
Abstract
Keywords
Introduction
Stent placement for symptomatic peripheral artery disease (PAD) is a common and accepted revascularization strategy. Prior publications on stent deployment for atherosclerotic iliac artery disease have supported favorable initial and late clinical benefit using balloon-expandable,1–5 self-expanding,6–9 and polytetrafluoroethylene (PTFE)–covered stents.10–13 Although gender has been shown to be an important determinant of outcomes in studies of coronary14,15 and other peripheral endovascular interventions,16,17 this effect has not been well defined for patients undergoing iliac artery stenting. This report evaluates procedural and clinical variables through 9 months of follow-up in a cohort of patients treated with the Visi-Pro Balloon-Expandable Peripheral Stent System (Medtronic, Dublin, Ireland), with particular attention to outcomes related to different prespecified patient characteristics, including gender.
Methods
Study Design
The VISIBILITY Iliac study was a prospective, multicenter, single-arm study to confirm the safety and effectiveness of primary stenting using the Visi-Pro Balloon-Expandable Peripheral Stent System for the treatment of stenotic, restenotic, or occluded lesions in the common iliac artery (CIA) and external iliac artery (EIA). Prior to patient enrollment, each of the 17 investigational sites in the United States (n=15) and Europe (n=2) obtained institutional review board approval. The trial was registered on the National Institutes of Health website (ClinicalTrials.gov; identifier NCT01402700).
Patients were eligible for participation if they had claudication or rest pain (Rutherford category 2–4) and de novo or restenotic ≥50% lesions ≤10 cm long in the CIA or EIA. Exclusion criteria included in-stent restenosis, previous implantation of stent(s) in the target vessel, angiographic evidence of an aneurysmal target vessel, presence of thrombus or other injury to the target vessel requiring additional treatment prior to treatment of the target lesion, or lack of blood flow to the foot or ankle of the target limb. Additionally, patients with allergies, hypersensitivities, or contraindications to known components of treatment in the trial were excluded. Patients were required to sign informed consent documents to participate. Between July 2011 and September 2012, 75 patients (mean age 64.2±8.9 years; 46 men) with 76 iliac artery target lesions were enrolled (Table 1).
Baseline Characteristics of the 75 Study Patients. a
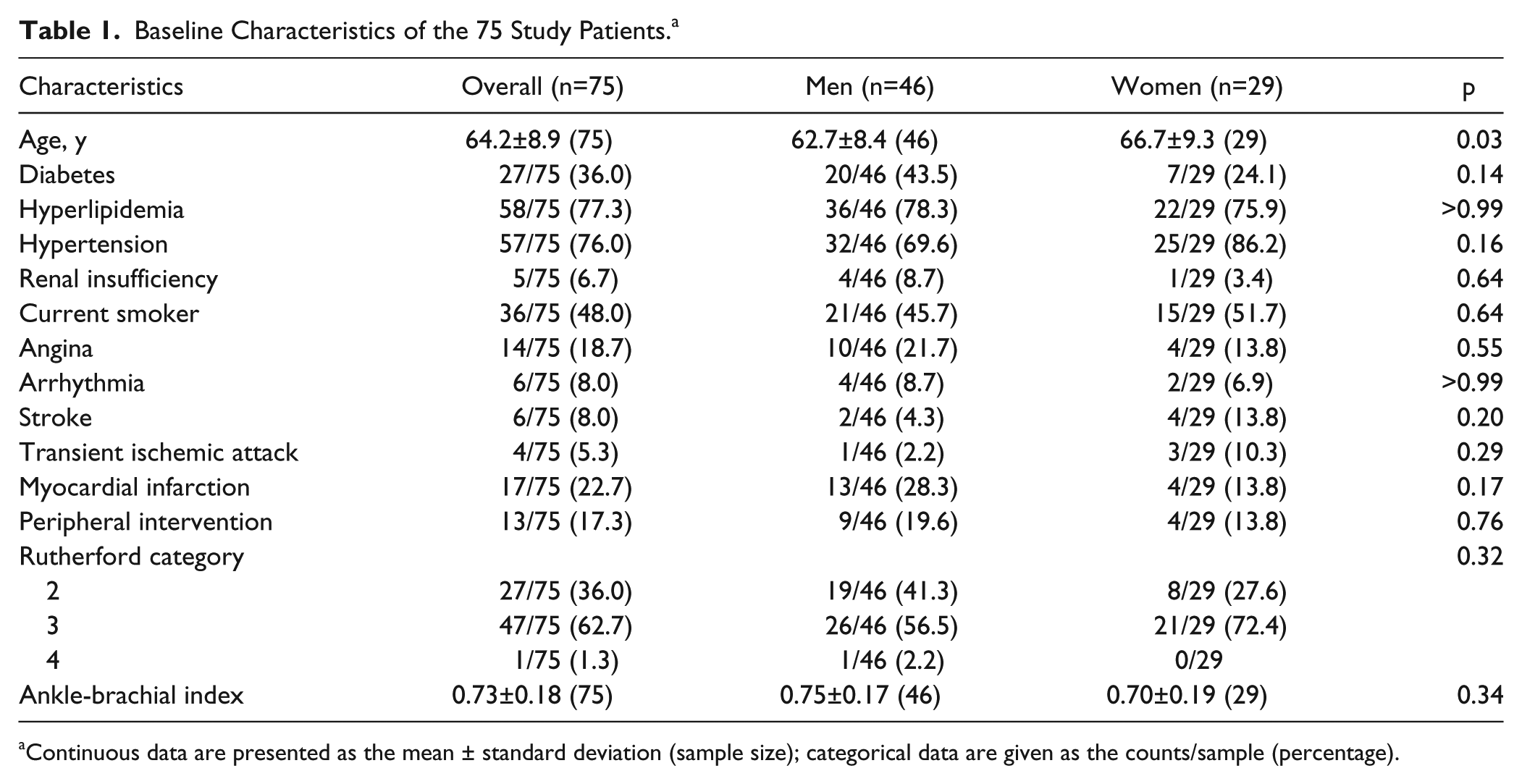
Continuous data are presented as the mean ± standard deviation (sample size); categorical data are given as the counts/sample (percentage).
