
Abstract
Objectives
The COVID-19 pandemic compelled a portion of healthcare to be delivered virtually. As the pandemic waned, health systems strived to find a balance between re-incorporating in-person care while maintaining virtual care. To find when virtual or in-person encounters are more appropriate, we surveyed pediatricians’ perceptions when comparing the suitability of virtual care to in-person care.
Methods
We surveyed a Canadian tertiary-level pediatric hospital where pediatricians assessed whether specific clinical encounters or tasks were more or less effective virtually than when performed in person. Pediatricians also rated the importance of clinical and patient factors when deciding if a patient needs to be seen in person.
Results
Of 160 pediatrics faculty members, 56 (35%) responded to the survey. When assessing different types of clinical encounters, triage, multidisciplinary meetings, discharge, and follow ups were more likely to favor virtual encounters. However, first consultations and family meetings were more likely to favor in-person encounters. Regarding clinical tasks, pediatricians were more likely to endorse explaining test results, offering treatment recommendations, and obtaining patient histories virtually. On the contrary, there was a preference for physical examinations, assessing patients visually, and assessing developmental milestones to be performed in person. When deciding if a patient should be seen in person versus virtual, pediatricians rated the patient's condition and communication barriers as the most important factors favoring an in-person appointment.
Discussion
These results offer an initial framework for pediatricians when choosing which encounter type may be most appropriate for their patients between virtual or in-person appointments.
Keywords
Introduction
Virtual care in pediatrics has been present for decades; however, its implementation and adoption have varied across sites and time. 1 The coronavirus disease 2019 (COVID-19) pandemic forced a sudden transition to virtual care in response to public health restrictions on in-person care. 2 Virtual care allowed for the continuity of care while minimizing transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection among patients, caregivers, and providers. 3 As the pandemic waned, virtual care remained an essential part of clinical care, reflecting the increased comfort in its use by patients and healthcare providers. 4 Virtual care improves child and family-centred care in pediatrics by increasing access for those with chronic disease 5 ; improving communication between family and providers by allowing the patient's extended circle of care to be present 6 ; and reducing anxiety for parents, care days outside of the home, serious illness, and healthcare costs. 7
While virtual care is cost-effective and offers multiple benefits, barriers exist among patients who need access to or may need to be more familiar with the use of technological devices and virtual platforms. 8 Furthermore, the advantages and challenges of virtual care may vary depending on the context of the patient encounter or the patient's condition. 9 Despite clinics and providers developing clinical workflows for virtual care, there is still a need to understand specific practices within virtual care delivery. A call to understand the core components of pediatric virtual care has been made. 10 These factors have yet to be examined in detail across pediatric specialties. Such factors are crucial in understanding pediatrician experiences in delivering virtual care within clinics and pediatrician preferences regarding virtual care for the future. The objective of this survey study was to understand pediatrician perceptions about the following: (a) the effectiveness of virtual clinical encounters when compared to in-person encounters, (b) the effectiveness of virtual clinical tasks compared to when performed in person, and (c) the importance of clinical and patient factors for considering when a clinic visit should be virtual or in person.
Methods
Study design
A survey was conducted with clinical faculty in the Department of Pediatrics at the McMaster Children's Hospital (MCH), located in Hamilton, Ontario, Canada. This project was a collaboration between the Hamilton Health Sciences (HHS) Centre for Evidence-Based Implementation (CEBI), the HHS Virtual Care Operations Team, and McMaster Children's Hospital. An exemption from the Hamilton Integrated Research Ethics Board was granted as the project was deemed a quality improvement project.
Eligibility criteria
Pediatricians in any division at the MCH who provided virtual care during the COVID-19 pandemic were eligible to participate.
Survey development and data collection
The survey was developed by the HHS CEBI and an MCH working group. Initial items in the survey were developed based on the virtual care experience gathered among the Department of Pediatrics Division Heads. The collected data were grouped into themes, which led to the survey's first draft. The survey draft was revised by the research team that included expertise in survey development, and the revised version was tested in a sample of 10 Faculty members. Further adjustments were made based on their feedback, the final version of the survey was coded into RedCap® and distributed across HHS through email. Participants received an initial email invitation to participate in the study followed by three email reminders at 1-month intervals. The initial invitation and the follow-up reminders contained a direct link to access the survey and provide consent to participate in the study. This study focused exclusively on the clinical faculty in the Department of Pediatrics. A copy of the survey is included as a Supplement.
