
Abstract
Introduction
Ultrasound imaging is an important aspect of antenatal care, though access to antenatal ultrasound imaging is limited in many developing countries. The objective of this study was to evaluate a pilot programme which aimed to improve access to antenatal ultrasound for rural Ethiopians through enhanced training of healthcare providers (including midwives, nurses and clinical officers) with support remotely provided by obstetricians using a tele-ultrasound platform.
Methods
Thirteen healthcare providers in the North Shoa Zone in Ethiopia completed training to enable them to perform antenatal ultrasound with the remote supervision of an obstetrician via a tele-ultrasound platform. Pregnant women attending an antenatal appointment at two facilities were offered an antenatal ultrasound exam performed by one of the healthcare providers. Image interpretations between obstetricians and healthcare providers were compared. Participants and healthcare providers were invited to complete a questionnaire regarding their experience with tele-ultrasound, and participants, healthcare providers and obstetricians were interviewed regarding their experience with the tele-ultrasound pilot programme.
Results
2795 pregnant women had an antenatal ultrasound exam. Of 100 exams randomly selected to assess concordance between healthcare providers’ and obstetricians’ image interpretations, concordance ranged from 79% to 100% for each parameter assessed. 99.4% of participants surveyed indicated that they would recommend antenatal ultrasound using tele-ultrasound to friends and family. Themes relating to participants’ experiences of having a tele-ultrasound exam were reduced travel and cost, equivalence in quality of virtual care to in-person care and empowerment through diagnostic information.
Conclusion
Healthcare provider–performed antenatal ultrasound – supported by obstetricians via tele-ultrasound – showed high levels of concordance, was well-received by participants and provided rural Ethiopian women with enhanced access to antenatal imaging.
Introduction
Ultrasound imaging is an integral part of antenatal care (ANC) in many countries around the world.1,2 Ultrasound is a valuable diagnostic tool for suspected pregnancy complications such as threatened abortion or ectopic pregnancy.1,3 In addition, the World Health Organization (WHO) currently recommends a routine screening ultrasound for pregnant women before 24 weeks of gestation to estimate gestational age, improve detection of foetal anomalies and multiple pregnancies, reduce induction of labour for post-term pregnancy and improve a woman's pregnancy experience. 1 Unfortunately, access to ANC – and antenatal ultrasound – remains limited in developing countries, where 99% of preventable maternal deaths take place.4,5
Portable and low-cost ultrasound systems have become commercially available, presenting a potential technological solution for offering antenatal ultrasound imaging in low-resource settings such as Ethiopia.6–9 However, a scarcity of healthcare professionals trained in antenatal ultrasound contributes to a lack of access to antenatal ultrasound for pregnant women in Ethiopia. This problem is further aggravated for patients who live in rural areas, as specialized healthcare professionals such as obstetricians are concentrated in urban centres, which can be difficult for women to access. The WHO recognizes that, in some settings due to resource challenges, antenatal ultrasound can be task shifted from physicians and trained sonographers to trained nurses, midwives and clinical officers. 1 However, strategies to ensure quality of care, including through ongoing training and appropriate supervision, are required. 1
Virtual care and telemedicine have gained much traction in offering patients in rural and remote areas improved access to specialty care, as well as ensuring high quality care.10,11 While the use of virtual care has significantly expanded during the COVID-19 pandemic to reduce interpersonal contact and ensure patient and provider safety, technological development and extensive study of the benefits and limitations of virtual care technologies predates the pandemic.12,13 Thanks to its safety and portability, ultrasound is a growing component of telemedicine services. 14 Tele-ultrasound services in which experienced sonographers acquire images which are transmitted to another site for interpretation by a subspecialist physician have been previously established.15,16 New portable, integrated, and affordable tele-ultrasound systems empower practitioners to perform an ultrasound exam under the remote guidance of a specialist via a video link. 14 Tele-ultrasound platforms have the potential to support low- or mid-level providers in performing ultrasound, broadening the group of healthcare providers who may perform ultrasound in low-resource settings. Antenatal imaging may be a particularly important use case for tele-ultrasound17–19 and may address known barriers faced in many developing countries of the need for advanced training in antenatal ultrasound. 20
To address the challenges which rural Ethiopian women face in accessing antenatal ultrasound, we launched the Remote Ultrasound Capacity Building for Antenatal Access (RUAA) pilot project, a capacity building programme to increase access to antenatal ultrasound in the North Shoa Zone in Ethiopia. In this pilot, 14 healthcare providers (7 midwives, 5 clinical health officers and 2 nurses) were trained to perform antenatal ultrasound exams. Pregnant women attending an ANC appointment were offered an antenatal ultrasound exam performed by one of the HCPs. Unique to this project was that ultrasound images were transmitted in real time to an obstetrician located at a main hospital via a tele-ultrasound platform, thereby providing HCPs support and guidance in image acquisition and interpretation during ultrasound scanning.
We used a mixed-methods study design to evaluate the effectiveness of the RUAA pilot. Specific objectives of this study were to assess the feasibility of having HCPs perform antenatal ultrasound with remote guidance and supervision by an obstetrician using a tele-ultrasound platform; to determine the concordance of the HCPs’ interpretation of imaging compared to that of obstetricians’ interpretations; to examine the experiences of pregnant women having an antenatal ultrasound with tele-ultrasound; and to examine the experiences and attitudes of HCPs and obstetricians towards the technology and its implementation. This study may inform the spread and scale of HCP-performed tele-ultrasound for antenatal imaging in low- and middle-income countries and improve access to antenatal ultrasound and ANC.
