
Abstract
Klippel–Trenaunay syndrome (KTS) is a congenital malformation syndrome with prominent vascular anomalies. A persistent embryonic vein (PEV) may be located on the affected leg(s) of patients with KTS. Our understanding of PEVs of the legs is limited and their nomenclature is confusing. The objective of this study was to obtain further insight in the prevalence, nomenclature and etiology of PEVs of the legs in KTS and to propose a standardized description of anomalous leg veins in KTS. We investigated 70 KTS patients for the presence of PEVs (lateral marginal vein, LMV) of the legs by duplex ultrasonography. We performed histopathological analysis of a surgically excised PEV (LMV) of a typical KTS patient, and we conducted an extensive literature study. Duplex ultrasonography showed LMVs in 12/70 (17.1%) patients. The terms used to describe PEVs in the leg are quite variable, while indicating only two types: lateral marginal vein (LMV) and persistent sciatic vein (PSV). The histology of the excised LMV showed remarkable similarity with that of varicose veins found in the general population. In conclusion, the prevalence of LMVs in our KTS cohort is 17.1%. Two PEVs can be found in the legs and we propose nomenclature based on anatomical criteria, thereby using only the terms persistent lateral marginal vein and persistent sciatic vein, combined with the patency of the deep venous system. We hypothesize that PEVs are most likely caused by a genetic defect leading to abnormal venous pattern formation, which is further supported by our histopathological findings.
Keywords
Introduction
Klippel–Trenaunay syndrome (KTS) is a congenital malformation syndrome characterized by variable combinations of vascular malformations (capillary, venous and lymphatic) and localized disturbed growth of bone and/or soft tissues.1,2 As a result of these abnormalities, signs and symptoms may arise such as pain, leg length discrepancy, erysipelas, venous thrombosis and pulmonary embolism.2 –8
Embryonic leg veins usually regress before birth, but in KTS a persistent embryonic vein (PEV) may be located on the lateral aspect of the affected leg. Known PEVs of the leg are the lateral marginal vein (LMV) and the persistent sciatic vein (PSV).5 –12 The nomenclature can be confusing because various terms are used to indicate the same aberrant leg vein in KTS (e.g. ‘vein of Servelle’, ‘Klippel–Trenaunay vein’, ‘lateral marginal vein’), which hampers comparisons between studies.5 –12 Furthermore, the etiology of persistent veins has been studied mostly in the brain.13,14 Understanding leg PEVs may help to further clarify the etiology of congenital vascular malformations.
The goal of our study therefore was to propose a uniform nomenclature for leg PEVs in KTS and gain more insight into their prevalence and etiology.
Methods
Between May 2006 and May 2007, a total of 105 KTS patients were seen at our dedicated tertiary vascular malformation center. The diagnosis of KTS was made by our team of experts using the International Society for the Study of Vascular Anomalies (ISSVA) classification system.2,8
Seventy patients agreed to undergo duplex ultrasonography at our facility, performed by two experienced vascular ultrasonographists, to determine whether a LMV was present. In the remaining 35 patients we evaluated their medical files for any mentions of LMVs. As surgical excision of PSVs is more rarely indicated and visualizing this vein with ultrasonography is not always reliable, we chose not to address the PSV during imaging and to focus on the LMV. There was no age or sex selection. The study was approved by our Medical Ethics Committee and all patients gave written informed consent.
We also performed histopathological analysis of a surgically excised LMV in a KTS patient. This vessel segment, measuring 47 cm in length, was fixed in buffered formalin and embedded in paraffin. Subsequently, 5 µm sections were stained with hematoxylin & eosin, Elastica van Gieson and Pico-sirius red, and examined with light microscopy.
Furthermore, we performed a literature search using PubMed, EMBASE, and Google Scholar (1900 to 2012). MeSH terms and keywords used for the search were: embryonic vein, embryonal vein, lateral marginal vein, sciatic vein, Klippel–Trenaunay syndrome and Klippel–Trenaunay–Weber syndrome. All references of relevant publications were hand searched for additional publications. A paper was considered relevant if it dealt with a PEV and one or more of the following combinations: (1) KTS; (2) hypotheses on etiology; (3) nomenclature; (4) embryogenesis; and (5) imaging techniques. All abstracts were evaluated for relevance by two independent authors (CEUO, DAYA). If in doubt, the complete publication was examined. If still unresolved, one of the other co-authors was consulted.
