
Abstract
Introduction
A wide range of study designs have been utilized in evaluations of home telemonitoring and these studies have produced conflicting outcomes over the years. While some of the research has shown that telemonitoring is beneficial in reducing all-cause mortality, hospital admission, length of stay in hospital and emergency room visits, other studies have not shown such benefits. This study, therefore, aims to examine several home telemonitoring study designs and the influence of study design on study outcomes.
Method
Articles were obtained by searching PubMed database with the term heart failure combined with the following terms: telemonitoring, telehealth, home monitoring, and remote monitoring. Searches were limited to randomized controlled trial conducted between year January 1, 2000 and February 6, 2021. The characteristics of the study designs and study outcomes were extracted and analyzed.
Result
Our review of 34 randomized controlled trials of heart failure telemonitoring did not show any significant influence of study design on reduction in number of hospitalizations and/or decrease in mortality. Studies that were done outside North America (USA and Canada) and studies that selected patients at high risk of re-hospitalization were more likely to result in decreased hospitalization and/or mortality, though this was not statistically significant. All the studies that met our inclusion criteria were from high-income countries and only one study enrolled patients at high risk of re-hospitalization.
Conclusion
There is a need for more studies to understand why telemonitoring studies in Europe were more likely to reduce hospital admission and mortality compared to those in North America. There is also a need for more studies on the effect of telemonitoring in patients at high risk of hospital readmission.
Introduction
The use of various electronic devices to track patients’ health status while at home, an intervention that has been named “telemonitoring,” has continued to gain traction in the medical field. Telemonitoring allows patients and their health care providers to monitor and record their weight, blood pressure, and other parameters. Health care professionals obtain the information that has been measured and recorded through communication technology.1,2 This technique is especially useful for patients with chronic disease, which is encouraged by their health care providers to monitor some of their vital signs daily. Rather than having to continuously present to clinics or hospitals to have these measurements taken, patients can record this data from the comfort of their homes.1,2 This is usually accompanied by frequent communication with a health care professional, telephonically or via video call, for additional assessment and recommendations. Telemonitoring may lead to an improved quality of care, reduced risk of readmission to hospital, better patients’ satisfaction, and other benefits.1,2
Heart failure is a chronic disease and a major public health problem, with a prevalence of over 5.8 million in the USA and over 23 million worldwide. 3 Heart failure is a complex clinical syndrome caused by structural or functional impairment of ventricular filling or blood ejection and manifests as dyspnea, fatigue, and/or fluid retention. 4 Heart failure is associated with high morbidity and mortality and recurrent admissions after an index hospitalization for heart failure, with a 50% readmission rate, and a 25%–35% incidence of death at 12 months. 3 Usually, patients tend to start gaining weight because of fluid retention, get short of breath or have worsening leg swelling, few days prior to them needing admission for intravenous medications.3,5 If proper interventions are made in a timely manner by adjusting the home medications, these admissions could be avoided. However, it will be challenging for patients who are monitoring themselves to make what may be perceived as complex decisions on medication management and so sharing of data with health care providers is an important aspect of home telemonitoring. Home telemonitoring in heart failure patients could potentially be associated with better clinical outcomes. However, telemonitoring studies in heart failure patients have produced conflicting outcomes over the years. While some studies showed that telemonitoring was beneficial in reducing all-cause mortality, hospital admission, length of stay in the hospital, and emergency room visits,6–8 others did not show such benefits.9–12 The diversity of telemonitoring study designs and outcomes makes it imperative to carefully review the impact of study design on study outcomes. This literature review aims to examine the different home telemonitoring study designs and their influence on study outcomes.
