
Abstract
Peripheral artery disease (PAD) is a strong predictor of cardiovascular morbidity and mortality yet it is under-recognised and undertreated. General practitioners (GPs) are best positioned to detect patients with PAD. This article investigates awareness of PAD by GPs; the prevalence of screening for PAD and tools used for screening and diagnosis, in particular the ankle–brachial index (ABI); and the barriers to PAD screening and measurement of the ABI in the general practice setting. A cross-sectional survey of primary care practitioners was conducted between September 2011 and March 2012. A mail-out survey was distributed to 1120 GPs practising in Queensland, Australia: 287 (26%) responded; 61% of GPs reported screening for PAD; 58% of GPs reported ‘never’ measuring the ABI; and 70% reported using arterial duplex ultrasound as their first-line diagnostic tool. Equipment availability, time constraints and lack of training and skills were identified as the most significant barriers to screening and ABI testing. In conclusion, there are deficits in the utilisation of guideline recommendations relating to PAD screening and diagnosis by Australian GPs. Our data suggest that earlier detection of PAD may be achieved through GP education combined with increased access to ABI equipment or the availability of a more time-efficient test.
Keywords
Introduction
Atherosclerotic disease is the leading cause of morbidity and mortality in the western world and manifests as coronary artery disease (CAD), cerebrovascular disease (CVD) and peripheral artery disease (PAD). 1 As atherosclerosis tends to develop in multiple vascular beds, detection of disease in one vascular bed predicts disease elsewhere. 2
PAD affects 15.6% of Australians and the majority are asymptomatic.3,4 PAD carries a worse prognosis than CAD or CVD, with almost one in five patients with PAD expected to suffer a major cardiovascular event within 1 year. 2 In comparison, amputation is a relatively rare complication of symptomatic PAD, required by only ~2% of patients within 5 years of diagnosis. 5 The risk of cardiovascular disease associated with PAD can be minimised by early intervention with multiple preventive therapies, such as antiplatelet therapy, a statin, and an angiotensin-converting enzyme inhibitor.6–9
The ankle–brachial index (ABI) is a non-invasive and inexpensive investigation for PAD detection that can be easily measured by a general practitioner (GP) or nurse in the office setting. 10 The sensitivity of the ABI for PAD detection, reported to be 78%, is comparable to other commonly available tools used for PAD diagnosis. 11 International guidelines recommend use of the ABI for PAD screening and as the first-line test to diagnose PAD in symptomatic patients.5,12
PAD has long been under-diagnosed and disease in up to half of those affected by PAD is yet to be detected. 13 Reasons for this include the high prevalence of asymptomatic disease, inappropriate use of screening and diagnostic tools, and poor awareness of PAD. 14 International evidence suggests that current guidelines for PAD screening and diagnosis have not been successfully implemented in general practice; however, no research has been performed to evaluate the situation in Australia.15,16 The purpose of this study was to: (1) determine the awareness of PAD among GPs; (2) determine the prevalence of screening for PAD and tools used for screening; (3) identify the methods used to diagnose PAD and the prevalence of ABI testing for diagnosis; and (4) identify the barriers to PAD screening and ABI measurement for diagnosis experienced by GPs in Australia.
Methods
Study and survey design
This epidemiologic cross-sectional study involved a survey of GPs in North Brisbane and Townsville. Data were collected via a mail-out survey that was designed for this study. (Supplementary data, available online with this article vmj.sagepub.com) Survey content was informed by a review of the literature and consisted of 26 questions arranged in four sections: (A) GP demographics, (B) PAD awareness, (C) PAD screening, and (D) PAD diagnosis. A pilot study of the survey, including eight GPs not involved in the target population, was conducted prior to the initial mail-out.
Setting and participants
GPs were included in the study population if they were currently practising, regularly consulted with PAD patients, and registered with either GP Partners Northside or the Townsville GP Network. Surveys were mailed to the GP practices in return-addressed reply-paid envelopes. The study consisted of two rounds of survey distribution, the first of which was conducted between September and October 2011 and the second in February 2012. Those who responded to the initial survey were asked to discard the second copy.