The study included independent oversight of safety, including adverse events, as well as independent evaluation of study outcomes. A Clinical Events Committee (CEC) of physicians who did not participate in the study adjudicated and classified site-reported device-, procedure-, or study-related adverse events. Core laboratory evaluation was performed for angiographic images (Beth Israel Deaconess Medical Center, Boston, MA, USA) and 9-month duplex patency (VasCore, Boston, MA, USA).
Patient Assessments and Follow-up
Patients were assessed before and during the procedure and subsequently at 30 days and 9 months as required by study protocol. Patient evaluations consisted of medical history, including concomitant medication use, physical examination, Rutherford category, TASC II (TransAtlantic Inter-Society Consensus II) classification, ankle-brachial index (ABI), the Walking Impairment Questionnaire (WIQ), and laboratory tests (creatinine and complete blood count). Calcification was determined from the preprocedural angiogram prior to contrast injection or digital subtraction; moderate calcification was defined as radiopacities <1 cm long on one side of the arterial wall while severe calcification referred to radiopacities >1 cm long on both sides of the arterial wall. Duplex ultrasound was performed at the 9-month follow-up visit only. Adverse event evaluation was performed at the end of the index procedure and at each follow-up visit.
Study Device
The Visi-Pro system consists of a balloon-expandable stent mounted on a noncompliant catheter (Figure 1). The stent is made from a 316L stainless steel tube cut into an open lattice design. It is deployed and expanded by inflating the balloon and is intended to be permanently implanted. Multiple balloon lengths (12, 17, 27, 37, and 57 mm) and diameters (5, 6, 7, 8, 9, and 10 mm) were available for the study. Standard angioplasty techniques were followed for balloon dilation during stent implantation with an intended 1:1 stent to vessel diameter sizing. The appropriate stent diameter of Visi-Pro was chosen using the diameter of the balloon. Predilation was allowed per protocol at operator discretion.
The Visi-Pro balloon-expandable peripheral stent is cut in an open lattice design and comes premounted onto a noncompliant balloon catheter, with tantalum markers at the proximal and distal ends of the stent. The stent is available in stent diameters of 5, 6, and 7 mm with corresponding stent lengths of 12, 17, 27, 37, and 57 mm and in larger diameters of 8, 9, and 10 with corresponding stent lengths of 17, 27, 37, and 57 mm.
