
Abstract
Objectives
Heavy cannabis use has been associated with the development of acute myocardial infarction and stroke. The objective of this study was to determine if heavy, chronic cannabis use is associated with the development of acute limb ischemia (ALI) or critical limb ischemia (CLI).
Methods
We conducted a retrospective cohort study within the National Inpatient Sample (2006–2015). Patients without cannabis use disorder (CUD) were matched to patients with CUD in a 2:1 ratio using propensity scores. Our primary outcomes were incidence of ALI and CLI. Secondary outcomes included incidence of acute mesenteric ischemia (AMI), chronic mesenteric ischemia (CMI), frequency of open or endovascular interventions, length of stay, and total costs. Sensitivity analyses were performed with alternative models, including in the entire unmatched cohort with regression models utilizing survey weights to account for sampling methodology.
Results
We identified a cohort of 46,297 857 unmatched patients. Patients with CUD in the unmatched cohort were younger, with less cardiovascular risk factors, but higher rates of smoking and substance abuse. The matched cohort included 824,856 patients with CUD and 1,610,497 controls. Those with CUD had a higher incidence of ALI (OR 1.20 95% CI: 1.04-1.38 P=.016). Following multiple sensitivity analyses, there was no robust association between CLI and CUD. We observed no robust association of CUD with AMI, CMI, procedures performed, frequency of amputation, costs, or total length of stay.
Conclusions
Cannabis use disorder was associated with a significantly higher incidence of admission for acute limb ischemia. CUD was not associated with an increased risk of critical limb ischemia following sensitivity analysis. Given CUD is often seen in younger, less co-morbid patients it provides an important target for intervention in this population.
Keywords
Introduction
In the past two decades, mounting evidence has accumulated demonstrating the negative impact of heavy, regular cannabis use on the coronary and cerebrovascular arterial systems.1-6 The 2016 American National Survey on Drug Use and Health recorded 4 million people (1.5% of the population) with cannabis use disorder (CUD). 7 An estimated 24 million Americans over twelve years of age used cannabis in the last month and 6% of Canadians over twelve report daily use.7,8
Cannabis use has been associated with acute myocardial infarction (MI), stroke, a thromboangitis obliterans like pathology called cannabis arteritis and complications in peripheral bypass surgery.1,4,9,10 Finally, cannabinoids play a complex role in the coagulatory cascade. Some authors have demonstrated increased platelet aggregation mediated by cannabinoid exposure.5,6 To date, there have been no large studies investigating the incidence of acute limb ischemia (ALI) or critical limb ischemia (CLI) in those with heavy cannabis use.
We therefore conducted a retrospective cohort study to investigate the association of cannabis use disorder (CUD) with episodes of (1) ALI and (2) presence of CLI. We additionally investigate rates of mesenteric ischemia, amputation, costs, and length of stay as secondary endpoints. We hypothesized that CUD would be associated with an increased rate of ALI and CLI as well as worse outcomes in those admitted for these conditions.
Methods
Dataset
We performed a retrospective cohort study utilizing the Nationwide Inpatient Sample (NIS) from 2006–2015. Due to changes from International Classification of Diseases, 9th edition (ICD-9) to ICD-10, data after October 1, 2015 was not included. The NIS is a stratified random sample of discharges from US hospitals, including 20% of all discharges that can be weighted to estimate nationally representative figures. It is therefore representative of the US inpatient population over the time period, however, does not capture out-patient data. The dataset is administered by the Agency for Healthcare Research and Quality (AHRQ) and is the largest all-payer inpatient database in the US. This study did not require review by an institutional review board because the deidentified data are publicly available.
Cohort Definition
The cohort included all discharges, excluding those with missing data elements required for propensity score and logistic regression analysis. Due to limitations in state-level reporting of race data, it is missing for 13% of patients. Therefore, an indicator variable was input for missing race classification. Individuals under 18 years of age were excluded. Those over 75 years of age were additionally excluded as CUD in this population is rare and inclusion may lead to violations in the assumption of positivity. 11
Exposure
CUD was defined by ICD-9 discharge diagnoses for cannabis dependence or abuse (‘30,430’ ’30,431’ ’30,432’ ’30,433’ ’30,520’ ’30,521’ ’30,522’ ’30,523’). Prior studies have demonstrated high specificity for illicit substance use disorders in administrative databases (>95%).12,13 Patients with a history of CUD in remission were included as well as active CUD. A sensitivity analysis was performed with CUD defined as only those with active cannabis dependence or abuse, not cannabis abuse or dependence in remission.
Outcomes
Our primary outcomes of interest include incidence of (1) ALI and (2) CLI. These were identified by ICD-9 codes, which have previously been used and validated.14-19 Patients were considered to have ALI if they had a relevant diagnosis code in the first position (4440, 44,401, 44,409, 44,422, 44,481) and were classified as a non-elective admission. All outcomes or covariates were identified by querying ICD-9 or clinical classification codes (CCS) provided by AHRQ, and are available in Supplemental Table I.
We considered three definitions of CLI. The first required a code indicating rest pain or tissue loss (44,022, 44,023, 44,024) in any position, or a primary diagnosis of peripheral arterial disease (PAD) and a code indicating tissue loss. We then repeated the analysis with alternate definitions; (2) a more restricted definition, where a CLI diagnostic code always had to be in the first position (primary diagnosis in the NIS); (3) the admission must be classified as non-elective. The purpose of these alternate definitions was to evaluate how robust the results were and evaluate for potential bias. The stricter definition leads to a reduced event rate but may be less prone to misclassification. The third definition, by targeting only non-elective admissions, aims to reduce the influence of selection bias. Patients were excluded from classification as CLI if they met criteria for ALI.
Secondary outcomes included incidence of acute mesenteric ischemia (AMI) and chronic mesenteric ischemia (CMI). The analysis for CMI, included three different definitions; (1) the CMI code in any position (2) a restricted definition, with diagnosis in the first position (3) admissions only classified as non-elective.