Method
Articles were obtained by searching PubMed database with the term heart failure, combined with the following terms: telemonitoring, telehealth, home monitoring, and remote monitoring. Searches were limited to randomized controlled trials conducted between January 1, 2000 and February 6, 2021. The searches produced a total of 461 articles, of which 281 were unique articles. One additional article identified through other sources was added. The 282 abstracts were independently reviewed by two researchers to assess if they met the inclusion and exclusion criteria to be included in the review. To be included in the review, the articles must have been randomized controlled trials of heart failure patients, written in English, involving patients that were self-measuring their vital signs (such as blood pressure, weight, pulse) at home, while using a device or technology that transmitted the data to health care professionals. Articles excluded include articles not in English (n = 9), articles on telemonitoring study protocol (n = 28), articles that used implantable devices such as pacemakers (n = 43), articles that did not include self-monitoring or did not measure heart failure patients’ hospitalization or mortality (n = 109), articles on teleconsulting (n = 31), articles studying another disease in heart failure patients (n = 15), and articles that pooled results for patients with heart failure and patients with other illnesses (n = 13) (Figure 1). For articles that included heart failure patients as well as patients with other illnesses but provided separate results, we reported only the result of the heart failure patients.
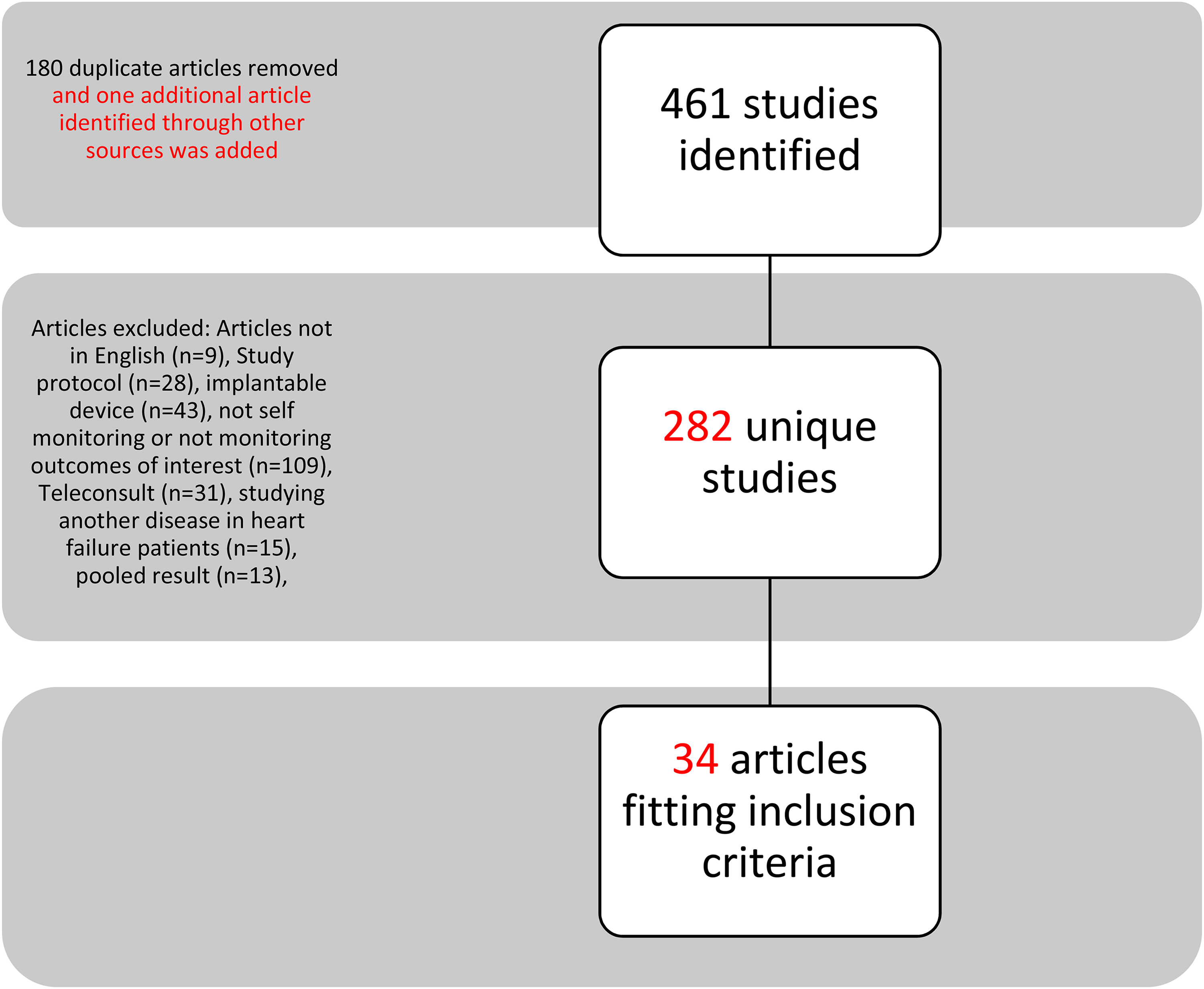
Article selection process.
