
Abstract
Vascular dysfunction has been described in women with a history of gestational diabetes mellitus. Furthermore, previous gestational diabetes mellitus increases the risk of developing Type 2 diabetes mellitus, a risk factor for cardiovascular disease. Factors contributing to vascular changes remain uncertain. The aim of this review was to summarize vascular structure and function changes found to occur in women with previous gestational diabetes mellitus and to identify factors that contribute to vascular dysfunction. A systematic search of electronic databases yielded 15 publications from 1998 to March 2014 that met the inclusion criteria. Our review confirmed that previous gestational diabetes mellitus contributes to vascular dysfunction, and the most consistent risk factor associated with previous gestational diabetes mellitus and vascular dysfunction was elevated body mass index. Heterogeneity existed across studies in determining the relationship of glycaemic levels and insulin resistance to vascular dysfunction.
Introduction
Gestational diabetes mellitus (GDM), defined as glucose intolerance with onset or first recognized during pregnancy, typically is diagnosed in the second or third trimesters.1,2 Although GDM usually resolves postpartum, it is a risk factor for the subsequent development of Type 2 diabetes mellitus (Type 2 DM).3,4 Consequently, women with a history of GDM also have an increased risk of developing cardiovascular disease. 1 However, the effects of previous GDM on vascular structure and function are uncertain. Vascular dysfunction has been associated with the alteration in vessel response to defined stimuli associated with impaired relaxation, resistance and blood flow.5,6 The effects of vascular dysfunction can be measured by various techniques5,6 and may be quantified at both a macrovascular level and microvascular level. Our first objective was to conduct a systematic review of the literature to identify the vascular changes in macrovascular and microvascular function that occur in women with previous GDM. The second objective was to determine which demographic and clinical features present in women with previous GDM have been detected as contributing to vascular dysfunction.
Materials and methods
Search methods
Based on a scoping review of the topic area, the published literature via electronic search methods was limited in number and dated back to 1997. A systematic search of the following databases was completed: MEDLINE, EMBASE, CINAHL, Cochrane, SCOPUS, Web of Science and BIOSIS. The keywords used were as follows: ‘gestational diabetes’, ‘diabetes mellitus’, ‘gestational’, ‘pregnancy-induced diabetes’, ‘glucose intolerance during pregnancy’, ‘vascular dysfunction’, ‘vascular’, ‘vascular disease’ and ‘blood vessels’. A manual search of retrieved references was further performed to identify relevant missed articles. The inclusion and exclusion criteria for the studies retrieved are listed in Table 1.
Inclusion/exclusion criteria for studies.
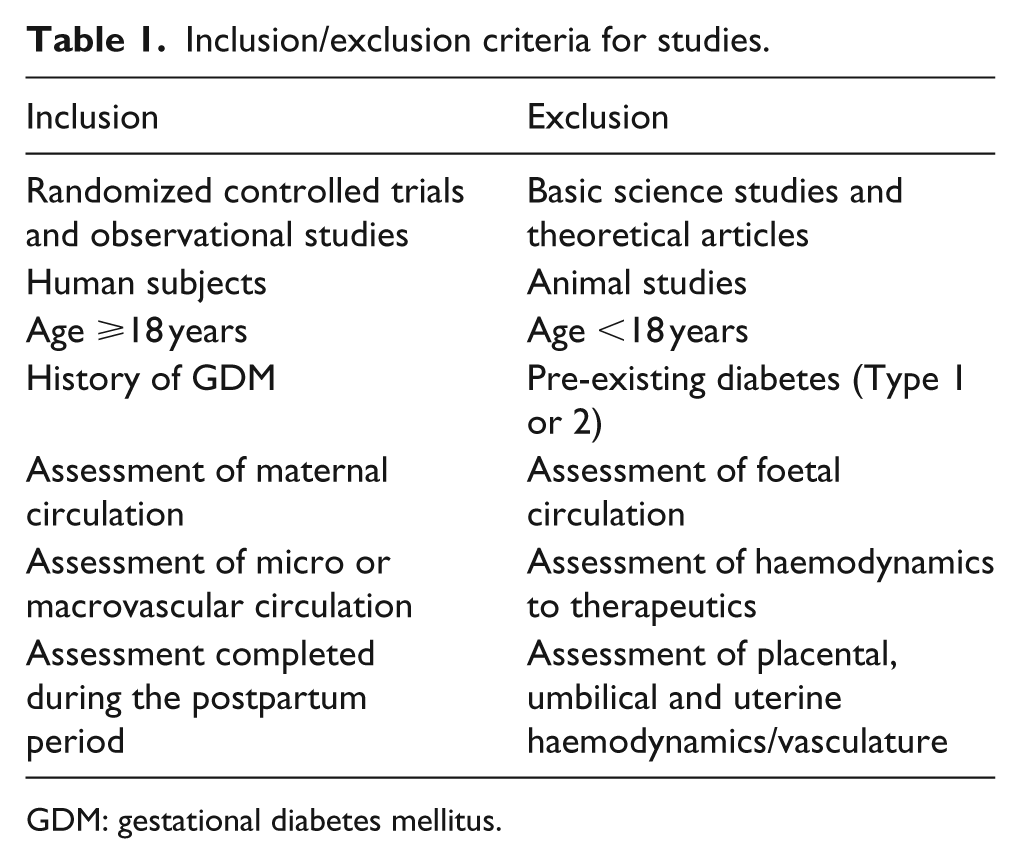
GDM: gestational diabetes mellitus.