For those in the matched cohort with CLI and ALI, we examined rates of endovascular intervention, open intervention, amputation, length of stay, and total cost. Total charges were converted to costs using cost to charge ratios provided by Healthcare Cost and Utilization Project (H-CUP). For the CLI cohort, outcomes are presented for the definition requiring cases to be identified as non-elective, as we feel this definition has the least risk of bias (analysis with the unrestricted definition is available in Supplemental Table IV). Finally, the prevalence of diagnoses, which may be the underlying cause of ALI, were examined among those with and without CUD in the matched cohort, both overall and in those with ALI. These included non-iatrogenic trauma or other external causes of injury (identified by external cause of injury CCS codes), atrial fibrillation, aneurysm of the arteries supplying the lower extremity, history of PAD, and acute MI.
Covariates
Relevant covariates were selected based on prior literature as well as clinical sensibility and biological plausibility for association with CUD and development of lower extremity ischemia. These included substance use disorders (SUD), psychiatric disorders, smoking, obesity, hypertension, diabetes, dyslipidemia, atrial fibrillation/flutter, other conduction abnormalities, chronic kidney disease (CKD), congestive heart failure (CHF), liver disease, malignancies (solid tumor, hematologic, metastatic), rheumatoid arthritis, and inflammatory bowel disease. Cocaine and amphetamine use disorder were included independently from other SUDs. A history of prior coronary artery disease (CAD) or stroke was included in the primary model. Due to concerns that a generalized development of atherosclerotic disease may be part of the mechanism of action leading to limb ischemia, a sensitivity analysis was performed without these variables in the model.
Age was included in models as a quadratic function. Race, sex, year of admission, hospital characteristics including bed size, teaching status and urbanicity, patient income quartile, and payer status (ex. self, Medicare, Medicaid, and private insurance) were included as categorical variables. A modified Elixhauser Comorbidity Index (excluding PAD and SUD) was included as a categorical variable (0, 1, 2, and 3 or more) to allow for non-linear associations.
Statistical Analysis
