
Abstract
Venous thromboembolism (VTE) is a common health condition with a high mortality and morbidity as well as significant health cost. Traditional treatment with parenteral heparin followed by vitamin K antagonist (VKA) has helped to decrease both morbidity and mortality over years. However, difficulties with warfarin such as INR monitoring, drug-drug interactions, and dietary restrictions has led to research for new anticoagulants. Thus, novel anticoagulants such as direct thrombin and factor X inhibitors have been developed and studied for various indications including the management of VTE. There is now good evidence that some novel anticoagulants are at least as effective as traditional anticoagulation therapy with probably safer outcomes. We have reviewed the literature on the medical management of VTE with the focus on the role of dabigatran, rivaroxaban, apixaban and edoxaban for this indication.
Introduction
Venous thromboembolism (VTE) is an important disorder that results from a thrombus formation within one or more of the deep veins due to an alteration in blood flow, vascular endothelial injury, and/or alteration in the constituents of the blood. 1 The two most common manifestations of VTE are pulmonary embolism (PE) and deep vein thrombosis (DVT), with the incidence of lower extremity DVT (LEDVT) higher than upper extremity DVT (UEDVT). 2 However, due to an increase in placement of pacemakers, internal cardioverter defibrillators, and peripherally inserted central catheters (PICC) over recent years, the incidence of UEDVT appears to be on the rise. 2 LEDVT is further divided into proximal (popliteal, femoral, or iliac vein) and distal (calf vein) forms. 3 Proximal LEDVT is of greater importance clinically due to its association with PE and chronic vein disease. 3 Cerebral, splanchnic, renal, and ovarian veins are less common atypical locations of VTE. 4
The incidence of VTE within the general population exceeds 1 per 1000 persons yearly, and approximately 900,000 new or recurrent cases of VTE are diagnosed each year in the United States. 5 A common complication of VTE is post-thrombotic syndrome, which results from vein damage caused by a thrombus. The cumulative incidence of post-thrombotic syndrome at one, two, and five years was 17%, 23%, and 28%, respectively. 6 The incidence rate of VTE increases exponentially with age for both genders. 5 Healthcare costs related to the diagnosis and treatment of VTE approximated 10 billion dollars in 2011. 7
Standard VTE anticoagulation therapy is expected to result in a mortality rate of less than 5%. 8 Traditionally, therapy has included initial unfractionated heparin (UFH) or low molecular weight heparin (LMWH) followed by vitamin K antagonist (VKA), most frequently warfarin. 9
Due primarily to findings from the CLOT (Randomized Comparison of Low-Molecular-Weight Heparin versus Oral Anticoagulant Therapy for the Prevention of Recurrent Venous Thromboembolism in Patients with Cancer) trial, LMWH has been the anticoagulant of choice to manage acute VTE in cancer patients. 10 Furthermore, LMWH may be used as a safe treatment for VTE in outpatient settings. 11
Fondaparinux is a synthetic pentasaccharide that binds to antithrombin with a higher affinity than LMWH, and does not lead to heparin-induced thrombocytopenia (HIT) since it does not interact with either platelets or platelet factor 4. 12 Therefore, Fondaparinux is sometimes used in patients with confirmed HIT. 12 The 2012 American College of Chest Physicians (ACCP) guidelines suggest the use of Fondaparinux or LMWH for the treatment of DVT. 13
Long-term warfarin therapy in VTE patients has been shown to reduce the incidence of recurrent VTE from 47% to 2%. 14 Despite its popularity, there are a number of inconveniences and issues associated with warfarin use, including significant variability in anticoagulant effect between individuals, numerous medication-medication interactions, and numerous dietary restrictions. 15 The need for anticoagulation therapies effective in treating VTE, combined with the problems surrounding warfarin use, has led to ongoing research to discover novel anticoagulation therapies that would be at least as effective as warfarin without the negative side effects. Two general classes of anticoagulant alternatives that have recently been identified are direct thrombin and Factor Xa (FXa) inhibitors. This paper provides an in-depth review of the relevant medical literature which evaluates the effectiveness of novel anticoagulation therapies for the treatment and prevention of VTE.
Direct thrombin inhibitors
Thrombin has been an important target in the research for novel anticoagulants due to its vital role as a coagulation factor that activates fibrinogen to fibrin, sends positive feedback to factors V, VIII, XI, and XIII, and activates platelet aggregation.16,17 Currently, there are several parenteral direct thrombin inhibitors and one oral direct thrombin inhibitor approved by the United States Food and Drug Administration (FDA) for different indications. The parenteral forms include Argatroban, Bivalirudin, Lepirudin, and Desirudin, with Dabigatran etexilate being the oral form. 18 The primary use of parenteral direct thrombin inhibitors has been in the management of HIT. 18 Meanwhile, dabigatran is FDA-approved for stroke and systemic embolism (SE) prevention in patients with non-valvular atrial fibrillation (NVAF). 15 Our paper will review the data for using dabigatran in the management and prevention of VTE.
