
Abstract
We describe a step-by-step instructional ‘how to’ case of trans-radial bilateral iliac stenting using a 5-Fr guide sheath in a symptomatic patient to illustrate an alternative to common femoral artery access.
Introduction
We describe a case of trans-radial bilateral iliac stenting using a 5-Fr guide sheath in a symptomatic patient to illustrate an alternative to common femoral artery access.
Case report
A 68-year-old man with severe bilateral thigh claudication after walking about 20 meters (Fontaine IIb) that had failed medical management including exercise, aspirin and cilostazol was brought for angiography and possible intervention. His symptoms were severely limiting his activity and lifestyle. His ankle–brachial index (ABI) was 0.48 on the right and 0.54 on the left. He had undergone right femoral-popliteal polytetrafluoroethylene (PTFE) bypass in 2003, with a revision of the distal anastomosis in 2005 secondary to a large popliteal cyst. He had undergone right common iliac artery (CIA) stenting in 2009 for severe thigh claudication. He also had poorly controlled hypertension and untreated dyslipidemia. A computerized tomography (CT) angiogram (Figures 1–3) showed a 50% stenosis of the right CIA proximal to a stent, a patent right CIA stent, severe stenosis of the left CIA, and bilateral occluded superficial femoral arteries.
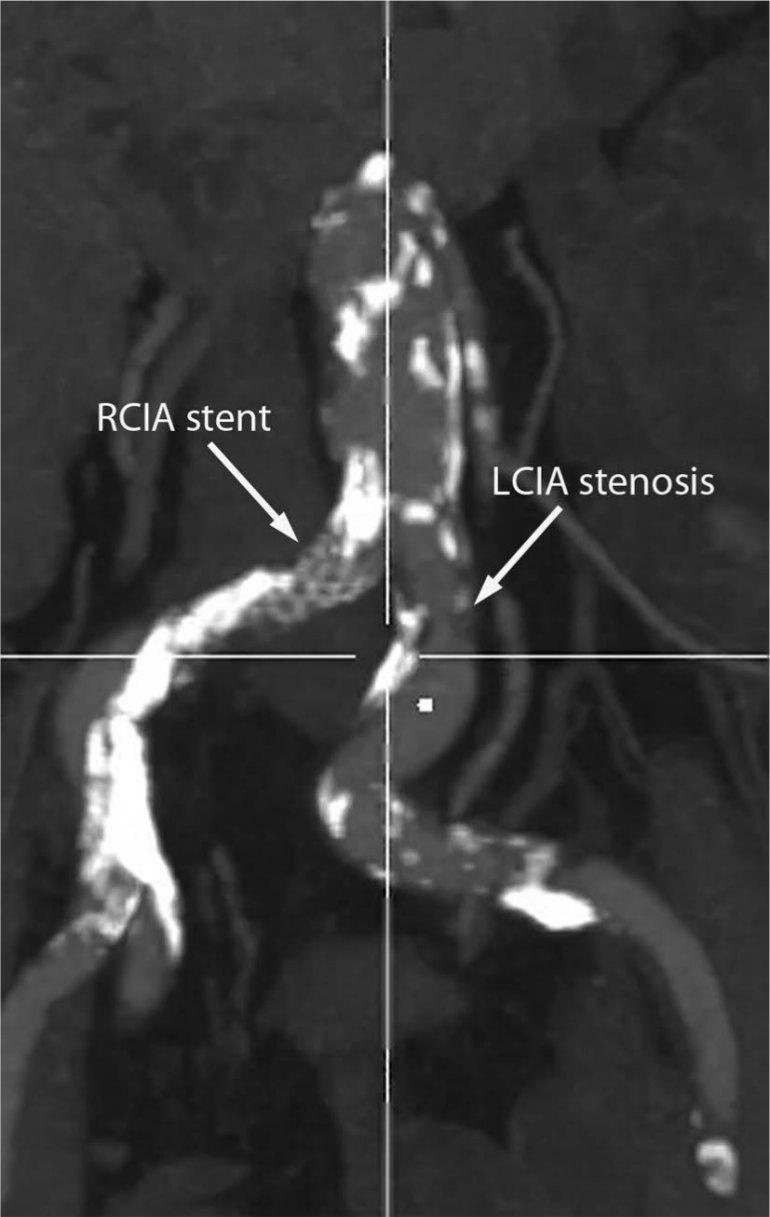
CT angiogram showing a previously placed right common iliac artery (RCIA) stent and a proximal left common iliac artery (LCIA) stenosis.