The characteristics of the study designs and study outcomes were extracted and analyzed. Descriptive analysis of the characteristics and outcomes of the study was done using mean and frequency. Bivariate and multivariate analyses of the effect of different study variables on positive study outcome (reduction in the number of hospitalization and/or decrease in mortality) were done using chi-square, t-test and logistic regression, with a p value of 0.05 considered as significant. The statistical analysis was done using IBM SPSS version 27. The study population, design, duration, outcomes of interest, significant findings as well as the country each study was performed in was categorized for each of the 34 included papers, and this data is reported in Table 4.
Papers included in the review.
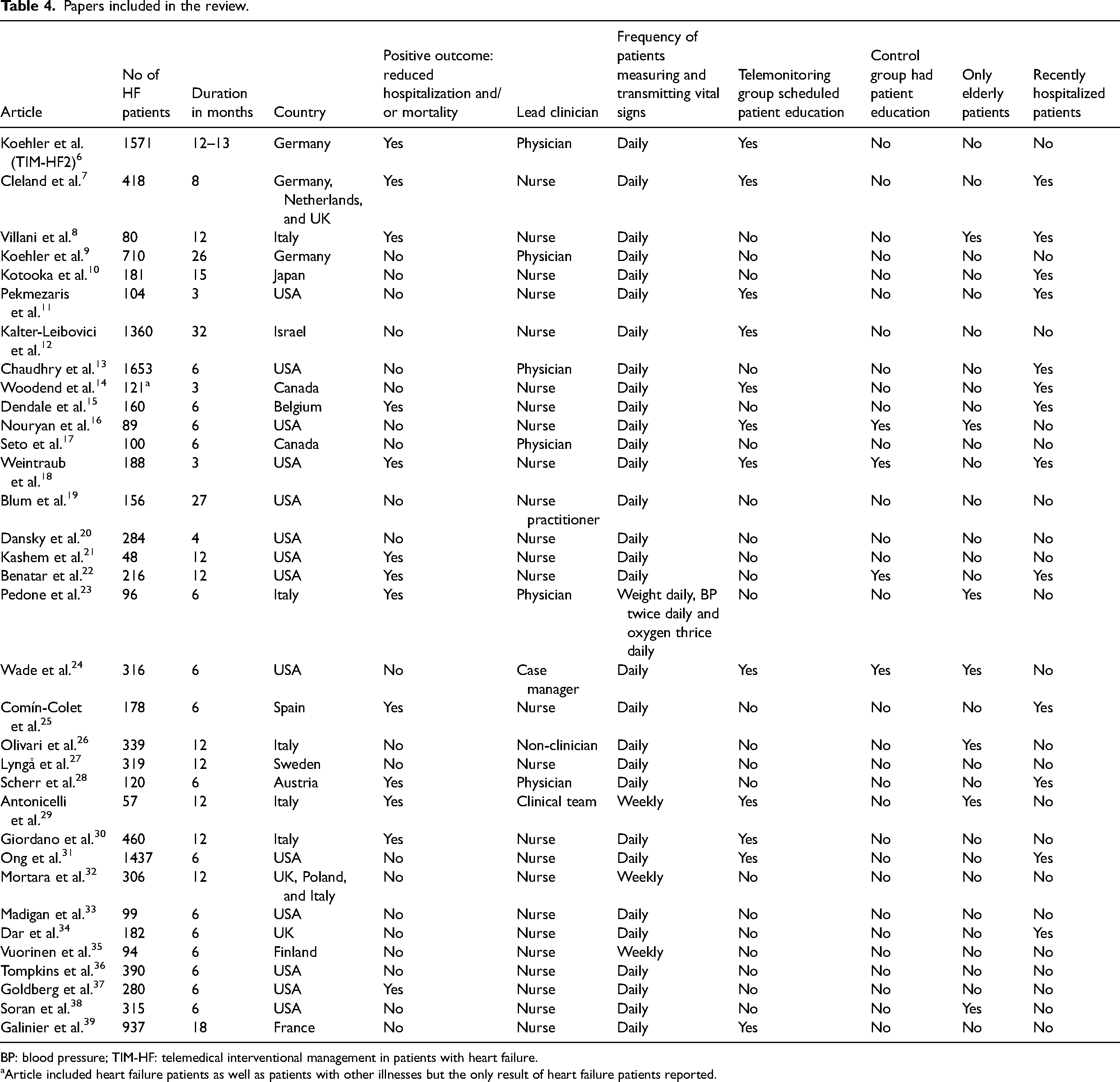
BP: blood pressure; TIM-HF: telemedical interventional management in patients with heart failure.