For our primary analysis, we performed a propensity score match with all identified covariates of interest, identified a priori, to predict CUD. Patients with CUD were matched in a 1:2 ratio nearest neighbor match, to patients without a diagnosis of CUD, using a maximum caliper width of .2 of the standard deviation of the logit of the propensity score. 20 Standardized differences were calculated and assessed for both the initial cohort and matched groups. In order to account for residual unbalance in covariates in the matched cohort, those with a standardized difference greater than 10% after matching were further adjusted with regression procedures. 21 Length of stay was analyzed utilizing a negative binomial regression and cost with a generalized linear model assuming a gamma distribution and a log link function. Statistical analysis between groups for dichotomous variables was carried out with Fischer’s exact test.
Due to the inability to fully account for discharge weights in a propensity matched analysis a sensitivity analysis was performed. We repeated the analysis using logistic regression models utilizing appropriate survey weights to account for the sampling methodology of the NIS in the entire unmatched cohort.
Outcomes and statistical models were determined a priori. The decision to evaluate both CLI and CMI with two alternate definitions (restricted and non-elective admission) was made during the course of the analysis, to evaluate for potential bias. The sensitivity analyses conducted (1) without prior history of CAD and stroke in the model, (2) definition of CUD not including those with CUD in remission, and (3) utilizing survey specific regression procedures, were planned a. priori. All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc, Cary, North Carolina). Reported P-values are 2 sided, with a P < .05 considered statistically significant. For our primary outcomes of rates of CLI and ALI, we applied a Bonferroni correction, considering P < .025 as statistically significant. A Bonferroni correction was applied separately when considering secondary outcomes as well (P < .005).
Results
Figure 1 shows the cohort assembly. We excluded 26,800,929 (35.8%) discharges outside the target age range and 1,678,641 (2.2%) discharges for missing data, providing an unmatched, unweighted, cohort of 46,297,857 patients. After matching on our propensity score, 824,856 patients with CUD (99.8%) were successfully matched to one or two patients without a diagnosis of CUD (n = 1,610,497). Flowchart dsemonstrating cohort formation.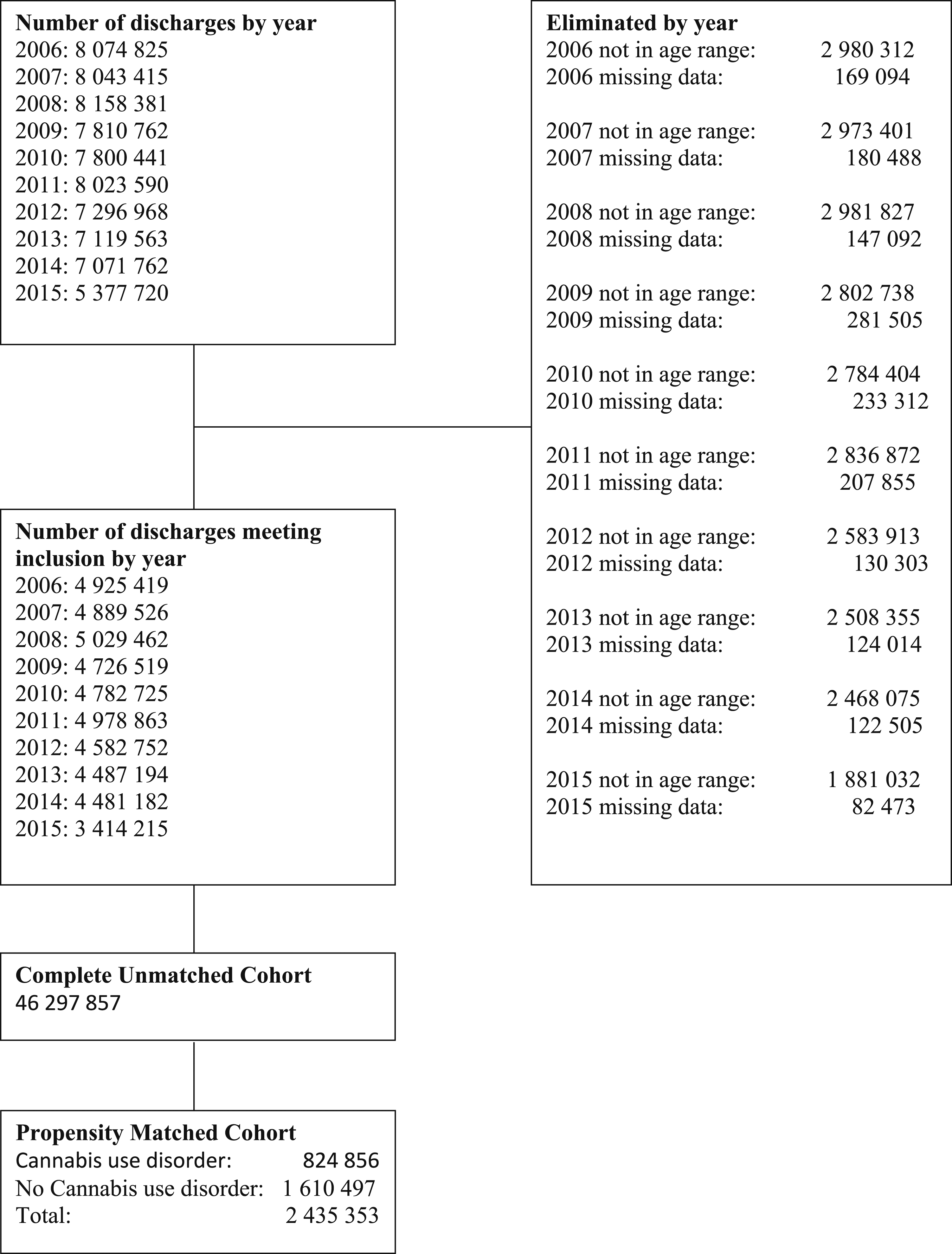
Patient Characteristics of Unmatched Cohort.
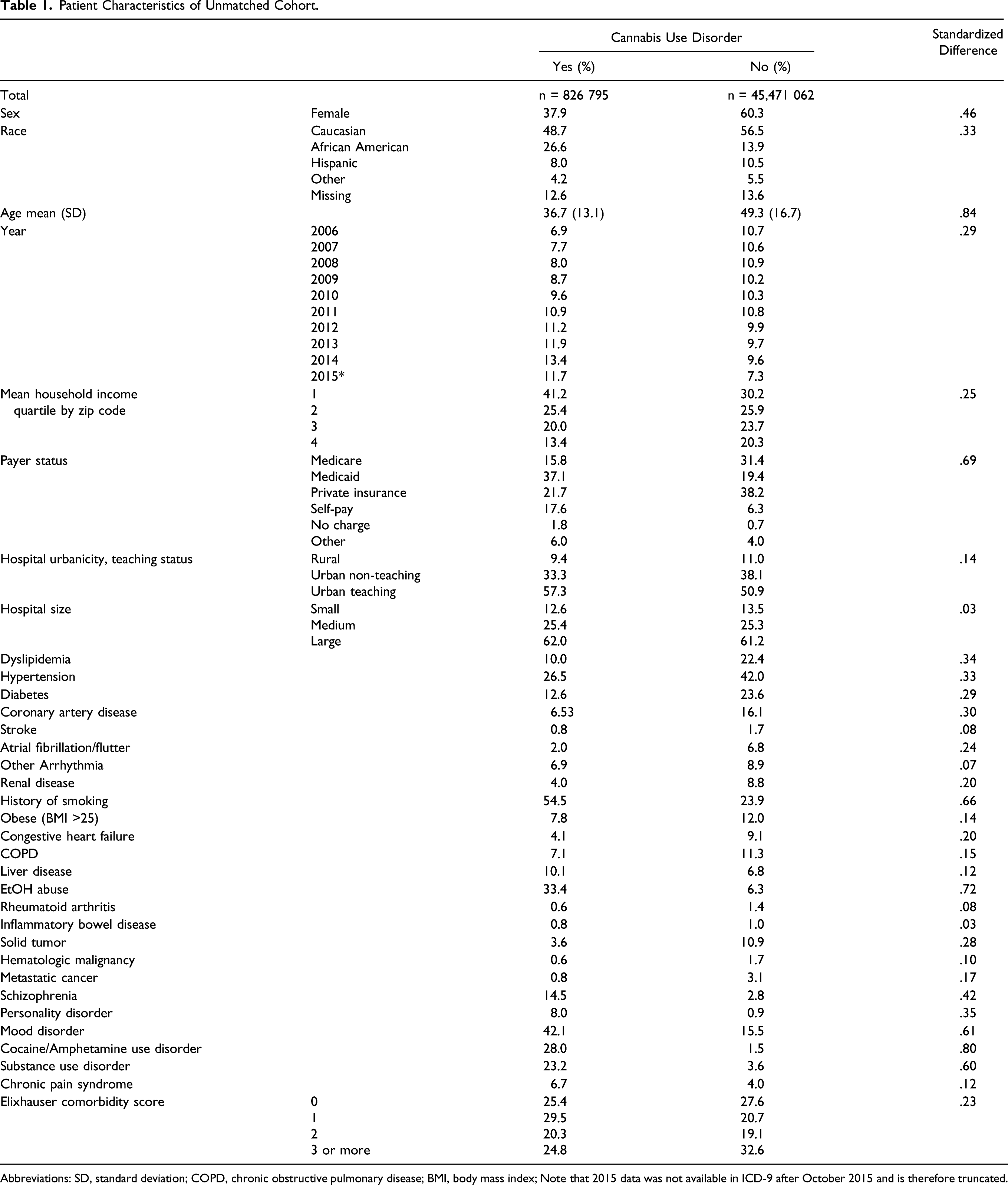
Abbreviations: SD, standard deviation; COPD, chronic obstructive pulmonary disease; BMI, body mass index; Note that 2015 data was not available in ICD-9 after October 2015 and is therefore truncated.
Patient Characteristics of Matched Cohort.
