
Abstract
We determined whether 7T magnetic resonance angiography (MRA) could be used for clearly observing microvessels in a clinically asymptomatic patient with steno-occlusion of the middle cerebral artery (MCA). We utilized 3T magnetic resonance imaging to obtain the brain images of a clinically asymptomatic patient and noted MCA steno-occlusion. In comparison with 3T MRA, 7T MRA could clearly delineate the microvessels, including lenticulostriate arteries and presumed collaterals, and our observation was comparable to that with conventional digital subtraction angiography. We report an interesting case of a clinically asymptomatic patient with MCA steno-occlusion.
Introduction
Atherosclerotic stenosis of major intracranial arteries (carotid siphon, middle cerebral, vertebral, and basilar arteries) is the main cause of ischemic stroke. Intracranial stenosis, especially in symptomatic patients, is not a static condition and may progress in a relatively short period. The progressive stenosis of intracranial arteries is strongly related to the development of ischemic events. 1 Although vascular problems are revealed after stroke in most patients, many of them are asymptomatic despite pathological changes in their intracranial arteries. 2 We often encounter clinically asymptomatic patients who have severe steno-occlusion of intracranial arteries. 3 In this situation, a precise diagnosis is a prerequisite for treating asymptomatic patients with steno-occlusion of the middle cerebral artery (MCA).
To date, the conventional catheter-based digital subtraction angiography (DSA) is the gold standard for examining cerebral vessels, evaluating the degree of arterial stenosis, and determining the existence of collaterals or microvessels. However, complications in cerebral angiography using DSA occur, even though they are less than 1% of procedures when performed by experienced physicians. 4
We report an interesting case of a clinically asymptomatic patient who had MCA steno-occlusion that was detected using 3T magnetic resonance angiography (MRA). However, microvessels, including lenticulostriate arteries and presumed collaterals, were observed using 7T MRA, a non-invasive technique.
Case report
A 42-year-old woman with no previously reported clinical history visited the neurology department with the complaint of a dull headache that had persisted for 1 month. The patient’s blood pressure was 120/69 mmHg and body mass index was 23.1 kg/m2. There was no past history of hypertension, diabetes mellitus, alcohol, smoking, infection, or drug use, such as oral contraceptives, and no family history of stroke. Laboratory findings such as levels of hemoglobin, glucose, cholesterol, and double-stranded DNA were within a normal range. Physical and neurological examinations were also normal. The patient was prescribed cilostazol for the primary prevention of stroke.
Brain 3T magnetic resonance imaging (MRI) with angiography revealed the presence of severe steno-occlusion of the right MCA without evidence of infarction or any other structural lesions of the brain, as assessed using fluid-attenuated inversion recovery (FLAIR) (Figures 1a and 1b). On perfusion computed tomography (CT), there was no significant prolongation of transit time on the time to peak perfusion on either of the MCA territories. After the patient signed the informed consent form, she underwent a 7T MRA study, which revealed the presence of microvessels around the steno-occluded MCA (Figure 1c). Findings on DSA were directly compared with those of 7T MRA, especially for microvessels (Figure 1d).