Study outcomes
The primary study outcome sought in this review was the changes in vascular structure and function, both macrovascular and microvascular, in women with previous GDM. The secondary outcome sought was factors that contribute to vascular dysfunction. These included age, time postpartum, smoking status, blood pressure, lipid profile, inflammatory markers, family history of cardiovascular disease, stroke, hypertension, DM, waist circumference, waist-to-hip ratio and body mass index (BMI).
Data extraction and analysis
The literature was systematically and comprehensively surveyed, as well as a tabular synthesis made of the extracted data by three independent researchers. All articles identified from the search and meeting the inclusion criteria were used in the final analysis. The limited number and marked variability in the studies reviewed confounded any statistical aggregation, permitting only a descriptive analysis.
Results
The results of the search are presented in Figure 1. In MEDLINE, 877 citations were screened; in EMBASE, 576 citations; in CINAHL, 1185 citations; in Cochrane, 13 reviews; and 5 other reviews were screened. In SCOPUS, 38 citations were screened; in Web of Science, 84 citations; and in BIOSIS, 482 citations. Of these 3260 citations, 49 citations were identified based on title alone. In reviewing the abstracts for these 49 citations, 34 citations were removed because they did not meet the inclusion criteria (Table 1; Figure 1). Following a detailed review, only 15 citations met the inclusion criteria and assessed vascular function in women with previous GDM during the postpartum period. These publications dated from 1998 to March 2014.
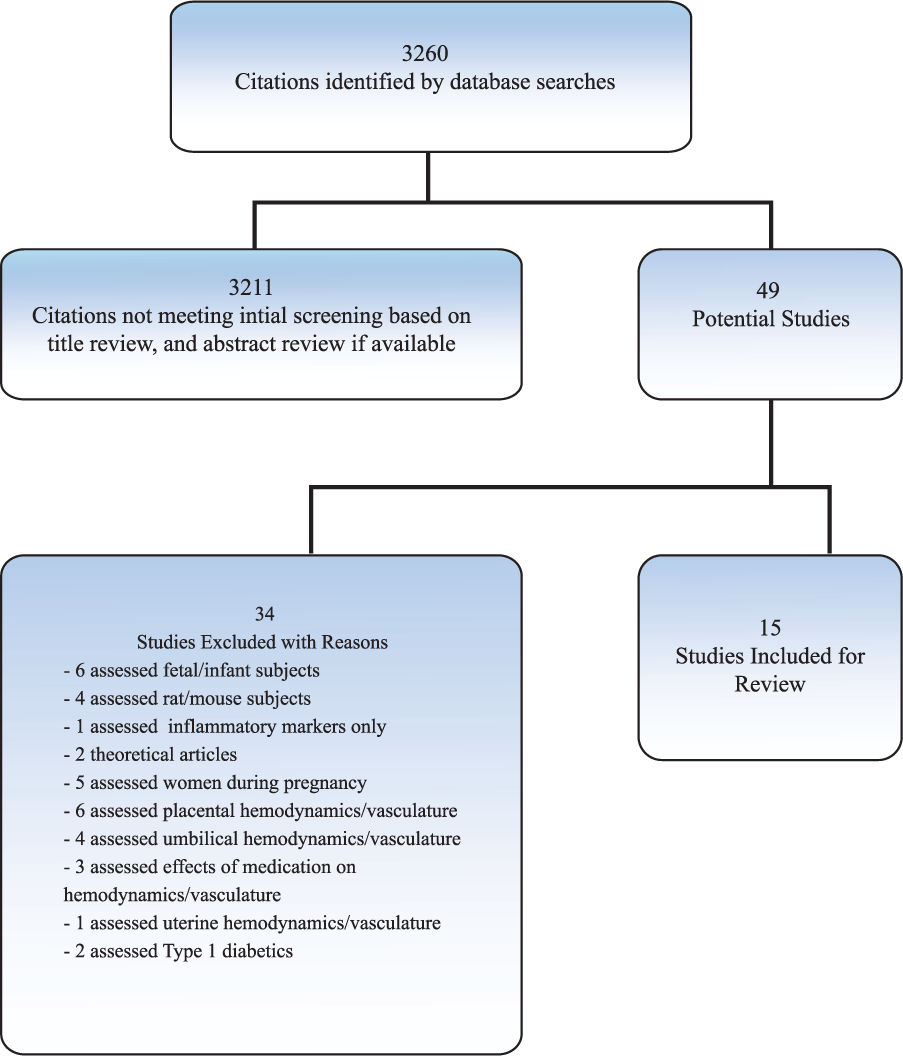
Search outcomes.