Endpoints and Outcome Measures
The primary outcome of the study was the major adverse event (MAE) rate at 9 months postprocedure, defined as a composite of periprocedural death related to the procedure or study device as adjudicated by the CEC, in-hospital myocardial infarction (MI), clinically driven target lesion revascularization (CD-TLR), and unplanned amputation of the treated limb above the metatarsal line. This endpoint was prespecified to be stratified by gender. Secondary safety outcomes included the MAE rate as defined above at 30 days postprocedure. Secondary clinical outcomes included (1) 9-month primary patency defined by a duplex ultrasound ratio ≤2.4 at the stented target lesion with no clinically driven reintervention within the stented segment; (2) the change in ABI and WIQ at 30 days and 9 months; (3) device success, defined as the ability to deploy the stent as intended at the treatment site; and (4) clinically-driven target vessel revascularization (CD-TVR) at 30 days and 9 months, defined as any reintervention or bypass graft surgery involving the target vessel in which the subject had recurrent symptoms and a ≥50% diameter stenosis (per angiographic core laboratory assessment) or a ≥70% stenosis without any symptoms. Additional post hoc analyses were done to examine patency of lesions stratified by gender, lesion location, calcification, occlusion, and TASC II status.
Statistical Analysis
Patient demographics, clinical history, procedure characteristics, and outcome variables were summarized using the mean ± standard deviation for continuous variables and count/sample (percentage) categorical variables. Comparisons for gender and other specified characteristics were performed using the Fisher exact or chi-square test for categorical variables and the Kruskal-Wallis test for continuous variables. Logistic regression models were used to identify the predictors for 9-month MAE. Primary patency and CD-TVR at 9 months were estimated by Kaplan-Meier analysis; the log-rank test was used for comparisons. Kaplan-Meier estimates are given with the 95% confidence interval (CI). Differences achieving p<0.05 were considered significant. All statistical analyses were performed using SAS for Windows software (version 9.1 or higher; SAS Institute, Cary, NC, USA).
Results
Patient and Lesion Characteristics
Overall, baseline characteristics (Table 1) were similar between men and women with the exception of mean age (women 66.7±9.3 years vs 62.7±8.4 years for men; p=0.03) and the greater proportion of women who presented with hypertension (86.2% vs 69.6%, p=0.16). Clinically, men were more likely than women to subjectively report moderate claudication (41.3% vs 27.6%) and conversely, women were more likely than men to present with severe claudication (72.4% vs 56.5%). These clinical differences were not statistically significant. Baseline ABI measurements were similar between genders, with mean values of 0.75 for men and 0.70 for women (p=0.34).
Patients were further stratified by lesion characteristics (Table 2). Lesions were located in the CIA (n=61) and EIA (n=15). The proportion of CIA lesions treated in women was significantly higher than those treated in men (93.1% vs 72.3%, p=0.04), and conversely, the proportion of EIA lesions treated in women was significantly lower (6.9% vs 27.7% in men, p=0.04). The overall mean lesion length was 29.3±13.9 mm. Per angiographic core laboratory assessment, the baseline diameter stenosis was 68.3%±13.5%; there were 6 (7.9%) total occlusions and 41 (53.9%) moderately to severely calcified lesions.