Provider demographics
The survey collected demographic information, such as pediatrics division and years of clinical practice.
Effectiveness of virtual clinical activities
The first part of the survey included 6-items designed to measure pediatricians’ perceptions of the effectiveness of various virtual clinical activities. This section included the following instructions: “For each type of clinical activity performed virtually, please indicate how effective you feel the virtual clinical activities were compared with your usual in-person care.” The six clinical activities were triage, first consultations, follow-up, discharge, family meetings, and multidisciplinary meetings. Five response options were provided: where 1 = a lot less effective than in person and 5 = a lot more effective than in person.
Effectiveness of virtual clinical tasks
The survey also included 11 items designed to measure pediatricians’ perceptions of the effectiveness of various virtual clinical tasks. This section asked: “For each type of clinical task, please indicate, if performed virtually, how effective you feel the clinical task was performed virtually compared to when performed in person during the COVID-19 pandemic.” The 11 clinical tasks were as follows: obtain the patient's history, assess treatment compliance, perform a physical examination, assess the patient visually, assess developmental milestones, perform a psychosocial assessment, provide psychosocial support, provide clinical information verbally, offer treatment recommendations, explain tests results, and have a serious conversation. Five responses were provided and ranged from 1 = a lot less effective than in person to 5 = a lot more effective than in person. This item set included two additional options: “I never performed this task virtually” and “Not applicable—I do not perform this clinical task.”
Important clinical and patient factors to consider for in-person visits