Study design
All 15 studies used a case–control design. Seven studies were conducted in Europe,7–13 two in Canada,14,15 one in Iran, 16 two in Turkey,17,18 one in Brazil 19 and two in the United States.20,21 Three studies created subgroups for women with previous GDM based on BMI;7,9,12 two studies created subgroups based on glycaemic levels.8,14 Finally, four studies matched subjects on age alone,14,16–18while Hannemann et al. 10 matched subjects on age, as well as BMI, menstrual phase, smoking, blood pressure and lipids; Fakhrzadeh et al. 16 matched subjects on age, BMI and follow-up period. Postpartum time period of assessment ranged from 2 months to 20 years (Table 2).
Subject characteristics.
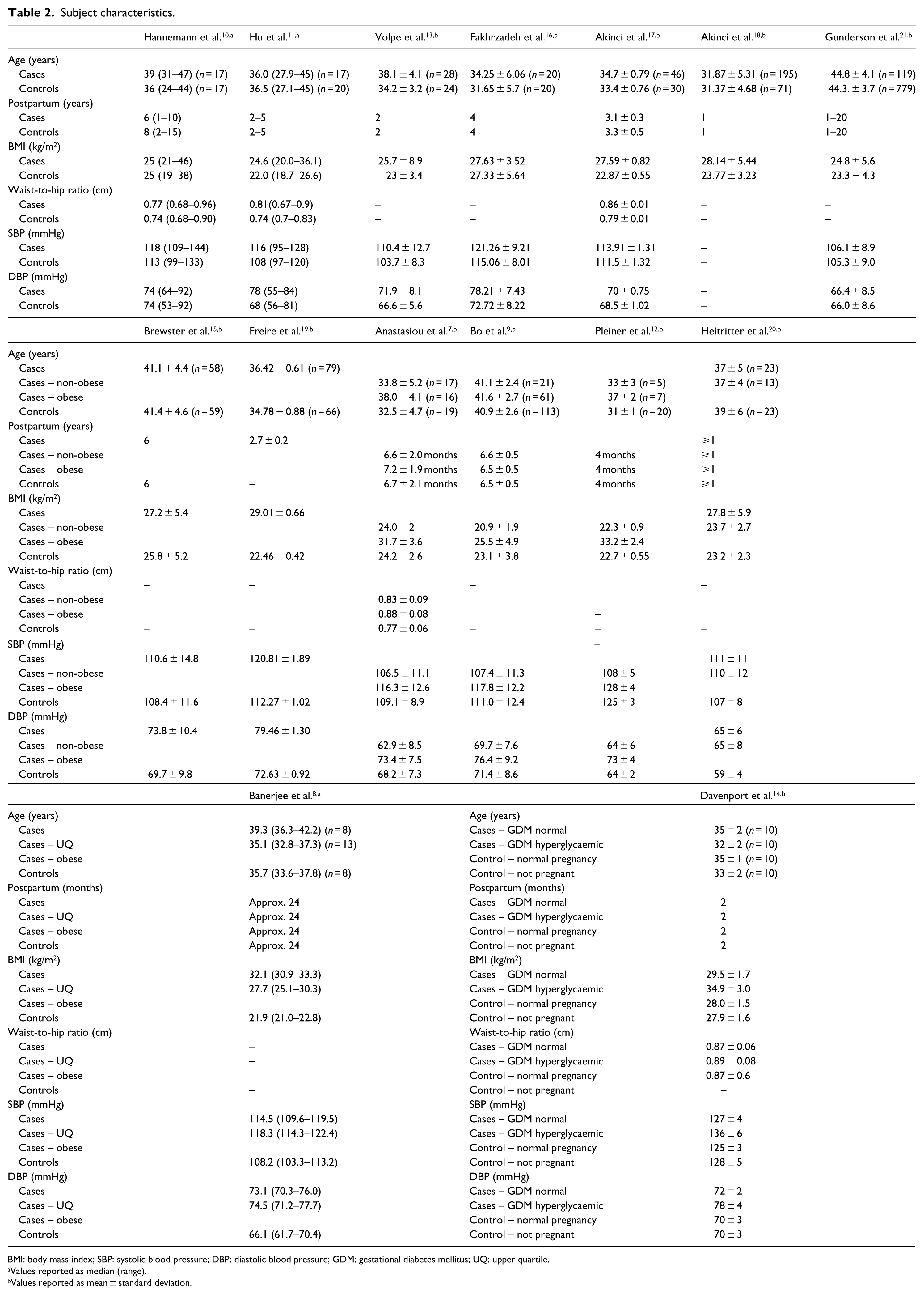
BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; GDM: gestational diabetes mellitus; UQ: upper quartile.