Results
Prevalence of LMV in 70 KTS patients
Of the 70 patients who underwent a duplex ultrasound exam, 11 (15.7 %) had a unilateral LMV and 1 (1.4%) a bilateral LMV in addition to their capillary-, venous- and/or lymphatic malformations.
A LMV (unilateral or bilateral) was mentioned in eight patients out of 35 (22.8%) who did not participate in the ultrasound study.
Case report and histology
An 11-year-old boy, previously diagnosed with KTS and a LMV in the right leg, presented with pain in the affected limb. Physical examination showed varicose veins on the lateral side of his right leg, combined with a reticular capillary malformation. The affected lower extremity was longer than the contralateral one by 1 cm and showed an increase in girth.
Duplex ultrasonography showed an extensive venous malformation around the knee extending both proximally and distally. The popliteal vein was widened, and the deep venous system was competent and open. There was an increase in flow in the femoral vein upon manual occlusion of the LMV on the lateral aspect of the leg just above the knee, indicating a connection between the LMV and the deep venous system. Magnetic resonance imaging (MRI) confirmed the extensive venous malformation and ascending phlebography showed the enlarged LMV (Figure 1).

MRI and phlebology: An extensive, tortuous low-flow venous malformation, located in the subcutaneous fat, muscle fascia, in and between muscles, and bone.
Because of the persisting pain, the LMV was excised, which was considered safe due to the patent deep system. Other treatments including compression and sclerotherapy had been unsuccessful due to the large size of the vein. However, pain persisted and the surgical scar over the lateral side of the leg became hypertrophic.
Histopathological analysis of the excised persistent embryonic vein was performed in the hope of gaining insights into the reasons for insufficiency of this vessel (at such an early age) and into possible etiological factors. Our examination showed significant changes in collagen, elastin and smooth muscle contents of the vessel wall. These findings in an overall markedly dilated vessel were comparable to those seen in varicose veins in the general population (Figure 2). 15
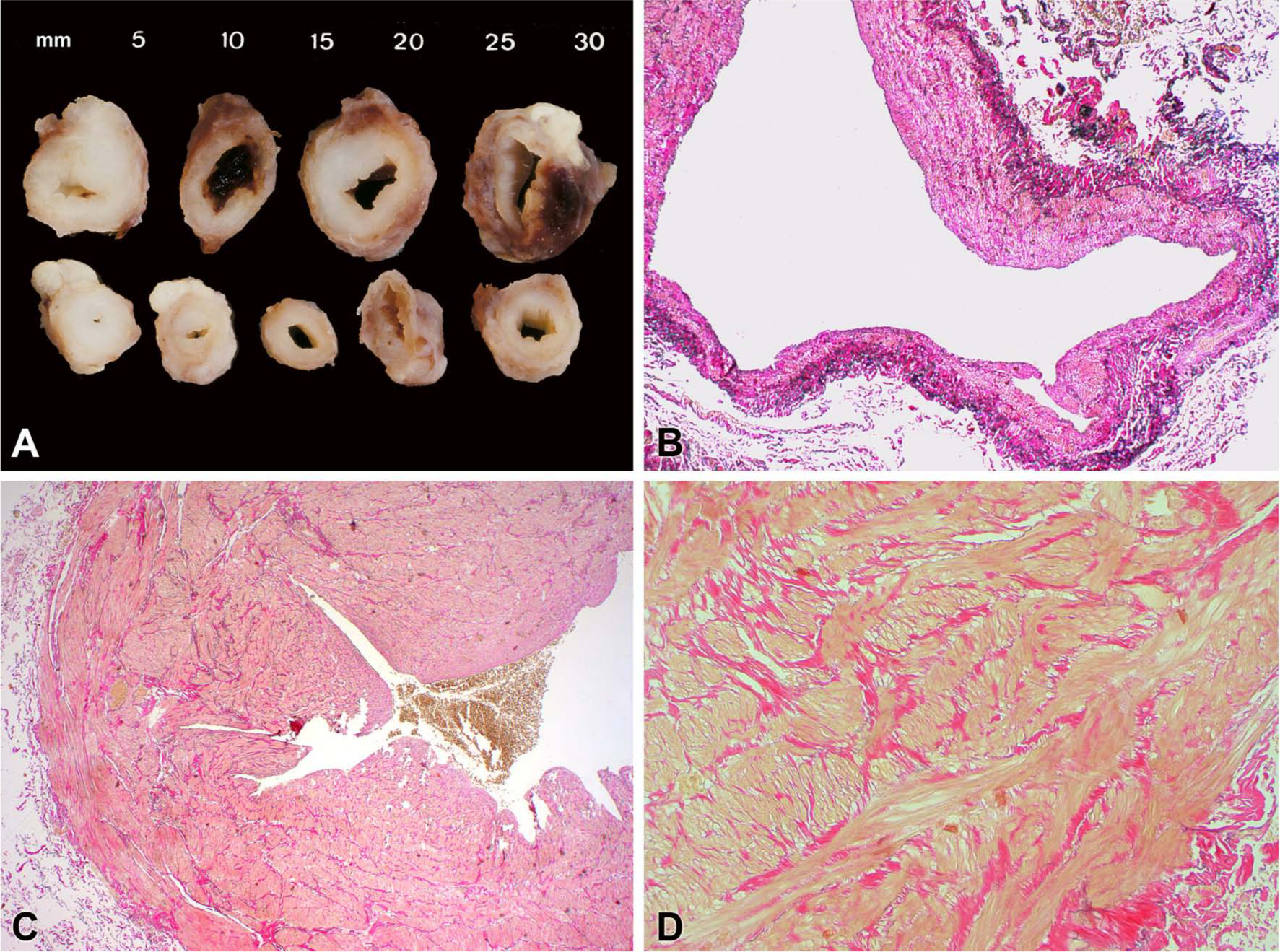