Baseline Characteristics 76 Target Lesions. a
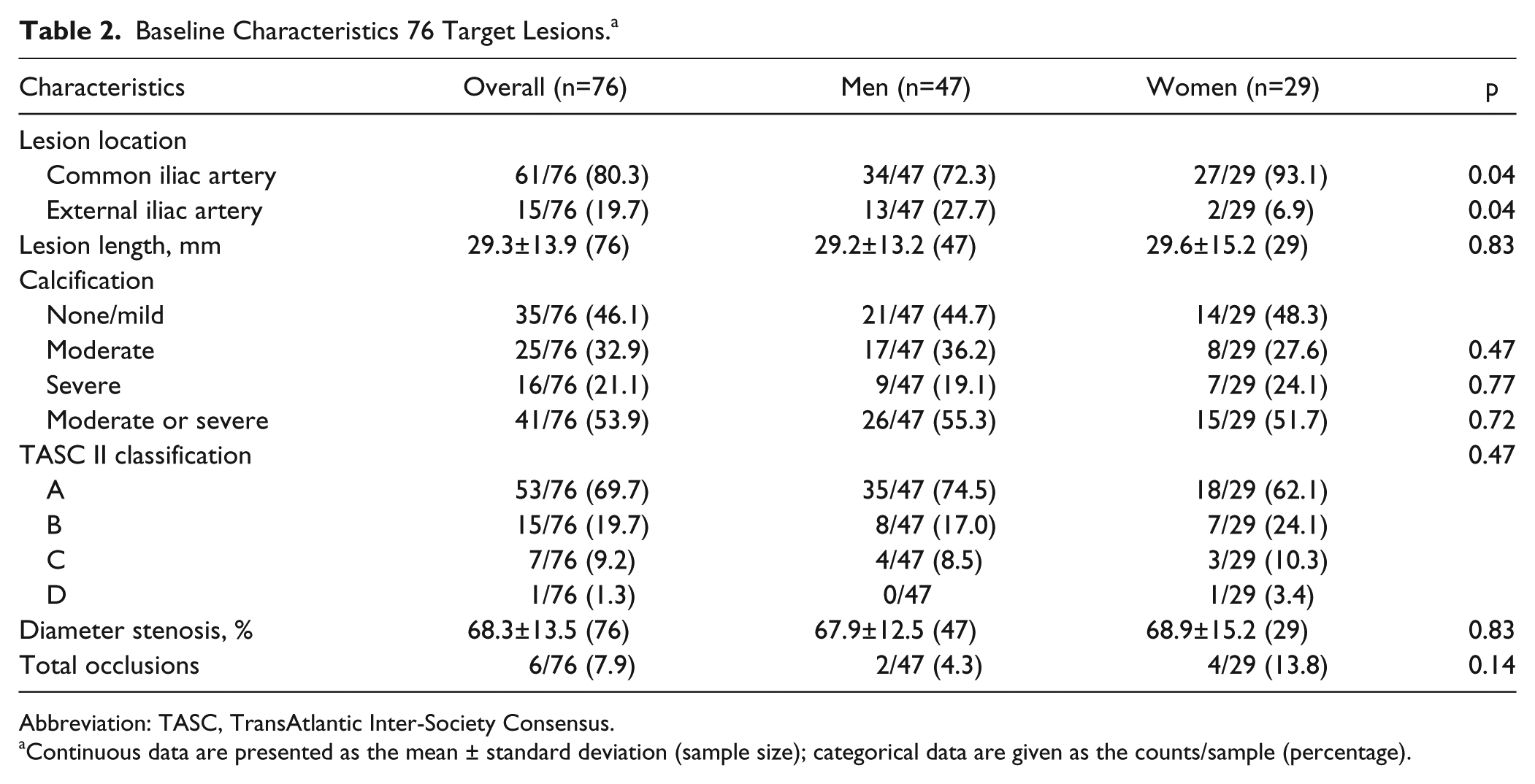
Abbreviation: TASC, TransAtlantic Inter-Society Consensus.
Continuous data are presented as the mean ± standard deviation (sample size); categorical data are given as the counts/sample (percentage).
A total of 81 stents were successfully implanted with no device malfunctions reported. The majority of patients (92.0%) had a single stent implanted; 6 patients had 2 stents implanted. One subject had 2 target lesions treated with individual stents, and the other 5 subjects had 2 stents implanted for complete coverage of a single target lesion (ie, no incidence of geographic miss). The postprocedural diameter stenosis was 7.7%±11.2% according to the core laboratory (Table 2).
Procedural Complications
As adjudicated by the CEC, periprocedural complications included 7 access site hematomas, 4 stent edge dissections, and 1 peripheral embolization. Two of the dissections were considered to be related to the procedure and device. All events were resolved without sequelae.
Primary Outcome
The MAE rate at 9 months consisted of 5 CD-TLRs in 3 (4.0%) patients; there were no periprocedural deaths, MIs, or amputations. Three interventions were performed in 1 subject in whom 1 target left CIA lesion and 1 nontarget right CIA lesion were treated during the index procedure. Reintervention was required for in-stent reocclusion of both index lesions and treatment of a de novo lesion in the aorta not treated at the index intervention. When stratified by gender, the MAE rate at 9 months was 4.3% for men and 3.4% for women. A Cox regression analysis failed to identify any predictors of the primary outcome. The cumulative rate of all-cause mortality was 4.0% (3/75) at 9 months and included 2 deaths due to metastatic lung cancer and 1 due to cardiac arrest.