This study was approved by the School of Medicine Internal Low Risk Ethics (SOMILRE) Review Panel, University of Queensland. SOM clearance number: 2011-SOMILRE-001. Participation in this study was entirely voluntary.
Statistical methods
Data were entered into Statistical Package for the Social Sciences (SPSS, IBM SPSS Statistics, V20.0) software and analysed using descriptive statistics. Differences in responses between selected demographic groups were analysed using the chi-squared test. All variables were reported as counts and percentages.
Results
Subject demographics
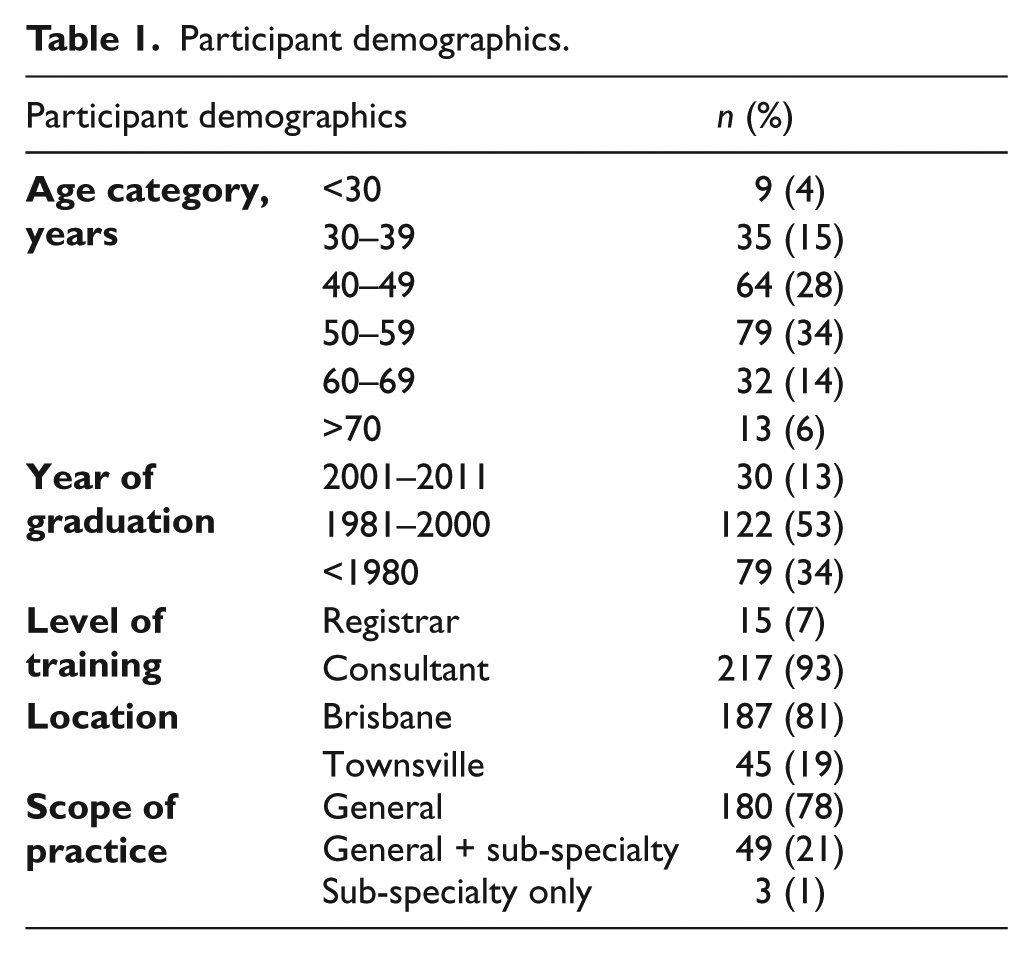
A total of 1120 GPs were invited to participate and 287 (26%) responded. Fifty-five responses were excluded, as those GPs reported not consulting with PAD patients, while 232 responses were analysed. Participant demographics are displayed in Table 1.