Pathology specimen of the resected vein. (A) Considerable variation in wall dimensions, ranging from irregular thickening with subtotal obliteration of the lumen to varicose dilatations with a thinned wall. Other segments appeared almost normal. No thrombus was found. There were no valvular structures discernible at the level of the cross sections. (B) Varicose segments in which the media was focally almost absent, apart from some sparse remaining smooth muscle cells, which was covered by thickened intima. There was increased elastin content mainly at the outer border of the wall. (C) Stenosed segments showed irregular cushion-like thickening (1–3 mm) of the media and an inconspicuous intima which was lined with a cobblestone type of endothelium. (D) In the media, hypertrophied bundles of smooth muscle were haphazardly arranged and embedded in dense collagen. A normal pattern of alternating layers of smooth muscle could be found in the grossly normal-appearing segments, but was almost absent in the segments with thickened wall.
Discussion
Nomenclature
The persistent LMV and the PSV are the only two PEV vein types that are found in the leg. The LMV is a superficial vein, while the PSV is part of the deep venous system. Both veins may occur in KTS5 –12 and may be associated with both normal and anomalous deep venous systems.3,9 –12,16 –19
An international interdisciplinary anatomical consensus was reached in 2002 and specifically named the ‘sciatic vein’, defining it as a deep vein of the posterior thigh perforators, lying along the midline of the posterior thigh and running along the sciatic nerve.20 –23 The sciatic vein should be regarded as ‘the main trunk of the primordial deep venous system’.20 –23
The same consensus defined the LMV as a superficial vein.20 –23 Normally, the LMV regresses before birth. Its remnant, the lateral venous system, extends from the dorsal venous arch of the foot to the lateral thigh and consists of all superficial veins on the lateral leg and thigh. These superficial veins are connected to tributaries of the great saphenous vein and small saphenous vein through communicating branches.9,20 –23
In spite of the consensus, in the pertinent literature five different names are used to indicate these two PEVs (Figures 3 and 4). A lateral marginal vein is also called ‘vein of Servelle’, ‘Klippel–Trenaunay vein’ and ‘lateral venous anomaly’, while a PSV is also referred to as a ‘lateral venous anomaly’.3,5 –12,18,24 –32 This variation in names hampers comparisons between studies.