Dabigatran (Pradaxa®)
In 2010, the FDA approved dabigatran for the prevention of stroke and SE in patients with NVAF, making it the first oral anticoagulant approved in more than 50 years. 15 In the United States, Dabigatran etexilate is available in two approved dosages: 150 mg BID (creatinine clearance (CrCl) of > 30 mL/min) and 75 mg BID (CrCl of 15-30 mL/min), with approval of the 75 mg dosage resting entirely on pharmokinetic profiling rather than clinical evidence.15,19,20 A third dosage of 110 mg has been approved in Europe. However, there is no dosing information available for pregnant/nursing mothers, children, or patients with a CrCl of < 15 mL/min.15,20 Studies suggest that dabigatran may be effective for the treatment or prevention of VTE, but it has yet to be approved for this purpose. 15
Mechanism of action and pharmacology (Table 1)
Pharmacologic comparison between the novel anticoagulants.
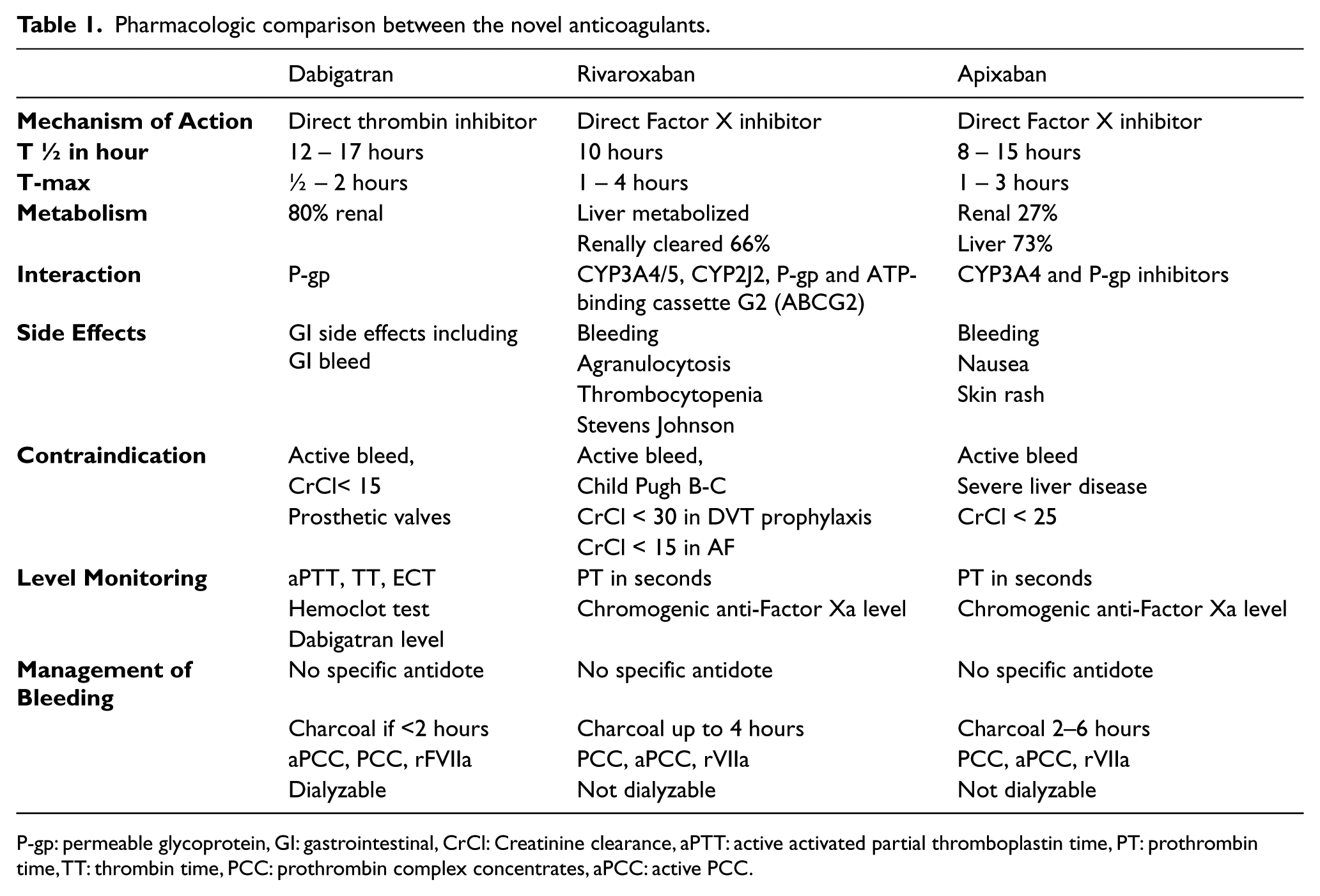
P-gp: permeable glycoprotein, GI: gastrointestinal, CrCl: Creatinine clearance, aPTT: active activated partial thromboplastin time, PT: prothrombin time, TT: thrombin time, PCC: prothrombin complex concentrates, aPCC: active PCC.