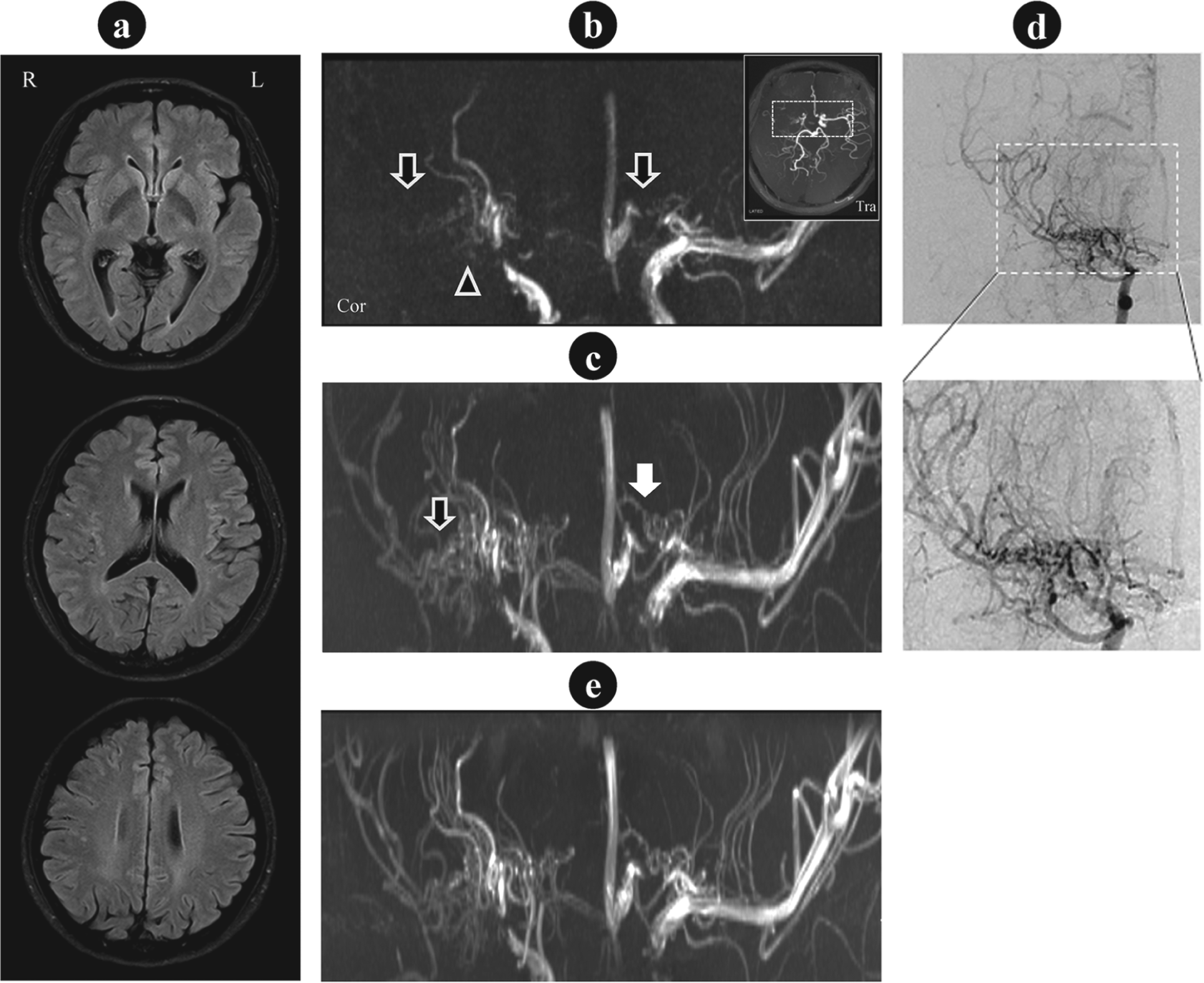
Magnetic resonance imaging (MRI) and digital subtraction angiography (DSA) images of a patient. (a) Fluid-attenuated inversion recovery (FLAIR) images at 3T MRI. (b) 3T magnetic resonance angiography (MRA) image within a white box in the axial maximum intensity projection (MIP) image. Note the undesired vessels were removed, showing complete occlusion (arrows) and a complex structure of the occlusive vessel segment (arrowhead). (c) 7T MRA image obtained at the first visit in coronal view. Connecting or collateral vessels in the MCA were clearly depicted. On 7T MRA, the white arrow indicates an anterior cerebral artery with connecting or collateral vessels, which are not visible on 3T MRA. (d) DSA dynamic images via right internal carotid artery injection. Below, the expanded view is presented for a direct comparison of the microvessels and collaterals with 7T MRA. (e) 7T MRA image obtained at the second visit, 18 months later. There was no difference in the microvessels between the first and second visits. (R, right; L, left; Tra, transaxial; Cor, coronal.).
