
Abstract
The aim of this study was to assess the association between peripheral arterial tonometry (PAT) and two more traditional measures of endothelial function – flow-mediated dilation (FMD) and its hyperemic stimulus, hyperemic peak velocity time integral (VTI). We related three vascular function measures (natural log transformed PAT, FMD, and VTI) from 304 patients (mean age 48.9 ± 12.5 years), including 105 with coronary artery disease (CAD). Using linear regression, we studied the relationships between lnPAT, FMD, and VTI, and compared differences in these parameters in those with and without CAD. Although FMD and lnPAT both had a correlation with VTI (Pearson’s r = 0.119, p = 0.039 and r = 0.167, p = 0.004, respectively), lnPAT had no correlation with FMD (r = −0.0471, p = 0.414). lnPAT was also lower in patients with CAD compared to controls (mean 0.51 ± 0.19 versus 0.65 ± 0.26, respectively, p < 0.0001). In multivariate analysis, VTI remained associated with lnPAT (standardized β = 0.1369, p = 0.04). Among this group of subjects with and without CAD, lnPAT was found to be unrelated to FMD but correlated with VTI. This would suggest that lnPAT is a measure of microvascular function. Although it is unrelated to FMD, lnPAT is decreased in patients with pre-existing cardiovascular disease. Further studies are required to determine if this can be used clinically as a tool for cardiac risk stratification and prediction of CAD.
Keywords
Introduction
Endothelial dysfunction is a well-described precursor to the development of clinically overt coronary artery disease (CAD) and is present early in the course of the disease. 1 Utility of endothelial function measures in predicting future cardiovascular events in those with and without prevalent disease has been demonstrated in myriad studies over the last decade.2 –4 However, the optimal method to assess vascular risk is not clear. Brachial flow-mediated dilation (FMD) has been the standard measure over the last two decades. Although it has been shown to be associated with cardiovascular outcomes,2,5,6 it is technically difficult to perform. Recently there has been interest in the hyperemic stimulus for FMD, hyperemic velocity, as it is more closely related to cardiovascular risk factors7,8 and may be related to outcomes. 9 However, finding a methodology for assessing endothelial function that is easily utilized with an automated, reproducible end point has been elusive. One emerging technology is peripheral arterial tonometry.
Peripheral arterial tonometry (PAT) is a new non-invasive technique that utilizes fingertip plethysmography to measure pulse volume amplitude (PVA). The PVA changes to reactive hyperemia compared to baseline have been shown to be nitric oxide (NO)-dependent, suggesting that PAT is a measure of endothelial function. 10 Furthermore, small studies have demonstrated that PAT measurements correlate with FMD, and PAT hyperemic ratios are lower in patients with increased cardiac risk factors or in patients with underlying CAD. However, there are few large-scale studies relating PAT to other established measures of endothelial function.
The objective of this study was to better define the role PAT plays in endothelial function assessment by assessing its correlation with established vascular function assessment tools and by investigating the relationship between PAT and prevalent cardiovascular disease.
Methods
Participants
Subjects over the age of 18 years who had undergone recent assessment of their endothelial function with both PAT and brachial artery ultrasound at either of two Canadian centers (Foothills Medical Center, Calgary and St Paul’s Hospital, Vancouver) were included. The study included individuals from several separate cohorts, all of which had the same diagnostic criteria for CAD (proven CAD on angiogram). Healthy controls were recruited from the general population with similar inclusion criteria. A total of 304 patients were available for analysis. Of those included, 105 had known CAD and the remainder had no cardiovascular risk factors or known CAD, or symptoms of cardiovascular disease. All subjects consented to participation in the study.
Subjects without coronary disease were control subjects for other studies comparing risk factor groups and control subjects, some of which have been published. 11 Patients with coronary disease all had angiographically proven coronary disease and had medically stabilized acute coronary syndromes. The data included here were the baseline studies prior to any new pharmacological intervention.