The third part of the survey included 16 items designed to measure factors pediatricians need to consider when deciding whether to see a patient in person or not. This section included the following instructions: “Based on your current clinical practice, how important are the following factors when deciding if a patient/family needs to be seen in person?” The 16 items covered whether the patient was a new referral, whether the visit was a follow-up, the patient's condition, the progression of the patient's condition, the severity of the patient's condition, how acute the patient's condition was, the patient's risk of deterioration, the presence of a new symptom, the presence of multiple clinical needs, the presence of complex clinical needs, the patient's age, how far away the patient lived, the patient's social context, whether the patient had transportation, the presence of communication barriers, and the patient/caregiver's preference. Six response options ranged from 0 = not at all important to 5 = very important. An overall score of importance, rated on a five-point scale, was determined by weighting the responses.
Analysis
Survey responses were analyzed using summary descriptive statistics. Due to small numbers in some cells, responses that ranged from “a lot less effective” to “a lot more effective” on a five-point scale were rescored into three categories: less effective, just as effective, and more effective. Other survey responses were described as frequencies for each response category.
Results
Provider demographics
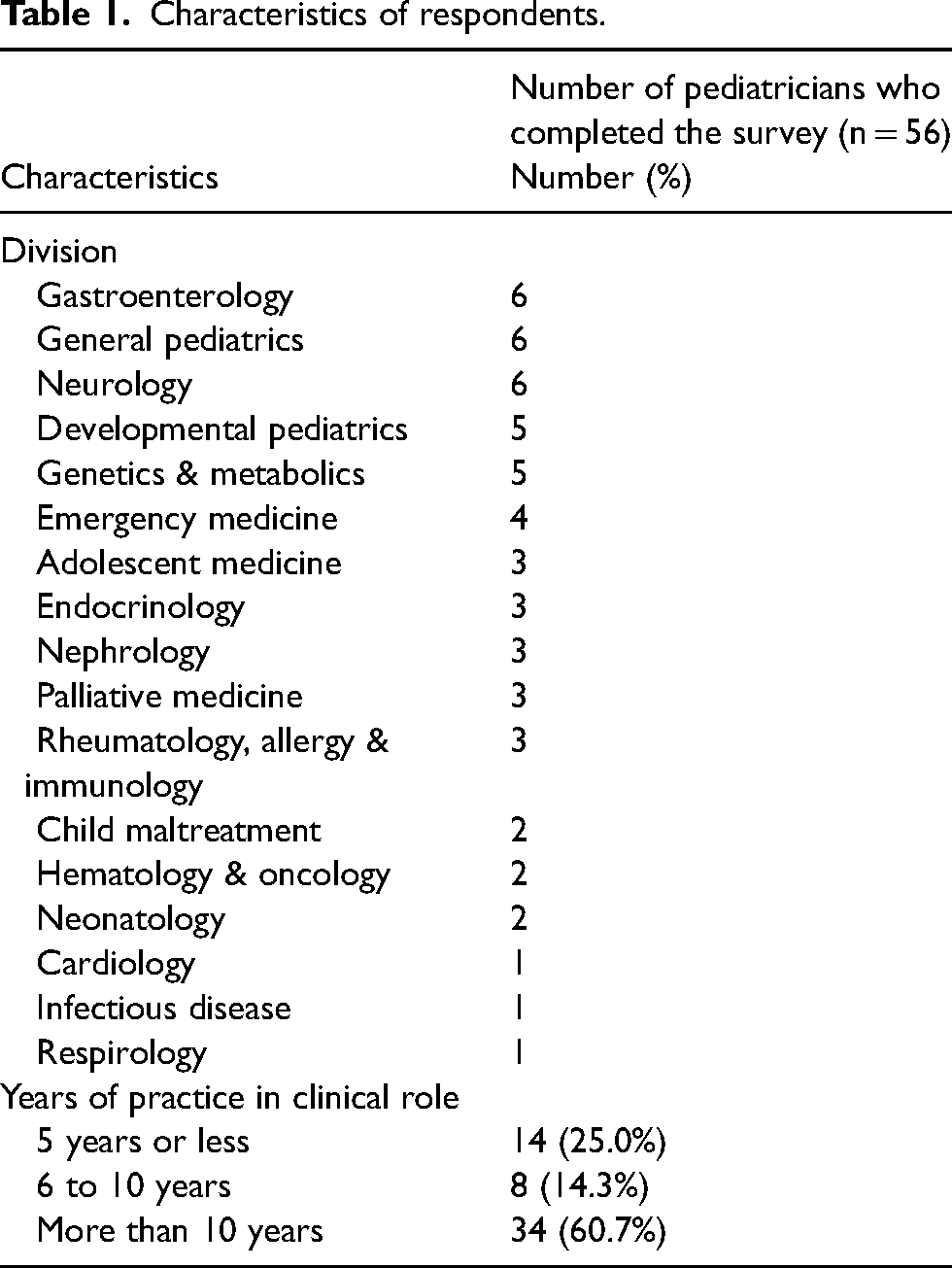
All 160 pediatrics faculty members received an invitation to participate in the survey; of those, 56 pediatricians completed the survey (35% response rate). See Table 1 for pediatrician characteristics.
Characteristics of respondents.
Effectiveness of virtual clinical activities
Clinical activities rated as just as effective or more effective virtually included triage (88%), multidisciplinary meetings (81%), discharge (76%), and follow up (58%). Clinical activities rated as less effective virtually included first consultations (83%) and family meetings (63%). Figure 1 shows the perceptions about the effectiveness of clinical activities.