Participant demographics.
PAD awareness
The largest proportion of GPs (45%) estimated the prevalence of PAD among patients over 55 years to be between 10% and 20%; 25% of GPs estimated the prevalence as 20–30%, and a further 15% estimated the prevalence to be less than 10%. The estimated prevalence of asymptomatic disease varied; however, the majority (62%) estimated that over 40% of PAD patients were asymptomatic.
Estimates of the 1- and 5-year mortality rates from CAD and CVD and the risk of amputation for patients with PAD stratified by symptom status are displayed in Table 2. Estimates of the mortality rates from CAD and CVD were similar and revealed that symptomatic PAD was viewed as more serious than asymptomatic PAD. Regarding amputation risk, over half of the respondents believed that more than 10% of patients with intermittent claudication (IC) would require amputation after 1 year; and at 5 years, 82% of the GPs thought that more than 10% of patients would require amputation.
GPs’ estimates of the incidence of PAD complications.
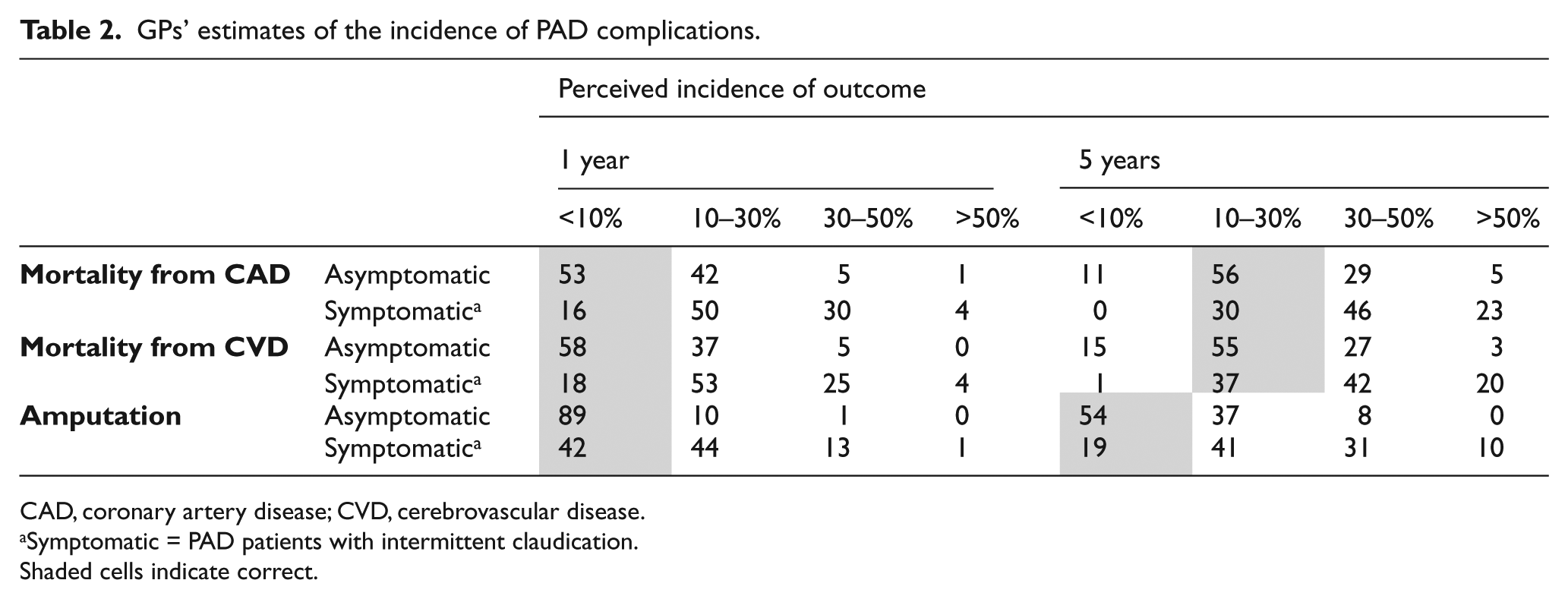
CAD, coronary artery disease; CVD, cerebrovascular disease.