Eighteen months after the first visit, a follow-up study was conducted using both 3T and 7T MRI to evaluate the progression of steno-occlusion of intracranial and/or extracranial arteries and the changes in the microvessels around the steno-occluded MCA (Figure 1e). Compared with those of the initial findings, the follow-up images showed no significant interval changes in MCA steno-occlusion and microvessels, including lenticulostriate arteries and collaterals. Normal blood circulation in the MCA territory was preserved with collaterals showing blood flow from the anterior cerebral artery (Figure 2a and 2b) and the posterior cerebral artery (Figure 2c and 2d), both of which were depicted using DSA. Similarly, 7T MRA clearly showed the blood flow from the small arteries of the collaterals that branch out from the anterior and posterior cerebral arteries.
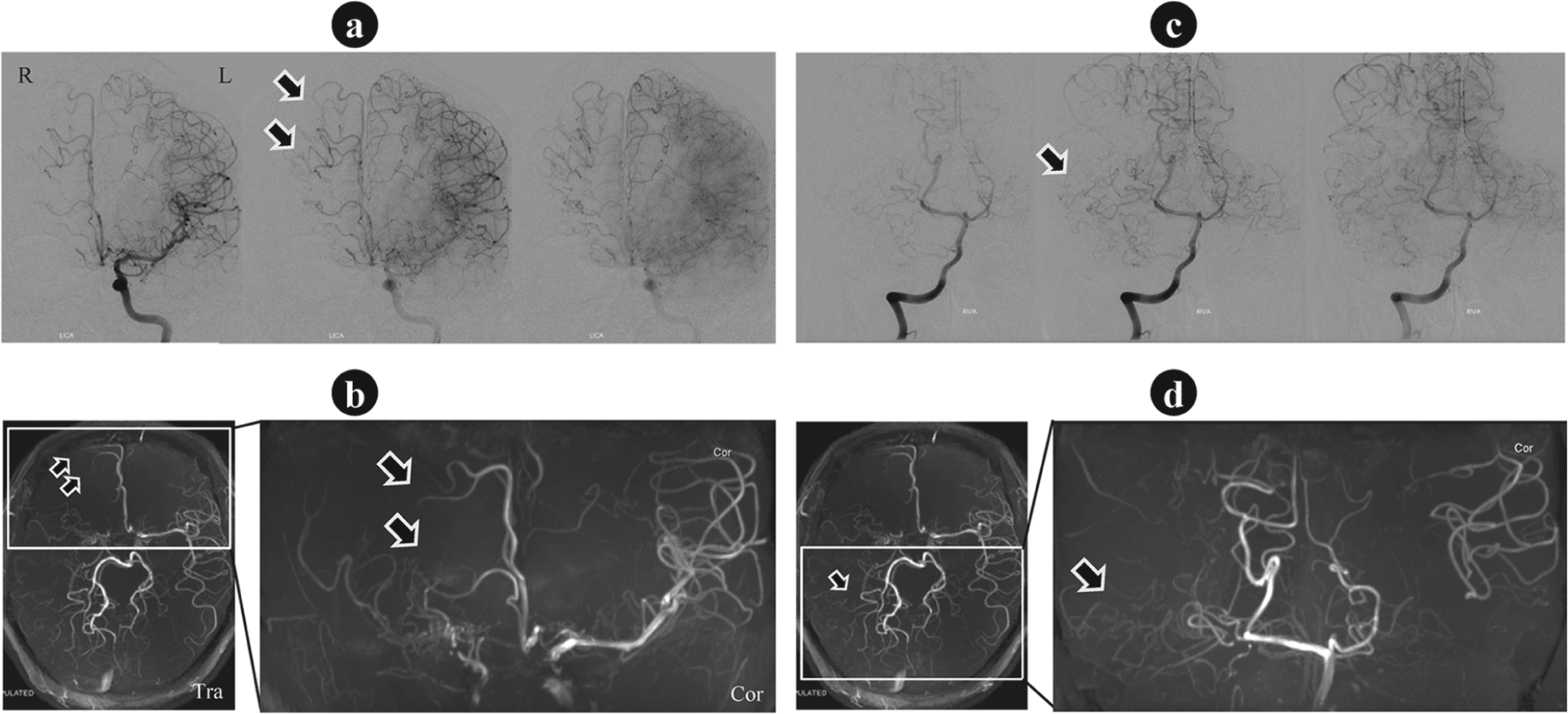
Collateral vessels from the anterior and posterior cerebral artery observed by digital subtraction angiography (DSA) and 7T magnetic resonance angiography (MRA). (a) DSA dynamic images via left internal carotid artery injection. (b) 7T MRA image with manual removal of the posterior cerebral artery and its branches for easy viewing of the region of interest. (c) DSA dynamic images via left basilar artery injection. (d) 7T MRA image with the anterior cerebral artery and its branches removed for easy viewing of the region of interest. There were collaterals supplying the territory of the middle cerebral artery, as observed by both DSA and 7T MRA images. (R, right; L, left; Tra, transaxial; Cor, coronal.)
Discussion
In this study, 7T MRA with a time-of-flight (TOF) sequence without contrast media was used to visualize microvessels proximal to the MCA, such as lenticulostriate arteries and presumed collaterals. The increased magnetic field results in longer T1 times of tissues, which improves the vessel-to-tissue contrast in TOF MRA in accordance with the increased signal-to-noise ratio that is obtainable with 7T MRI.5,6
Detection of microvessels proximal to the MCA in an asymptomatic patient with MCA steno-occlusion using a non-invasive method has not been reported. However, the present study demonstrated that this non-invasive technique of 7T MRA for evaluating microvessels provided valuable information on preservation of normal blood circulation from the ischemic insults in asymptomatic patients with MCA steno-occlusion. 7T MRA exhibited a microvascular image quality that was comparable with that of invasive imaging procedures, such as DSA, which may result in complications.4,7