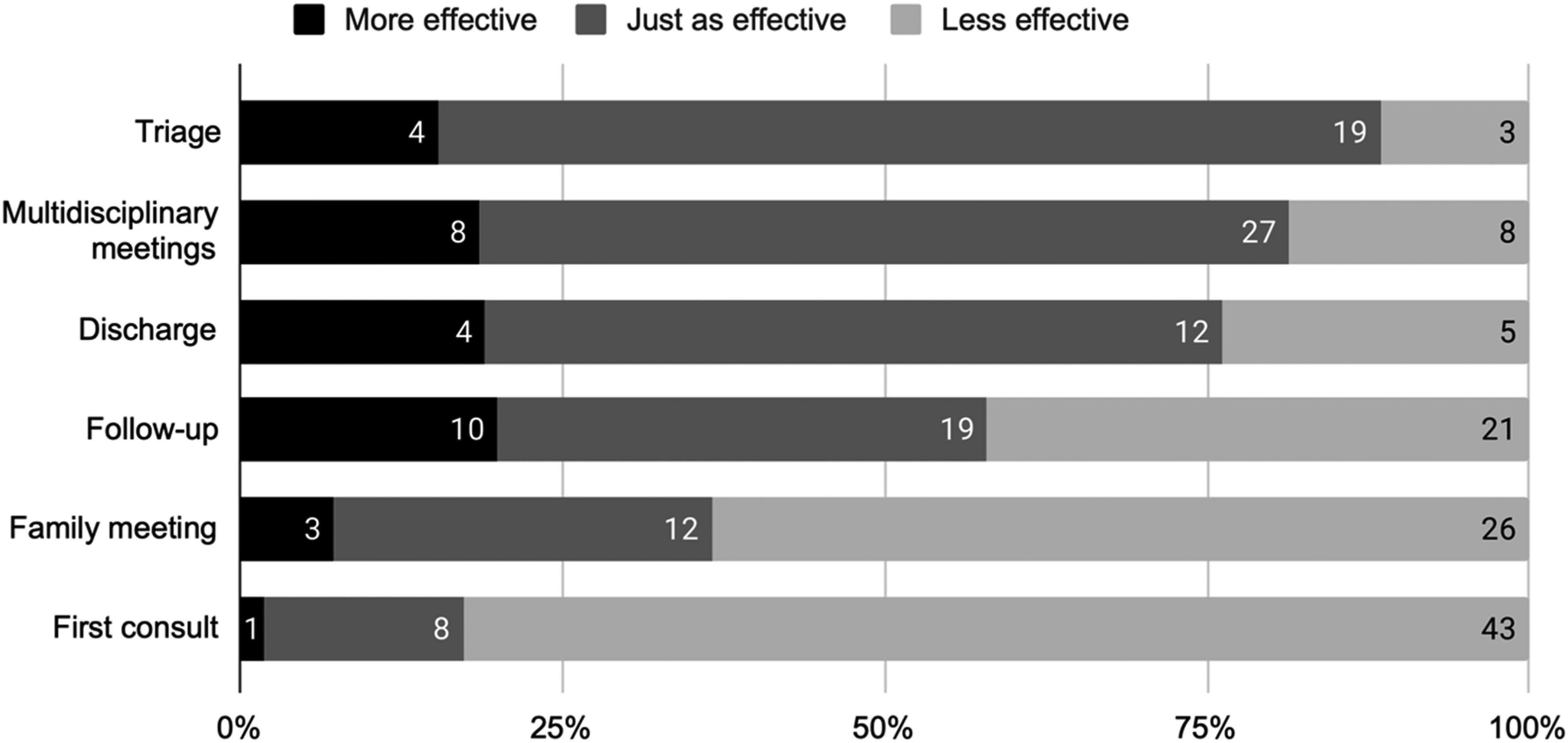
Effectiveness of clinical activities when performed virtually compared to when performed in person.
Effectiveness of virtual clinical tasks
Clinical tasks rated as just as effective or more effective virtually included explaining test results (75%), offering treatment recommendations (69%), obtaining patient histories (67%), assessing treatment compliance (60%), and providing clinical information verbally (58%). Clinical tasks rated as less effective virtually included performing a physical examination (100%), assessing a patient visually (87%), assessing developmental milestones (78%), having a serious conversation (76%), providing psychosocial support (65%), and performing a psychosocial assessment (58%). Figure 2 shows the perceptions about the effectiveness of different clinical tasks.