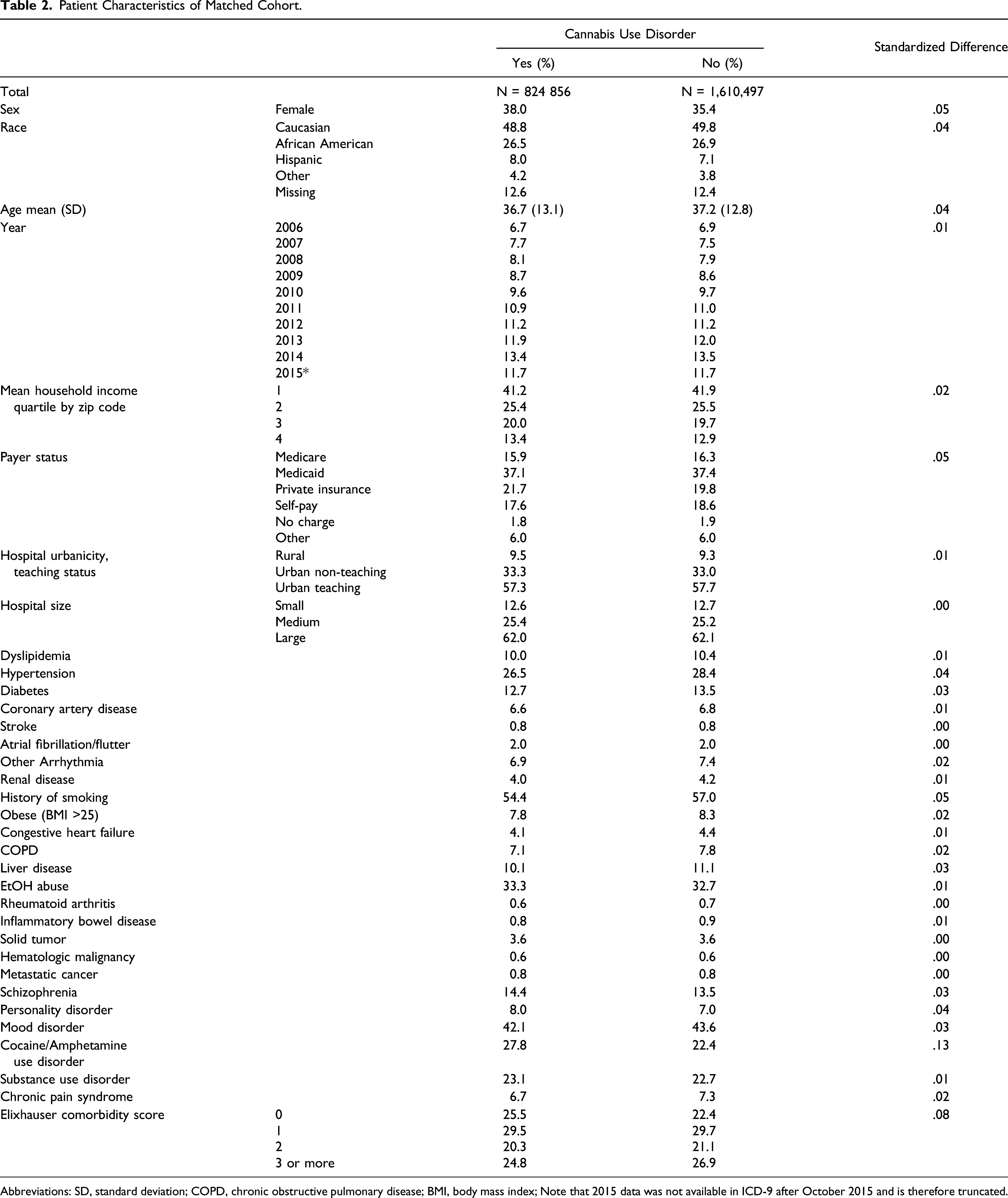
Abbreviations: SD, standard deviation; COPD, chronic obstructive pulmonary disease; BMI, body mass index; Note that 2015 data was not available in ICD-9 after October 2015 and is therefore truncated.
Association Between Cannabis Use Disorder (CUD) and Lower Extremity or Mesenteric Ischemia Among Patients in a Propensity-Matched Cohort (Nationwide Inpatient Sample, 2006–2015). Three definitions are presented for critical limb ischemia and chronic mesenteric ischemia (Supplemental Table I). The restricted definition requires a relevant diagnostic code in the first position. The urgent cases definition required the case to be coded as non-elective.