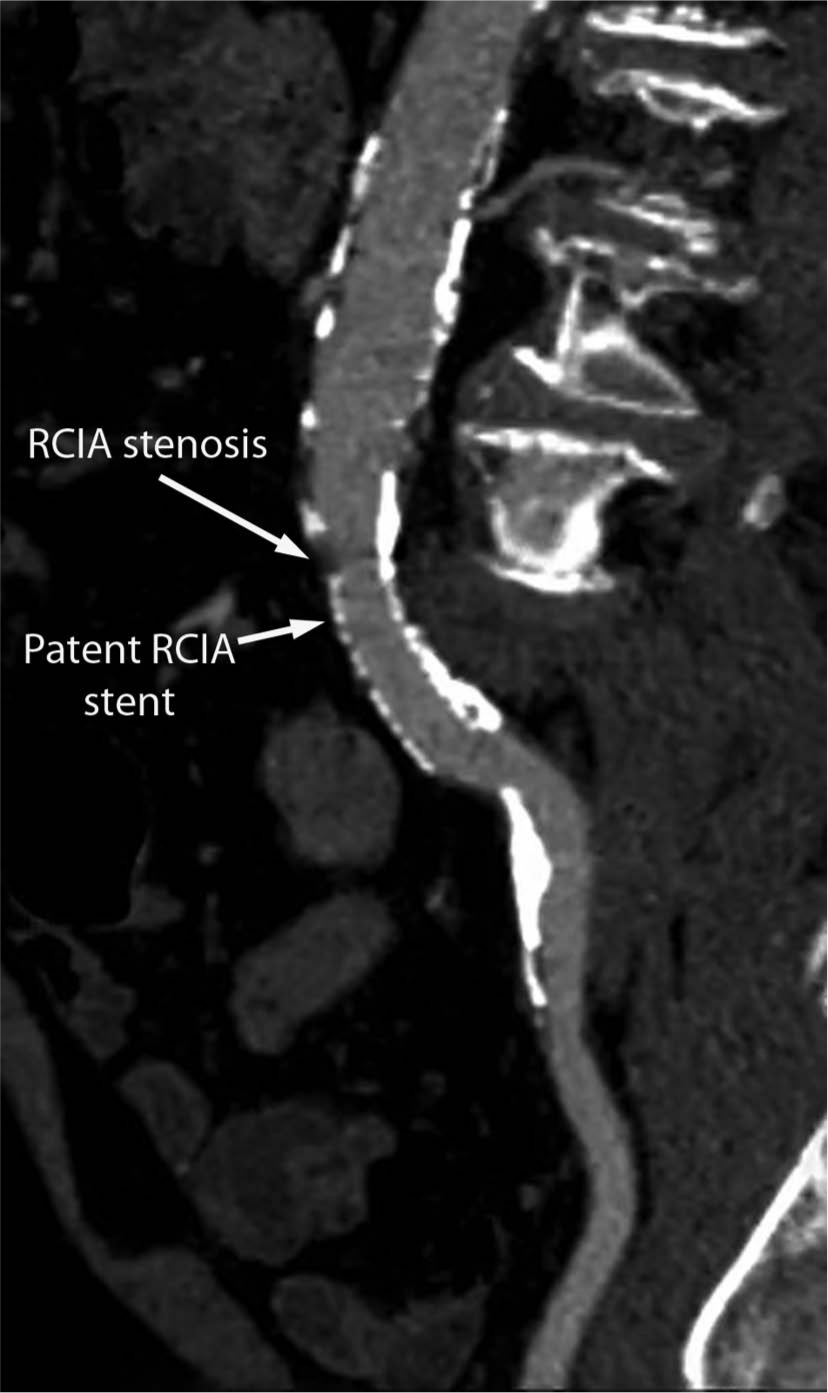
CT angiogram of the right common iliac artery (RCIA), showing stenosis proximal to a previously placed stent.