Determination of endothelial function
Subjects fasted for a minimum of 8 hours and abstained from caffeine and tobacco for 4 hours prior to their assessment; all subjects were instructed to not take any vasoactive medications on the morning of testing. 12 All measurements were done in a temperature-controlled room, and subjects were acclimatized to the temperature for a minimum of 10 minutes before testing began. Vascular function assessment by both PAT and brachial artery ultrasound was performed simultaneously. PAT studies were conducted using a finger plethysmograph (Itamar Medical, Caesaria, Israel) to determine digital blood volume at baseline and during reactive hyperemia. FMD of the brachial artery was determined using previously described and validated methodology.12,13 The diameter of the brachial artery above the antecubital fossa was measured using B-mode ultrasound, and blood velocity was measured using pulsed-wave velocity Doppler. Baseline measurements were taken and then arterial flow was occluded by inflating a pneumatic cuff to suprasystolic pressures (200 mmHg) on the forearm. Following the 5-minute occlusion, the artery was imaged continuously for 3 minutes.
Analysis
Briefly, automated edge detection software was utilized to measure baseline diameter and peak diameter post-reactive hyperemia (generally between 45 and 90 seconds) for the calculation of FMD. Two end-diastolic frames were averaged for each intervention. FMD was calculated using the formula: % FMD = [(hyperemic diameter – baseline diameter) / baseline diameter]*100%. In our laboratory the intra-observer coefficient of variation for repeated measurements on the same image using the above approach is 4–5%. 13
At the same time as the FMD procedure, patients underwent assessment of pulsatile blood volume responses by PAT to measure the PVA. PAT measurements were simultaneously measured from the index finger of both hands. 11 Results were expressed as an index calculated between the active and control fingers at baseline and during reactive hyperemia. The variable measured is therefore the ratio of PVA index in hyperemia to PVA index at baseline. As the result is automated the intra-observer variability is near zero. In our laboratory the coefficient of variation for PAT is between 13% and 14%. 14
The velocity time integral (VTI) was measured as the first complete velocity envelope post-cuff occlusion traced manually. In our laboratory the intra-observer coefficient of variation for repeated measurements of VTI on the same image using the above approach is 2%. Shear stress at baseline (BSS) and following hyperemia (HSS) was calculated as: (8 × µ × V) / (brachial artery diameter), where µ is blood viscosity and V is brachial velocity. 9
Statistical analysis
Data for our baseline variables are presented as means ± standard deviation. The primary end point of the study was the PAT index. The primary efficacy analysis was the relationship between PAT index and FMD. Comparisons were made between characteristics of patients with and without CAD using t-tests with a pre-determined alpha of 0.05. The PAT index was also natural log transformed (lnPAT) as this end point has been more recently reported.15,16 Univariable analysis was used to compare the correlations between various measurements of endothelial function and available demographics. Backward linear regression was then undertaken to determine predictors of PAT. As VTI and HSS are correlated, VTI was included in the multivariable models and HSS was excluded. Each of these models included variables shown in the univariable analysis to have correlations with a p-value < 0.25. Using a post-hoc power calculator, we have a power of at least 79.2% with our pre-specified alpha of 0.05 for the regression analyses. All analyses were conducted using Intercooled STATA, version 11 (College Station, TX, USA).
Results
The baseline demographics and all vascular function measures of the 304 study participants are shown in Table 1. The subjects included in our study were relatively young, with a mean age of 48.9 years. Approximately one-third of the study subjects had a clinical diagnosis of CAD.