Methods
Setting
The RUAA pilot was implemented in Ethiopia, a sub-Saharan African country with a population of 114,963,583 people. 21 The country has a high annual population growth rate of 2.5% and a fertility rate of 4.1 births per woman. 21 The high population growth rate, increasing demand for health care, rising healthcare costs and a less developed industrial base and low national income create challenges in effectively providing healthcare services to the population. 22 Healthcare human resources are significantly limited, with only 0.1 physicians per 1000 people, and patients often must travel long distances to see a specialist.21,22 Patients are further challenged by inadequate transportation and limited financial means to travel. 22 Maternal and neonatal morbidity and mortality rates are significantly greater in Ethiopia than in developed countries, with a neonatal mortality rate of 28 per 1000 live births and maternal mortality rate of 401 per 100,000 live births. 21 Gender inequality is prominent in Ethiopia, which has a male-dominated society with high education and employment disparities between men and women. 23 The low status of women and their disempowerment has been shown to be highly associated with poor health outcomes. 23
The RUAA pilot project was implemented at two health centres (Hambiso Health Centre, located in a rural area, and Fitche 1 Health Centre, located in a semi-urban area) and one comprehensive specialized teaching hospital (Salale University Comprehensive Specialized Hospital [SlUCSH]) in the North Shoa Zone of Ethiopia. Prior to the pilot project, antenatal ultrasound was not available at either of these health centres, and patients inconsistently accessed limited ultrasound resources available at SlUCSH. A very small proportion of pregnant women accessed antenatal ultrasound services in Addis Ababa, the capital and largest city in Ethiopia. The catchment population of Hambiso Health Centre is 37,926, of which 19,152 are female and 8393 are women of reproductive age (15–49 years), while the catchment population of Fitche 1 Health Centre is 27,666, of which 14,663 are female and 6122 are women of reproductive age. SlUCSH is one of three regional hospitals in the North Shoa Zone, which has a catchment area of approximately 1.6 million people, and is often the only hospital in the zone with a full time obstetrician.
Challenges in telemedicine implementation in Ethiopia include inconsistent electricity, limited e-health literacy, limited network coverage, and limited internet connectivity. 22 Ethiopia's telecommunications network is one of the least developed in the world, ranking 127th out of the 130 economies included in the Network Readiness Index 2021, and ranking 27th within Africa. 24 The international transmission speed per Internet user was 2 kbits/s as of June 2018, far below the global average of 76.6 kbits/s. 25 In 2019, the mobile cellular subscription rate was 39%, well below the sub-Saharan African average mobile-cellular subscription rate of 80%, and the Internet penetration rate was 20%, also below the sub-Saharan African average of 28%. 25 To support real-time tele-ultrasound consultations as part of the RUAA pilot, a fibre-optic internet connection was installed at SlUCSH and Fitche 1 Health Centre, and a copper-based Internet connection at Hambiso Health Centre was upgraded from 2 Mb to 4 Mb.
Healthcare providers’ training
Fourteen HCPs (six male, eight female) were trained on antenatal ultrasound image acquisition and interpretation through a three-week curriculum developed and provided in-person by the project's lead obstetrician and IT staff (Figure 1). One HCP was on leave during data collection, resulting in 13 HCPs represented in this paper. The HCPs had an average 8.1 years (standard deviation [SD] ± 3.1 years) of experience providing antenatal care, though none of the HCPs had any prior experience using ultrasound or tele-ultrasound technology prior to the study.

A group of healthcare providers participate in a training session on using the ultrasound probe.
The curriculum consisted of didactic and practical components to enable HCPs to perform antenatal ultrasound with remote guidance and supervision of an obstetrician via a tele-ultrasound platform. Topics included in the didactic component included: (1) telemedicine and an introduction to ultrasound, including probe orientation; (2) 1st trimester pregnancy, including indications, patient preparation, normal anatomy, pathological findings, multiple pregnancy, aneuploidy screening and reporting and (3) 2nd and 3rd trimester pregnancy, including indications, normal foetal anatomy, foetal biometry, foetal malformations, placenta, amniotic fluid, biophysical profile and reporting. A 25 question multiple choice test with questions relating to ultrasound physics, antenatal ultrasound acquisition and obstetrical pathology was administered to HCPs before and after the didactic component of the training sessions.
The practical component of the curriculum, which was delivered to two separate groups of trainees, consisted of scanning pregnant patients at SlUCSH with direct supervision by the lead obstetrician. Ultrasound images were obtained using portable ultrasound transducers (Lumify, Philips, Amsterdam, Netherlands) connected to a tablet computer (Galaxy S7 tablet, Samsung, Suwon-si, South Korea).
At the end of the training, the lead obstetrician evaluated each HCP on eight core competencies using a 3-point scale, with a score of 1 indicating insufficient demonstration of the competency, 2 indicating partial demonstration of the competency and 3 indicating complete demonstration of the competency. The clinical competencies assessed were: (1) accurate measurements of biometric parameters, (2) appropriate gestational age estimation, (3) appropriate foetal weight estimation, (4) identification of intrauterine growth restriction and multiple pregnancies, (5) appropriate amniotic fluid volume assessment, (6) conducting effective imaging for locating the placenta including identification of placenta previa and placental anomalies, (7) conducting effective imaging of foetal morphology and (8) identification of foetal malformations in the head, spine, lungs, heart, musculoskeletal, gastrointestinal and genitourinary systems.