Dabigatran is a pro-drug and is converted to its active form, etexilate ester, within the body. 15 Following administration to a fasting patient, peak plasma concentration is reached by 1.5 hours on average. 15 The half-life of dabigatran in healthy patients after multiple doses is 12-14 hours.15,21 Its duration of action is 24 hours in patients with normal renal function and up to five days in patients with renal insufficiency.15,21,22 Approximately 35% of dabigatran remains bound to human plasma proteins, and 80% is excreted via the renal system.15,20,21,23,24 Absolute bioavailability is approximately 3-7%.15,20,22
Dabigatran etexilate is a substrate of the efflux permeability glycoprotein transporter (P-gp). The P-gp transporter is highly expressed in the intestine and kidneys and promotes excretion of dabigatran. 15 Circulating levels of dabigatran are increased by an inhibition of drug secretion, brought about by the action of P-gp inhibitors such as amiodarone, dronedarone, quinidine, ketoconazole, and verapamil. 15 P-gp transporter inducers, such as rifampicin, have an opposite effect of decreasing dabigatran concentration and thus efficacy. 15 Concomitant use of dabigatran with P-gp inducers or inhibitors should be avoided. 20 Administration of verapamil or dronedarone within one hour prior to dabigatran has resulted in the largest observed increases in circulating drug levels.15,20,25 However, administration of P-gp inducers two hours following dabigatran results in a minimization of this interaction. In the case of concurrent use of dronedarone or systemic ketoconazole with dabigatran in patients with creatinine clearance of 30-50 mL/min, it is suggested that the 75 mg BID dabigatran dose be used. 20 In case of creatinine clearance of 15-30 mL/min this concurrent use should be avoided entirely. 20
Conversion and reversal
There is no consensus on how to switch from and to dabigatran in patients on a different anticoagulant. However, there is some evidence to support the following practice recommendations. Warfarin can be discontinued and dabigatran can be started once international normalized ratio (INR) has fallen below 2.0. 15 Conversely, when converting from dabigatran to warfarin, warfarin should be started three days before discontinuation of dabigatran in patients with a CrCl of > 50 mL/min, two days prior for CrCl of 30-50 mL/min and one day prior for CrCl of 15-30 mL/min.20,26 There are no recommendations for CrCl of < 15 mL/min.20,26 When switching from a parenteral anticoagulant it is acceptable to take the first dabigatran dose zero to two hours prior to the next scheduled dose of the parenteral anticoagulation.20,27 Dabigatran can be discontinued 12 or 24 hours prior to initiating parenteral anticoagulation in patients with CrCl of ≥ 30 mL/min or CrCl of 15-30 mL/min, respectively. 20
As with other direct thrombin inhibitors, dabigatran does not have a specific antidote. However, effective absorption of dabigatran by activated charcoal has been demonstrated by in vitro trials. Thus, it is currently recommended that activated charcoal be administered within one to two hours following a dabigatran overdose. 23 In cases with severe bleeding, hemodialysis was shown to help eliminate around 60% of the drug from the system. 28 In vitro human plasma studies and animal studies have shown the ability of active prothrombin complex concentrates (aPCC), and to less extent PCC, to significantly reduce dabigatran-induced bleeding time.23,26 However, aPCC and PCC should only be used as a last resort due to the increased risk of disseminated intravascular coagulopathy (DIC) and/or SE.23,26 Another possible last resort agent is recombinant factor VII, as it carries the same risk as aPCC.23,26 Vitamin K and fresh frozen plasma are ineffective in reversing the effects of dabigatran.23,26 Another promising reversing agent being researched is aDabi-Fab. It is a specific fragment antigen binding antidote that binds to dabigatran with approximately 350 times greater affinity than thrombin and has been demonstrated to reverse dabigatran anticoagulation effects in animal models. 29
Common side effects
Based on data from the RE-LY trial, gastrointestinal (GI)-related adverse reactions occur in 35% of patients and are by far the most common side effects related to dabigatran use. 29 These adverse reactions include dyspepsia, abdominal pain, epigastric discomfort, acid reflux, esophagitis, erosive gastritis, gastric hemorrhage, and gastrointestinal ulcer. 29 Hypersensitivity reactions, occurring in < 0.1% of patients, are much less common. Hepatitis risk was not statistically different with dabigatran 150 mg versus warfarin (1.9% and 2.2%, respectively). 29 Worthy of note is that both these rates are significantly lower than the hepatitis risk resulting from ximelagatran use, which was observed to be 6.4% during the THRIVE III trial. 30
Clinical use of dabigatran in the management and prevention of VTE (Table 2)
Novel anticoagulants: Indications, dosages, and evidence.