Article included heart failure patients as well as patients with other illnesses but the only result of heart failure patients reported.
Results
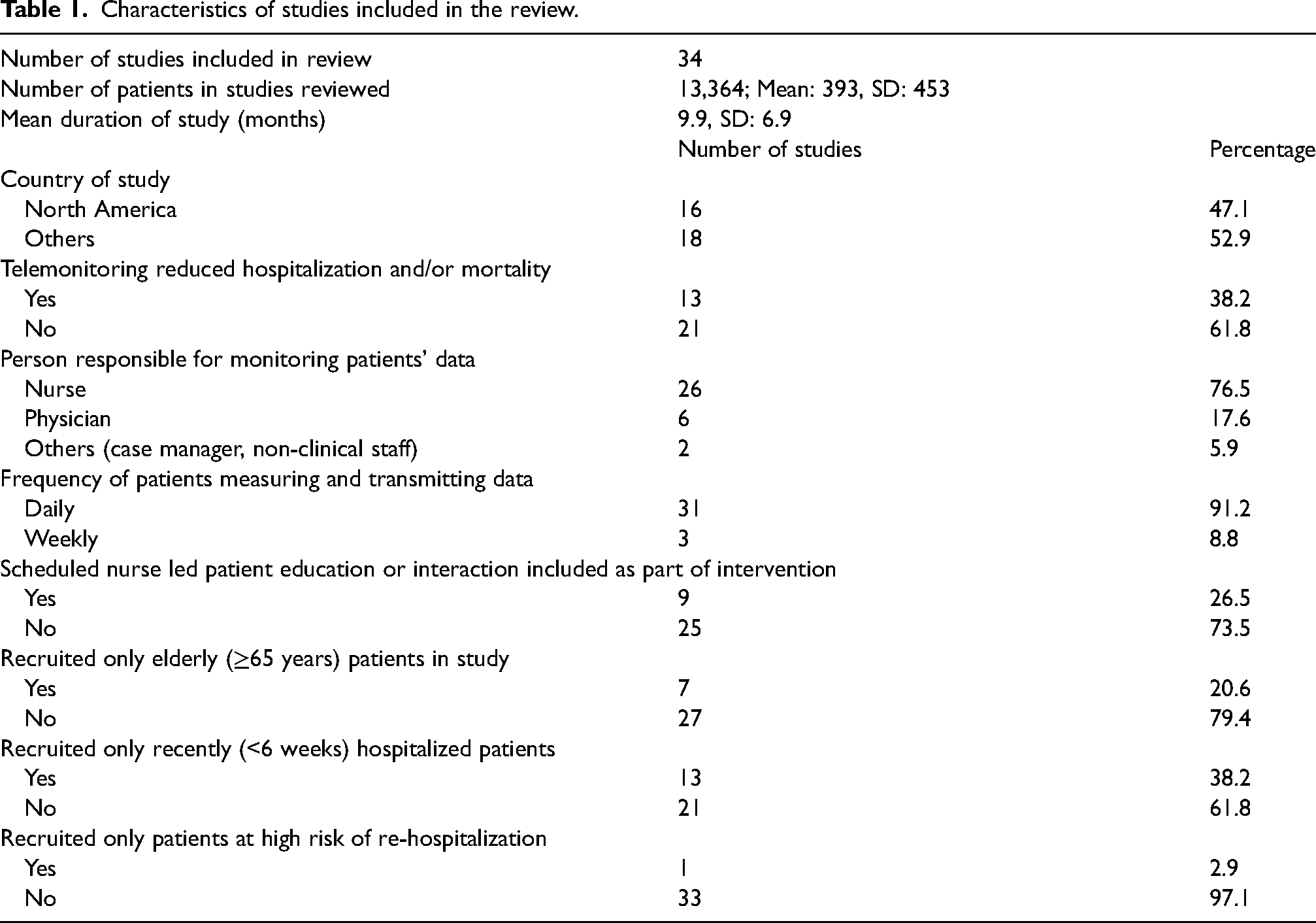
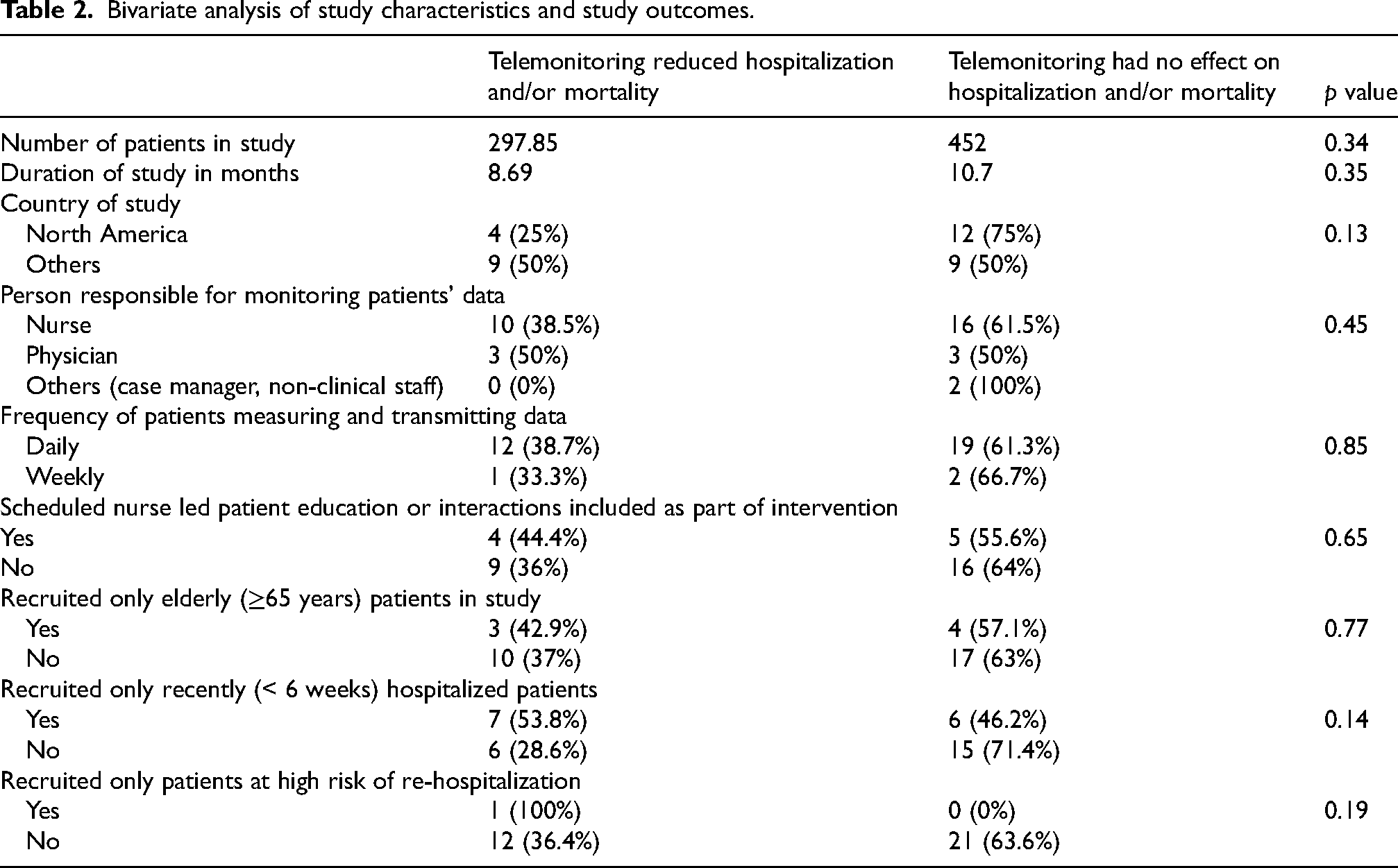
Our study involved a review of 34 randomized controlled trials on heart failure and telemonitoring conducted between January 1, 2000 and February 6, 2021. A total of 13,364 patients were recruited in all the 34 studies with a mean of 393, standard deviation of 453 and a range of 48–1653 (Table 1). There was no statistically significant relationship between the number of patients in the studies and study outcome (p = 0.34) (Table 2). The mean duration of study was 10 months with standard deviation of 7 months and range of 3–32 months. There was no statistically significant relationship between the duration of the studies and study outcome (p = 0.35) (Table 2). The positive outcomes of interest in our review were the reduced number of hospitalizations and/or decrease in mortality. Thirteen of the 34 studies (38%) reported a positive outcome (reduction in the number of hospitalization and/or decrease in mortality).
Characteristics of studies included in the review.
Bivariate analysis of study characteristics and study outcomes.
Country of study and study outcome