Participant recruitment and study cohort
Participants were recruited from women who attended ANC appointments at Fitche 1 Health Center and Hambiso Health Center in the North Shoa Zone, Oromia Regional State of Ethiopia from November 16, 2020 to November 30, 2021. Inclusion criteria were women between 15 and 49 years of age, at least 20 weeks gestational age and those who were able and willing to consent directly or through proxy to participate in the study.
Culturally appropriate radio and television messages were created to educate community members on antenatal care and support recruitment for the tele-ultrasound services offered at Fitche 1 Health Center and Hambiso Health Centre. A 73 s television segment aired for 18 sessions on OBN television station, and a 69 s radio session aired for a total of 18 sessions. The media campaigns supported transparency in the availability of tele-ultrasound services offered at no cost at Fitche 1 Health Center and Hambiso Health Centre. Local health authorities’ support for the project during the media campaigns was aimed at helping contribute to acceptance and local ownership of the project.
Tele-ultrasound exams
Women who attended ANC appointments at Fitche 1 Health Center and Hambiso Health Center were offered an antenatal ultrasound exam in addition to routine ANC during their appointment. Ultrasound images were obtained by an HCP using a Lumify ultrasound probe connected to a Samsung Galaxy tablet computer (Figure 2). Transfer of ultrasound video data between the participant site and the obstetrician's hospital, as well as videoconferencing data to facilitate communication between the participant and HCP and the obstetrician, was facilitated using a videoconferencing platform (Reacts, Innovative Imaging Technologies, Montreal, Canada). An obstetrician supervised the HCPs in performing the ultrasound exams and was available to provide real-time support and ongoing feedback on image acquisition and interpretation through the tele-ultrasound platform. After each exam, the obstetrician was available to speak to the patient regarding ultrasound findings and other relevant aspects of ANC. Ultrasound exams consisted of a combination of routine screening second trimester exams and limited or complete second or third trimester exams based on the participant's clinical presentation.

A healthcare provider performs an antenatal ultrasound exam using a portable ultrasound probe (a). Images are transmitted in real-time to an obstetrician located at SlUCSH via a tele-ultrasound platform (b). The obstetrician, healthcare provider and patient can see and hear each other using the videoconferencing function of the tele-ultrasound platform, allowing the obstetrician to provide guidance to the healthcare provider on image acquisition and interpretation and allowing the obstetrician and patient to speak with each other.
An obstetrician at SlUCSH was available for remote tele-ultrasound consultations for four hours Monday through Friday. As this was insufficient to meet patient demand, two additional obstetricians were recruited from Addis Ababa to remotely supervise antenatal ultrasound exams on Saturdays. This provided an opportunity for women who were in Fitche that day due to the Saturday market to avail themselves of ANC and antenatal ultrasound. As the cost and time associated with travel are understood to be primary reasons for women not accessing ANC, expansion of antenatal ultrasound services to Saturdays was supported by all stakeholders.
Technical support was provided by Canadian Physicians for Aid and Relief (CPAR) project staff and IT specialists from Salale University to facilitate communication between the HCPs and the remote obstetricians. In addition, instructional videos and IT support from Philips and Reacts were available to project personnel.
Image interpretation
A random subset of 100 ultrasound exams from July 1, 2021 to August 30, 2021 was selected to compare image interpretations made by HCPs to interpretations of obstetricians. Parameters which were assessed included presence/absence of foetal cardiac activity, placental location, placental maturity (Grannum classification), amniotic fluid volume, biophysical profile and foetal pathology (including ventriculomegaly, anencephaly, spina bifida, cephalocele, anterior abdominal wall defects and foetal hydrops). Concordance in interpretations between HCPs and obstetricians was represented by counts and proportions for each parameter.
Questionnaires
Following their ultrasound exam, a random subset of 180 participants from July 1, 2021 to August 30, 2021 were invited to complete a questionnaire exploring access to antenatal care, previous exposure to antenatal ultrasound, experience with tele-ultrasound and attitudes towards the technology. Participants were also asked the duration of their travel from their residence to the healthcare facility, and the cost associated with travel. An additional 100 participants who had exams on Saturdays were administered a questionnaire with questions relating to having ultrasound clinics on Saturdays. The HCPs involved in the participants’ care were also given questionnaires eliciting their experiences and attitudes towards the technology. The questionnaires were initially developed in English, translated to local languages Afan Oromo and Amharic and translated back to English to ensure proper translation.
Qualitative analysis
We held a series of discussions with participants to investigate their experience with and attitudes towards antenatal ultrasound, tele-ultrasound and access to antenatal care. Using purposive sampling, we selected 48 pregnant women to take part in focus group discussions and 5 pregnant women for in-depth interviews; 13 HCPs to take part in a focus group discussion; and 3 obstetricians to participate in in-depth interviews. The discussions were recorded, transcribed and translated from Amharic and Afan Oromo to English.