Secondary Outcomes
There were no MAEs within 30 days of the procedure. Primary patency at 9 months was 95.8% (95% CI 91.3% to 100.0%; Figure 2). In the post hoc analyses, there was no difference in the patency between genders (Table 3); men had a patency rate of 95.6% (95% CI 89.5% to 100.0%) vs 96.6% (95% CI 89.9% to 100.0%, p=0.21) for women. There were also no significant differences in patency based on lesion location, calcification, or presence of an occlusion. However, lower patency was observed in TASC C/D lesions (83.3%) compared with TASC A or B lesions (98.1% and 92.9%, respectively; p<0.001). Freedom from CD-TVR at 9 months, which was 95.8% for the overall cohort, was similar between genders in the post hoc analysis (95.6% for men and 96.6% for women, p=0.62).
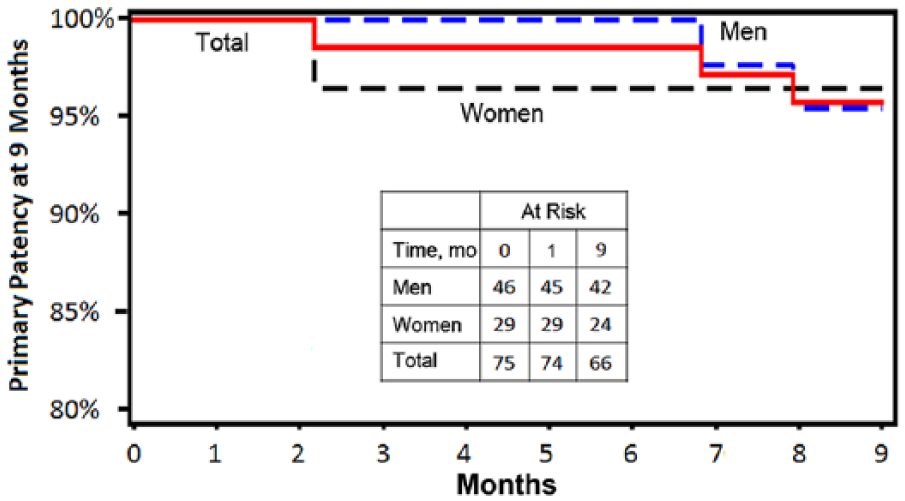
Kaplan-Meier estimate of 9-month primary patency overall and by gender. The standard error did not exceed 10%.
Primary Patency per Patient at 9 Months. a