In this study, we considered the possibility of moyamoya disease because of the presence of abundant microvessels proximal to the MCA. The diagnosis of moyamoya disease is based on a distinct arteriographic appearance characterized by steno-occlusion of the distal intracranial internal carotid arteries on both sides, extending to the proximal anterior and middle cerebral arteries. 8 Therefore, we performed a follow-up study but found no evidence of angiographic and anatomic changes, such as ivy signs, that could be indicative of moyamoya disease.
However, we believe that rather than atherosclerosis, moyamoya disease may be a cause of MCA steno-occlusion in this asymptomatic patient because an 18-month follow-up is too short to rule out the diagnosis of moyamoya disease. In addition, MRI images can be intrinsically sensitive to patient movement during the scan, especially when for microvascular imaging, for which a long scan time is necessary. An artifactual result was obtained (as shown in Figure 1c), but it did not affect the evaluation of vascular structural progress.
In conclusion, different imaging modalities are available to evaluate both collateral circulation and brain perfusion. Among diagnostic methods, although the findings of conventional lower-field MRA are somewhat poorer than those of DSA, MRI has been used most frequently because it is a non-invasive technique and aids the diagnosis of hypoperfused tissues and infarcts in patients. In addition, the increased sensitivity of ultra-high-field 7T MRI seems a promising candidate for observing microvascular abnormalities, such as those involved in collateral circulation and tissue status in patients with occlusive artery disease.5,6 We believe this is the first report demonstrating the recruitment of abundant microvessels around a steno-occluded MCA in an asymptomatic patient using 7T MRA, a non-invasive technique.
Footnotes
Declaration of conflicting interest
The authors have no relevant disclosures to make.
Funding
This work was supported by Gachon University Gil Hospital and the International R&D Program of the National Research Foundation of Korea funded by the Ministry of Education, Science and Technology of Korea [NRF-2011-0031541].