Baseline characteristics of patients undergoing peripheral arterial tonometry testing
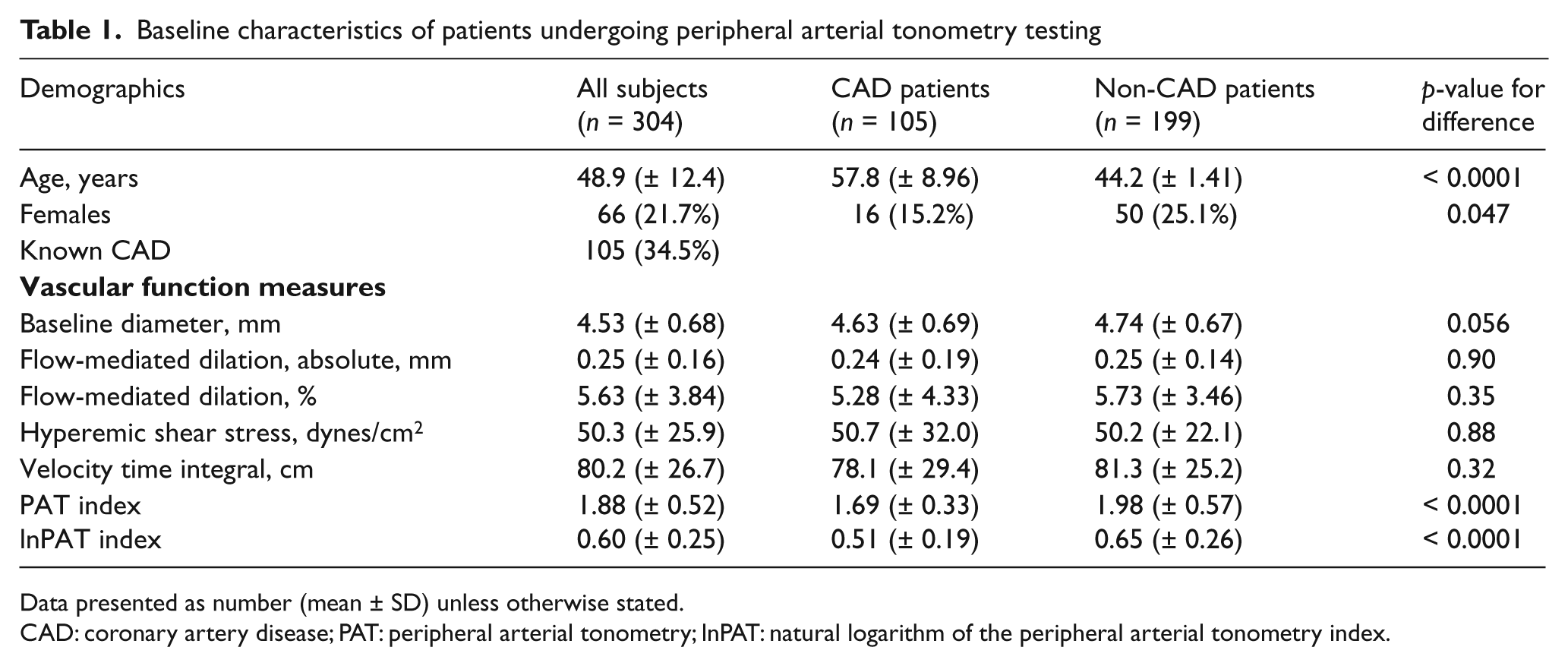
Data presented as number (mean ± SD) unless otherwise stated.
CAD: coronary artery disease; PAT: peripheral arterial tonometry; lnPAT: natural logarithm of the peripheral arterial tonometry index.
Vascular end point correlation
The univariable correlation between lnPAT and our other measures of endothelial function are shown in Table 2. VTI was found to be significantly correlated with lnPAT (r = 0.167, p = 0.004), HSS, a derivative of VTI (r = 0.6524, p < 0.0001) and FMD (r = 0.119, p = 0.039). HSS was also correlated with lnPAT (r = 0.125, p = 0.030). There was, however, no significant correlation between lnPAT and FMD (lnPAT: r = −0.047, p = 0.414).