The transcripts from focus groups and interviews from participants, HCPs and obstetricians were analyzed using thematic analysis. 26 This process involved developing initial codes reflective of key concepts in the transcripts, identifying relationships between the codes and combining codes with common elements into categories to best represent the data.26,27 The analysis was a collaborative effort among a local research team at Salale University and a research team at the University of Saskatchewan in Canada. This collaboration allowed an understanding of the local context to be brought to the data analysis from the Salale University research team, as well as an independent viewpoint from the University of Saskatchewan research team which contributed to objective interpretation of the data.
Research ethics
Research ethics approval was obtained from the Salale University Ethical Review Board. Written permission to conduct the project was also obtained from the North Shewa Zone Health Bureau (NSZHB) and each health centre. Written informed consent was obtained from each study participant. The research-related risks and benefits and alternatives, right to withdraw, privacy of participants and confidentiality of data were discussed with potential participants as part of the informed consent process.
Results
Healthcare providers’ training outcomes
The didactic and practical components of the antenatal ultrasound curriculum effectively supported HCPs in achieving competence in performing basic antenatal ultrasound. HCPs scored an average (±SD) of 27.4% (±9.5%) on the multiple choice pre-test and 85.7% (±11.6%) on the post-test. Scores demonstrating HCPs’ attainment of each of the eight clinical competencies are presented in Table 1.
Healthcare providers’ level of attainment of clinical competencies following initial training.
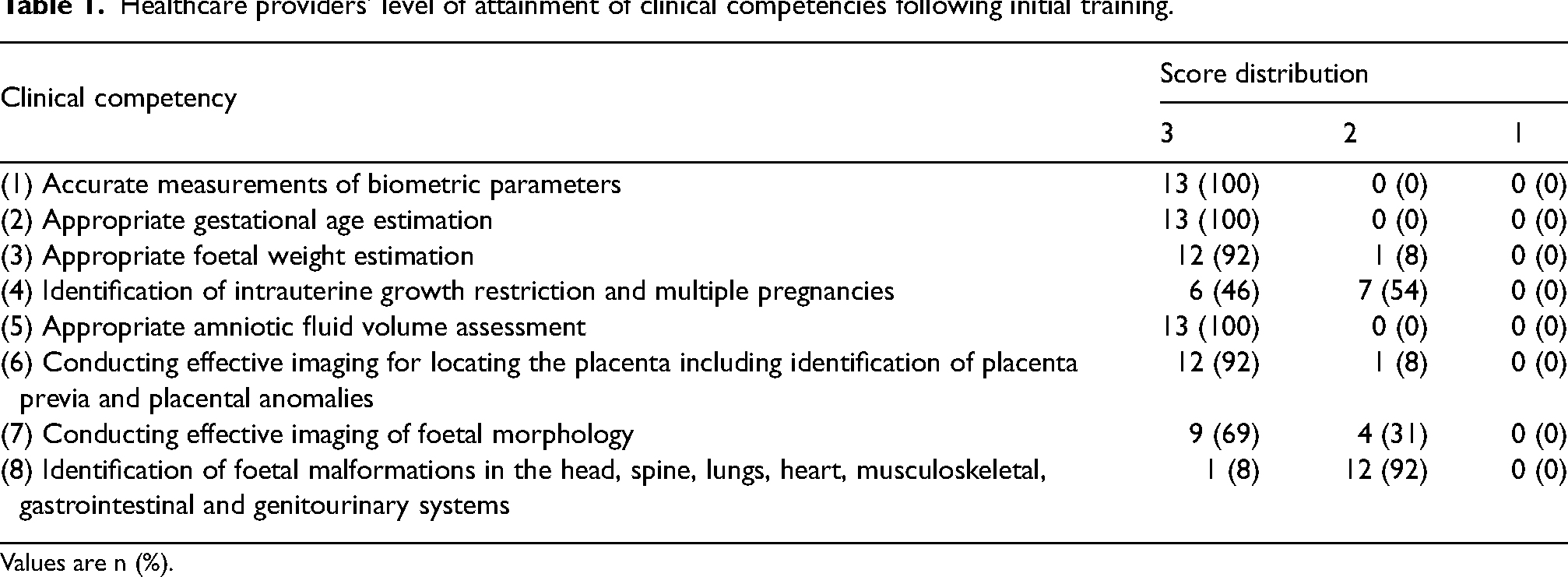
Values are n (%).
Study cohort
Over the course of the pilot, 2795 pregnant women (1419 at Fitche 1 Health Centre and 1376 at Hambiso Health Centre) had an ultrasound exam performed by the trained HCPs with remote supervision by an obstetrician via the tele-ultrasound platform. This number was greater than expected based on the population of the catchment areas of the health centres, and it was noted that women from beyond the catchment areas travelled further than their closest health centre to access ANC because of the antenatal ultrasound service which they heard was available at Fitche 1 Health Centre and Hambiso Health Centre. Of the 2795 participants who had an antenatal ultrasound, 108 (58 from Hambiso Health Centre and 50 from Fitche 1 Health Centre) were referred to SlUCSH to be physically seen by obstetrician for early intervention and/or follow-up. Clinical indications for referral included multiple gestation (n = 35), malpresentation (n = 29), missed or incomplete abortion or intrauterine foetal demise (n = 18), ventriculomegaly (n = 8), anencephaly (n = 5), spina bifida (n = 2), oligohydramnios (n = 5), polyhydramnios (n = 2), foetal hydrops (n = 1), low lying placenta (n = 1) and ovarian cyst (n = 2).
