
Abstract
Introduction
A piezoelectric sensor (PS) converts mechanical deformations into electrical signals. We used a contactless under-the-mattress PS to monitor physiological vibrations resulting from breathing, pumping of the heart, and body movements, among individuals at home following hospitalization for heart failure (HF). Our objectives were to assess acceptability of the device in the home, to assess physiological patterns, and to determine if altered patterns correlate with readmission.
Methods
We conducted a prospective observational study of 30 patients discharged home following HF hospitalization. PS data included a continuous nightly assessment of heart rate, respiration rate, movement rate, rapid and shallow respiration duration, and a behaviour score. We utilized random forest classification to classify average nightly data by readmission status.
Results
We collected 640 nights of PS data from 29 patients. There were nine readmissions, of which four were for HF. PS monitoring was tolerated by all but one of the participants. We inspected continuous nightly physiological profiles and noted differences between patients who were and were not readmitted. Patients readmitted for HF had higher average heart and respiration rates, and more respiration variability. Average nightly respiratory rate was most predictive of readmission.
Discussion
We are the first to study nocturnal physiological patterns of HF patients at home using a contactless under-the-mattress monitoring system. We noted patterns that may be unique to patients at risk for readmission due to HF. Respiratory rate was the most important risk-adjusted associate of readmission for HF. Further studies should investigate the efficacy of home PS monitoring in HF populations.
Introduction
Home monitoring of physiological parameters in patients with heart failure (HF) may lead to early identification of decompensation, therefore potentially allowing for intervention before a hospital readmission occurs. Regardless, non-invasive monitoring of routine daily vital signs (weight, heart rate, blood pressure) has shown a limited ability to detect early deterioration of HF in clinical studies.1–3 It is unknown if more frequent monitoring of vital signs, or monitoring of novel physiological parameters, may improve early identification of decompensation.
A piezoelectric sensor (PS) converts pressure into electrical signals. EverOn (EarlySense, Ramat Gan, Israel) is a novel PS that can detect subtle physiological vibrations resulting from breathing, pumping of the heart, and generalized body movements, across consumer-grade bed mattresses. 4 Mathematical algorithms convert these signals in a continuous manner to meaningful metrics including heart rate, respiratory rate and movement rate. Additionally, the technology is able to report on breathing patterns, such as rapid and shallow breathing, and on behavioural patterns, such as amount of time spent in bed. This sensor technology has been validated in hospitalized adults, but has not been studied in patients in their home environment. 5
The EverOn device has multiple potential telemedicine capabilities. It is able to send signal data to a central monitoring station via local area network (LAN) or Wi-Fi (www.earlysense.com) in a hospital environment. 6 A newer model of the same device (www.myearlysense.com), which was released after the current study ended, has the ability to send information wirelessly to a smartphone app in a home environment.
We utilized this under-the-mattress PS to monitor adults who were discharged home after hospitalization for HF. Our primary objectives were to assess normal and altered physiological patterns in the home environment, and to determine if altered physiological patterns correlate with hospital readmissions.
Methods
Study design
We performed a prospective observational study of patients who were discharged to home following hospitalization for HF. The study was approved by Cleveland Clinic's Institutional Review Board. Patients were enrolled prior to hospital discharge. Patients were eligible if they were over the age of 18, had symptomatic HF as the admitting diagnosis as documented by a staff cardiologist, lived in Northeast Ohio, and slept on a mattress at home. Patients with systolic left ventricular dysfunction as well as those with preserved ejection fraction were included. Exclusion criteria included planned readmission or plans to travel out of Northeast Ohio within 30 days of discharge. Patients who shared a mattress with another person or pet were excluded from the study. We obtained written informed consent from all patients prior to study enrolment.
EverOn consists of a sensor and control unit, connected by a shielded cable (Figure 1). The sensor is 300mm long, 210mm wide, and has a thickness of 6.45mm. The sensor produces an electrical signal in response to physiological stimulation. The system records information continuously when a person's chest lies on a mattress above, or within approximately 40cm of, its edges. The system initiates recording when physiological signals are noted, usually within <1 minute after a person lies down, and it stops recording immediately after a signal is lost. EverOn has been validated on a variety of mattress types including spring, foam, memory foam, and sleep number mattresses. It has not been validated on water or air mattresses. The sensor is effective with mattresses ranging in thickness from 5cm to 40cm and calibrates automatically.