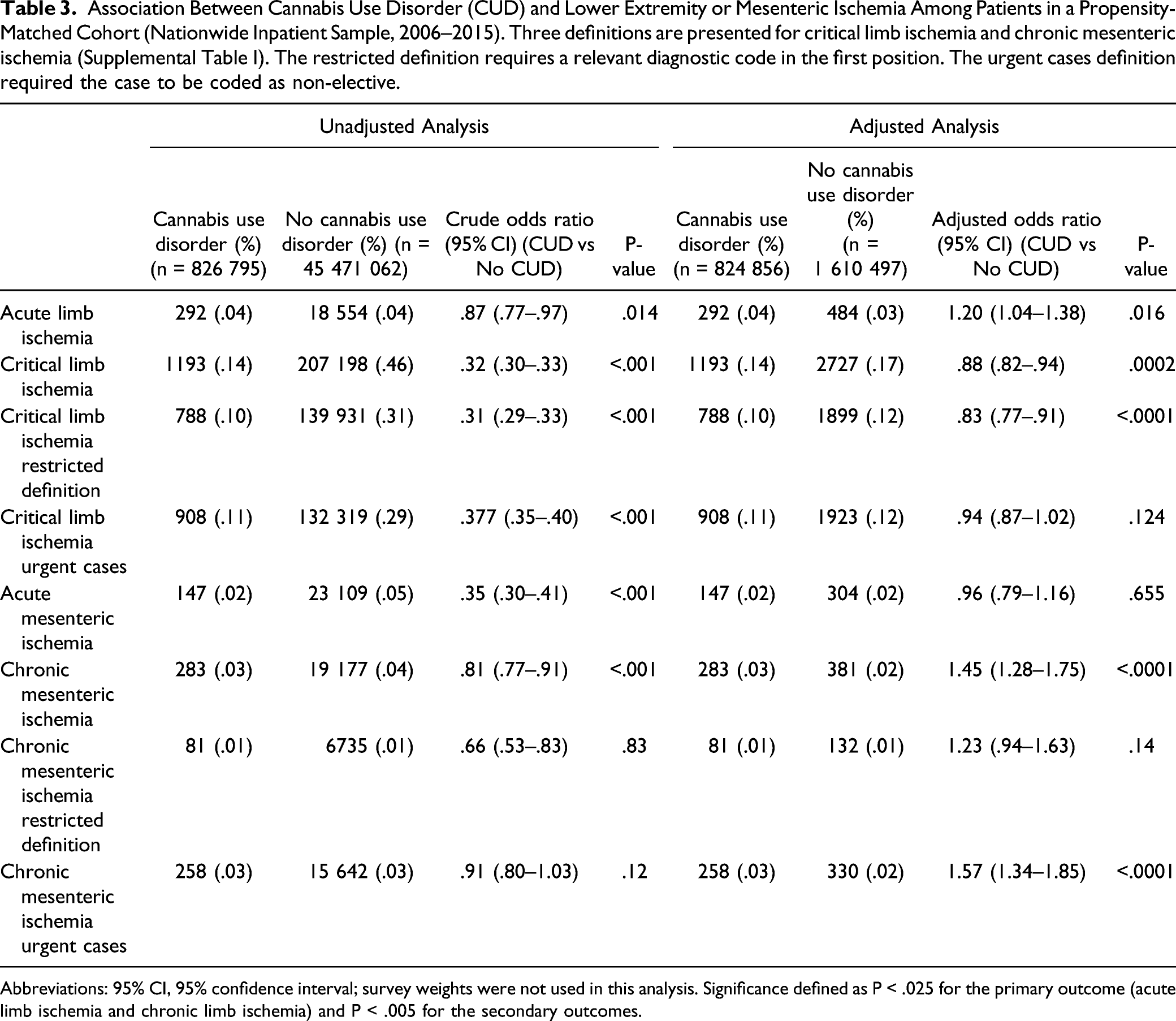
Abbreviations: 95% CI, 95% confidence interval; survey weights were not used in this analysis. Significance defined as P < .025 for the primary outcome (acute limb ischemia and chronic limb ischemia) and P < .005 for the secondary outcomes.
Initially, we completed the analysis with a definition of CLI of either (1) a diagnostic code for CLI in any position or (2) a diagnosis for lower extremity atherosclerosis in the first position with a code for tissue loss in any position. This yielded a lower incidence of CLI in those with a diagnosis of CUD (OR:0.88 95% CI:0.82-.94, P = .002). We repeated the analysis using a stricter criterion regarding the diagnostic codes (that there must always be a CLI related diagnosis in the first position) with consistent results (OR:0.83 95% CI:0.77-.9,1 P < .001). However, when requiring in the definition of CLI that the admission was non-elective, the association was non-statistically significant (OR:0.94 95% CI:0.87-1.02, P = .124). These results were consistent in the sensitivity analyses (Supplementary tables II and III).
We demonstrated no statistically significant association between CUD and AMI (OR:0.96 95% CI:0.79-1.16, P = .655). A higher incidence of CMI was observed in those with a diagnosis of CUD (OR:1.45 95% CI:1.28-1.75, P = <.0001). We performed the analysis with two alternate definitions. In the analysis requiring the diagnosis code to be in the first position this effect was in the same direction but non-significant (OR:1.23 95% CI:0.94-1.63, P = .14). When requiring cases to be non-elective, there was a significantly higher incidence of CMI in those with CUD (OR:1.57 95% CI:1.34-1.85, P = <.0001).
Analysis of Outcomes of Those with Acute Limb Ischemia in the Matched Cohort, With and Without Cannabis Use Disorder. Comparison of rates of interventions performed, cost, and length of stay in those with a diagnosis of acute limb ischemia in the matched cohort. Odds ratios are adjusted for stimulant use disorder which remained unbalanced in the matched cohort.
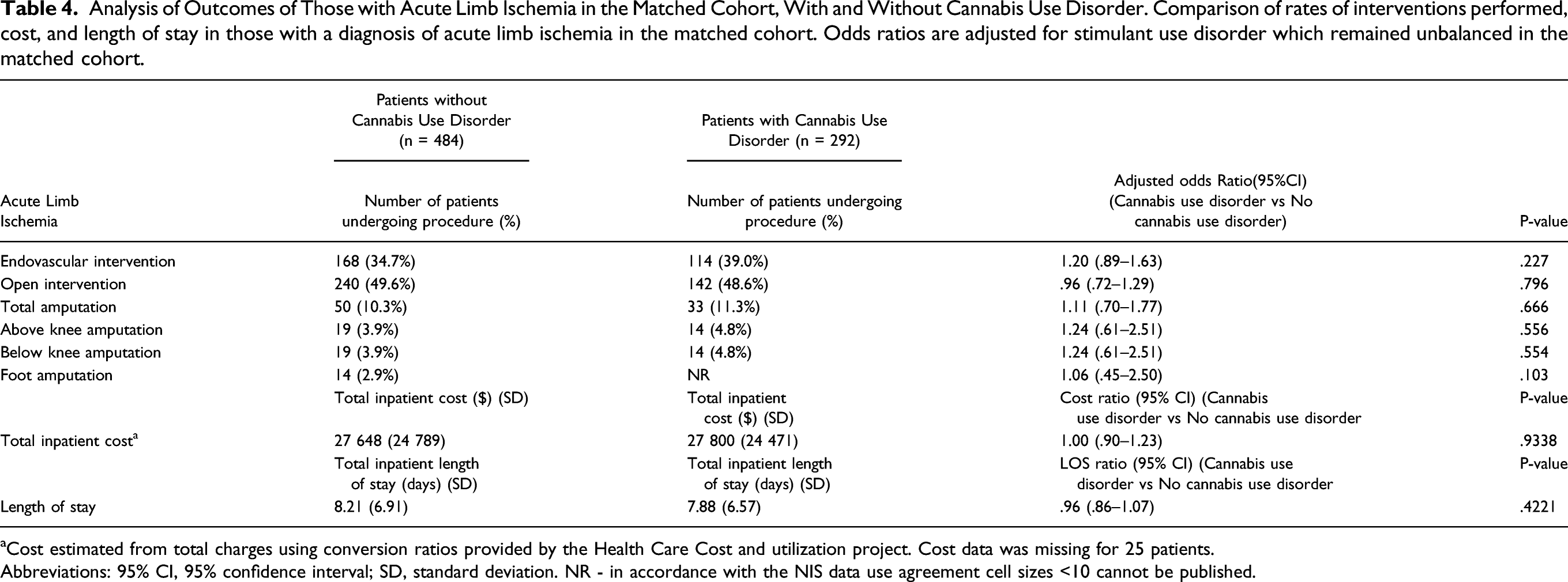
aCost estimated from total charges using conversion ratios provided by the Health Care Cost and utilization project. Cost data was missing for 25 patients.