Correlations between various measures of endothelial function
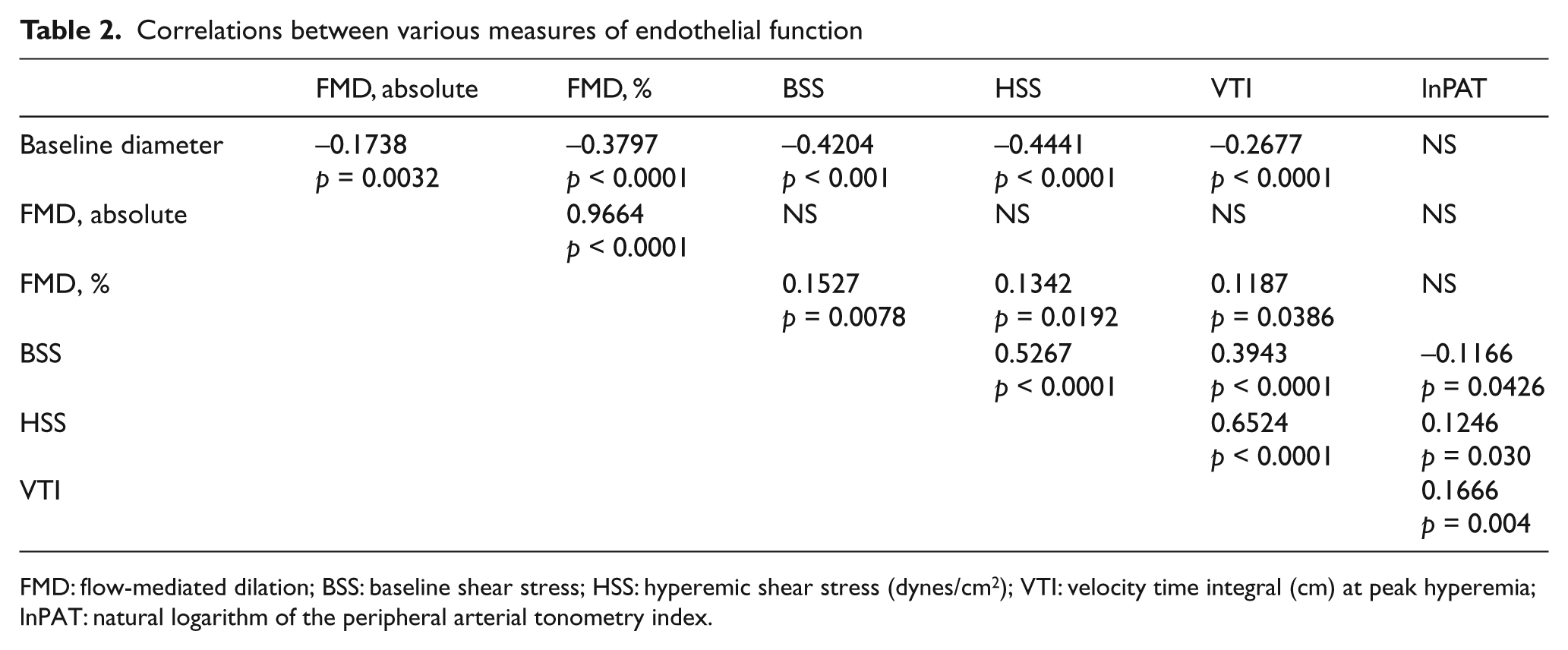
FMD: flow-mediated dilation; BSS: baseline shear stress; HSS: hyperemic shear stress (dynes/cm2); VTI: velocity time integral (cm) at peak hyperemia; lnPAT: natural logarithm of the peripheral arterial tonometry index.
Coronary artery disease, risk factors and the association with vascular function
Those subjects with CAD were older (57.8 vs 44.2 years, p < 0.0001) and more likely to be male (84.8 vs 74.9%, p = 0.047). In terms of endothelial function, those with CAD had diminished lnPAT index (0.51 ± 0.19 vs 0.65 ± 0.26, p < 0.0001) but had similar VTI (78.1 ± 25.2 vs 81.3 ± 29.4, p = 0.322) and percent FMD (5.49 ± 4.46 vs 5.71 ± 3.47, p = 0.629) and HSS (50.65 ± 32.04 vs 50.18 ± 22.06, p = 0.880) as those without CAD. Baseline brachial artery diameter was not significantly different between the two groups (with CAD: 4.63 ± 0.69 mm vs without CAD: 4.47 ± 0.67, p = 0.056).