Piezoelectric sensor and placement.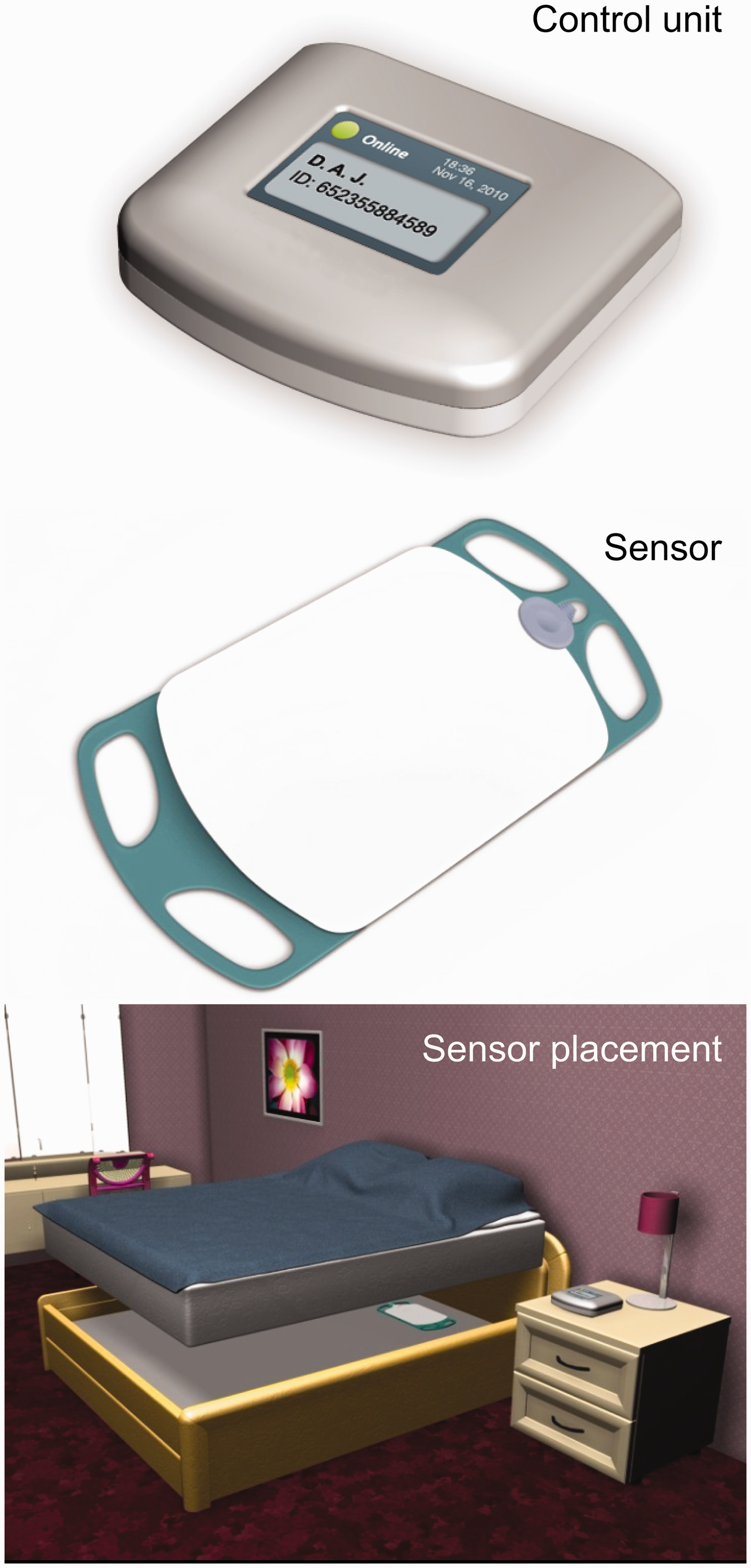
In our study a technician visited the patient at home within 48 hours of hospital discharge and installed the sensor under the patient's mattress. The control unit was secured in a metal box next to the bed. The technician subsequently visited once a week to confirm that the device was functioning and was tolerated by the patient. The technician also downloaded physiological data from the control unit to a secure database. Weights and standard vital signs were collected daily at home as part of routine clinical care throughout the study period. Patients were monitored for a period of 30 to 40 days or until they were readmitted. Adverse events were collected.