Symptomatic = PAD patients with intermittent claudication.
Shaded cells indicate correct.
Screening
Only 15 respondents (6%) were aware of evidence-based guidelines relating to PAD screening and 142 (61%) respondents reported screening for PAD. Of those GPs who screen for PAD, the most common factors reported to prompt screening were symptoms of PAD and history of smoking or type 2 diabetes, each listed by more than 85% of the GPs.
Screening tests used by GPs included history and physical examination, each used by 98% of respondents, followed by ABI and arterial duplex ultrasound (DUS), which were used by 54% and 42%, respectively (Figure 1). A total of 27% of GPs who screened for PAD reported screening using history and / or physical examination only.
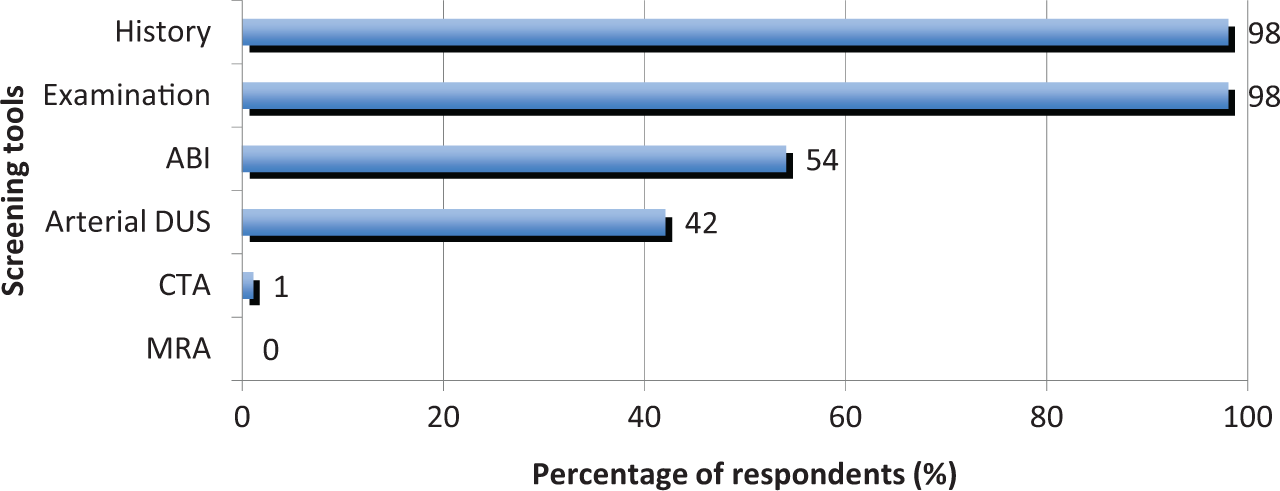
Screening tools nominated by GPs who screen for PAD. (ABI, ankle–brachial index; DUS, duplex ultrasound; CTA, computed tomography angiography; MRA, magnetic resonance angiography.)
Responses from the total cohort to questions about barriers to screening for PAD are presented in Figure 2. Time constraints and equipment availability were identified as the most significant barriers to screening, identified as moderate-major barriers by approximately two-thirds of respondents.