The associations between age and sex and lnPAT, FMD, and the VTI stimulus were examined in further detail. FMD, lnPAT, and VTI during reactive hyperemia were all unrelated to age (r = −0.020, p = 0.733; r = −0.012, p = 0.841; r = 0.035, p = 0.540, respectively). However, lnPAT and VTI were all significantly lower in males versus females, while baseline brachial diameter was higher. The mean lnPAT in the female subjects was (mean ± standard deviation) 0.66 ± 0.28 versus 0.58 ± 0.23 in males (p = 0.016), the mean VTI was 88.62 ± 24.10 versus 77.81 ± 26.97 (p = 0.003), and the mean brachial diameter was 3.79 ± 0.44 versus 4.73 ± 0.59 (p < 0.0001). FMD was higher in women (7.08 ± 4.06 vs 5.23 ± 3.68, p = 0.0005), mainly because of lower baseline brachial artery diameter.
Multivariable analysis
Stepwise multivariable regression models were constructed for the healthy controls and CAD subjects combined. For the multivariate model only those variables univariately correlated with lnPAT with a p-value < 0.25 were included in the starting model; these variables are shown in the first column of Table 3. In stepwise multivariable regression models, the only measures of vascular function significantly associated with a higher mean lnPAT index were VTI and baseline shear stress (BSS) (Table 3). In the same model, the presence of CAD was associated with a lower lnPAT, and female sex a higher lnPAT index.
Linear regression model for the prediction of the natural logarithm of the peripheral arterial tonometry index (lnPAT) in reactive hyperemia
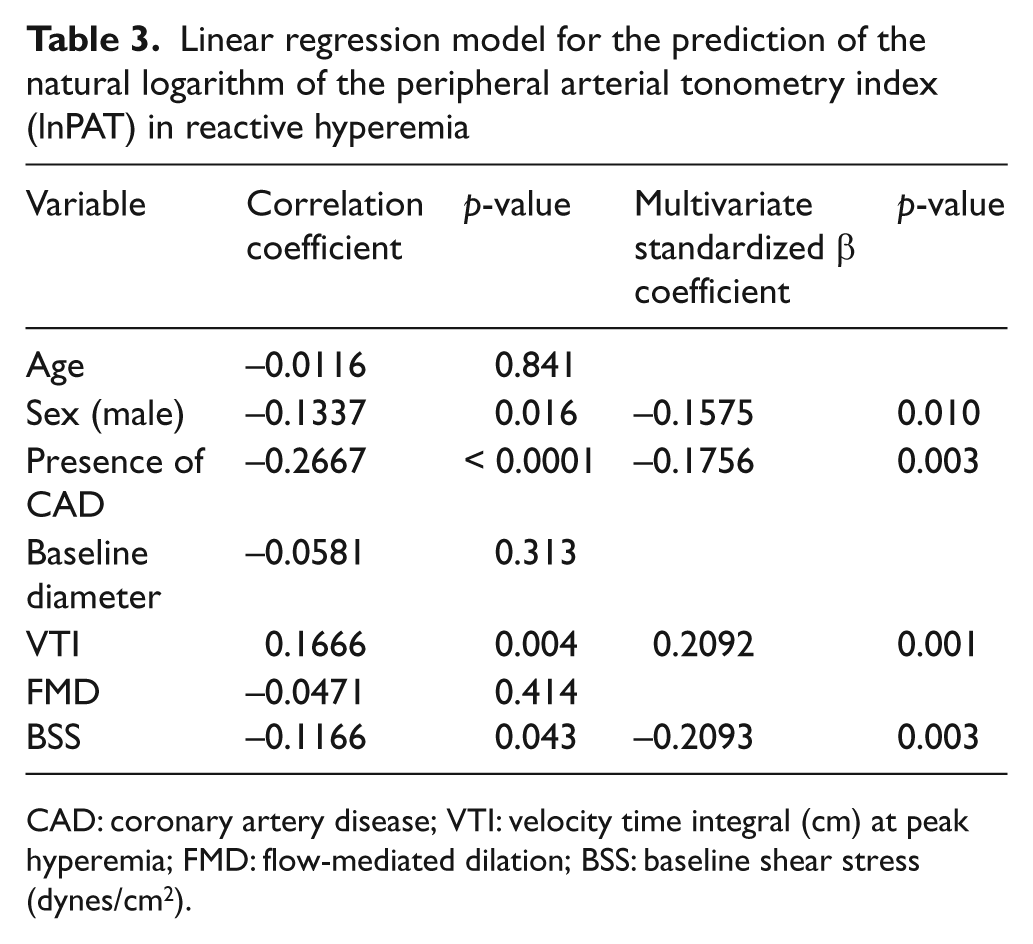
CAD: coronary artery disease; VTI: velocity time integral (cm) at peak hyperemia; FMD: flow-mediated dilation; BSS: baseline shear stress (dynes/cm2).