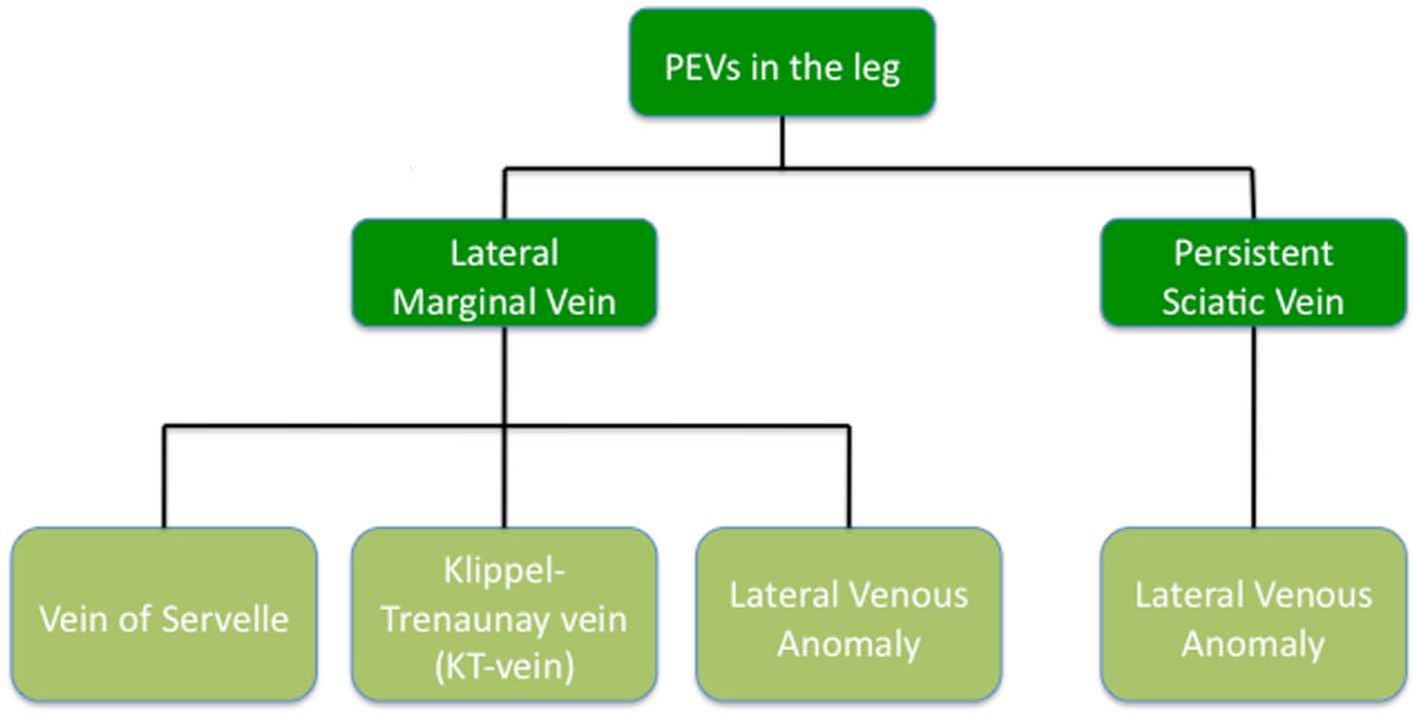
Terms used in the literature to indicate persistent embryonic veins of the leg.
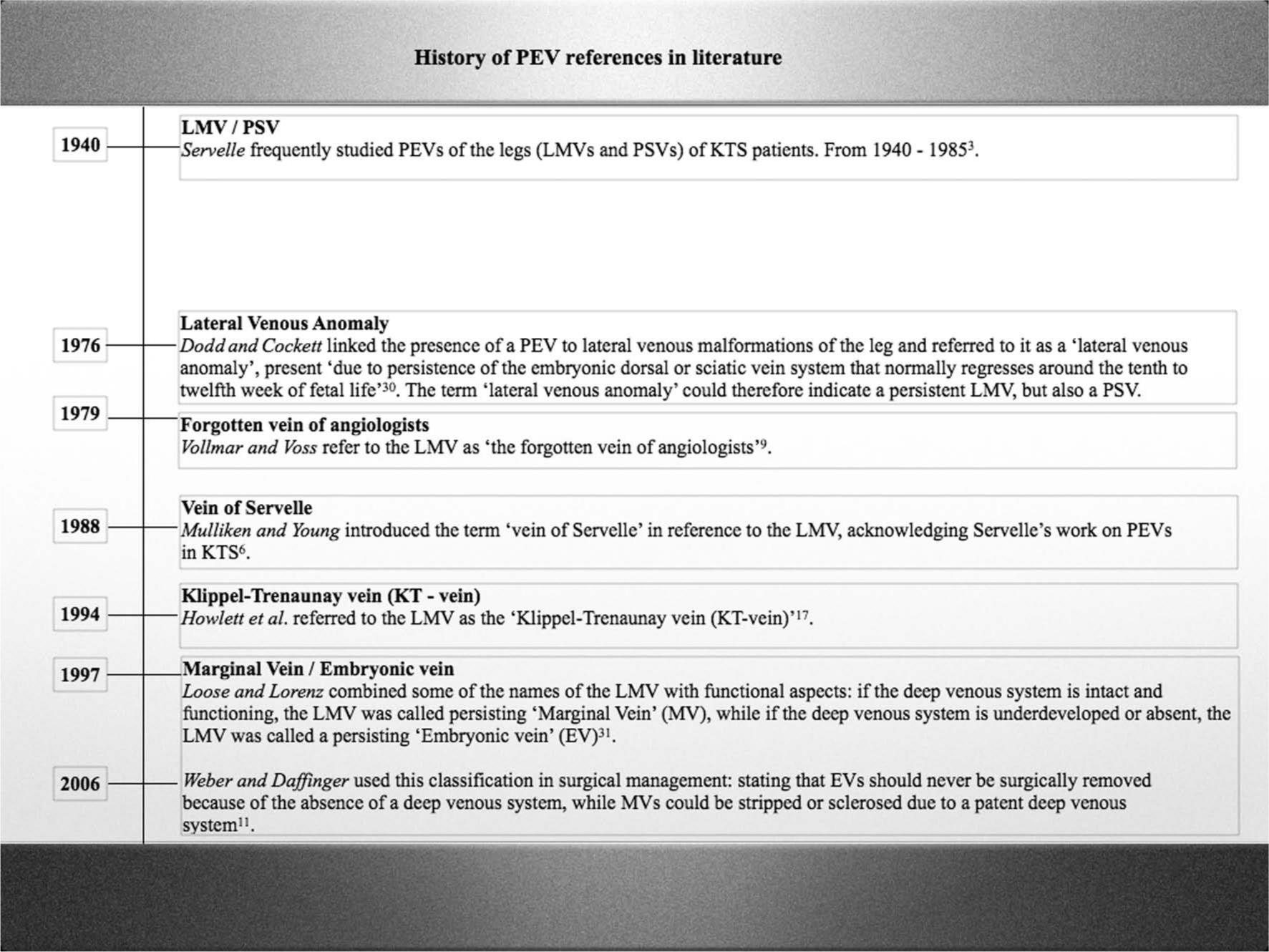
Timeline of persistent embryonic vein references in the literature. (PEV, persistent embryonic vein; LMV, lateral marginal vein; PSV, persistent sciatic vein; KTS, Klippel–Trenaunay syndrome).
We propose to name PEVs of the leg based on anatomical criteria, thereby only using the terms ‘persistent lateral marginal vein’ and ‘persistent sciatic vein’, and to always include information on patency of the deep venous system. This provides a clear, uniform classification based on international anatomical consensus,20 –23 and information on whether surgical intervention is possible as deep venous insufficiency precludes this.9 –11,17,19,26,33
Prevalence
The reported prevalence of persistent embryonic veins in the legs of KTS patients ranges from 9% to 68%.3,8 –10,16 –19,33 –35 These differences are due to small study groups and variations in nomenclature, diagnostic methods used and criteria for patient acquisition. Leg PEVs have also been described in other entities such as (presumed) Proteus syndrome 24 and, rarely, as an isolated lesion.9 –12,25
Difficulties in accurately imaging the deep venous system might also explain the high incidence of deep vein anomalies in KTS reported in the past. Patency of the deep venous system can be determined by ultrasonography, especially when performed by experienced ultrasonographists.11,17 When patency is confirmed, phlebography is advised prior to surgical intervention.9 –11,19
However, both imaging techniques have drawbacks. For instance, ultrasound studies have shown that a previously diagnosed hypoplastic deep venous system became competent and open after compression of a LMV just above and just below the knee. 17 Phlebography, likewise, not always accurately visualizes the deep venous system, as it is difficult to fill a patent deep venous system adequately with contrast dye when there is a concomitant large superficial venous channel present leading to dilution of contrast and flow effects. 17
The prevalence of LMV in our study group in patients who received ultrasound was 17.1%; however, in the group that declined examination, a LMV was described in 22.8% of their patient files. As the main reason for declining ultrasound in that group was pain or severe complaints of the leg, there might be a direct relationship between physical complaints, and the presence and extension of a PEV.