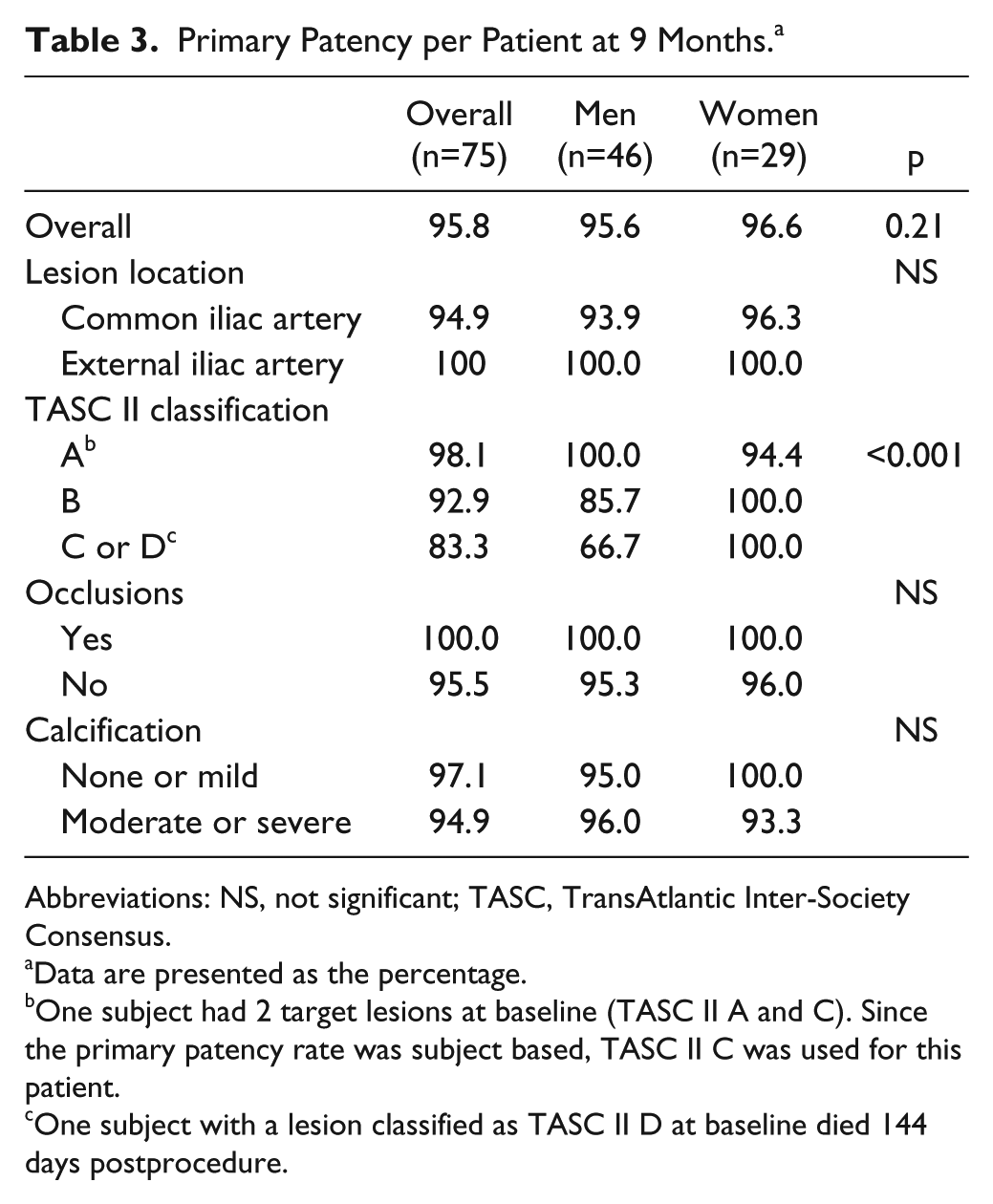
Abbreviations: NS, not significant; TASC, TransAtlantic Inter-Society Consensus.
Data are presented as the percentage.
One subject had 2 target lesions at baseline (TASC II A and C). Since the primary patency rate was subject based, TASC II C was used for this patient.
One subject with a lesion classified as TASC II D at baseline died 144 days postprocedure.
The mean ABI increased by 0.28 from baseline to 30 days and 9 months (p<0.001). The proportion of patients with improvement in ABI was stable at 30 days and 9 months, remaining at 91.4% and 92.2%, respectively (Table 4). Based on the change in the WIQ score from baseline (Table 4), walking improved at 30 days and 9 months in terms of limb pain (p<0.001), the mean walking distance score (p<0.001), the walking speed score (p<0.001), and the stair climbing score (p<0.001). Overall, 98.6% and 92.4% of patients showed improvements in 1 or more Rutherford clinical categories at 30 days and 9 months, respectively.