Outcomes
The primary outcome was hospital readmission within 30 days of hospital discharge. Aetiology of readmission was determined by review of medical records.
Data analysis
Data were analysed in a case-control manner, whereby cases were patients who were readmitted and controls were patients who were not readmitted. Data are expressed as mean and standard deviation (SD). Categorical data are reported as frequency and percent. Differences in mean values were compared by a Student's t-test or a nonparametric method as appropriate. Data from the PS system included heart rate, respiration rate, and movement rate. Additional parameters included rapid and shallow respiration duration based on the raw signal patterns of respiration, and a behaviour score derived from bed occupancy patterns and movement while in bed. We inspected data trends among patients who were and were not readmitted, and visually identified device data patterns of interest. These patterns later informed our statistical modelling.
We utilized random forest classification (RF-C) methodology to classify data into three categories: readmission for HF exacerbation; readmission for causes other than HF; and no readmission by study end. In order to maximize our ability to detect associations between device data and readmission outcomes we analysed each patient night as an individual unit. There were 640 nights of interpretable data available for analysis. Candidate predictor variables included device output (average nightly heart rate, respiratory rate, and movement rate; standard deviation of nightly heart rate, respiratory rate, and movement rate; hours with rapid and shallow breathing; and behaviour score), as well as age, sex, race, body mass index (BMI), change in daily weight, heart rate (measured once daily), systolic and diastolic blood pressures (measured once daily), oxygen saturation (measured once daily), medication use (ACE inhibitor, beta blocker, angiotensin receptor blocker, aldosterone blocker, digoxin, nitrate, hydralazine, inotrope, calcium channel blocker, diuretic), and day number since study entry.
RF-C is a machine learning algorithmic methodology whereby a multitude of uncorrelated classification trees are constructed by computer software, and then used in concert to assess prediction. This statistical methodology has been described in detail elsewhere,7–10 and has been used in contemporary cardiovascular literature.10,11 In the current analysis our RF-C framework included 1000 individually grown trees. We utilized this framework to identify which variables were most important in classification (a variable importance measurement quantifying change in prediction error). Analyses were performed with R version 3.0.2 (www.R-project.org). RF-C was implemented using Ishwaran and Kogalur's random forest Survival, Regression and Classification (SRC) library at default settings. 12
Results
Demographic and baseline clinical characteristics.
HF: heart failure; BMI: body mass index; EF: ejection fraction; HFpEF: heart failure with preserved ejection fraction; NYHA: New York Heart Association class; ICD: internal cardioverter defibrillator; CRT-D: cardiac resynchronization therapy defibrillator; ARB: angiotensin II receptor blocker.
There were a total of 107 patient home visits by the study technician. Based on patient feedback, overall tolerance of the home monitoring experience was 97%. A single patient complained of disrupted sleep related to perceived intolerance of the monitoring device. Four patients were readmitted for HF within 30 days. Five patients were readmitted for reasons other than HF. A total of 20 patients were not readmitted during the study period.
Figure 2 shows representative PS data collected from two patients. Subject A was an elderly woman with chronic diastolic HF who had a normal heart rate that decreased in a reproducible U-shaped pattern during sleep. Subject B was a middle aged woman with advanced chronic systolic HF. Subject B had higher and more variable respiratory and movement rates as well as persistent tachycardia that did not decrease during sleep. Subject B was readmitted due to recurrent HF within nine days of index discharge.