Etiology
Embryogenesis
It has been previously reported that the embryonic dorsal or sciatic vein system normally regresses around weeks 10 to 12 of fetal life, but evidence from human studies is lacking.10,19,30 A study conducted on the limbs of rabbit embryos in 1906 by Lewis showed that the sciatic vein is the second leg vein generated during embryogenesis (the first being the lateral/posterior fibular (peroneal) vein) and consists of the anterior tibial and primitive fibular veins. In rabbits, the proximal section of the sciatic vein regresses after the femoral anastomosis near the knee has formed. The sciatic vein eventually only comprises the collateral circulation of the thigh. A homology between the cephalic (arm) and the sciatic vein was suggested. It remains uncertain to what extent the findings can be translated to humans. 36
Hypotheses
We found limited information in the literature with regard to the etiology of PEVs in the legs. Usually, only outdated hypotheses and no new insights were presented.9 –11,18,19,27 –30
Servelle hypothesized that the sciatic vein does not regress when the superficial femoral vein (distal part of the femoral vein) is occluded and, hence, serves as the main venous outflow tract. 3 In this way, these veins may persist and serve as a substitute channel for obstructed deep veins, atresia of iliac veins, 37 and undeveloped or absent femoral or popliteal veins.3,11,28
Like others, we believe that Servelle’s hypothesis on the etiology of PEVs is too mechanistic, as PEVs have also been described in the presence of a patent deep venous system.3,9 –11,18,27 –29
Another explanation we considered is that the embryonic vein serves as a main venous outflow tract, causing other veins to become smaller in size because of reduced flow. This suggests that there is a primary localized dysplasia of the PEV, which is not present in other veins. However, we have been unable to find support for this theory. Nonetheless, we do think a genetic defect is the most likely explanation, as we will explain further on.
Histology
As mentioned before, histopathological reports of persistent embryonic veins are very rare and in most instances deal with PEVs in the brain. Concerning those, it was noted that cerebrovascular malformations morphologically resemble the primitive venous channels of the early embryonic cerebrovascular system. 13
The prominent endothelial cell lining in these brain PEVs was similar to that of veins of human fetuses of 11–16 weeks of gestation (45–110 mm, respectively), which may be an indication for the stage at which these PEVs arise.13,36 –40 If brain PEVs develop at Carnegie stage 23 (± 8 to ± 9 weeks, 20 mm) and do not regress after 14 weeks of gestation (> 80 mm), which occurs in the majority of occasions, the embryonic character of the veins is obvious.13,36 –40 If PEVs are formed at a later stage, a more marked structural maturity is seen in the flatter endothelium. 13 However, the etiological hypotheses of PEVs of the brain cannot be applied to the leg, since conditions in the leg, such as the venous pressure, differ significantly from those in the brain. The PEVs in brain arteriovenous malformations are subjected to arterialization, in contrary to the PEVs of the leg.
We performed histopathological examination of an excised LMV to gain additional insights into the etiology of leg PEVs. We found that its histology is remarkably similar to varicose veins in the general population. This could support a genetic cause rather than a mechanical cause because genetic factors are known to strongly contribute to varicose veins. 15
There is abundant evidence from animal studies that venous patterning is under genetic control.37,40 –43 Thus, we think that the vascular malformations defining KTS are caused by abnormal venous pattern formation due to genetic defects that may or may not be present in a mosaic state. The PEV likely persists because normal pattern formation, which includes its regression, is interrupted. The abnormal flow patterns that result may cause the veins to dilate, leading to varicosities later in life. A primary abnormality of the vessel wall is therefore not a prerequisite, which is consistent with our histopathological findings.
Conclusions
Two types of PEVs are found in the legs and we propose that their names should be based on anatomical criteria, thus only using the terms persistent lateral marginal vein and persistent sciatic vein. Information on patency of the deep venous system should be included so as to inform treatment decisions because surgical intervention is precluded when the deep venous system is insufficient. The frequency of LMVs in our KTS cohort as examined with ultrasound is 17.1%. We suggest that PEVs are most likely caused by a genetic defect leading to abnormal venous pattern formation, which is further supported by our histopathological findings.
Footnotes
Acknowledgements
We thank Hanny Vriends for her help preparing this review, and Roelof-Jan Oostra for providing the fetal length table. MvS is supported by the GROW School for Oncology and Developmental Biology.
Declaration of conflicting interests
The authors declare no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.