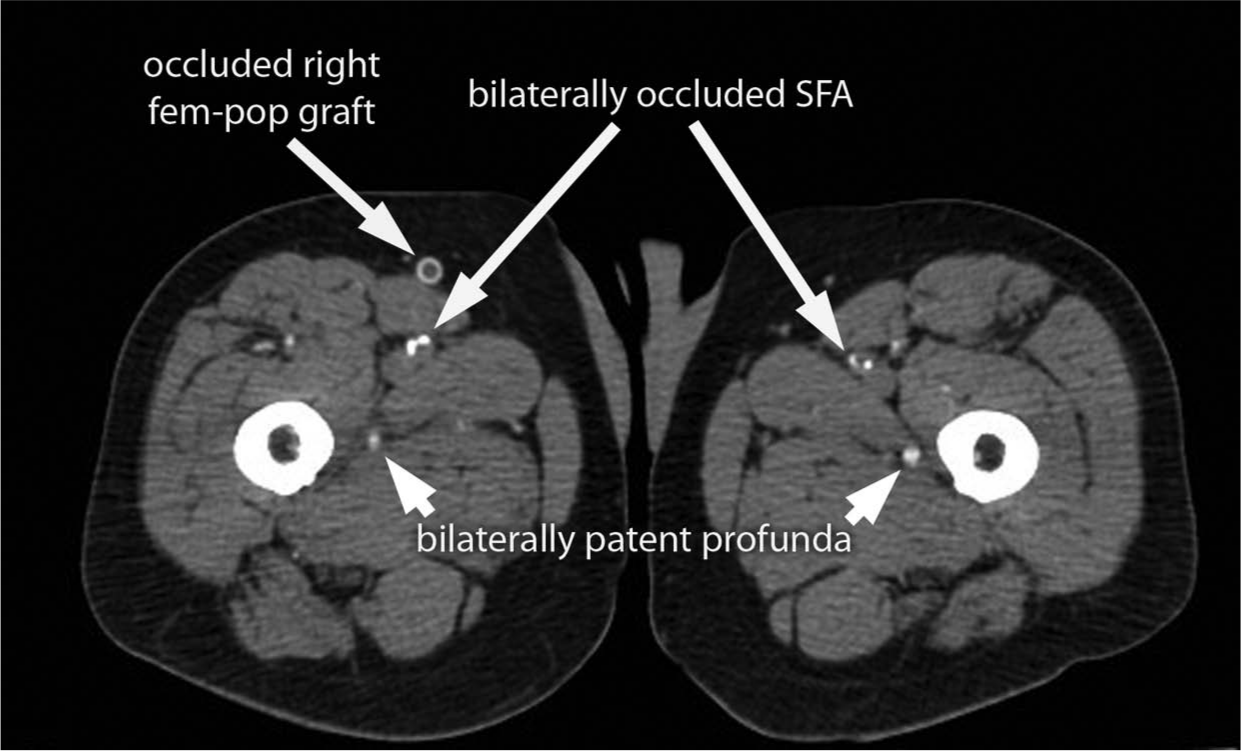
CT angiogram showing bilaterally occluded superficial femoral arteries (SFAs) and occluded right fem-pop bypass graft with patent profunda arteries.
Angiography
Trans-radial artery access was preferred over the trans-femoral approach for angiography because of the patient’s severe superficial femoral artery disease that was evident on CT angiography (Figure 3). Any complications of common femoral artery (CFA) access could potentially embarrass critical distal limb flow being provided by the profunda femoris artery.
Invasive angiography was performed via the right radial approach using a 5-Fr/11-cm sheath (Terumo, Tokyo, Japan). Catheter exchanges were done with a 260-cm long 0.035-in J-tipped guidewire (Boston Scientific, Natick, MA, USA). A 110-cm long 4-Fr pigtail catheter was used for infrarenal aortography with runoff (Figure 4). The angiogram demonstrated severe stenosis of the proximal left CIA and moderate to severe stenosis of the right CIA proximal to a previously placed stent.