Discussion
In this study of over 300 subjects, we have demonstrated that lnPAT index is related to other measures of vascular function: namely, hyperemic blood velocity. This provides some potential insight into its mechanism as well as its future utility.
In the context of recent epidemiological studies demonstrating the ability of reactive hyperemic velocity to predict future cardiovascular risk, the association between lnPAT and this measure in our study is promising, although the correlation is not robust and long-term follow-up studies are required to determine whether lnPAT is truly predictive of future cardiovascular events. This relationship has not been previously reported. Mitchell et al. were the first to demonstrate the strength of association between traditional cardiovascular risk factors and shear stress, a derivative of VTI. 7 Subsequent to that, it has been demonstrated that diminished VTI was predictive of future cardiovascular events. 17 In a recently reported study by our own group, we demonstrated a relationship between VTI, but not FMD, and cardiovascular events in middle-aged males. 18
The lack of correlation between FMD and lnPAT is not unique to our study nor is it surprising, as it has been demonstrated in some but not all studies. Aizer et al. found no correlation between FMD and the PAT index in either normal control subjects or those afflicted with lupus in a study of 58 subjects. 19 However, in two separate studies by Dhindsa et al. 20 and Kuvin et al., 21 the PAT index was shown to be associated with FMD – this association may have been due to the fact that each of these studies looked at homogeneous patient populations. The study by Dhindsa considered only 40 healthy young adults, whereas Kuvin’s study considered 31 subjects with overt cardiovascular disease and 29 without, finding a PAT–FMD correlation within each subpopulation, but not across the whole group. In more diverse populations, such as in our study, such correlations were lacking. In particular, in the large, community-based Framingham Heart Study, Hamburg et al. found no correlation between FMD and PAT in over 1800 subjects who had undergone concurrent testing but a correlation between hyperemic flow and PAT in age- and sex-adjusted models. 22 In contrast, a modest correlation between PAT and FMD was shown in the Gutenberg Heart Study. 23 The reasons for this difference are not clear, but may be attributable to methodological concerns. Namely, while the majority of studies, including ours and that by Hamburg, used lower arm occlusion to induce hyperemia, upper arm cuff occlusion was used by Schnabel.
While we have shown that lnPAT is diminished in males, another larger study recently published by Hamburg confirms that and clearly shows that lnPAT was also reduced in those with other cardiovascular risk factors, including diabetes and hyperlipidemia. Hamburg et al. demonstrated that variability in cardiovascular risk factors explained about 16% of the variability in lnPAT in a cohort of about 2000 people with no CAD. 24 In particular, male sex was associated with a lower lnPAT index and advanced age with a higher lnPAT index. This was similarly found in our healthy subjects though, in those with diagnosed CAD, lnPAT was not correlated with age. The explanation for this is unknown at present. That there were similar associations between risk factors and lnPAT and VTI, as well as associations between VTI and cardiovascular events, lends credence to the hypothesis that lnPAT may also be predictive of events and potentially have use in risk stratification of individuals with no overt cardiovascular disease.