Values reported as median (range).
Values reported as mean ± standard deviation.
Details of the diagnostic approach to GDM were not provided in four studies.10,12,13,19 The remaining studies each used differing criteria, ranging from serum glucose values proposed by Carpenter and Coustan, 22 to the World Health Organization Expert Committee on Diabetes Mellitus 23 guidelines, the American Diabetes Association (ADA) 24 criteria, the National Diabetes Data Group Criteria 25 guidelines, the World Health Organization 26 Diagnosis and Classification of Diabetes Mellitus Part 1 Report for GDM criteria or the Canadian Diabetes Association 27 criteria. Gunderson et al. 21 validated self-reported GDM against the oral glucose tolerance test (OGTT) results from prenatal records.
Subject characteristics
There were a total of 2062 subjects, with the smallest study 11 having 20 subjects and the largest study 9 having 898 subjects. Cases of previous GDM women ranged from 8 to 195, while the number of controls ranged from 8 to 779. The latter includes the 20 male controls in Pleiner et al.’s 12 study (Table 2). Six studies10,11,14–16,20 examined women during either the follicular or luteal phases, whereas one study 7 examined women at various stages during their menstrual cycle. Seven other studies8,9,12,13,17–19 did not comment on the stage of the women’s menstrual cycle. Brewster et al. 15 noted the use of oral contraception, and another study 21 included menopausal status. Six studies7,9,14,16,19,20 did not include smokers. Although Akinci et al. 18 noted smoking habits, it was not included within their analysis. Two studies10,17 asked subjects to refrain from smoking ‘on the day of the study’, while Volpe et al. 13 and Gunderson et al. 21 included subjects who were smokers.
Cardiometabolic risk assessment
Blood pressure
Blood pressure ranged from 103.7/66.6 ± 8.3/5.6 to 128/72 ± 5/3 mmHg in the control women and from 106.5/62.9 ± 11.1/8.5 to 136.78/73.8 ± 6/10.4 mmHg in women with previous GDM (Table 2).
Adiposity
All studies reported BMI, with previous GDM women consistently higher than the control women. Five studies7,10,11,14,17 reported waist-to-hip ratio, with previous GDM women having a higher ratio in three studies.2,11,17 Of those reporting, waist circumference ranged from 71.7 ± 8.8 to 87 ± 0.6 cm in the controls and 73.6 ± 5.7 to 92 ± 13.19 cm in the previous GDM cases (Table 2).
Glycaemic status
In 13 studies,7–15,17,19–21 the control groups had lower fasting blood sugar (FBS) and OGTT levels than all previous GDM groups, while Fakhrzadeh et al. 16 reported no difference between groups (Table 3). Akinci et al. 18 noted that the prevalence of impaired fasting glucose (IFG) and impaired glucose tolerance (IGT) was higher in the previous GDM group after adjusting for pre-pregnancy BMI, family history of T2DM and postpartum diabetes. Additionally, Fakhrzadeh et al., 16 Akinci et al. 18 and Gunderson et al. 21 reported basal insulin resistance with the homeostatic model assessment index (HOMA), noting that the HOMA index was higher in the previous GDM women versus the controls.
Subject metabolic parameters.
