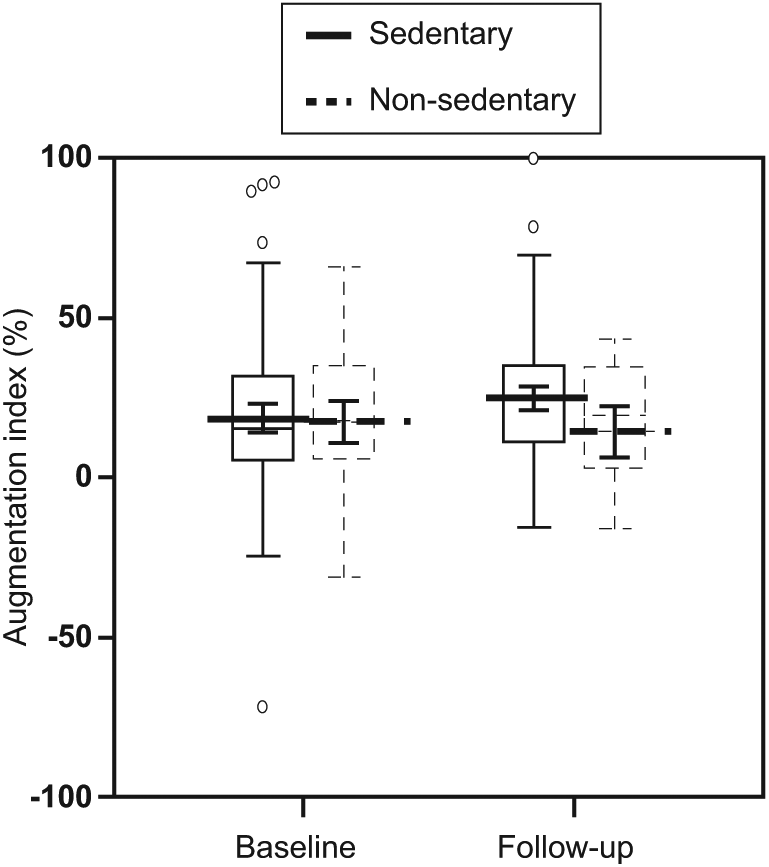
Box-and-whisker plots for the augmentation index at baseline and after 6 years of follow-up in 138 subjects. Results of one-way repeated measure ANCOVA analysis. The central box represents the values from the lower to upper quartile (25 to 75 percentile). The middle line represents the median. The horizontal line extends from the minimum to the maximum value, excluding ‘far out’ values which are displayed as separate points. The p-value for sedentary versus non-sedentary subjects = n.s.; p-value for baseline versus follow-up = n.s.; p-value for interaction = 0.017. The p-values are adjusted for age, sex, BMI, SBP, DBP, lifestyle habits, parental hypertension, presence/absence of anti-hypertensive therapy, and time elapsed from first to second measurement.
At follow-up end, a decrease in total peripheral resistance was observed in both groups. However, the fall was higher in the non-sedentary than in the sedentary patients, with a borderline significant interaction between the physical activity group and time on peripheral resistance (Figure 3).
Box-and-whisker plots for total peripheral resistance at baseline and after 6 years of follow-up in 151 subjects. Results of one-way repeated measure ANCOVA analysis. The central box represents the values from the lower to upper quartile (25 to 75 percentile). The middle line represents the median. The horizontal line extends from the minimum to the maximum value, excluding ‘far out’ values which are displayed as separate points. The p-value for sedentary versus non-sedentary subjects = n.s.; p-value for baseline versus follow-up = n.s.; p-value for interaction = 0.056. The p-values are adjusted for age, sex, BMI, SBP, DBP, lifestyle habits, parental hypertension, presence/absence of anti-hypertensive therapy, and time elapsed from first to second measurement.
In all ANCOVA models, inclusion of heart rate only marginally affected the levels of statistical significance.