Participant travel
Participants took an average (±SD) of 44.1 (±56.7) minutes to travel to the health centres versus 54.2 (±65.3) minutes to the SlUCSH. Furthermore, travelling to the health centres was less expensive for women than traveling to the SlUCSH. Travelling to the health centres cost on average (±SD) 11.7 (±12.7) Ethiopian Birr, whereas travelling to the SlUCSH cost an average of 20.8 (±20.9) Ethiopian Birr.
Healthcare providers’ versus obstetricians’ image interpretations
The average gestational age of participants randomly selected for image comparisons between HCPs and obstetricians was 28 weeks 4 days, with a range from 14 weeks 0 days to 37 weeks 5 days. Among binary and categorical variables, placental grading (Grannum classification) had the greatest discrepancy between HCPs and obstetricians, with 79% concordance. Concordance of 94% was observed for biophysical profile (BPP), and the remaining anatomic assessments had concordances of 98% or greater (Table 2).
Concordance between healthcare providers’ and obstetricians’ interpretations of ultrasound images.
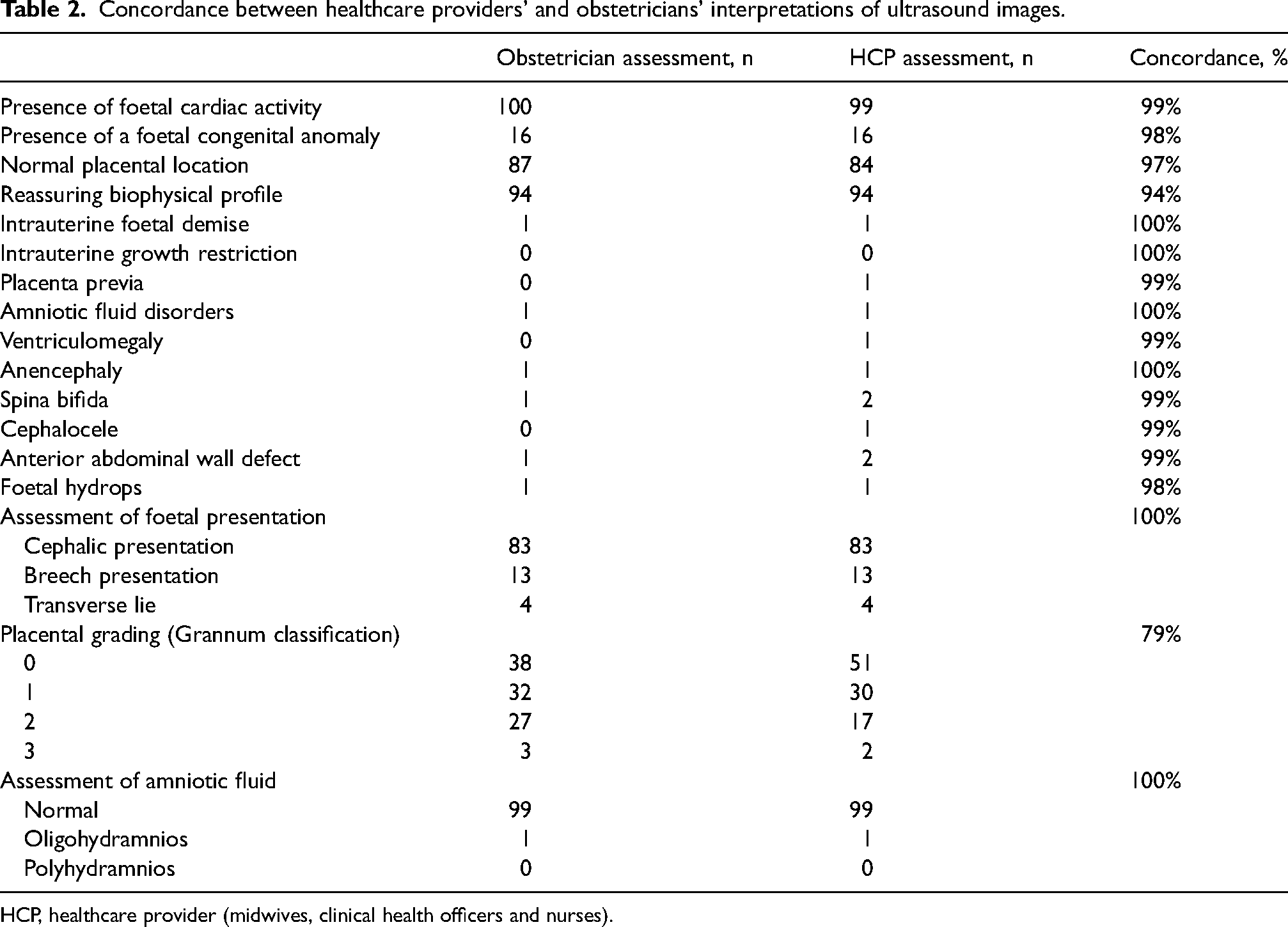
HCP, healthcare provider (midwives, clinical health officers and nurses).
Patient questionnaire
Participants reported an overall positive experience having an antenatal ultrasound using telemedicine (Table 3). Of the 180 participants, 173 (96%) agreed that they felt comfortable during the procedure and 179 (99%) agreed that they would recommend antenatal ultrasound using telemedicine to friends and family. Furthermore, 176 (98%) of the respondents agreed that they would be willing to undergo another antenatal ultrasound through telemedicine and 174 (97%) agreed that they are more willing to use telemedicine again.