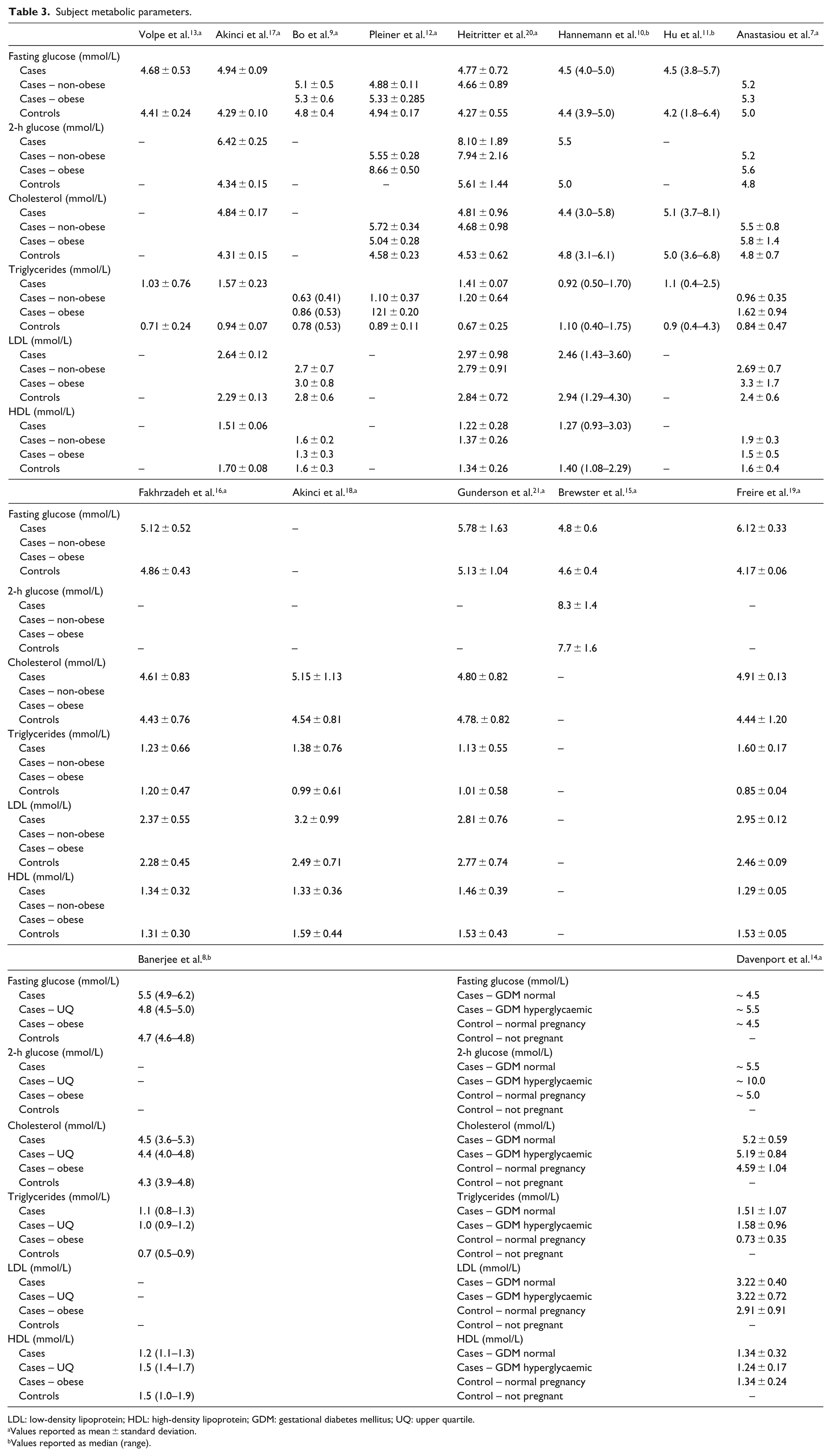
LDL: low-density lipoprotein; HDL: high-density lipoprotein; GDM: gestational diabetes mellitus; UQ: upper quartile.
Values reported as mean ± standard deviation.
Values reported as median (range).
Lipid status
The total cholesterol levels for previous GDM women were elevated in eight studies.7,8,12,16–20 In all but one of the studies 19 that assessed high-density lipoprotein (HDL) cholesterol, the controls had higher levels of HDL than previous GDM cases. However, the non-obese previous GDM groups had HDL levels similar to or higher than the controls, while the obese previous GDM groups had HDL levels lower than the controls.7–9,14 The low-density lipoprotein (LDL) was higher in the previous GDM groups in 8 of 10 studies.7,9,14,16,17,19–21 The non-obese previous GDM women had LDL levels similar to or lower than the controls, while obese previous GDM women had higher LDL levels than the controls.7,9,14 However, two studies10,21 reported similar LDL levels between previous GDM and control groups, with statin use higher in the previous GDM women in one study. 21 In all but four studies,9–11,16 triglycerides levels were significantly higher in previous GDM than control women (Table 3).