Sixteen studies were done in North America (USA: 14, Canada: 2) (47%), and the rest were performed mainly in Europe, with Italy having the highest number of studies (five studies). While only 25% of studies done in North America had a positive outcome (reduction in the number of hospitalization and/or decrease in mortality), 50% of studies done in other countries had a positive outcome. However, there was no statistically significant difference in outcome based on the region where the study was conducted (p = 0.09) (Table 3)
Multivariate analysis of study characteristics and study outcomes.
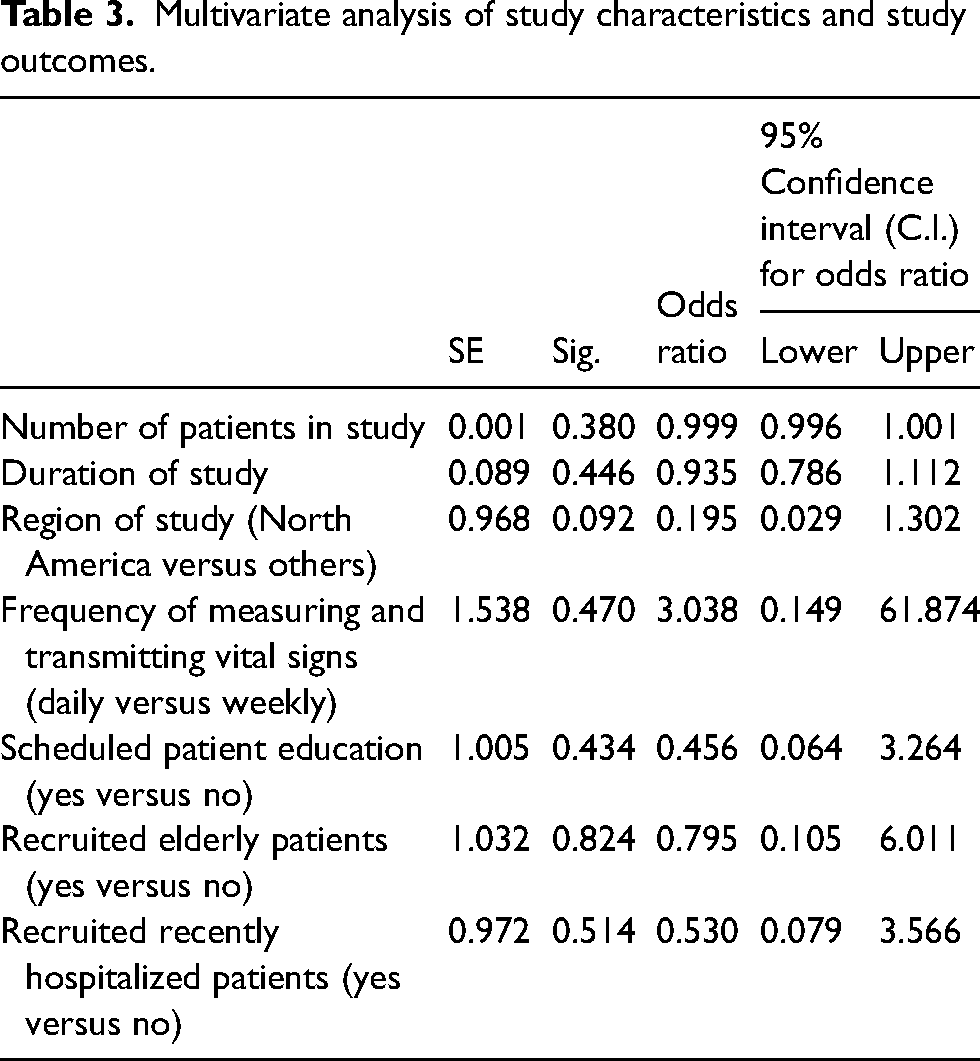
Type of patients recruited in the studies and study outcome
There was a diversity of heart patients recruited in the studies. Some studies recruited only patients with systolic heart failure while most studies included both systolic and diastolic heart failure patients. While some studies recruited patients, who were recently hospitalized for heart failure, others recruited only elderly patients. Our analysis did not show a statistically significant difference in study outcomes based on the type of patients recruited in the study. Only 54% of studies that recruited patients recently hospitalized for heart failure, defined as heart failure hospitalization within 6 weeks of being