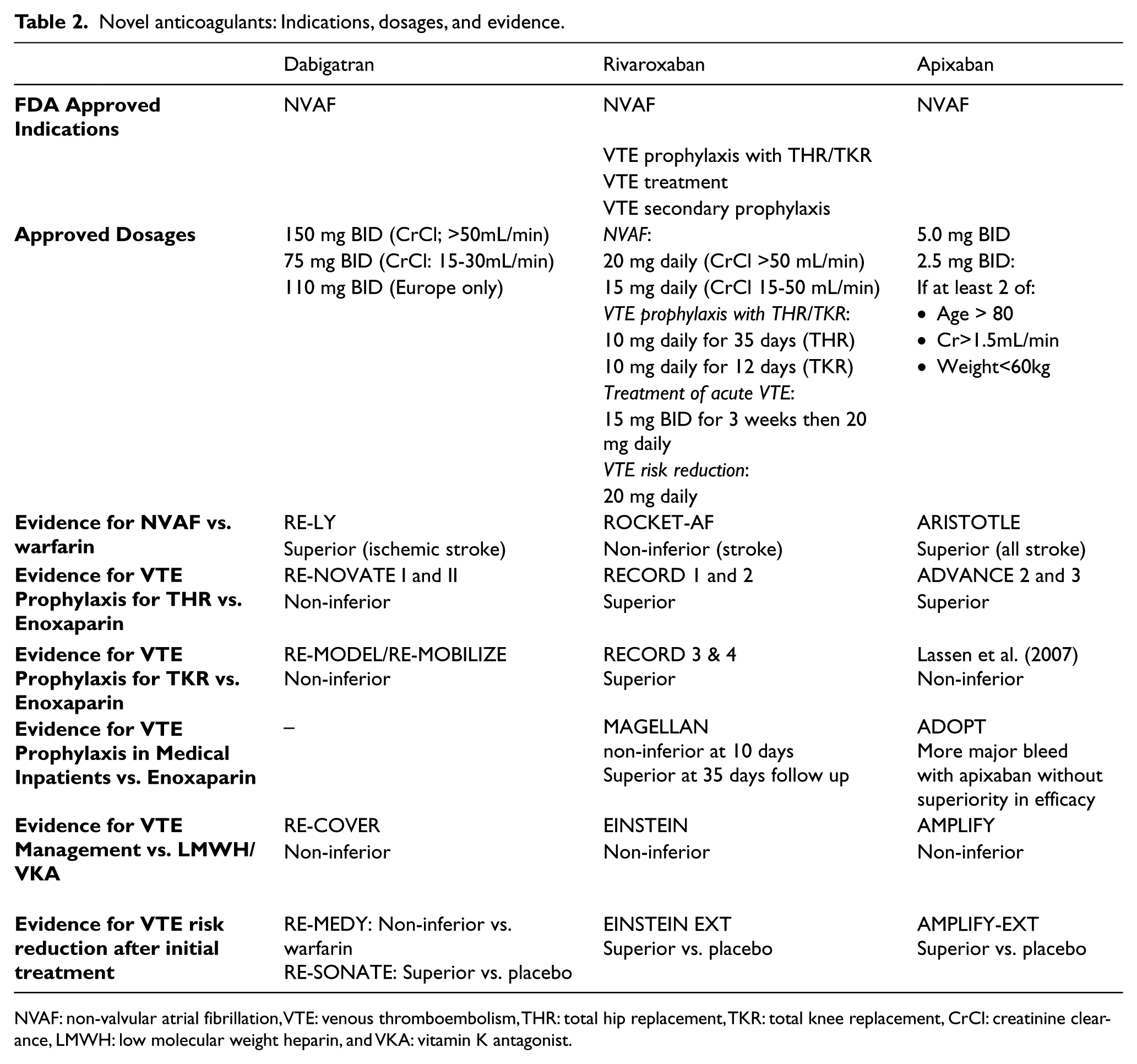
NVAF: non-valvular atrial fibrillation, VTE: venous thromboembolism, THR: total hip replacement, TKR: total knee replacement, CrCl: creatinine clearance, LMWH: low molecular weight heparin, and VKA: vitamin K antagonist.