Inflammatory markers
The parameters measured in more than one study were high sensitivity C-reactive protein (hsCRP), interleukin (IL)-6, adiponectin, plasminogen activator inhibitor (PAI)-1 and fibrinogen. Fibrinogen was higher in the previous GDM women,12,17,18 while high adiponectin was negatively correlated with previous GDM.13,16,20 In addition, women with previous GDM had higher levels of hsCRP and PAI-1 than the control women;9,13,17,20 however, Fakhrzadeh et al. 16 reported hsCRP and PAI-1 levels to be lower in the previous GDM group. Heitritter et al. 20 found that IL-6 was increased in previous GDM women, whereas Fakhrzadeh et al. 16 reported lower IL-6 for the previous GDM group, and Bo et al. 9 found that previous GDM women with a BMI ⩾25 kg/m2 had higher IL-6 levels than the controls.
Circulating E-selectin, vascular cell adhesion molecule-1 (VCAM-1) and intercellular adhesion molecule-1 (ICAM-1) were measured only by Bo et al.,
9
who found that E-selectin and ICAM-1 were highest in previous GDM women with a BMI ⩾25 kg/m2 and lowest in control women. Interestingly, VCAM-1 was highest in previous GDM women with a BMI <25 kg/m2. In addition, asymmetric NG, NG-dimethyl
Vascular structure and function assessment
Macrovascular arterial structure and function
Eight studies used ultrasound as the primary method of choice when measuring macrovascular structure (Table 4). Bo et al., 9 Hu et al., 11 Volpe et al., 13 Fakhrzadeh et al., 16 Akinci et al.,17,18 Freire et al. 19 and Gunderson et al. 21 used high-resolution Doppler ultrasound to measure carotid intima medial thickness (CIMT). Bo et al. 9 found that previous GDM women, despite no metabolic abnormalities and independent of BMI, had higher CIMT, E-selectin and ICAM-1 values than control women 6 years postpartum. Hu et al. 11 also found that women with previous GDM had increased common carotid artery wall stiffness and lower pulsatile diameter changes 2–4 years postpartum compared to control women. Interestingly, in the control group, age was associated with arterial stiffness in both the carotid artery and aorta; however, in the previous GDM group, this trend was not shown. Similarly, Volpe et al. 13 found increased CIMT in previous GDM women compared to controls 2 years postpartum, despite no difference in BMI between groups and only one woman meeting the criteria for metabolic syndrome. Akinci et al. 17 noted that serum osteoprotegerin (OPG) levels were elevated in previous GDM women and a significant predictor for elevated CIMT 3 years postpartum. Later, Akinci et al. 18 found that the development of postpartum diabetes and metabolic syndrome were associated with increased CIMT in previous GDM women compared to controls at 1 year. Freire et al. 19 were the first to show that previous GDM women and women with metabolic syndrome had similar increased CIMT; however, in the regression models used, previous GDM was associated with increased CIMT regardless of cardiometabolic status and parity at 32 months postpartum.
Vascular function.