recruited in the study, had a positive outcome (p = 0.14). There was no difference in outcomes in studies that recruited only elderly patients (≥ 65 years) and those that did not (p = 0.77) (Table 2). However, the only study that enrolled patients at high risk of readmission, defined as patients with New York Heart Association class III/IV patients with at least two of the following: >2 heart failure in the last 6 months, age greater than 70 years and more than one comorbidity such as diabetes and renal failure, had a positive outcome (100%). 8
Health care professional involved in study and study outcome
Different types of health care professionals were involved in the studies including nurses, internists, cardiologists, case managers, and clinical psychologists. In 26 studies (77%), the nurses were the primary health care professionals in charge of monitoring the data from the patient and informing the physicians of abnormal values. Additionally, the nurses were also responsible for calling the patient to follow up on abnormal values and advising them on the next steps. Physicians were the lead in six studies (18%), where the physicians reviewed the data and contacted the patient if values were abnormal with instructions on the next steps. One of the studies was led by a case manager and another by a non-clinician. In total, 39% of the studies led by nurses, 50% of the studies led by physicians and 0% of the studies led by case manager or non-clinician had a positive outcome. However, there was no statistically significant relationship between the type of health professional leading the study and the outcome of the study (p = 0.45) (Table 2).
Frequency of measuring and transmitting patient data and study outcome
All the studies involved patients self-measuring their vital signs and transmitting the numbers to a health care professional who reviewed the data and contacted the patient if necessary. Most studies required patients to measure and transmit their weight, blood pressure, and heart rate. Most studies also required patients to answer simple symptom questions such as whether they were having shortness of breath, swelling of the legs, etc. Some studies included measuring and transmitting peripheral oxygen levels and heart rhythms from single-lead electrocardiogram. Most studies (91%) required patients to measure and transmit their vital signs at least once daily, while 9% required weekly measurement of vital signs and transmission of vital signs. There was no association between the frequency of data measurement and transmission and the study outcomes (p = 0.85) (Table 2).