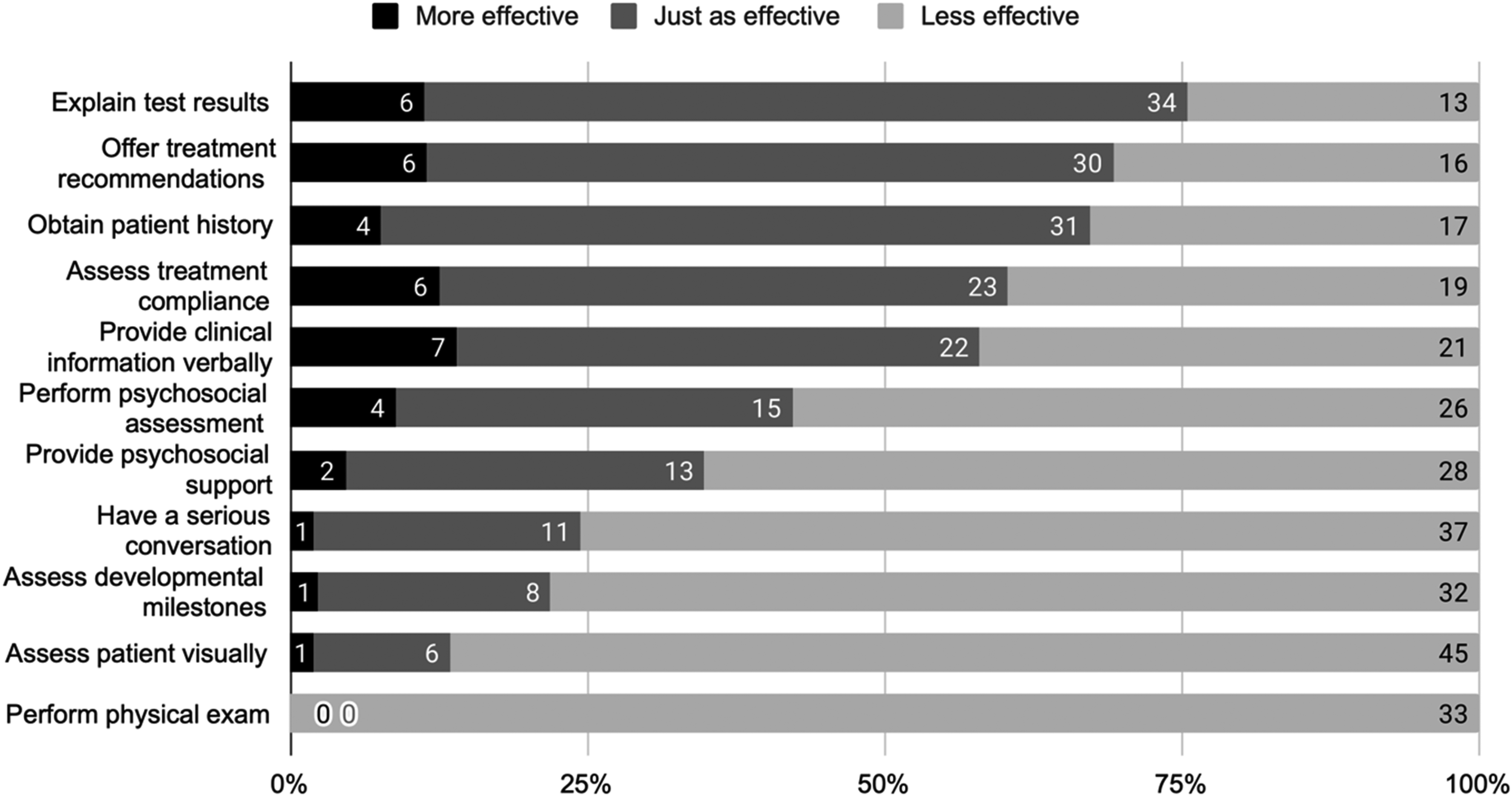
Effectiveness of clinical tasks when performed virtually compared to when performed in person.
Important clinical and patient factors to consider for in-person visits
Important clinical factors included the acuteness of the condition, the patient's condition, their risk of deterioration, the severity of the condition, and the progression of their condition. Patient factors that pediatricians considered important included the presence of communication barriers, whether the patient was a new referral and the patient/caregiver's preference. The patient's age was thought to be the least important factor. Figure 3 shows the perceptions about the importance of clinical and patient characteristics to consider when deciding if a patient needs to be seen in person.