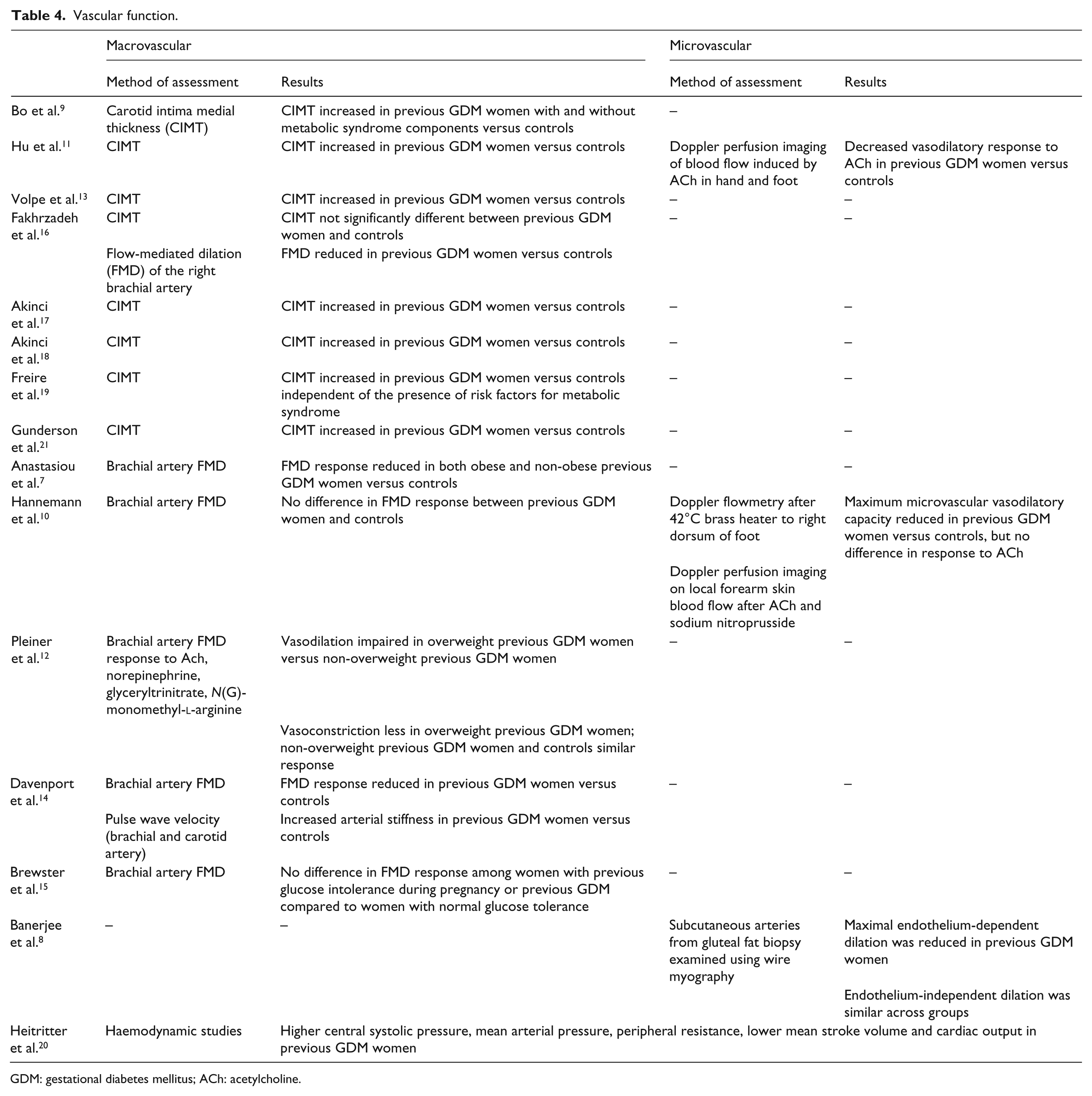
GDM: gestational diabetes mellitus; ACh: acetylcholine.
Of the five studies7,10,12,14,16 that used flow-mediated dilation (FMD) to assess arterial function, four studies7,12,14,16 found reduced FMD response in previous GDM women versus the controls. Fakhrzadeh et al. 16 evaluated vascular properties by both CIMT and FMD. After adjusting for age and blood pressure in the previous GDM group, they were the only study to conclude no difference in CIMT between groups; however, they noted an impairment of FMD in the previous GDM group compared with the control group that showed no correlation with biochemical or inflammatory markers 4 years postpartum. Anastasiou et al. 7 found that FMD was compromised in both the obese and non-obese previous GDM women 3–6 months postpartum as compared with the control subjects, even with normal glucose tolerance. In contrast, Hannemann et al. 10 found no difference in FMD of normoglycaemic previous GDM women compared to the control women matched on age, BMI and smoking. Pleiner et al. 12 following the trend reported by others found that the arterial response in previous GDM women and in overweight women was significantly compromised compared to the control group of healthy men. Davenport et al. 14 assessed FMD of the right brachial artery and the carotid artery, finding distensibility in both control groups was higher than both previous GDM groups, and suggested this possibly a factor of clinical and/or subclinical hyperglycaemia and decreased insulin sensitivity in the postpartum period. Brewster et al. 15 compared brachial artery FMD measurements and noted no difference between previous GDM and control groups 6 years postpartum despite having long-term cardiovascular risks (Table 4).
Microvascular arterial function
Three studies measured microvascular function (Table 4). Hannemann et al. 10 and Hu et al. 11 used laser Doppler flowmetry and acetylcholine on the skin of the dorsum of the foot and forearm. Hu et al. 11 found that the microvascular response in women with previous GDM was lower than in the control women. Hannemann et al. 10 also observed that maximum microvascular vasodilatory capacity (MMVC) was significantly reduced in women with previous GDM compared to the control group. However, this difference was only observed in the dorsum of the foot, while the brachial artery dilation revealed no difference in flow between the control and previous GDM groups. Banerjee et al. 8 used a subcutaneous fat biopsy to isolate the small arteries which were then put through different chemical stimuli. They found that overweight women with either previous GDM or marginally raised glycaemia during pregnancy had impaired small artery endothelial function at 2 years postpartum.