Discussion
The main finding of this study is that regular physical activity in young-to-middle-age subjects screened for stage 1 hypertension was accompanied by an increase in small artery distensibility, as indicated by the higher C2 and the lower AIx in the non-sedentary individuals compared to the sedentary subjects. Inclusion of heart rate in the models only marginally affected the results. When BP was also incorporated the between-group difference lost the statistical significance for AIx. The between-group differences present at baseline further increased after 6 years of observation. The longitudinal association of physical activity with C2 and AIx was independent of the effect of heart rate and BP on arterial distensibility parameters. In addition, our data confirmed the association of regular exercise with large artery compliance.9–12
Most results on the effect of aerobic exercise on arterial distensibility were obtained in adult to elderly individuals, showing that physical activity was generally associated with improved arterial elasticity. Much less is known on the effect of exercise in young individuals. Our results are in keeping with those obtained by Nettlefold et al. 19 in a cross-sectional study of 102 normotensive children. Also in that study, moderate to vigorous physical activity was associated with higher C2, whereas no data were available for the AIx. In 131 healthy individuals <40 years of age, McGavock et al. 30 found a cross-sectional association between aerobic training and both C1 and C2. In that study of normotensive subjects (mean BP in both groups <120/70 mmHg), no difference in total peripheral resistance was found according to physical activity status. Whether aerobic exercise is as effective in young adults with chronic elevations in BP is unclear. In particular, little is known on the long-term effects of regular physical activity in young hypertensive subjects. At baseline, our non-sedentary participants already had better elasticity indices than the sedentary subjects. During the 6 years of follow-up an improvement in both parameters of small artery distensibility was observed among the non-sedentary individuals, whereas a tendency to impairment was found in their sedentary counterparts.
Besides decreasing heart rate, which is a strong determinant of arterial distensibility,31–33 the reduction in sympathetic activity mediated by physical training 17 may reduce the peripheral vasoconstriction and prevent the long-term effects of sympathetic activity on the arterial wall. This was attested to by the drop in peripheral resistance and ambulatory DBP after 6 years of follow-up in our non-sedentary participants, which was consensual with the improvement in the elasticity indices. Prolonged sympathetic activation in hypertension may lead to small artery remodeling with a progressive increase in the wall/lumen ratio. 34 Physical activity can have a favorable impact on the vascular tree in hypertension, preventing the remodeling of the small arteries and promoting an increase in the cross-section of the microcirculation. 35 This may explain the reduction in vascular hyper-responsiveness seen in trained hypertensive individuals compared to sedentary hypertensives. 36 The robustness of our findings is supported by the consistent longitudinal trends of C2 and AIx, which were obtained with two different devices. As shown by our results, AIx is inversely related to the compliance of the small arteries 37 because it is based on the hemodynamic principle of pressure wave propagation and reflection, 37 giving information chiefly about small artery stiffness. 38 When BP was accounted for in our cross-sectional and longitudinal models, a slight attenuation was found for the strength of the association between physical activity status and elasticity indices. This indicates that the relationship between physical activity and arterial elasticity may be partially explained by the effect of regular exercise on BP.
Humoral factors not measured in the present study may contribute to the beneficial effect of dynamic sports activities on small artery distensibility. Maeda et al. 39 observed that young subjects, after 8 weeks of exercise, had a significant reduction in endothelin-1 and an increase in nitric oxide concentrations, with an inverse correlation between the two biochemical factors. A reduction of oxidative stress and an increased expression and activation of nitric oxide synthase 40 with enhanced endothelium-dependent dilation have been described in middle-aged endurance exercise-trained men compared to less active peers.41–43 In addition, regular physical activity may improve vascular function by protecting the arterial tree from the adverse effects of traditional risk factors for cardiovascular disease.
Limitations
One limitation of the current study is the absence of a classification of non-sedentary subjects according to different levels of physical activity due to the small number of subjects in each physical activity category. However, non-sedentary subjects were grouped together because we observed similar changes in arterial elasticity data in the non-sedentary groups. A second limitation is that physical activity habits were self-reported and could thus be inaccurate or biased. However, previous analyses of physical activity habits in the HARVEST have demonstrated that the participants were likely to have a fairly stable physical activity pattern over the years, 44 thus indicating internal consistency and a reduced opportunity for bias. A third limitation is that distensibility parameters were derived non-invasively, using a generalized transfer function. However, we assessed our subjects with two different devices that provide data based on different methodological approaches – obtaining consistent results. Another limitation is that only 151 out of the 366 subjects could complete the 6-year follow-up and have a second arterial distensibility assessment. However, their baseline arterial characteristics were similar to those of the rest of the group. Finally, the higher prevalence of male hypertensive subjects in our population limits generalizability to women.
Conclusions
In conclusion, our results show that physical activity in young hypertensive adults is associated with an increase in C2 and a reduction in AIx and total peripheral resistance, which may prevent the arterial stiffening due to aging. These associations persisted also when the effect of heart rate was accounted for and were slightly attenuated when BP was incorporated in the models. The present findings suggest that exercise causes favorable changes on the functional and structural properties of the small muscular arteries in hypertension.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The study was funded by the University of Padova, Padova, Italy and the Associazione ‘18 maggio 1370’, San Daniele del Friuli, Italy.