Abbreviations: 95% CI, 95% confidence interval; SD, standard deviation. NR - in accordance with the NIS data use agreement cell sizes <10 cannot be published.
Analysis of Outcomes of Those with Critical Limb Ischemia in the Matched Cohort, With and Without Cannabis Use Disorder. Comparison of rates of interventions performed, cost and length of stay in those with a diagnosis of critical limb ischemia, defined as non-elective admissions, in the matched cohort. Odds ratios are adjusted for stimulant use disorder which remained unbalanced in the matched cohort.
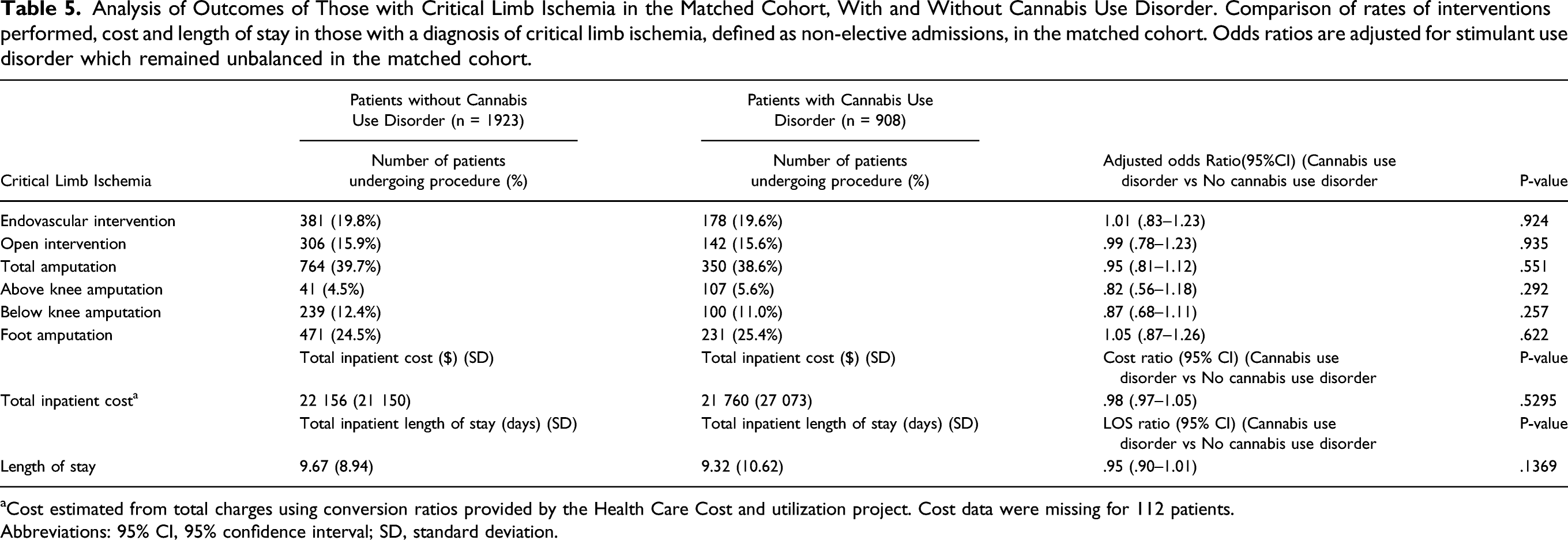
aCost estimated from total charges using conversion ratios provided by the Health Care Cost and utilization project. Cost data were missing for 112 patients.
Abbreviations: 95% CI, 95% confidence interval; SD, standard deviation.
Prevalence of Comorbidities Associated with Acute Limb Ischemia Among Patients in a Propensity-Matched Cohort (Nationwide Inpatient Sample, 2006- 2015). The records of patients in the matched cohort were queried for diagnoses, identified by ICD-9 codes, which may be part of the underlying mechanism of developing acute limb ischemia. This was performed both in the entire matched cohort and in those with a diagnosis of ALI in the matched cohort.