Prevention of VTE after total hip replacement
The RE-NOVATE trial assessed the efficacy and safety of once-daily dabigatran etexilate 220 mg or 150 mg versus once-daily subcutaneous (SQ) enoxaparin 40 mg for VTE prevention in patients undergoing total hip replacement (THR). Dabigatran 220 mg or 150 mg were non-inferior to enoxaparin with regards to VTE prevention (P < 0.0001), which was observed in 6.7% of patients on enoxaparin versus 6.0% and 8.6% with dabigatran 220 mg and 150 mg, respectively. 31 Additionally, there was no difference in major bleeding rates between enoxaparin and either dabigatran 220 mg (P = 0.44) or 150 mg (P = 0.60). 32 Overall, when used to prevent VTE following THR, oral dabigatran was at least as effective as enoxaparin with a similar safety profile. 31
Prevention of VTE after total knee replacement
Similarly, the RE-MODEL trial assessed dabigatran 220 mg or 150 mg versus enoxaparin 40 mg for the reduction of VTE incidence following total knee replacement (TKR). For a composite of total VTE and mortality, dabigatran in both 220 and 150 mg doses was non-inferior to the enoxaparin arm (P = 0.0003 and P = 0.017, respectively), with no significant difference in bleeding events. 32 Overall, the 220 mg and 150 mg doses of dabigatran were as effective and safe as enoxaparin for prevention of VTE following TKR. 32
Meta-analysis of dabigatran vs. enoxaparin
A meta-analysis of four clinical trials (RE-MODEL, RE-MOBILIZE, RE-NOVATE, and RE-NOVATE II) was conducted comparing the efficacy and safety of dabigatran versus enoxaparin in patients undergoing THR and TKR. With regards to VTE incidence and all-cause mortality, dabigatran was found to be non-inferior to enoxaparin (RR 1.03, 95% CI 0.93-1.15). 15 Additionally, dabigatran and enoxaparin were found to have a similar safety profile (RR 1.09, 95% CI 0.74-1.61). 15
Treatment of acute VTE
The RE-COVER study trial compared the efficacy and safety of dabigatran 150 mg BID versus dose-adjusted warfarin (target INR 2-3) for the treatment of acute VTE after an initial anticoagulation with parenteral anticoagulation (generally intravenous UFH or LMWH) for a median of nine days. The primary outcome was the six month incidence of recurrent symptomatic VTE and related deaths. Incidence of recurrent VTE occurred at similar rates with dabigatran and warfarin (2.4% and 2.1%, respectively; P<0.001 for non-inferiority). 33 Although major bleeding episodes occurred at similar rates in both groups, bleeding episodes of any severity were observed at a lower rate in patients on dabigatran (dabigatran risk ratio 0.71; 95% CI, 0.59 to 0.85). 33 For the treatment of acute VTE, and after initial transient anticoagulation with heparin, dabigatran was found to be as effective as warfarin, had a similar safety profile, and did not require laboratory monitoring. 33
Extended anticoagulant use in patients with VTE
The RE-MEDY and RE-SONATE trials compared the efficacy and safety of dabigatran 150 mg BID versus warfarin or placebo, respectively, for extension VTE management in patients who completed at least three months of initial anticoagulation. In the active-control RE-MEDY trial, recurrent VTE occurred at similar rates in dabigatran and warfarin patients (P = 0.01 for non-inferiority). 34 The dabigatran group (0.9%) and the warfarin group (1.8%) had similar occurrences of major bleeding alone (95% CI, 0.27-1.02). 34 However, combined major or clinically relevant bleeding was less frequent with dabigatran compared to warfarin (95% CI, 0.41-0.71). 34 Dabigatran was determined to be as effective as warfarin for the extended treatment of VTE and carried a lower risk of major or clinically relevant bleeding. 34
In the placebo-control RE-SONATE trial, recurrent VTE was less frequent in the dabigatran than the placebo group (P < 0.001). However, dabigatran presented an increased risk of major or clinically relevant bleeding (5.3% vs. 1.8%, respectively; 95% CI, 1.52-5.60). 34 Dabigatran was more effective than placebo in preventing VTE, but also presented increased incidence of major or clinically relevant bleeding. 34
Direct factor Xa inhibitors
Both the intrinsic and extrinsic clotting pathways converge at the activation of enzyme FXa, which is a major activator for thrombin. Thus, FXa inhibition has been another ideal goal for anticoagulation therapies. 35 Indirect FXa inhibitors function as co-factors to proteases such as antithrombin; such inhibitors include UFH, LMWH and Fondaparinux. Direct FXa inhibitors bind directly to FXa and prevent it from catalyzing the production of thrombin from prothrombin. An advantage of direct FXa inhibitors is that they bind directly to clot-bound FXa, which produces a stronger anticoagulation effect.36,37 Multiple direct FXa inhibitors have been developed, including rivaroxaban, apixaban, betrixaban, and edoxaban. This paper will only review the data related to rivaroxaban, apixaban and edoxaban.
Rivaroxaban (Xarelto®)
Mechanism of action and pharmacology (Table 1)
Rivaroxaban is a direct FXa inhibitor taken once daily, orally with a rapid onset of one to four hours post-ingestion. 38 In healthy individuals, rivaroxaban has an average half-life of 10 hours and is eliminated through both hepatic metabolism and renal excretion (33% and 66%, respectively). 38 As with other direct FXa inhibitors, rivaroxaban has been demonstrated to block both free and clot-bound FXa.39,40 Rivaroxaban may interact with both CYP3A4/5 and P-gp activators as well as inhibitors. P-gp inhibitors such as ketoconazole, ritonavir, clarithromycin, erythromycin, and fluconazole may increase rivaroxaban plasma level, whereas P-gp inducers such as carbamazepine, phenytoin, rifampin, and St. John’s wort may decrease rivaroxaban level. 41 It is recommended to avoid using rivaroxaban with these drugs. Bleeding was the most common rivaroxaban side effect that led to its discontinuation during the VTE trials. Other rare side effects include agranulocytosis, thrombocytopenia, retroperitoneal hemorrhage, cholestasis, and anaphylactic reactions. 42