Summary of Secondary Outcomes Through 9 Months. a
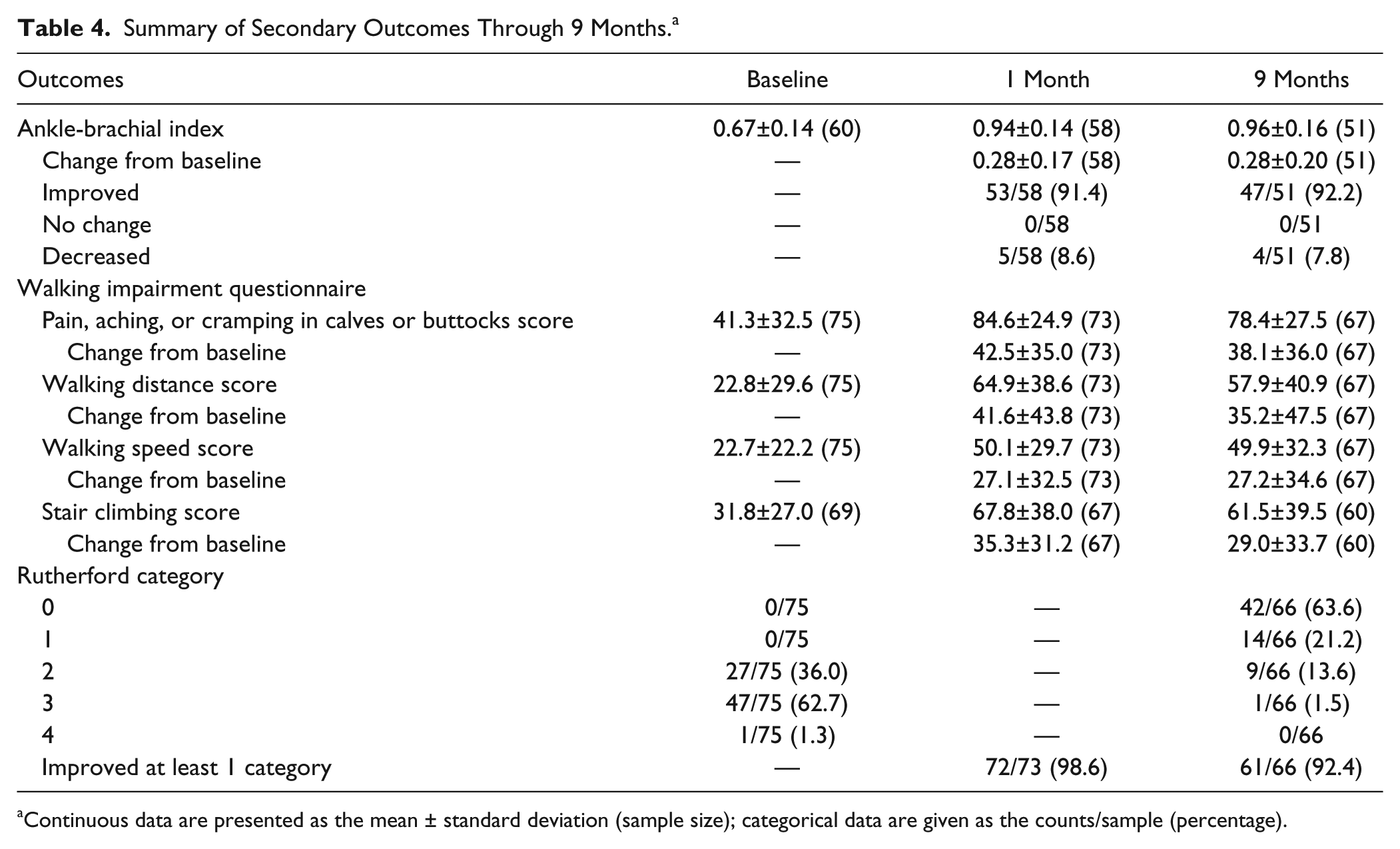
Continuous data are presented as the mean ± standard deviation (sample size); categorical data are given as the counts/sample (percentage).
Additional post hoc analyses showed no significant differences between men and women at the 1- and 9-month time points with regards to both ABI measurements and Rutherford categories. At 30 days, men had a higher WIQ walking distance score (71.9±34.8) than women (53.5±42.2, p=0.038) and a higher walking speed score (57.0±28.7 vs 38.9±28.2, p<0.01). WIQ climbing scores were statistically higher for men at 30 days (75.3±34.8 vs 55.2±40.4, p=0.03) and 9 months (69.5±37.8 vs 47.7±39.5, p=0.04). WIQ pain scores were not significantly different between men and women at either 1 month (87.2±22.4 vs 80.4±28.3, p=0.35) or 9 months (75.0±29.7 vs 84.0±22.7, p=0.26).