48 hours of piezoelectric sensor data for two patients.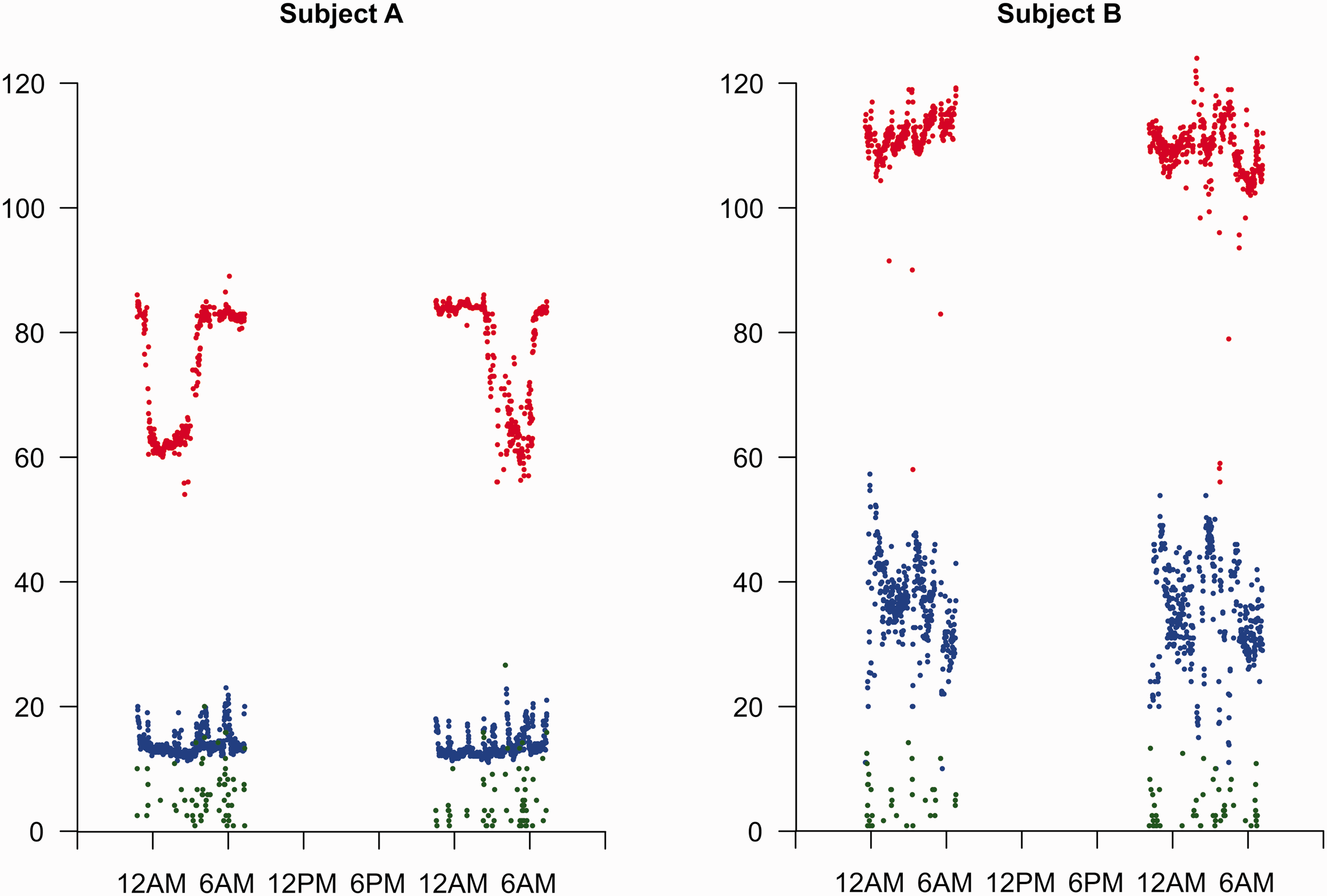
Figure 3 shows the heart rate, respiration rate, and movement across the entire study period for each patient for the same two patients shown in Figure 2. Also shown are trends of hours with rapid and shallow breathing and behaviour score. Subject A had very few hours of rapid and shallow breathing, as well as a low behaviour score across the study period. In contrast, Subject B had many more hours of rapid and shallow breathing, as well as a behaviour score that was not only more variable than Subject A, but also trended upwards during the study period.