Conversion and reversal
There is no main consensus guideline on how to exchange rivaroxaban with other anticoagulants. Although solid clinical data is lacking, based on the evidence from the ROCKET AF trial, it has been suggested to discontinue warfarin and start rivaroxaban once the INR has fallen below 3.0. 43 Conversely, when converting from rivaroxaban to warfarin, warfarin should be started four days before discontinuation of rivaroxaban in patients with a CrCl of > 50 mL/min, three days prior for CrCl of 30-50 mL/min, and two days prior for CrCl of 15-30 mL/min. There are no recommendations for CrCl of < 15 mL/min. 26 Due to rivaroxaban effects on prothrombin time, point-of-care INR monitors during rivaroxaban/warfarin conversions should be avoided. 26
As with dabigatran, rivaroxaban lacks a specific antidote. Four-factor PCCs containing clotting factors II, VII, IX, and X have been shown to reverse rivaroxaban anticoagulant effects in healthy volunteers. 23 Although clinical data is lacking, due to side effects of DIC and SE, it is cautiously suggested to administer 4-factor PCCs or aPCC in case of acute major bleeding. 26 However, it is unclear whether 3-factor PCCs are effective. 27 Due to high plasma protein binding of approximately 95%, hemodialysis is not an effective treatment for rivaroxaban overdose. 26 Additionally, fresh frozen plasma has no known effect on rivaroxaban anticoagulation effects. 28
Clinical use (Table 2)
Clinical indications and contraindications
Rivaroxaban is currently approved for several indications in the United States. It was first approved for VTE prophylaxis in patients undergoing THR or TKR.38,42,44,45,46,47 Based on results from the ROCKET AF trial, rivaroxaban was then approved for prevention of ischemic stroke and SE in patients with NVAF.42,43 Finally, rivaroxaban received approval for treatment and then secondary prevention of acute DVT and PE.42,48,49,50 Current Institute for Clinical Systems Improvement (ICSI) guidelines suggest initial treatment of DVT and PE with rivaroxaban as an alternative to UFH, LMWH, or Fondaparinux. 51 Rivaroxaban is contraindicated in cases of hypersensitivity, active major bleeding, hepatic impairment, renal insufficiency with a CrCl level of < 30 mL/min for DVT prophylaxis, and a CrCl level of < 15 mL/min for thromboembolism/stroke prophylaxis.42,43,44,45,46,47,48,49,50
VTE prophylaxis following THR and TKR
The four RECORD trials assessed the safety and efficacy of once-daily rivaroxaban 10 mg versus SQ enoxaparin (40 mg in RECORD 1-3, 30 mg in RECORD 4). Patients were treated following THR (RECORD 1 and 2) and TKR (RECORD 3 and 4).44,45,46,47,52 In all four RECORD trials, rivaroxaban was significantly superior to enoxaparin in total VTE reduction. In RECORD 1, 2, and 3, rivaroxaban was superior in reducing the incidence of a composite outcome of proximal DVT, symptomatic PE, and all-cause mortality. RECORD 2 and 3 found that rivaroxaban was superior to enoxaparin in reducing a composite outcome of symptomatic DVT, symptomatic PE, and VTE-related death. 52 In addition, in all four RECORD trials there was no statistically significant difference in major bleeding events between patients receiving rivaroxaban or enoxaparin (less than 0.7% in each trial). 52 A pooled analysis of the four RECORD trials revealed rivaroxaban to be superior to enoxaparin in reducing symptomatic VTE and all-cause mortality. 52 The results of the RECORD trials led to the approval of rivaroxaban for VTE prevention following THR and TKR.52,53
VTE management in acutely ill patients
The MAGELLAN study assessed the efficacy and safety of once-daily rivaroxaban 10 mg versus 40 mg of daily SQ enoxaparin in patients hospitalized for an acute medical illness with an age greater than 40 years. At day 10 of treatment, the incidence of asymptomatic proximal or symptomatic VTE was 2.7% in both groups (P=0.003 for non-inferiority). 54 At day 35 of treatment, a VTE event was observed in 4.4% of the rivaroxaban and 5.7% of the enoxaparin population (P=0.02 for superiority). 54 However, there was more major or clinically relevant non-major bleeding with rivaroxaban versus enoxaparin (P<0.001). 54 For VTE reduction, standard-duration thromboprophylaxis with rivaroxaban proved non-inferior to enoxaparin, and extended-duration use of rivaroxaban proved superior to enoxaparin/placebo. However, rivaroxaban use was associated with an increased risk of bleeding at both durations. 54
Symptomatic VTE treatment
The EINSTEIN-DVT study assessed the efficacy and safety of rivaroxaban alone (15 mg BID, followed by 20 mg once-daily) versus enoxaparin followed by VKA (either warfarin or acenocoumarol) in patients with acute, symptomatic DVT without PE. In a parallel continued-treatment study, EINSTEIN-EXT, the efficacy of 20 mg of daily rivaroxaban was compared to placebo in patients who had already undergone six or 12 months of initial VTE therapy. The primary efficacy outcome for both studies was recurrent venous thromboembolism. The principal safety outcome was major or clinically relevant non-major bleeding for the initial-treatment study, and major bleeding for the continued-treatment study. 49