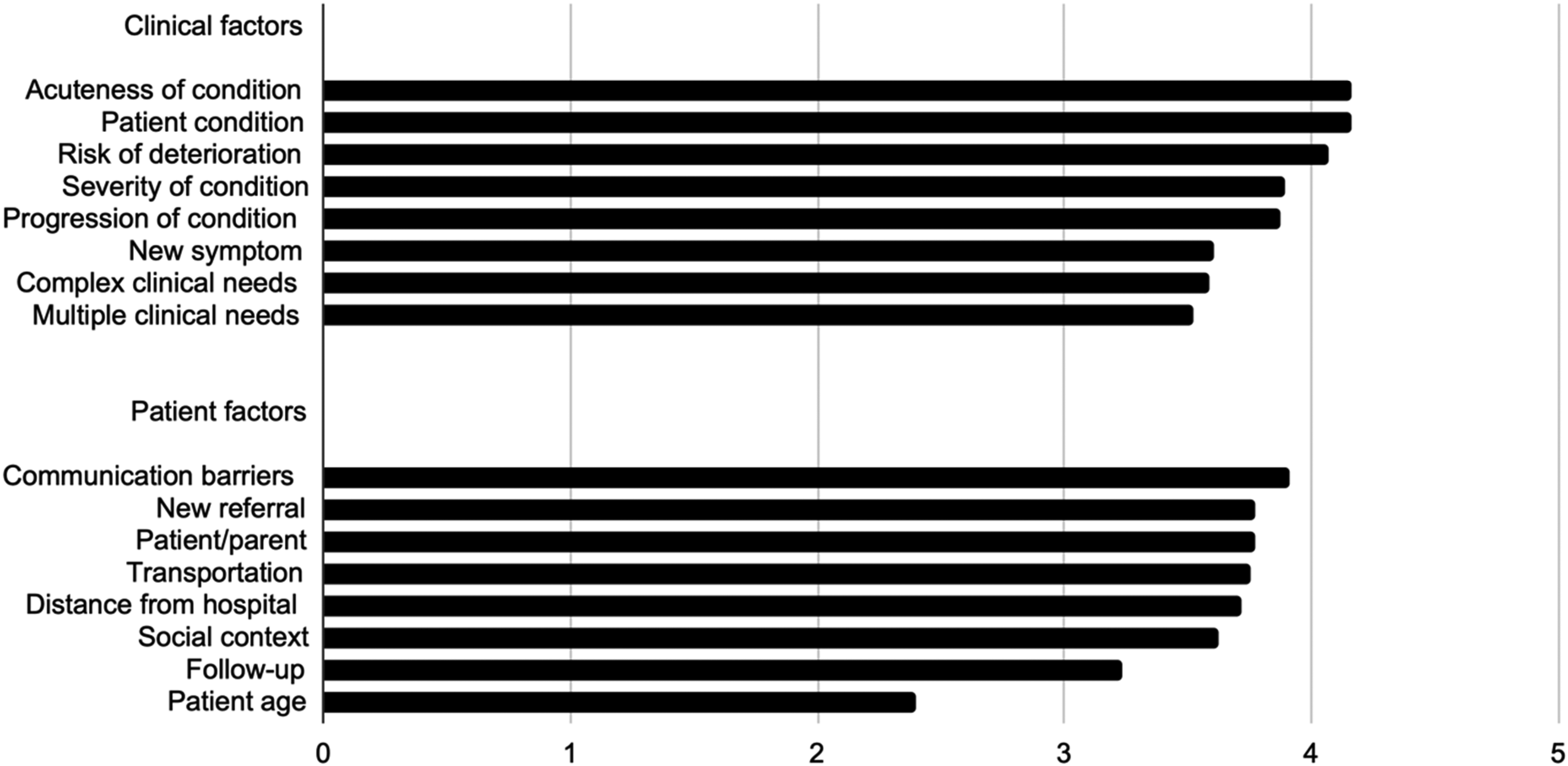
Importance of clinical and patient factors when considering an in-person patient encounter, rated on a five-point scale. 1 = Not at all important; 5 = very important.
Discussion
We conducted a survey to better understand pediatrician perceptions of virtual care during the COVID-19 pandemic. Several clinical encounters and tasks were considered just as effective or more effective when conducted virtually, including triage, multidisciplinary meetings, explaining test results, and offering treatment recommendations. Other encounters and tasks were less effective when conducted virtually, including first consultations, family meetings, performing a physical examination, and assessing a patient visually. Important factors considered when deciding if a patient needs to be seen in person include the patient's condition and the presence of communication barriers.