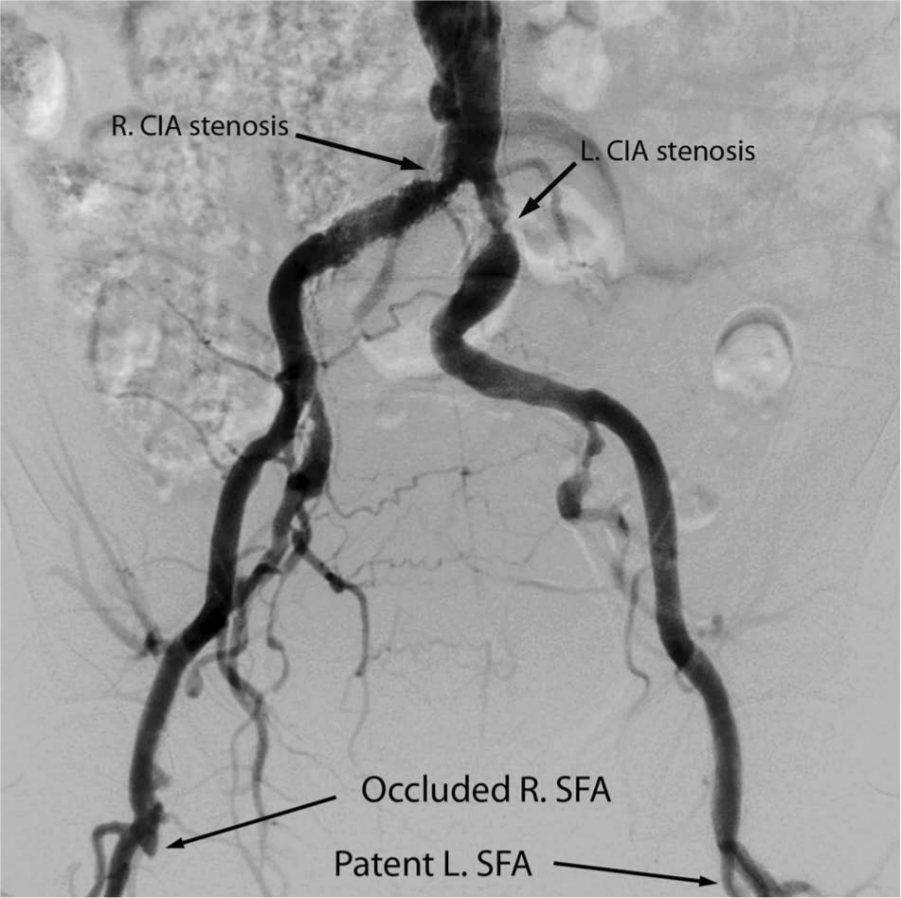
Distal aortic angiogram with runoff showing severe proximal left common iliac artery (LCIA) stenosis and moderate to severe proximal right common iliac artery (RCIA) stenosis proximal to a previously placed stent. (SFA, superficial femoral artery.)
The pigtail catheter was exchanged for a 125-cm long 4-Fr multipurpose (MP) (Cordis, Miami, FL, USA) catheter using the 0.035-in J-tipped guidewire. To establish hemodynamic significance, the right CIA stenosis was crossed with a 0.18-in × 300-cm long guidewire (Roadrunner; Cook, Bloomington, IN, USA). The MP catheter was advanced over this guidewire, across the right CIA lesion and a 12 mmHg hyperemic (following 25 mg of intra-arterial papaverine) mean trans-lesional gradient was documented on pullback of the catheter to the abdominal aorta. Care was taken to flush the catheter with non-heparinized saline prior to administering papaverine as papaverine will precipitate in heparin-containing solutions. The treatment 1 plan for this patient’s limiting chronic claudication was to improve the inflow to the legs, by treating both common iliac arteries.
Intervention
The 4-Fr MP catheter was removed over the 0.035-in J-tipped guidewire (Boston Scientific). The 5-Fr/11-cm right radial sheath was then exchanged for a 5-Fr 110-cm sheath (Shuttle; Cook). The patient was anticoagulated with 5000 units of heparin intravenously. The 0.018-in 300-cm long guidewire (Roadrunner) was advanced across the right CIA lesion and into the right common femoral artery (CFA). A 7-mm × 15-mm × 135-cm balloon-expandable stent (Express LD; Boston Scientific) was advanced over the 0.018-in guidewire and deployed and then post-dilated with an 8-mm × 20-mm × 135-cm balloon (Sterling; Boston Scientific) to 12 atm, with an excellent angiographic result (Figure 5). The proximal left CIA lesion was then crossed with the 0.018-in × 300-cm Roadrunner guidewire over which a 7-mm × 19-mm × 150-cm balloon-expandable stent (Express SD) was deployed and post-dilated with an 8-mm × 20-mm × 135-cm balloon (Sterling) at 8 atm with an excellent result (Figure 5).

Final angiogram showing patent bilateral common iliac artery stents.
There were no peri-procedural complications. The patient ambulated prior to discharge and reported no claudication. A post-procedure ABI was unchanged from baseline at 0.46 on the right and 0.47 on the left. The lack of improvement in ABI is due to the multi-level occlusive disease in the SFA, tibio-peroneal trunk (right) and popliteal artery (left). The patient was discharged on aspirin, clopidogrel and a statin with follow-up planned in 30 days.