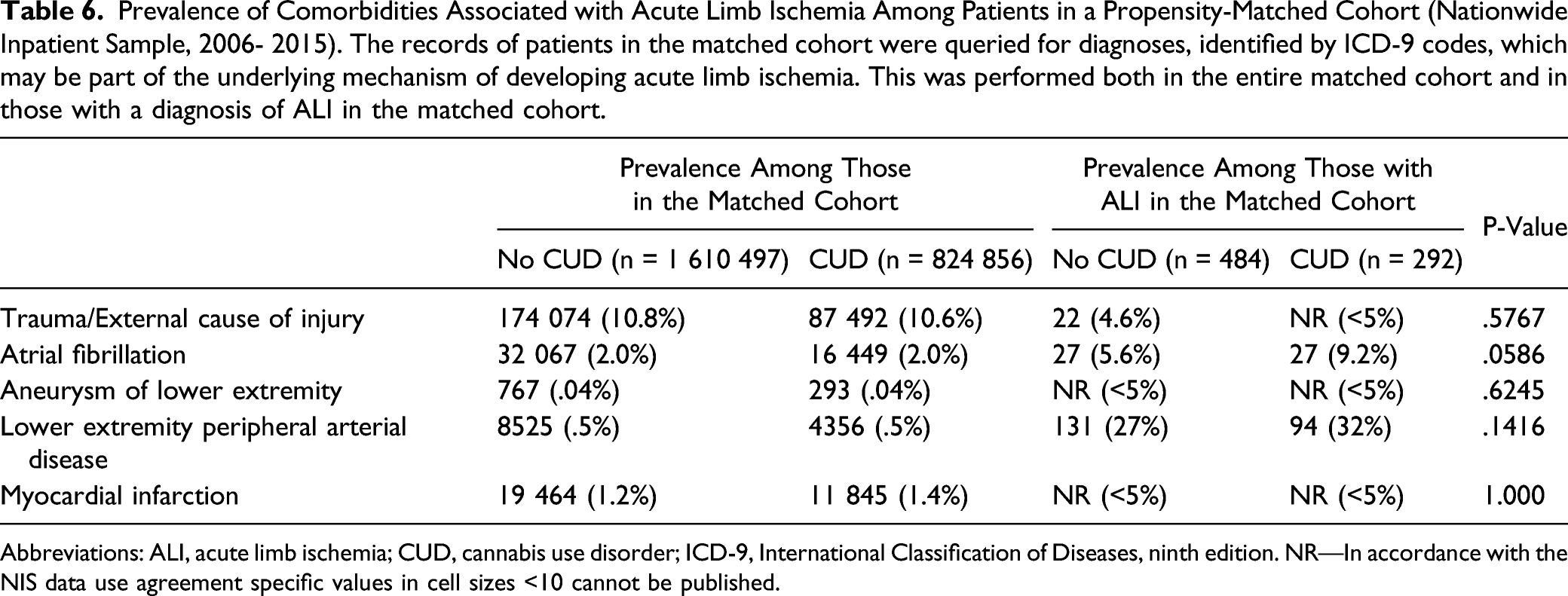
Abbreviations: ALI, acute limb ischemia; CUD, cannabis use disorder; ICD-9, International Classification of Diseases, ninth edition. NR—In accordance with the NIS data use agreement specific values in cell sizes <10 cannot be published.
Discussion
Acute Limb Ischemia
We observed a significantly increased incidence of ALI in those with CUD relative to those without, which was robust to sensitivity analyses. Notably, in the sensitivity analysis excluding CUD in remission from the definition of CUD, the OR was higher (1.28 vs 1.20). This would be expected if it is acute exposure to cannabis that mediates increased risk of ALI rather than lifetime exposure. In the coronary system, Mittleman et al, demonstrated risk is time dependent, with a 4.8 times greater risk of MI in the first hour after cannabis exposure. 1 The mechanism by which cannabis use increases occlusive complications in the arterial system, is not entirely understood. Endogenous cannabinoid receptors are present on platelets.6,22,23 Although the net in vivo effects of cannabis use are still subject to debate, exposure to THC has been demonstrated to lead to platelet aggregation in vitro6,22 There have also been reports of coronary artery thrombosis and aortic thrombus in heavy cannabis users, which may be secondary to a pro-coagulatory state.5,24,25 It has been observed that heavy cannabis users may develop MI in the absence of significant CAD.5,26,27
Cannabis is also known to impact arterial tone which is mediated by the autonomic nervous system and possibly by direct arterial effects.28,29 In the cerebral vasculature, one suspected mechanism for cannabis induced stroke is by inducing vasospasm.4,10 Cannabis induced changes to cerebral autoregulation has been demonstrated through transcranial doppler velocities following acute and chronic cannabis exposure.30,31 Similarly, cannabis affects peripheral vascular tone and impairs normal peripheral vascular reflexes.28,32 Generally cannabis causes peripheral vasodilation in the calf and forearm and constriction of cutaneous vessels of the digits.28,32,33 However, some patients have an atypical response. In a study by Benowitz et al. one participant after exposure to intravenous THC as well as smoked cannabis, demonstrated a greater than average hypertensive response and an abnormal increase in peripheral vascular tone. 33 Other authors have suggested increased vascular tone and decreased nitric oxide availability can cause endothelial dysfunction, release of pro-thrombotic mediators and thrombosis in the coronary system.5,34 There is also an impact from exposure to the products of plant matter combustion. Endothelial dysfunction following exposure to smoked cannabis has been observed, which is independent of THC. 35
Acute limb ischemia may be the result of numerous underlying disease processes. It did not appear that any one specific pathway was driving the increased rates of ALI in those with CUD (Table 6) in our cohort. Instead, as discussed above, it is likely alterations in patient physiology including a prothrombotic state or abnormal vascular tone which causes ALI through numerous underlying pathways. These may include thrombosis of peripheral aneurysms and critical stenosis or embolus from atrial fibrillation and proximal arterial thrombus. It is important to note we are only able to identify diagnostic codes associated with known pathways of developing ALI. We are unable to definitively know the exact cause or timeline of ALI in each patient, as the NIS does not contain this level of granularity.
Critical Limb Ischemia
Our initial hypothesis was cannabis use would lead to increased rates of CLI. This was based on prior reports of cannabis arteritis within the literature which is similar to, and may be a subtype of Buerger’s disease.9,10,36 Smoked cannabis also exposes the user to the negative arterial effects of the products of plant matter combustion which may contribute to PAD. 37 Our findings, however, are most consistent with a minimal or non-impact of cannabis use on CLI.