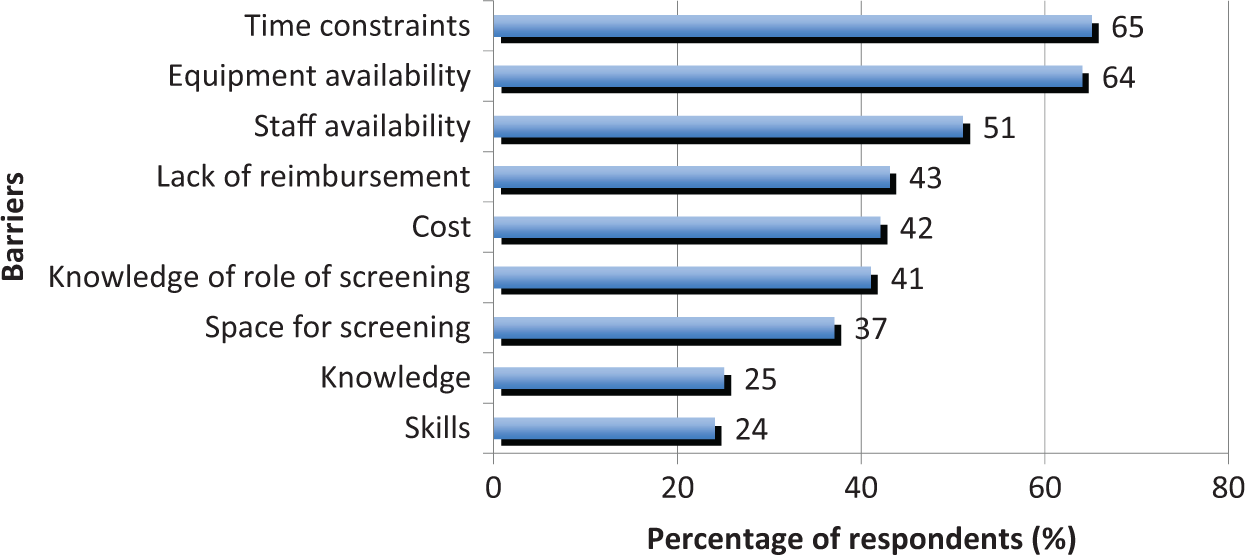
Factors nominated by respondents as moderate-major barriers to PAD screening.
Diagnosis
Only 11 (5%) respondents were aware of guidelines relating to PAD diagnosis. The tools nominated by GPs as necessary to make a diagnosis of PAD are displayed in Figure 3. History and physical examination formed part of the diagnostic work-up for almost all GPs (90% and 84%, respectively) and ABI and arterial DUS were each viewed as necessary by approximately two-thirds of GPs.
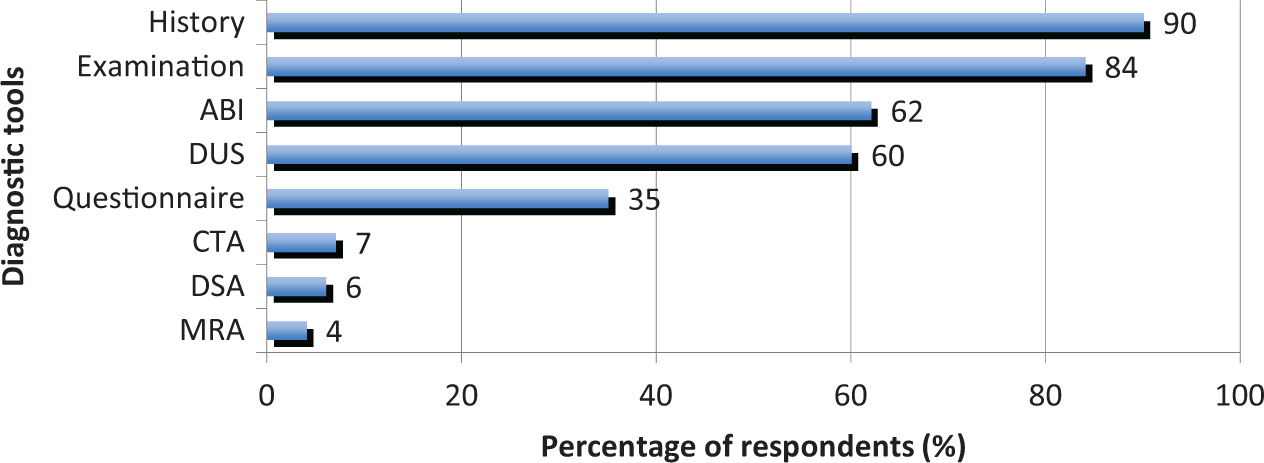
Diagnostic tools for PAD nominated by GPs. (ABI, ankle–brachial index; DUS, duplex ultrasound; CTA, computed tomography angiography; DSA, digital subtraction angiography; MRA, magnetic resonance angiography.)