Discussion
Since Palmaz et al 1 first reported iliac artery stenting in 1992, several other prospective randomized and nonrandomized studies have evaluated balloon-expandable, self-expanding, and PTFE-covered stents for iliac PAD.2–13 The current study was conducted as part of a supplemental premarket approval (PMA) investigation and confirmed the safety and efficacy of the Visi-Pro Balloon-Expandable Peripheral Stent System. The Visi-Pro stent has radiopaque markers to optimize positioning and reduce geographic miss and a cell design that optimizes outward expansion. The observed 7.7% residual stenosis after stenting with the Visi-Pro stent is lower than reported for other balloon-expandable stents, despite a similar prevalence of moderate and severe calcification in this and other studies. The primary 9-month patency of 95.8% and the 95.8% 9-month freedom from CD-TVR are consistent with prior nonrandomized reports for both balloon-expandable and self-expanding stents.1,2,4,6–9 In addition, there was a high rate of both initial and sustained patient-reported benefit, consistent with the findings of the iliac stent cohort treated in the Endovascular Revascularization And Supervised Exercise for claudication (ERASE) study. 18
Few trials have reported comparative outcomes for iliac intervention by gender. In the MOBILITY study evaluating the Absolute Pro vascular self-expanding stent system (Abbott Vascular, Santa Clara, CA, USA), 19 the 9-month patency rate was 87.2% for women and 92.1% for men. In a study by Bechter-Hugl et al, 20 patency rates were similar for iliac artery stenting between men and women out to 7 years, despite the more advanced age and disease of the female patients. In our study, there was no distinction in overall primary patency by gender with Visi-Pro, although higher patency rates were observed for women in the small number of patients (n=8) with higher TASC grades (p<0.001; Table 3). Despite similar patency, there was a statistically significant difference between genders in the level of symptomatic WIQ score improvement. This finding is supportive of the observations made by McDermott et al, 21 who showed that men do not subjectively experience as significant or rapid a functional decline as do women. These differences could be due to the differential size of calf muscles and generalized lower extremity strength at baseline in women compared with men.
Outcomes relative to stent implantation in the CIA compared with the EIA have not been well described.22,23 A retrospective study conducted by Timaran and colleagues 23 reported significantly decreased patency rates out to 5 years for EIA compared with CIA stents. Additionally, women with EIA lesions had significantly worse patency outcomes compared to their male counterparts. In contrast, although men within the VISIBILITY Iliac study were more likely to have EIA lesions, no differences were observed in primary patency or MAE by stent location.
Although prior studies have suggested superiority of covered stents compared to bare metal stents for patients with complex iliac artery stenoses and occlusions, 12 our data did not confirm these findings. Patency with the Visi-Pro in this series was superior to the 23% restenosis observed with bare metal stents when randomized against PTFE-covered stent-grafts in the COBEST trial. 12 Similarly, a retrospective analysis by Humphries and colleagues 5 supports equivalent patency for covered vs bare metal iliac stents, with patency rates of 85% and 92% (p<0.01), respectively. Further studies will be needed to determine if the additional cost and larger sheath size needed for covered stent placement is warranted in patients with challenging iliac anatomy.
Limitations
As a PMA single-arm study, this evaluation had no control group for comparison. Overall study sample size was small, and the study was not statistically powered to observe any differences in subgroups. As such, reported event rates by gender represent post hoc rather than prespecified analyses. Also, multivariate analyses were not performed due to the low prespecified event rates. Although lesions up to 10 cm were included in the study, the overall mean lesion length was 29.3 mm, reflecting inclusion of a cohort of individuals that for the most part did not have advanced iliac lesion characteristics. Similarly, there were fewer patients with TASC C (9.2%) and TASC D (1.3%) lesions, which necessitated combining the two for the purposes of endpoint analysis. Finally, the study was designed as a confirmatory study given that the predicate device had been extensively studied in a larger trial.
Conclusion
These data suggested that patients with symptomatic iliac PAD benefit from implantation of the Visi-Pro stent and that treatment with this balloon-expandable stent was safe and effective. No differences were observed between genders or related to iliac stent location or severity of calcification. Results were less favorable in pooled TASC C/D patients. Patency rates were comparable to data that have been reported for covered stents in the iliac arteries.
Footnotes
Acknowledgements
The VISIBILITY Iliac investigators would like to recognize and thank the patients involved with this clinical study for their participation. The authors acknowledge the following individuals from Medtronic for their contributions: Jennifer Wolvers for study coordination, Haiying Lin for statistical analysis, and Azah Tabah, PhD, and Bridget Wall, PhD, for medical writing support.
Authors’ Note
Various data from this study were presented in abstract or poster form at the following meetings: EuroPCR 2014, Paris, France; VEITHSymposium 2014, New York, NY, USA; VIVA 2014 and 2015, Las Vegas, NV, USA; and LINC 2015, Leipzig, Germany.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: John H. Rundback is a paid consultant to Covidien/Medtronic. Jon C. George is a consultant to Covidien/Medtronic and received a research grant. Michael R. Jaff is a noncompensated advisor for Covidien Vascular and a board member of VIVA Physicians, a 501c not-for-profit education and research organization.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Medtronic.