Patient and healthcare provider responses to Likert items on the questionnaire.
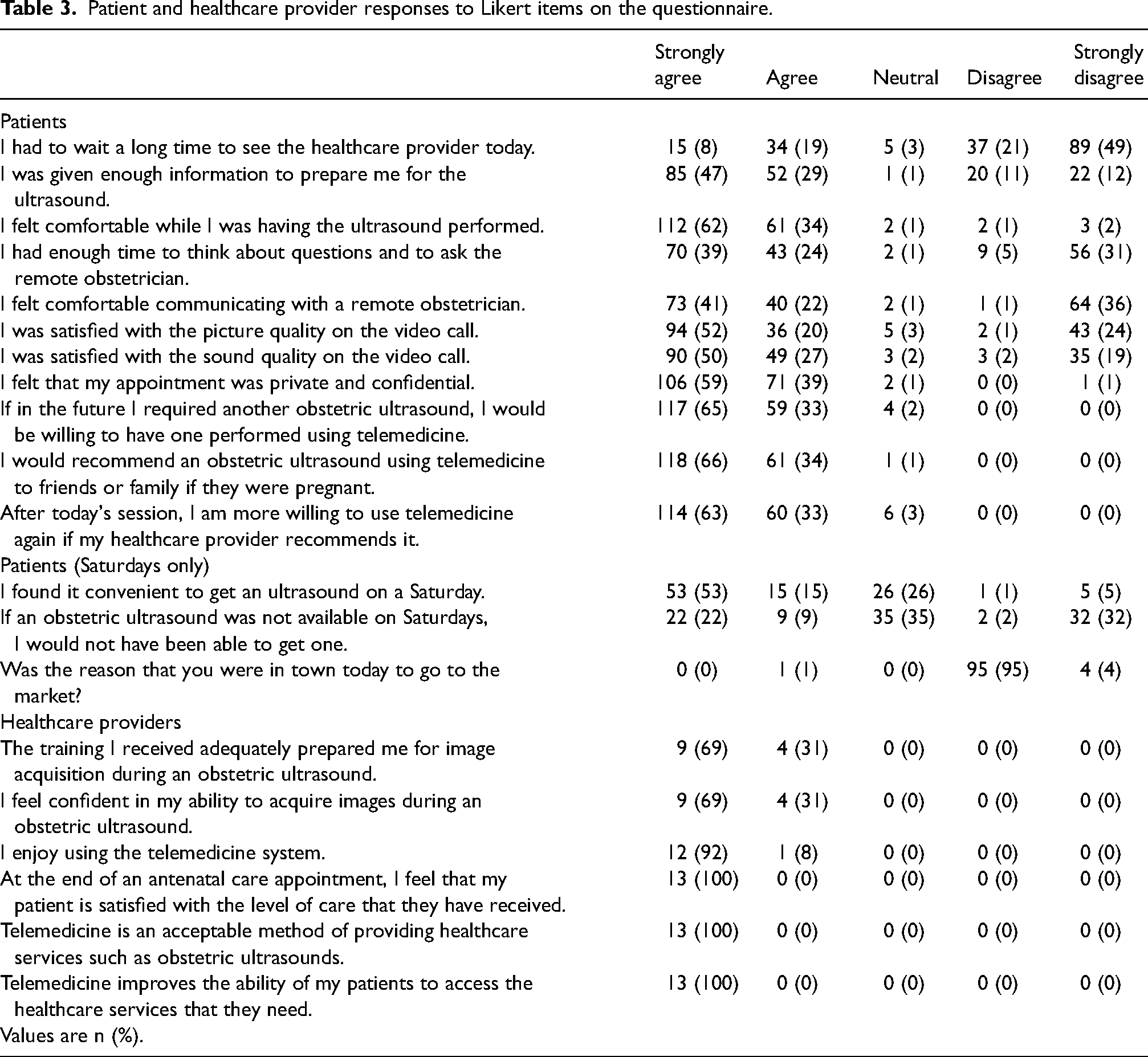
Patients were generally satisfied with the telecommunications technology. 130 (72%) and 139 (77%) of the women agreed that they were satisfied with the picture and sound quality, respectively; however, most of the remainder strongly disagreed. Sixty-four (36%) participants strongly disagreed that they were comfortable communicating with a remote obstetrician but this was not due to a lack of privacy; 177 of respondents (98%) agreed that the encounter was private and confidential.
Many but not all patients were satisfied with the timeliness and information related to care. Most disagreed that they had to wait long to receive healthcare, but 54 (30%) were unsure or agreed that they had to wait a long time to see the healthcare provider on the day of their appointment. Forty-three participants (24%) did not agree that they were given enough information to prepare for the ultrasound and 67 (37%) participants did not agree that they had enough time to think about the questions to ask the remote obstetrician.
Sixty-eight pregnant women (68%) agreed that they found it convenient to receive the ultrasound on a Saturday. Thirty-one patients (31%) agreed with the statement that they would not have been able to obtain an ultrasound on another day of the week other than Saturday and 35 (35%) respondents answered that they were unsure.