Piezoelectric sensor data for the entire study period for two patients.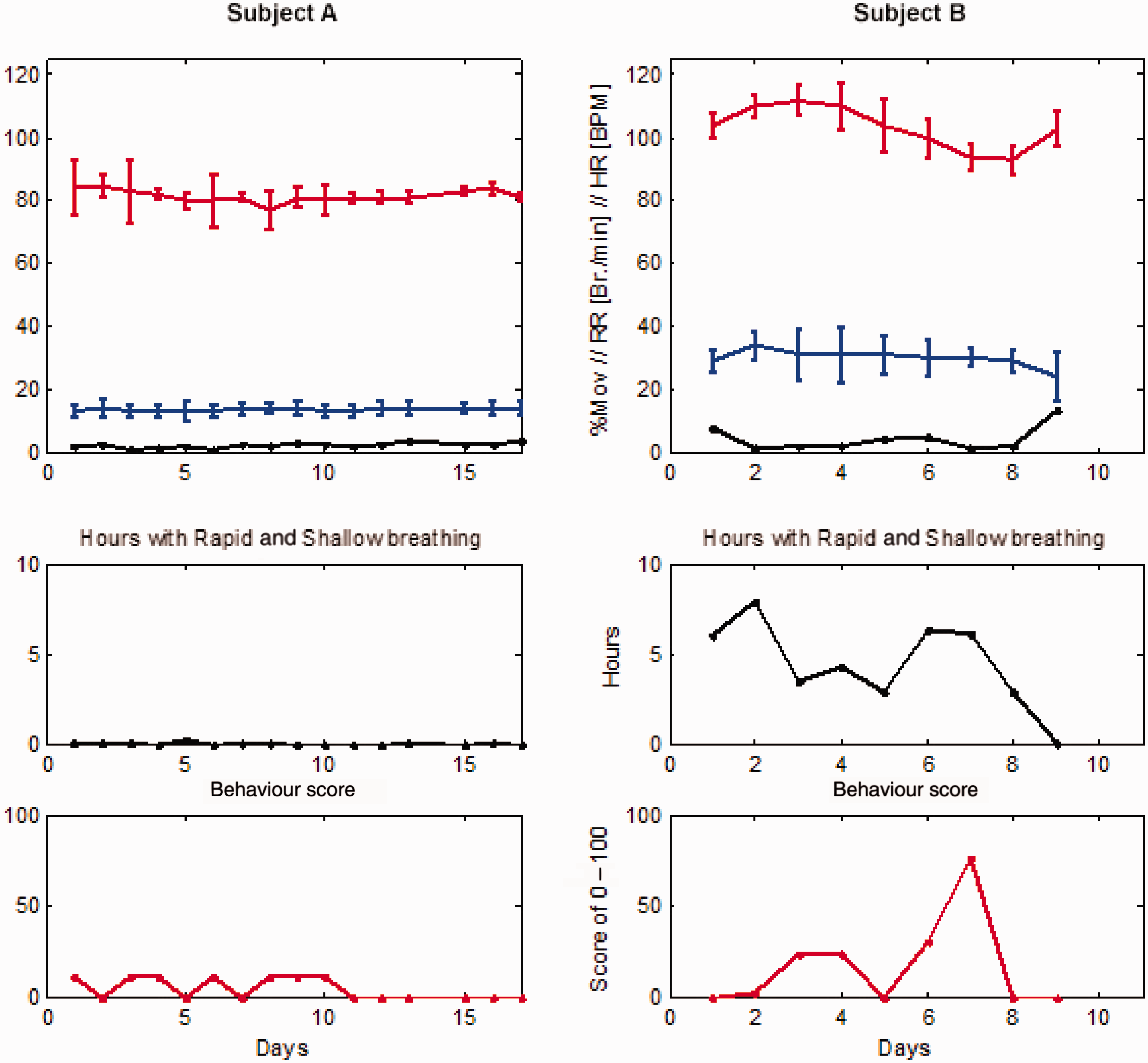
Physiological parameters.