Discussion
It has thus been shown that previous GDM generally impairs vascular structure and function. In addition, it was found to be even more impaired in obese than in non-obese women with previous GDM. All but one 16 of the studies9,11,13,16–19,21 that examined CIMT found an increased arterial thickness in women with previous GDM. Each of the studies7,10,12,14 except for one 15 that examined brachial artery FMD found impaired arterial function in women with previous GDM. Additionally, in the limited studies8,10,11 that measured microvascular function, maximum vasodilatory capacity was found to be reduced in women with previous GDM.
Multiple cardiovascular risk factors identified as being associated with previous GDM are recognized features of the metabolic syndrome. The unexpected finding of Hu et al. 11 that arterial stiffness was related to increasing age in control but not previous GDM women may be a reflection that the increased arterial stiffness in the previous GDM group masked any influence of age and may be testimony to the predominant influence of the history of GDM. Overall, women with previous GDM had higher FBS, triglyceride and LDL levels. Also, women with previous GDM had elevated inflammatory markers, higher fibrinogen, hsCRP, PAI-1 and IL-6 levels, while adiponectin levels were lower than controls. Additional markers of endothelial dysfunction – E-selectin, VCAM-1, ICAM-1, ADAMA, SDMA and OPG – were reported to be higher in women with previous GDM. Six studies examined the association between inflammatory markers or glycaemic status such as HOMA and vascular dysfunction. Whereas Fakhrzadeh et al. 16 identified no correlation between IL-6, hsCRP or adiponectin and FMD, IL-6 and hsCRP were associated with CIMT in the study by Bo et al., 9 while Volpe et al. 13 found that CIMT was related to HOMA and hsCRP, but inversely related to adiponectin. CIMT was also correlated with fasting and post-load glucose and PAI-1 in the initial study by Akinci et al. 17 and with fasting glucose and HOMA in their second study. 18 In contrast, Gunderson et al. 21 reported no impact of pre-pregnancy HOMA on CIMT. In addition, the BMI of women with previous GDM was higher than the control women and the most consistent risk factor associated with previous GDM and vascular dysfunction.
Thus, findings suggest that women with previous GDM display a phenotype for future vascular problems – increased weight, fasting glucose and triglyceride levels, and higher levels of inflammatory cytokines including hsCRP, PAI-1 and fibrinogen – all manifesting in macro- and microvascular changes. However, the case–control design limits impaired glucose metabolism postpartum being a risk factor for atherosclerosis among women with previous GDM. Furthermore, most studies were unable to assess pre-pregnancy-related factors making it difficult to determine the presence of cardiometabolic risk prior to pregnancy. In addition, this review has several limitations. Only 15 studies were found to be relevant to previous GDM and vascular structure and function in the postpartum period. Another limitation is the variation in subject characteristics in each of the studies, in particular choice of controls, length of follow-up periods and differing hormonal status and smoking status. Because there is no consistency between subject groups, it is difficult to see parallels in the results. In addition, over recent years, the definition of GDM has changed, making comparisons also difficult. Finally, there was heterogeneity in measures used to assess vascular structure and function.
Conclusion
Women with a history of GDM, both obese and non-obese women, have evidence of increased arterial stiffness and decreased endothelial function in the post pregnancy period. Increased BMI and other cardiometabolic factors identified in women with previous GDM may be consistent with metabolic syndrome and thus future risk of DM and cardiovascular disease. Despite these findings, actual mechanisms contributing to a risk of vascular dysfunction in women with previous GDM remain uncertain. Heterogeneity existed across studies in this novel review. Further investigations are needed with a larger sample size to identify and validate markers of vascular risk before development of DM, metabolic syndrome or cardiovascular morbidity. Examining the effect of duration after the index GDM pregnancy on different cardiovascular risk markers has implications for postpartum screening. Longitudinal studies may assist to determine the relationship among glycaemic levels, insulin resistance, endothelial function and vascular disease.
Footnotes
Acknowledgements
The authors acknowledge graduate students Rajamalar Senthuran and Corinne Rogers for assistance with data collection and compilation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received funding support from the Faculty of Medicine & Dentistry and Capital Health Emerging Research Teams Grant, University of Alberta.