Rivaroxaban was found to be non-inferior to enoxaparin/VKA and superior to placebo for the prevention of recurrent VTE in the EINSTEIN-DVT and EINSTEIN-EXT trial, respectively (P<0.001 for both). 49 There was no major bleeding difference between rivaroxaban and enoxaparin/VKA in the DVT study or versus placebo in the EXT study. However, clinically relevant non-major bleeding was increased from 1.2% in the placebo group to 5.4% with rivaroxaban. 49 Use of rivaroxaban offers a single drug approach for the initial and extended management of symptomatic VTE, with potentially improved risk-to-benefit anticoagulation profile. 49
Treatment of symptomatic PE
Similarly, the EINSTEIN-PE study compared rivaroxaban alone to enoxaparin followed by VKA for the treatment of acute symptomatic PE. Symptomatic recurrent VTE occurred at similar rates in both the rivaroxaban and standard therapy groups (P=0.003 for non-inferiority). 50 Additionally, rivaroxaban therapy and enoxaparin/VKA therapy resulted in similar incidence of major or clinically relevant bleeding (P=0.23). However, major bleeding occurred less often with rivaroxaban than standard therapy (1.1% and 2.2%, respectively; P=0.003). 50 Compared to enoxaparin followed by VKA, rivaroxaban alone presented non-inferior efficacy and a potentially improved benefit-to-risk anticoagulation profile for the treatment of acute PE. 50
Apixaban (Eliquis®)
Apixaban is another direct FXa inhibitor that was approved by the FDA in December of 2012 for stroke prevention in patients with NVAF. 55
Pharmacodynamics (Table 1)
Apixaban is administered orally BID and is approved for 2.5 mg and 5.0 mg dosages. 55 The drug has a half-life of 12 hours in healthy patients and a high oral bioavailability of greater than 50% across different animal models.56,57 Approximately 73% of the drug is metabolized hepatically, with the remaining 23% excreted renally. There are drug interactions with potent CYP3A4 and P-gp transporter inhibitors similar to the ones observed with rivaroxaban.56,57
Conversion and reversal
Similar to the other novel anticoagulants, there are no consensus guidelines on the conversion between apixaban and other anticoagulants, and clinical data on apixaban conversion is very limited. It has been suggested to switch warfarin to apixaban once INR has fallen below 2.0. 55 As with rivaroxaban, INR monitoring during apixaban/warfarin conversions is inaccurate. Conversely, when switching from apixaban to warfarin, it has been suggested to simultaneously discontinue apixaban and begin warfarin along with parenteral anticoagulation. 55 Once the INR is accurately measured to be in an acceptable range, parental anticoagulation may be stopped. When converting between apixaban and non-warfarin anticoagulants, it is recommended to discontinue one anticoagulant and begin the other at the next scheduled dose. 55
Clinical data on apixaban reversal is very limited. 58 As with other direct FXa inhibitors, apixaban has no antidote. However, it is suggested that administration of activated charcoal within two to six hours post-ingestion is effective for reducing apixaban blood levels in the event of overdose or accidental ingestion.55,58 As a direct FXa inhibitor similar to rivaroxaban, it is thought that 4-factor PCCs and aPCC may be effective and fresh frozen plasma ineffective in reversing apixaban effects. 59
In 2013, results of a Phase 2 trial involving FXa inhibitor antidote PRT4445 demonstrated 95% reversal of apixaban anticoagulation effects in healthy patients. 60 PRT4445 acts as a FXa decoy that binds and sequestors direct FXa inhibitors in the blood. Use of PRT4445 was not associated with adverse events. This antidote, tentatively named andexanet alfa, is still in clinical trials. 60
Clinical use (Table 2)
Thromboprophylaxis after THR
Efficacy and safety of 2.5 mg apixaban BID versus 40 mg enoxaparin in patients undergoing THR was assessed by the ADVANCE-3 study. Apixaban was not only non-inferior but superior to enoxaparin for the primary efficacy outcome, defined as a composite of asymptomatic or symptomatic DVT, nonfatal PE, or death from any cause during the treatment period (P<0.001 for both). 61 Additionally, a composite of major and clinically relevant non-major bleeding was observed in 4.8% of the apixaban group and 5.0% of the enoxaparin group, for an absolute risk reduction of -0.2% (95% CI, -1.4 to 1.0). Following THR, apixaban was more effective than enoxaparin in reducing VTE and had a similar safety profile. 61
Thromboprophylaxis after TKR
Lassen et al. (2007) compared 5, 10, and 20 mg apixaban BID-divided and once daily (six options total), versus 30 mg enoxaparin BID, and open-label warfarin (titrated to 2.8-3.0 INR) in patients undergoing TKR. 62 Following 10-14 days of anticoagulation therapy, each apixaban group had experienced lower rates of a composite of VTE and all-cause mortality than either the enoxaparin or warfarin group. 62 In addition, an increased apixaban dosage was associated with increased efficacy (P=0.09 for daily/BID combined) with the expense of increased incidence of bleeding events for both BID and daily apixaban groups (P=0.01 and P = 0.02, respectively). 62 Efficacy and safety of each apixaban dosage was not affected by daily or BID-divided options. Compared to current thromboprophylaxis standards following TKR, apixaban had a favorable benefit-to-risk anticoagulation profile in doses of 2.5 mg BID or 5 mg daily. 62