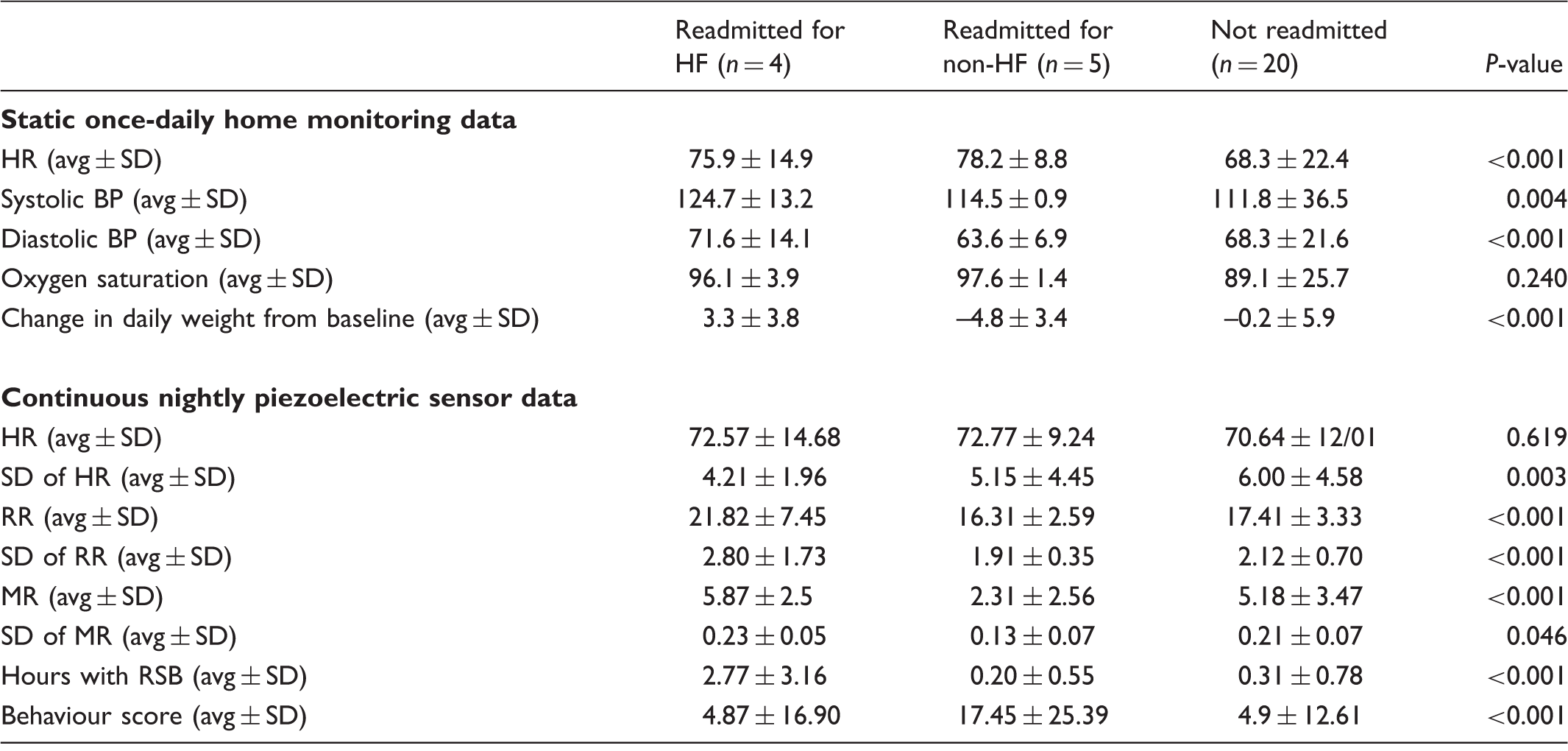
HF: heart failure; SD: standard deviation; HR: heart rate; RR: respiratory rate; MR: movement rate; RSB: rapid shallow breathing
Table 2 also summarizes PS data during the study period. There was no significant difference in the nightly heart rate between patients regardless of readmission status. Patients readmitted for HF had a higher average nightly respiration rate, compared to those readmitted for reasons other than failure, and those not readmitted (21.8 versus 16.3 and 17.4). Patients readmitted for HF also had more nightly variability in respiration rate (2.8 versus 1.9 and 2.1), and a higher nightly average movement rate (5.9 versus 2.3 and 5.2). Patients readmitted for HF had more hours of rapid and shallow respiration, compared to those readmitted for reasons other than HF and those who were not readmitted (2.77 vs 0.20 and 0.31 hours, respectively). Patients readmitted for reasons other than HF had a higher nightly behaviour score compared to those readmitted for HF or those not readmitted (17.45 versus 4.9).