When presented with a patient history and physical examination findings consistent with lower limb PAD, 70% of respondents indicated they would choose arterial DUS as their first-line diagnostic tool. Younger GPs (less than 40 years of age) were more likely to choose ABI as their first-line diagnostic tool and this association was statistically significant (χ2 (n = 228) = 9.67, p = 0.008, Cramer’s V = 0.206, std residual = 2.4).
Fifty-eight percent of the GPs surveyed reported ‘never’ measuring the ABI and less than 10% of GPs reported measuring the ABI daily or weekly. ABI measurements were performed approximately one-third each by the GP, the practice nurse, and the vascular laboratory.
Over half (57%) of respondents reported that the sensitivity of the ABI was ‘equal to’ or ‘less’ (not ‘much less’) than the DUS. ABI was viewed as costing ‘less’ or ‘much less’ than arterial DUS by two-thirds of respondents.
Factors reported to limit use of ABI measurement for PAD diagnosis are displayed in Figure 4. Lack of equipment, time constraints, lack of training and skills, and staff availability were reported as moderate-major barriers by over half of the respondents.
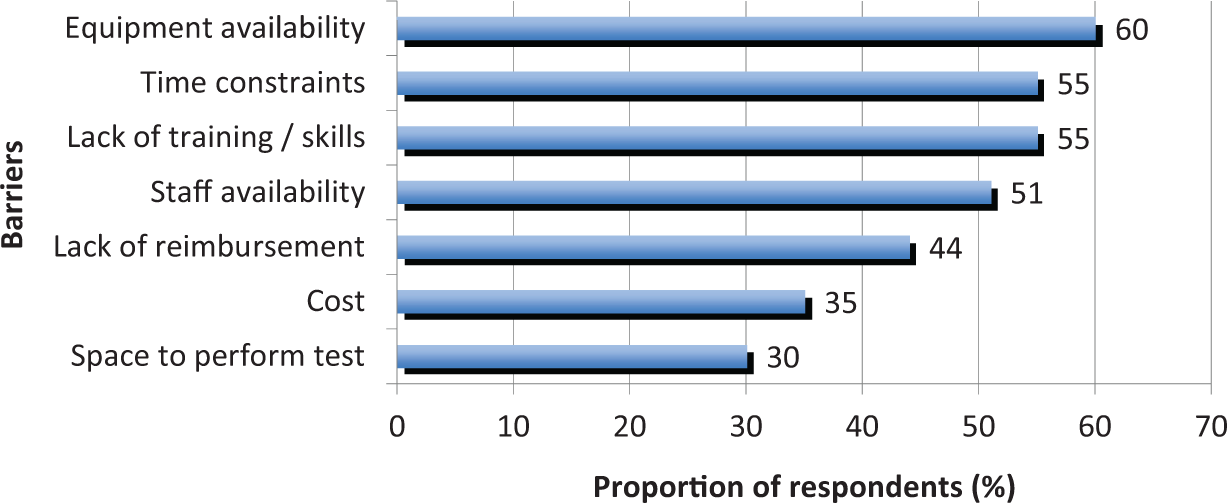
Factors reported by GPs as moderate-major barriers to ABI measurement.
Discussion
Summary
This study was designed to increase our understanding of the awareness of PAD among GPs and provide information on current screening and diagnostic practices. Such an evaluation of current GP practice in Australia has not been performed previously. The most significant findings demonstrated by this study are listed below.
GPs tended to overestimate the rate of cardiovascular mortality and amputation risk for PAD patients, and rated asymptomatic disease as less serious than symptomatic disease.
The majority of GPs screened for PAD but only a minority used the recommended screening test.
There is limited use of ABI assessment by GPs and arterial DUS was preferred as the primary diagnostic test for PAD.
Equipment availability, time constraints, staff availability and lack of training and skills were the most important stated barriers to PAD screening and ABI measurement.