Patient–health care provider interactions and study outcome
In addition to measuring and transmitting vital signs, some of the studies included scheduled nurse-led patient education or interaction as part of the intervention. The scheduled patient–nurse interactions included patient self-care education, monitoring disease signs and symptoms, adjusting medications using designated protocols, monitoring medication adherence, counseling in the event of an acute change in health status and addressing technical and social issues.6,7,12
Three studies had scheduled patient–nurse interaction in both the telemonitoring and control group, while nine studies had the interaction in only the telemonitoring group. Of the nine studies that had scheduled patient–nurse interaction in only the telemonitoring group, 44% had a positive outcome (reduction in number of hospitalization and/or decrease in mortality). The scheduled interactions were either weekly, biweekly, or monthly and there was no difference in outcome in the studies that included scheduled nurse-led patient education or interactions and those that did not (p = 0.65).
Discussion
Our review of 34 randomized controlled trials of heart failure telemonitoring did not show any significant influence of study design on hospitalization and/or decrease in mortality in heart failure patients. Studies that were done outside North America (USA and Canada) and studies that selected patients at high risk of re-hospitalization were more likely to have a positive outcome, though this was not statistically significant.
The studies that were done in Europe were more likely to reduce heart failure hospitalization and/or mortality than those in North America. While only 25% of the studies done in North America had a positive outcome (reduction in the number of hospitalization and/or decrease in mortality), 50% of the studies done in other countries (mainly European countries) had a positive outcome, although the difference in outcome was not statistically different (p = 0.09) after adjusting for other covariables. The reason for the difference between studies in Europe and North America is unclear. The study design including the study population, the health care provider leading the study (nurse vs. physician), the frequency of patients measuring and transmitting vital signs, patient–health care provider interactions and the types of patients recruited in the studies (elderly vs. recently hospitalized) were similar in both the European and North American studies. The major difference between the studies in Europe and those in North America was the duration of the study (how long the patients were monitored). The studies in Europe had a mean and mode duration of 12 months respectively, compared to a mean of 7 months and mode of 6 months in North America. However, our analysis did not show any statistically significant relationship between study duration and study outcomes.
Our study did not show any difference in outcomes in studies that recruited only elderly or recently discharged patients and those that did not. We had expected that home telemonitoring might have more beneficial effects in studies that recruited patients with more advanced disease, or patients at high risk of hospital readmission but unfortunately, we only had one study that specifically recruited heart failure patients at high risk of relapse. However, the single study that specifically recruited heart failure patients at high risk of hospital readmission on discharge, which included New York Heart Association class III/IV patients with at least two of the following: greater than two heart failure in the last six months, age greater than 70 years and more than one comorbidity such as diabetes and renal failure had a reduction in mortality and hospital readmission. The ability to detect early signs of clinical decline and perform an intervention early might have been helpful in this group of patients at high risk of hospital readmission. There is a need for more research on the effect of telemonitoring on patients that are at high risk of hospital readmission.
The type of health care professionals involved in the studies, the frequency of measuring and transmitting patients’ vital signs and incorporating scheduled patient–health care provider interaction as part of the intervention did not influence the outcome of the studies. We had anticipated that patients that had home telemonitoring with scheduled weekly, biweekly, or monthly patient–nurse interaction and education as part of the intervention would fare better than those in the usual care group, however, this was not so. This could signify that patient education at hospital discharge and education during regular outpatient follow up clinic visits are sufficient for many heart failure patients.
There are limitations to this study. First, all the randomized controlled studies included in the study were from high-income countries and the results of this study may not be applicable to low- and middle-income countries. In addition, our ability to perform sub-group analysis was limited because of the number of studies included in this review.
In conclusion, our study, focused on examining the influence of study designs on study outcomes, did not show a significant influence of study design on reduction of hospitalization and/or mortality. However, there is need for more studies to understand why telemonitoring studies in Europe were more likely to reduce hospital admission and mortality compared to those in North America. There is also need for more evaluation of the effect of telemonitoring on patients at high risk of hospital readmission.
Footnotes
Author contribution
CAU and MR extracted the data. CAU analyzed and interpreted the data with input from all other authors. CAU and MR wrote the first draft of the paper. AD, MY, SC, and SS reviewed and substantially revised the paper. All authors have read and approved the final version of the article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.