Women who received ultrasound exams during the workweek were more likely to be introduced to obstetrical ultrasound for the first time thanks to the programme than those who received the procedure on Saturday. Forty (50%) of the workweek participants and 3 (3%) Saturday participants first heard about obstetrical ultrasound through the RUAA pilot, respectively. However, the proportion of women who were receiving their first antenatal ultrasound was similar between the cohorts (48 [60%] of workweek vs. 67 [67%] of Saturday participants).
Healthcare providers questionnaire
The HCPs were comfortable with the experience of using tele-ultrasound (Table 3). All (100%) respondents agreed or strongly agreed that the training they received adequately prepared them for image acquisition for an antenatal ultrasound, that they felt confident in their ability to acquire images and that they enjoyed using the system. Furthermore, the HCPs felt optimistic about the role of telemedicine in patient care. All (100%) strongly agreed that they felt that patients were satisfied with the level of care that they received, that telemedicine is an acceptable method of providing care in the given context and that the technology improves access to needed healthcare services.
A total of 43 technical issues relating to internet connectivity, the ultrasound probe, or the tele-ultrasound platform were encountered over the course of the pilot and were managed by the project's IT specialists.
Qualitative analysis
Participants. Three themes were identified from focus groups and in-depth interviews regarding participants’ experience with antenatal tele-ultrasound: reduced travel and cost, equivalence in quality of virtual care compared to in-person care and empowerment through information. Participants found that having ultrasound services available at the local health centre eliminated the need to travel to another city for a prenatal ultrasound exam, resulting in time and cost savings. Participants felt that the quality of care received virtually using tele-ultrasound was equivalent to that received if it had been in person. For example, one participant commented, ‘I could feel like [the obstetrician was] face to face; I noticed no difference [to in-person care]’. Participants felt empowered by the information which ultrasound provided them. A participant commented, ‘The advantages of this ultrasound are many; I know my baby's health, gestational age, position, time for delivery and foetal weight. I have obtained the service for free and the doctor with local midwives advised me’. Another participant commented that ultrasound findings of a foetal anomaly directly informed their decision to terminate their pregnancy.
HCPs. The following themes were identified based on focus groups with HCPs: overcoming the learning curve, professional development, and infrastructure and language challenges. HCPs found that although they were initially uncertain about their ability to acquire ultrasound scanning skills, following training and continued practice they gained increased confidence: ‘Although I know ultrasound theoretically, I had never seen it before. I had an internal fear during training that I asked myself, could I perform this ultrasound? After practicing, it became simple and now I can perform it independently. For such an interesting opportunity that is important for our clinic, I am very happy’. HCPs felt that gaining these new skills was important for their professional development. For example, one HCP commented, ‘I have gained skills in performing ultrasound and increased my depth of knowledge, which is important for my future career’. HCPs noted a number of infrastructure and language challenges, including poor Internet connection, intermittent electric power, the need for additional ultrasound units to meet patient demands, and language barriers between the remote obstetrician and local practitioners and patients.
Obstetricians. Improved quality of care, professional satisfaction and infrastructure challenges were three themes identified following in-depth interviews with obstetricians. Obstetricians commented that the tele-ultrasound programme increased the accessibility of ultrasound for rural pregnant women, helping improve obstetrical care: ‘Using telemedicine for ultrasound in a remote area has many, many, many advantages, especially for pregnant women. Examining pregnancy with the support of ultrasound compared to without ultrasound is indeed a remarkable difference. Without ultrasound, you could not identify adequate or inadequate amniotic fluid, exact gestational age, malpresentation, and other findings’. The opportunity to contribute to a pilot programme which offered improved quality of care, particularly for underserved patients, brought professional satisfaction. For example, one obstetrician commented, ‘During my break, I am serving pregnant women from the remote area, which allows me to make a successful contribution for my profession to provide quality mentoring and I am happy with this pilot implementation’. Obstetricians also noted infrastructure challenges which hindered the provision of tele-ultrasound, including intermittent interruption in electric power and poor Internet connection.
Discussion
The RUAA pilot project successfully trained Ethiopian HCPs to perform antenatal ultrasound exams and supported them in performing antenatal ultrasound exams with remote consultation from an obstetrician using a tele-ultrasound platform. The project had positive reception from the Ethiopian women in the North Shoa Zone who had an antenatal ultrasound, with specific benefits including reduced travel time and cost and personal empowerment through the additional information which the antenatal ultrasound exam provided. Of note, participants were comfortable with telemedicine technology, which provided them with enhanced access to an obstetrician at a remote location. As a result, many pregnant women received an ultrasound they would not previously have been able to access, and obstetrical risks were identified and addressed.
The RUAA project helped to provide care consistent with the WHO's 2016 antenatal care guidelines which recommend that pregnant women should be offered one ultrasound exam before 24 weeks’ gestation. 1 Antenatal ultrasound can be used to estimate gestational age, diagnose placenta previa, foetal malposition, multiple gestation, ectopic pregnancy, retained products of conception, foetal anomalies, foetal growth restriction, poly- and oligo-hydramnios, among other conditions. 28 Although healthcare providers widely recognize that ultrasound has an important role in management of pregnancy complications,20,29 a cluster randomized trial involving 47,403 births in five countries (Democratic Republic of Congo, Guatemala, Kenya, Pakistan and Zambia) found no reduction in maternal mortality, near-miss maternal mortality, stillbirth, or neonatal mortality, or increase in ANC utilization or hospital delivery for women with pregnancy complications, among those in clusters with routine antenatal ultrasound available. 30 While the medical community reflects on these results, some of which contrast with results from previous studies,9,31,32 what is clear is that health systems must have the capacity to adequately manage conditions diagnosed on antenatal ultrasound in order for ultrasound to benefit patients, 28 and this capacity should be established prior to commencing an antenatal ultrasound programme. It is also important that ANC programmes develop criteria for appropriate clinical indications for antenatal ultrasound to ensure appropriate use of limited resources.