VTE management in acutely Ill patients
The ADOPT trial assessed the efficacy and safety of apixaban 2.5 mg twice daily for 30 days, or enoxaparin, administered subcutaneously at a dose of 40 mg once daily for six to 14 days, in acutely ill hospitalized medical patients. 63 The primary efficacy outcome was the 30-day composite of death related to VTE, PE, symptomatic DVT, or asymptomatic proximal-leg DVT. The primary safety outcome was bleeding. The results showed more major bleeding in the apixaban versus enoxaparin group (P=0.04) without evidence of superiority for the primary efficacy outcomes. 63
Initial and extended VTE treatment
The AMPLIFY trial compared apixaban to the standard therapy of enoxaparin followed by VKA for the treatment of acute VTE. Apixaban was non-inferior to enoxaparin/VKA for incidence of recurrent symptomatic VTE or VTE-related death (P<0.001 for both relative risk and difference in risk), and was associated with a lowered incidence of major bleeding (P<0.001 for superiority). 64 Additionally, a composite of major bleeding and clinically relevant non-major bleeding was observed in only 4.3% of apixaban versus 9.7% of standard therapy patients (P<0.001). 64 Apixaban provided non-inferior efficacy for the initial treatment of acute VTE, while significantly reducing bleeding events. 64
The AMPLIFY-EXT study compared 2.5 mg and 5.0 mg dosages of apixaban BID versus placebo for extended treatment of VTE. All patients had already completed six to 12 months of anticoagulation therapy. Incidence of symptomatic recurrent VTE or VTE-related death over the six- or 12-month trial period was greatly reduced with apixaban (1.7% for both apixaban dosages versus 8.8% for placebo; P<0.001 for both comparisons). 65 Additionally, a composite of major and relevant non-major bleeding found both apixaban doses to be non-inferior to placebo, although the 5.0 mg apixaban was associated with increased incidence of relevant non-major bleeding compared to placebo (RR 1.82; 95% CI, 1.05-3.18). 65 Apixaban at either a 2.5 mg or 5.0 mg dose for extended anticoagulation reduced the risk of recurrent VTE without increasing major bleeding events. 65
Edoxaban
Edoxaban is another direct FXa inhibitor which is used at a single daily dose of 30 or 60 mg that is not currently available in the United States. 66
Pharmacodynamics
Despite a half-life of six to 10 hours, it is administered once daily, and its absorption is unaffected by food. Edoxaban is renally excreted and is a substrate for P-gp. 66
Clinical use
Thromboprophylaxis after TKR and THR
A pooled analysis of STARS E-3 and STARS J-5 trials that compared edoxaban 30 mg once daily with subcutaneous enoxaparin 20 mg twice daily in Japanese and Taiwanese patients undergoing TKR and THR, respectively, showed that edoxaban was associated with a lower incidence of composite of symptomatic and asymptomatic DVT and PE (5.1% versus 10.7%, P<0.001). 67 The incidence of major and clinically relevant non-major bleeding events as a safety outcome was 4.6% versus 3.7% in the edoxaban and enoxaparin groups, respectively (P = 0.427). 67
Initial VTE treatment
The Hokusai-VTE investigators randomly assigned patients with acute VTE, who had initially received heparin, to receive edoxaban at a dose of 60 mg once daily, or 30 mg once daily (e.g., in the case of patients with creatinine clearance of 30 to 50 ml/min or a body weight below 60 kg), or to receive therapeutic dose of warfarin for three to 12 months. 68 The primary efficacy outcome was recurrent symptomatic VTE and safety outcome was major or clinically relevant non-major bleeding. While edoxaban was non-inferior to warfarin with respect to the primary efficacy outcome (P<0.001 for non-inferiority), it was superior to warfarin in terms of safety outcome (P=0.004 for superiority). 68
Edoxaban is commercially available in Japan but has limited availability elsewhere. Further study of its safety in the general population is needed.
Current antithrombotic therapy recommendation with novel anticoagulants
When the 2012 ACCP guidelines were prepared, most of the clinical data discussed above were not published. Even so, the guidelines suggested using the novel anticoagulant agents in lieu of VKA or LMWH in the management and prevention of VTE if VKA and LMWH could not be used or tolerated. 69 The more recent ICSI practice guidelines recommended rivaroxaban as an alternative anticoagulant for the initial and maintenance phases of VTE treatment. 51 To our knowledge, there is no evidence to support the use of novel anticoagulants in the management of thrombosis caused by HIT.
Conclusion
Clinical data from recent years offers strong support for the use of novel anticoagulants for the treatment and prevention of VTE. For VTE management and prevention novel anticoagulants may provide similar efficacy and safety as traditional therapy with heparin and VKA. Furthermore, they do not require regular level monitoring. Although these drugs currently lack a specific antidote, current evidence showed that major bleeding was relatively lower when compared to traditional anticoagulation. Rivaroxaban is currently the only oral anticoagulant with FDA approval for treatment and prevention of VTE. We call for research to address the use of these novel anticoagulation agents for the management of HIT related thrombosis.
Footnotes
Declaration of conflicting interest
The authors report no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.