We initially observed a decreased incidence of CLI in those with CUD. We considered two possible sources of bias that may produce these findings, a misclassification leading to measurement bias or a selection bias. In order to maximize our sample size, we did not initially require diagnostic codes relating to rest pain (ICD-9:440.22) or tissue loss (ICD-9:440.23, 440.24) to appear in the first position (primary reason for admission in the NIS). The rational for this was CLI may be present in those admitted for other conditions, such as uncontrolled diabetes or renal disease. Other authors have required CLI to be the primary reason for admission in their definitions, which may be less prone to misclassification.16,17 We therefore repeated our analysis with this stricter definition of CLI, which yielded consistent results.
Another consideration was a selection bias. Those with SUDs are known to have barriers to accessing care because of stigma and patient specific factors.38-40 With ALI the loss of function, sensation or significant pain generally mandates presentation and admission to hospital. CLI on the other hand, is more insidious in nature and it is possible for care to be delayed for a prolonged period. As the NIS is an inpatient data set, if patients are not admitted they would not be captured. By defining CLI as only non-elective admissions we reduce this bias by only targeting severe cases, where presentation to hospital is less likely to be avoided. This demonstrated no significant difference in incidence of CLI in those with and without CUD. The initial finding of a decreased incidence of CLI in those with CUD may therefore be secondary to selection bias caused by barriers to receiving healthcare in less severe cases of CLI.
The absence of an association of CUD with increased rates of CLI is unexpected given what is known about tobacco addiction. Although cannabis may cause a distinct form of arterial disease in some individuals, our results are in keeping with this being a rare phenomenon.9,10,33 Cannabis arteritis likely represents an atypical response to cannabinoid exposure much like Buerger’s disease represents a unique response to tobacco smoke in a small group of individuals.9,10,33 Nicotine smoke does lead to peripheral arterial disease in the general population, through distinct mechanisms from that in Buerger’s disease. The products of combustion of cannabis are similar to tobacco and have greater tar and carcinogen levels, however, we do not see this reflected in rates of CLI.41,42 This may be due to less frequent use of cannabis relative to those who smoke nicotine. It also may reflect the lower addictive potential of marijuana relative to nicotine, leading to a lower cumulative exposure over one’s lifetime. 43 Nicotine itself is also believed to act in the development of PAD.44,45
Mesenteric Ischemia
We did not make any definitive findings with regards to mesenteric ischemia. We failed to demonstrate a statistically significant relation between heavy cannabis use and acute mesenteric ischemia. In the case of chronic mesenteric ischemia, we demonstrated an increased risk in those with CUD though this was not robust to sensitivity analysis. The results were not consistent when we required the diagnostic code to appear in the first position. Although this may be due to a reduced event rate and statistical power, it may also reflect misclassification when allowing the code to appear in any position.
The lack of association of CUD with AMI, despite an association with ALI, may be explained by the lower event rate of AMI. Alternatively, it may be due to differences in the physiologic effect of cannabinoids on the splanchnic circulation relative to the extremity circulation. Cannabinoids impact vascular tone in the mesenteric circulation.46,47 Studies conducted on rats demonstrate a primarily vasodilatory effect, though differences exist in response to cannabis between human and animal models.46,47 Further study is required regarding the effects of cannabis in the human splanchnic circulation and our results should be confirmed in prospective study designs.
Procedures and Cost
Our findings demonstrated that within a population that has ALI or CLI, there are no differences between the number of endovascular or open procedures performed, number of amputations, costs, or length of stay between those with CUD and without CUD. In a study by Dakour-Aridi et al., in the Premier Healthcare Database, there was an increased risk of their composite outcome for bypass graft related complication in those with cannabis abuse disorder, however, no change in rates of amputation. 48 Although they also demonstrated increased costs and length of stay in those with substance use disorders, this was not specific to CUD. 48 There are significant differences between those with opiate, hallucinogen, stimulant use disorders, and cannabis abuse. Our results suggest these increased costs and length of stay associated with the management of limb ischemia may not extend to those with CUD, when correcting for other forms of substance abuse. Our results also suggest those with CUD are generally managed in a similar fashion to those without CUD once the patient has developed limb threatening ischemia.
Limitations
There are a number of limitations to consider in this study. The NIS is a valuable resource to address questions such as ours, due to its large and nationally representative sample, however, it is limited by its administrative nature. We removed 2.2% of discharges due to missing data. Granular data regarding the means of cannabis consumption, dose, and frequency are not available. The ICD-9 codes for substance use disorders are known to be specific; however, they lack sensitivity.12,13 We therefore only capture those with heavy, regular cannabis use. Our results at this time cannot be generalized to casual users. In addition to this, due to lack of sensitivity, those with less frequent cannabis exposure would be present in the control cohort. Misclassification of those with CUD and ALI as non-CUD patients, would tend to bias our results to the null.
Our results are limited to those between 18 and 75 years of age. CUD is a rare exposure in those >75 years old and therefore the inclusion of this age group would lead to violations of the assumption of positivity. 11 This may have contributed to a lack of association with CLI and CUD, as patients had not accumulated a sufficient lifetime exposure to develop CLI.
CLI is a complex disease process and varies in its presentation and distribution within the peripheral circulation. Although administrative data have been used to investigate CLI in a similar fashion to our analysis, the lack of granularity in disease distribution and presentation may limit our findings.
Finally, there may still be unmeasured confounding present within the data set. Despite these limitations we believe these findings act as preliminary evidence that cannabis use can cause ALI which should be further confirmed in prospective designs with more detailed data capture.
Conclusions
This study demonstrated an increased incidence of ALI in those with CUD. There was no consistent association of CUD and CLI or AMI. We demonstrated an increased incidence of CMI in those with CUD, however, these results were not robust on sensitivity analysis. We found no differences in terms of procedures performed, rates of amputation, costs, or total length of stay.
Supplemental Material
Supplemental Material - The Association of Cannabis Use Disorder with Acute Limb Ischemia and Critical Limb Ischemia
Supplemental Material for The Association of Cannabis Use Disorder with Acute Limb Ischemia and Critical Limb Ischemia by Brandon McGuinness, Akash Goel, Jerry Chen, David Szalay, Karim Ladha, Murray A Mittleman, and John Harlock in Vascular and Endovascular Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.