In an exploratory multivariable RF-C framework where each patient night was analysed as an individual unit we found that variables predictive of readmission outcome differed by type of readmission (Figure 4). Among nights of study patients who were readmitted due to HF, average respiratory rate collected by PS was the most important risk-adjusted contributor to prediction.
Variable importance for heart failure (HF) and non-HF readmissions.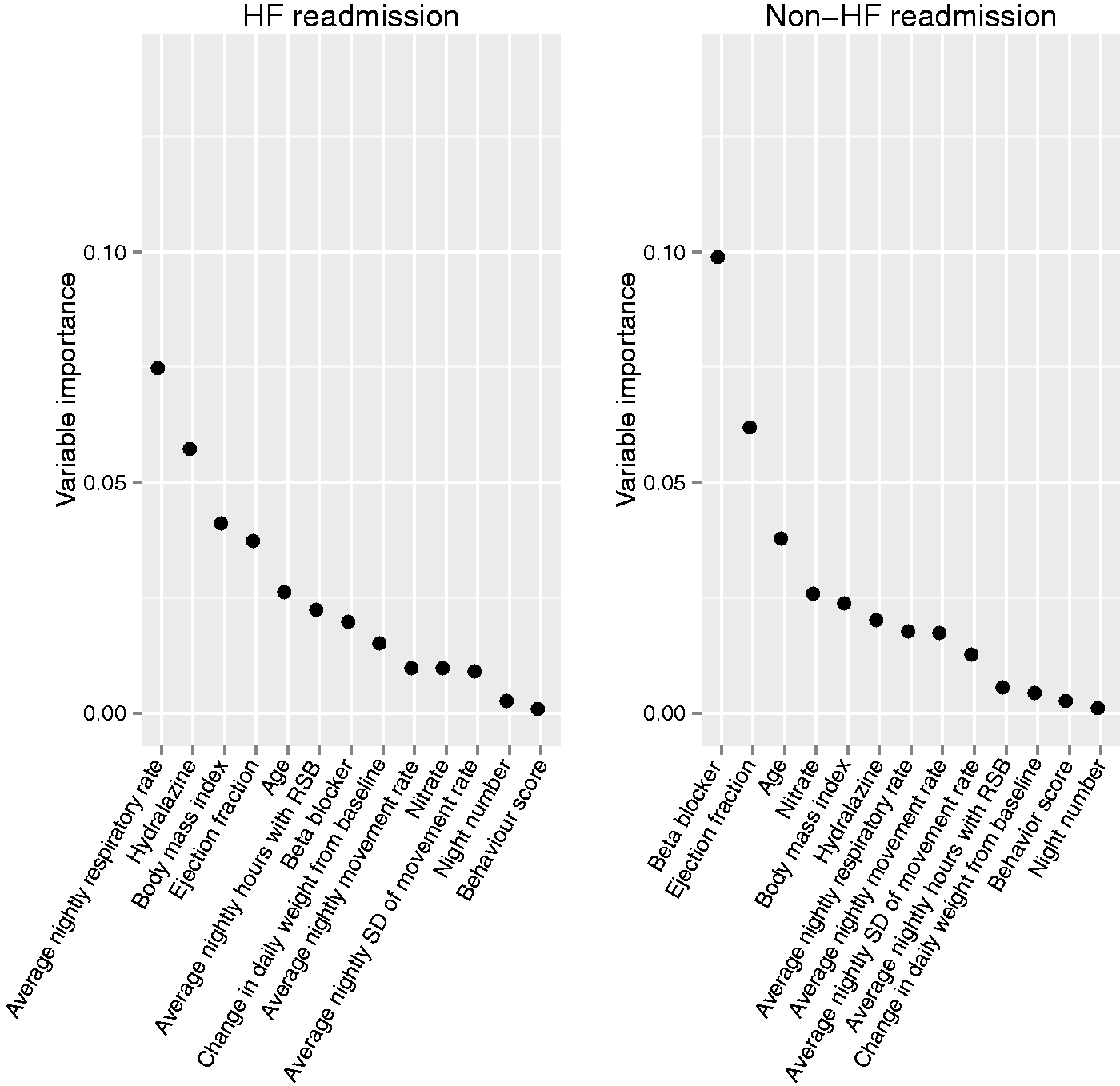
Discussion
To the best of our knowledge, we are the first to study recumbent nocturnal physiological patterns of older adults who were discharged to home after hospitalization for HF, using an entirely non-invasive and contactless monitoring system that requires minimal patient compliance. We found that the PS was well tolerated and reliably provided physiological data for up to 30 days in a patient population that is at high risk for readmission after hospitalization for HF. We found that it may be possible to distinguish between readmitted patients and non-readmitted patients by inspection of individual nightly a patterns and trends over time for a given individual. In our study population, we observed significant differences in respiration rate, movement rate, and behaviour score for patients readmitted for HF compared to patients not readmitted, or readmitted for reasons other than HF. Additionally, in an exploratory analysis using patient nights as individual analysis units, we found that the average nightly respiratory rate collected by PS was the variable most predictive of readmission.
PS monitoring has been previously utilized to accurately measure the respiratory and heart rates of patients in a sleep lab setting, as well as patients hospitalized in the intensive care unit. 4 Brown and colleagues used PS monitoring on a medical-surgical unit to decrease overall length of stay, decrease the number of days in the intensive care unit, and reduce adverse events for hospitalized patients.13 PS parameters have also been tested as risk assessment tools for the development of pressure ulcers, and for early recognition of acutely deteriorating patients in non-intensive care units.14,15