Pleasingly, this survey has demonstrated that GPs are aware that PAD is common and associated with significant cardiovascular mortality. However, the overestimation of the incidence of PAD complications, particularly amputation risk, suggests that better education regarding the prognosis for PAD patients is required. It should be emphasised that in PAD patients, cardiac and cerebrovascular events are far more likely than amputation, pointing to the importance of secondary prevention of cardiovascular events.
Comparison with existing literature
Most GPs in our survey reported that they screened for PAD; however, over a quarter of GPs who screen for PAD utilised history and / or examination only and one-third of all study participants reported screening with an ABI. This compares favourably with data from a Swiss study that reported the prevalence of PAD screening with an ABI to be 20%. 16
Use of the ABI among general and specialist practitioners is likely to be limited by the ready availability of convenient alternative diagnostic tests, such as the arterial DUS. Most GPs in Australia never perform an ABI measurement and those who do seldom measure it. These findings are consistent with data from the United States, where approximately 70% of GPs reported ‘never’ measuring the ABI. 15 Our study clearly demonstrated that GPs show a preference for arterial DUS over ABI as the first-line tool for PAD detection and this is despite awareness that the ABI costs less than the arterial DUS and has comparable sensitivity. In Australia, an arterial DUS scan costs approximately three-times that of an ABI and requires referral to a vascular laboratory.17,18 A study by Jack reported that 38% of arterial DUS scans performed prior to specialist referral were considered by vascular specialists to be unnecessary. 19 Despite circumventing many of the barriers to ABI use experienced by GPs in Australia, the current reliance on arterial DUS for PAD detection mandates exploration of the barriers to ABI use and strategies to address these barriers.
The most significant reported barriers to ABI use included equipment availability, time constraints, staff availability and lack of training and skills. These factors are in contrast to data reported by Mohler et al. from the United States, which identified time limitation as the only moderate-major barrier reported by the majority of respondents, while equipment availability was not considered a significant barrier. 15
It is evident from our data that appropriate equipment for ABI measurement is not available to the majority of GPs. Even though ABI measurements using appropriate equipment attract a Medicare rebate (providing waveforms are also recorded), a large proportion of GPs identified lack of reimbursement as a moderate-major barrier, suggesting that improved awareness of the criteria for reimbursement, in association with greater equipment availability, may increase access to ABI testing. 17
Time limitation is consistently identified as a significant barrier to ABI use throughout the literature. Existing data indicate that GPs measure an ABI in 15 minutes or less, the same amount of time allocated for a standard GP consultation in Australia. 15 The automated oscillometric measurement of the ABI is a novel technology that is quick and easy to perform in the office setting and demonstrates high accuracy for detecting PAD. 20
Our study identified that many Australian GPs do not feel adequately trained to measure an ABI. Mohler et al. found that ABI utilisation by GPs significantly increased 1 year following a practical educational intervention. 15 This suggests that a similar program in Australia may aid in addressing the skills deficit in ABI measurement experienced by Australian GPs.
Limitations
Our study is limited by a relatively small sample size and response rate. Selection of Queensland GPs may limit the generalisabiliy of the results due to interstate differences in medical school and GP training. The use of survey questions with pre-designed answers restricted participant responses to the options provided, potentially failing to include the respondent’s true answer.
Implications for practice
In conclusion, this study has identified that international guideline recommendations relating to PAD screening and ABI measurement for the diagnosis of PAD are not currently widely implemented by Australian GPs. The greater understanding of the barriers to screening and ABI use provided by this study suggest that earlier detection of PAD could be effectively facilitated by an appropriately designed education program in combination with greater access to ABI equipment or the availability of a quicker and easier automated ABI test.
Footnotes
Acknowledgements
From the National Health and Medical Research Council funded Centre of Research Excellence for Peripheral Artery Disease. JG holds a Practitioner Fellowship from the National Health and Medical Research Council, Australia (1019921) and a Senior Clinical Research Fellowship from the Queensland Government.
Declaration of conflicting interest
The authors declare there are no competing interests identified for this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.