Another key finding of our study is that lnPAT was attenuated in the presence of CAD. Whether this was related to the atherosclerosis milieu or the associated risk factors of these subjects cannot be ascertained. However, it did occur in the presence of older age in those with diagnosed CAD, which if anything tends to increase lnPAT. 24 This is not to suggest that PAT should be used for the purposes of diagnosis of CAD, but rather it gives the measure some face validity. A recently published study presents some evidence for the use of PAT in predicting late cardiovascular events. In a study of 270 symptomatic outpatients without established disease, a low lnPAT index predicted future cardiovascular events out to 7 years. 15 PAT has also been shown to relate to the presence of coronary disease, in both obstructive CAD and non-obstructive disease, a notoriously difficult condition to diagnose. In a recently published Japanese study, lnPAT was attenuated in all subjects with ischemic heart disease, even those with non-obstructive disease on coronary catheterization. 16 Heffernan et al. had previously demonstrated that the presence of overt cardiovascular disease, as assessed using myocardial perfusion imaging, is associated with impaired PAT index. 25
Current physiologic evidence indicates that the PAT index is reflective of NO availability, similar to other methodologies used to assess the endothelium in human subjects. Nohria et al. assessed the role of NO in determining digital pulse volume amplitude in a group of 19 healthy subjects.
10
Administration of NG-nitro-
The lack of association between FMD and lnPAT would also suggest that these two variables measure different aspects of vascular function. It is well established that FMD is a NO-dependent phenomenon in the conduit vessel. NO accounts for the majority of dilation in larger vessels. FMD was related to hyperemic VTI and its associated measures of hyperemic flow and shear stress, due to the fact that shear stress is the stimulus for FMD. PAT is thus likely a measure of small vessel function, some of which is NO dependent. However, the control of microvascular dilation to shear stress is much more complex and involves a variety of other mediators, including endothelium-derived hyperpolarizing factor (EDHF), vasodilator prostaglandins, K+ ATP channels and adenosine. 27 The NO contribution of hyperemic VTI is present but minimal. 27 Thus, the association between VTI and lnPAT in the present study demonstrates that the hyperemic stimulus is an important determinant of the PAT response. It may also be that the association infers that they are measuring two different microvascular beds and hence are related.
Likely owing in part to its ease of use, PAT is becoming an increasingly popular methodology for assessing endothelial function. In particular, it has recently been used to assess the efficacy of phosphodiesterase inhibitors in improving endothelial function in diabetic patients, 28 used in a number of sleep and ventilation studies, 29 and used to assess the efficacy of mechanical interventions in heart failure, such as external counterpulsation, 30 without use of other assessments of endothelial function, such as the more validated FMD. The science currently lags behind and physiological studies beyond those highlighted here are still underway to help explore the physiologic basis of PAT assessment.
Limitations
One of the limitations of our study is the fact that we are lacking data on cardiovascular risk factors, as well as some important demographic factors for some of our study participants. In previously published cohort studies, significant correlations were found between the presence of risk factors and PAT impairment. We have only made specific comment on the demographic data present in the majority of subjects, namely age, sex, coronary status and the vascular end points. The small sample size in this study may account for our inability to find associations between certain risk factors and vascular measures.
This study is unique in the number of vascular end points collected simultaneously on a diverse group of subjects (i.e. both those with and without coronary disease). We have found evidence in human subjects that measures of vascular health derived from PAT are related to previously established measures, and are specifically correlated with measures felt to reflect microvascular health. Further, we have shown lnPAT to be diminished in those with CAD.
Summary
The present study has demonstrated a relationship between lnPAT and hyperemic velocity, a measure of microvascular function. In addition, there was no relationship between lnPAT and FMD. This suggests that lnPAT is predominantly a measure of peripheral microvascular function. The attenuation of lnPAT in patients with coronary disease would also suggest that it is an alternate measure of vascular dysfunction in these subjects. Ongoing studies will further evaluate the relationship between various vascular markers and cardiovascular outcomes, clarifying the clinical utility of this parameter.
Footnotes
Acknowledgements
We are grateful to the staff of the human vascular laboratories in Vancouver and Calgary for their expertise in patient recruitment and data analysis, and to the subjects who participated in this study.
Funding
TJA is a Senior Scholar of the Alberta Heritage Foundation for Medical Research (now Alberta Innovates – Health Solution, Edmonton, AB). BJM is also funded by AIHS with a Clinical Research Fellowship. Funding was provided for analysis by a grant-in-aid from the Alberta Heart and Stroke Foundation (Calgary, AB). PAT probes were provided by Itamar Medical (Caesaria, Israel).
Conflict of interest
The authors report no conflicts of interest.