Discussion
A trans-femoral approach for this patient would have required bilateral femoral artery access given the acute angle of the aorto-iliac bifurcation and the previously placed right CIA stent, which would have made single femoral access with cross-over difficult. The advantage of the radial approach in this case was that it avoided femoral artery access entirely, thus reducing the risk of peri-procedural bleeding. 2 The risk of limb ischemia or stent thrombosis following compression of the femoral artery for hemostasis distal to the stent placement in this patient was avoided. Also, early ambulation was possible because of the radial approach. Additional advantages of the radial over the femoral approach 3 are shown in Table 1.
Advantages of radial artery over femoral artery access.
The 5-Fr 110-cm sheath (Shuttle) with an outer diameter of 2.28 mm facilitated the delivery of large balloon-expandable stents and balloons without the need for upsizing to accommodate a 7-Fr guide catheter (Table 2). The hyperemia-induced mean trans-lesional gradient using 25 mg of papaverine was 12 mmHg. In the Dutch Iliac Stent Trial, 4 a mean trans-lesional gradient of greater than 10 mmHg following hyperemia (with 25 mg papaverine, 40 mg tolazoline, or 100 μg glyceryl trinitrate) was considered hemodynamically significant, justifying stent placement.
Comparison of sheaths versus guides.
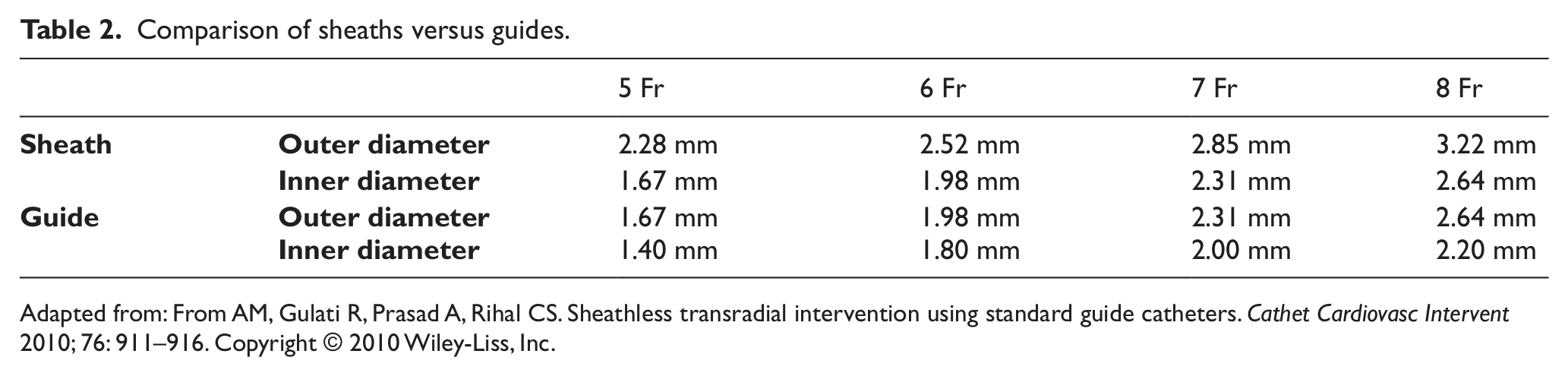
Adapted from: From AM, Gulati R, Prasad A, Rihal CS. Sheathless transradial intervention using standard guide catheters. Cathet Cardiovasc Intervent 2010; 76: 911–916. Copyright © 2010 Wiley-Liss, Inc.
Balloon-expandable stents were preferred in this case of bilateral proximal common iliac lesions because of their radial strength and the precision of deployment compared to self-expanding stents. The extra-long (≥ 135 cm) shaft lengths made the balloons and stents deliverable to the iliac artery from the radial approach.
The treatment strategy for this patient’s chronic claudication was to improve inflow to the legs. However, in the presence of critical limb ischemia (CLI) (e.g. presence of rest pain, non-healing ulcer or gangrene), the treatment strategy would have been to restore pulsatile, straight-line flow to the foot. 5 The patient’s height (arm and torso length) may be a limitation for trans-radial iliac interventions, as the longest sheath currently available in the USA is 110 cm, and the longest shaft lengths for stents is 135–150 cm.
In summary, trans-radial iliac intervention is feasible and safe with currently available devices, and with currently available equipment may be considered a reasonable option.
Footnotes
Declaration of conflicting interest
None of the authors have any conflict of interest to disclose as pertains to this manuscript.
Funding
This article received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.