Pediatricians were more likely to endorse virtual follow-up consultations than virtual first consultations. This might be because virtual follow-up visits reduce the chances of missing appointments, shorten the time required for visits, and decrease costs associated with completing consultations. 11 In contrast, first consultations are more likely to require physical examinations, which are typically more effective when conducted in person. 12 Pediatricians were more likely to endorse virtual multidisciplinary meetings than virtual family meetings. This is consistent with other studies noting that virtual multidisciplinary meetings promote continuity of care, allow for better viewing of images and histological samples, and reduce instances of multiple people speaking simultaneously. 13
On the other hand, family meetings may have been more effective in person as this allows pediatricians to build rapport with the family and discuss important information related to the patient's medical status, prognosis, and goals of care. 14 In addition, triage was more likely to be endorsed virtually. Other studies have shown that virtual triage allows emergency physicians and hospitals to reduce emergency department overcrowding and point patients to the most appropriate care settings. 11
Tasks that involve pediatrician delivery of information or expertise, such as explaining test results, offering treatment recommendations, and providing clinical information verbally, tended to be endorsed as virtual encounters. This finding seems obvious as such tasks do not typically require the patient's physical presence and thus can be made possible via virtual methods of information delivery. 9 In contrast, tasks that involve pediatrician assessment of the patient, such as performing a physical examination, assessing a patient visually, and assessing developmental milestones, tended to be endorsed as in-person encounters. These tasks typically require the patient's physical presence to be conducted accurately and effectively. 15 Thus, replacing in-person physical assessments with virtual encounters might lead to limitations in optimal care.
When deciding if a patient should be seen in person, the patient's condition tends to be an essential factor to consider. The patient's condition influences decisions in clinical settings where the acuity and urgency of the patient's condition are first assessed before redirecting the patient to the most appropriate care setting. 16 Hence, a more serious, urgent, or acute condition might require an in-person visit. Other important factors included the presence of communication barriers and whether the patient was a new referral. Communication barriers, including background noise or a lack of privacy and confidentiality, were some concerns commonly expressed by adolescents during their virtual care experience. 17 Additionally, similar to first consultations, new referrals may be more likely to require a physical examination that is more effective when conducted in person. 18 Patient age was scored as the least important, suggesting that age is not a defining factor in deciding whether in-person or virtual visits are more appropriate.
There were several limitations of our study. First, the survey was conducted in 2021. As such, pediatrician perceptions may have changed since then, especially after gaining more experience with virtual care as the COVID-19 pandemic progressed. Second, the survey sample was small and was from a single site, limiting our results’ generalizability to all pediatricians. Third, the survey questions were only relevant to some respondents. For example, several surveyed pediatricians do not perform triage or discharge. As such, some respondents were unable to assess the effectiveness of every clinical activity or task listed in the survey. Fourth, our survey did not explore other barriers to virtual care. Fifth, while our results showed responses from different pediatric subspecialties, some services were underrepresented or not represented at all, limiting the analysis to their perspective, particularly in specialties with high acuity like intensive care. Reasons for not engaging in the study remain unknown, and due to the anonymity of the responses, no comparison between respondents and nonrespondents could be made.
Virtual care will remain a pivotal component of pediatric care. Assisting pediatricians with the decision-making process of in-person or virtual visits for their patients should remain a priority. Our findings provide the first guiding step to clarify the types of encounters, clinical tasks, and patient traits that help healthcare providers decide if a patient appointment should be virtual or in person. These findings could help develop clinical workflows, improve procedures in health services and be used for training purposes. Future research could focus on assessing how clinical decisions are being made in the longer-term integration of virtual encounters in healthcare while exploring if perceptions and implementation of virtual care have changed after the COVID-19 pandemic.
Supplemental Material
sj-docx-1-jtt-10.1177_1357633X231205329 - Supplemental material for Comparing the suitability of virtual versus in-person care: Perceptions from pediatricians
Supplemental material, sj-docx-1-jtt-10.1177_1357633X231205329 for Comparing the suitability of virtual versus in-person care: Perceptions from pediatricians by Russell Leong, Kate E Sanderson, Anne F Klassen, Elyanne M Ratcliffe and Gregorio Zuniga-Villanueva in Journal of Telemedicine and Telecare
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.