The development of an antenatal ultrasound programme may provide additional benefits beyond the specific diagnostic benefits mentioned. Many pregnant patients in Ethiopia do not seek ANC, or seek ANC late in their pregnancy, resulting in missed opportunities for appropriate interventions to benefit maternal and foetal health. A study in the Kersa district in Ethiopia, for example, revealed that only 53.6% of respondents accessed ANC during their last pregnancy and only 15.3% had four or more ANC visits. 33 Studies in Uganda and Tanzania have found an increase in general ANC utilization when antenatal ultrasound programmes are developed.9,31,32 Although not specifically evaluated in our study, the widespread enthusiasm for antenatal ultrasound coupled with routine ANC suggests that the RUAA pilot may have promoted routine ANC utilization, particularly as the pilot was largely accepted by men in the community and expecting fathers took a keen interest in the ultrasound services. Many men accompanied their partners to ANC visits, resulting in increased understanding of maternal needs during pregnancy. The RUAA pilot attracted interest from local leaders, government authorities, community members and religious leaders who actively encouraged women and girls to seek services through the RUAA pilot. The potential of an antenatal ultrasound programme to be implemented in rural areas with support from obstetricians in larger centres via a tele-ultrasound platform is particularly promising, as it is known that women living in rural areas are less likely to use healthcare facilities, a pattern attributed to geographic and socioeconomic factors. 34
The number of tele-ultrasound exams performed during the study period far exceeded our expectations. Increasing access during Saturday market days, public culturally appropriate advertising and the support of local authorities may have contributed to this increase. However, the empowerment of pregnant women who want to ensure their health and the health of their unborn babies may have been a major factor in this high level of participation.
An additional potential benefit of the RUAA pilot was the significant decrease in staff turnover at the health centres during and after the RUAA pilot. None of those who completed ultrasound training has left their position at the time of writing. This raises the possibility that the use of innovative technology and increased scope of practice may decrease healthcare provider attrition.
Other studies have similarly trained lower-level obstetric providers such as midwives, nurses and clinical health officers to perform antenatal ultrasound exams using portable ultrasound probes.6,8,35,36 For example, a pilot project in Kenya trained midwives to perform basic ultrasound to identify high-risk pregnancies, and used an internet connection through a mobile phone to transmit the acquired images to a main hospital for radiologists to review the images and validate the reports. 6 In the 20 patients identified as high risk, two discrepancies were identified between image interpretation versus actual outcomes, and three adverse pregnancy outcomes from 220 patients available for follow-up were observed with no ultrasound correlate or possible etiology previously identified on midwife-performed ultrasound. 6 An advantage of the ultrasound system used in our study in Ethiopia is the real-time guidance available from an obstetrician via the tele-ultrasound platform. In resource limited settings and a health system with a shortage of doctors, task shifting antenatal sonography to HCPs may reduce obstetricians’ workload and minimize physician resources. While concordance between HCPs’ and obstetricians’ image interpretations appears to be high in our study, ultrasound images were obtained only by HCPs, with no comparison to images obtained directly by obstetricians. Further research in a larger study with direct comparison to expert-obtained images or appropriate patient follow-up is suggested to determine whether a tele-ultrasound (remotely mentored scanning) feature increases diagnostic accuracy.
There are a few limitations of the study. While images were interpreted by both HCPs and obstetricians to assess concordance in interpretation, ultrasound exams were performed by only HCPs, with no exams also performed by obstetricians to assess concordance in biometric measurements and anatomic findings. Many significant findings which may not have been appreciated and captured by HCPs or not observed due to scanning technique may not be available for an obstetrician's review, potentially leading to a falsely high concordance rate between HCPs and obstetricians. As such, comparisons between HCPs’ and obstetricians’ interpretations must be interpreted with caution. Due to the low prevalence of some clinically significant findings on the foetal anatomic survey, the small sample size of 100 participants further limits the comparison of interpretations between HCPs and obstetricians. As the study was conducted across only two facilities in a single zone in Ethiopia, findings of this study may not be generalizable to other settings due to differences in local resources, expertise and cultural expectations.
Conclusion
The RUAA pilot project demonstrated the potential of increasing antenatal ultrasound capacity in a low-resource region of Ethiopia through training HCPs to perform an ultrasound exam using a portable ultrasound transducer and supporting them through remote consultation with an obstetrician via tele-ultrasound. The overwhelmingly positive response from patients, HCPs and obstetricians motivates further continuation, refinement and expansion of this programme, and the exciting potential to spread and scale this pilot across other regions of Ethiopia and other low- and middle-income countries.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Institutional review board statement
This study was approved by the Salale University Ethical Review Board.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Fund for Innovation and Transformation, Global Affairs Canada, Manitoba Council for International Cooperation, Blossom Foundation, Canadian Physicians for Aid and Relief, Inter-Council Network.