We report the first use of PS monitoring in the home setting for HF patients. HF has a prevalence of over 6 million in the United States, and is associated with a high rate of hospitalizations, as well as substantial morbidity, mortality, and healthcare costs.16–18 These facts underscore the need for effective home monitoring strategies in order to prevent hospitalizations in patients with chronic HF. Studies of various other monitoring approaches have found variable success.2,19,20 Use of home-based PS monitoring may detect early decompensation of disease non-invasively, and provide an opportunity for intervention prior to hospitalization. Our findings suggest that further study in larger clinical trials is warranted. The EverOn (EarlySense, Ramat Gan, Israel) PS monitoring device used in our study has the capability to transmit signals wirelessly to a smartphone app. As such, this monitoring technology may emerge as a component of a novel home telehealth strategy for this population of patients, if found effective in further investigations.
There are several limitations to our study. We performed a non-randomized, observational study with a small sample size and short follow up period. We assessed PS monitoring at one medical centre only. The small number of patients meeting readmission endpoints limited statistical analysis. Our study was not designed to test the efficacy of PS monitoring on readmission outcomes.
In conclusion, we found that patients tolerated an under-the-mattress PS monitor placed in their home. We were able to collect physiological data and identify changes in physiological patterns that may be unique to patients at risk for hospital readmission due to HF. In an exploratory analysis using patient nights as individual analysis units, respiratory rate was the most important associate of readmission for HF. Further studies should investigate the efficacy of continuous nocturnal PS monitoring in home-based HF populations. PS monitoring may emerge as a novel telehealth home monitoring technology for this high-risk population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Cleveland Clinic was awarded a research grant from EarlySense to conduct this study. There were no financial relationships between the investigators and the company.