
Abstract
Keywords
Introduction
Singapore Civil Defence Force (SCDF) provides nationwide pre-hospital emergency medical services (EMS) in Singapore. Singapore witnessed about 11,061 1 adult out of hospital cardiac arrests from 2011 to 2016 and despite improvements in the systems and advancement of the resuscitation measures most of the patients do not survive. There are many termination of resuscitation (TOR) guidelines available for usage in out-of-hospital cardiac arrest (OHCA) like BLS (Basic Life Support), ALS (Advanced Life Support), ERC (European Resuscitation Council), Petrie, 2 Verbeek et al 3 and Marsden et al., 4 UN10 rule, 5 and they essentially consist of absence of some key characteristics in the patients like in-field defibrillation, witnessed arrest, bystander CPR or return of spontaneous circulation [ROSC], or asystole despite 10–20 min of ALS. On the other hand, there is a paucity of definitive guidelines and a lack of consensus regarding the optimal duration of cardiopulmonary resuscitation (CPR) and resuscitative efforts in the emergency department for patients with non-traumatic cardiac arrest. The SCDF run EMS instituted a termination of resuscitation protocol in January, 2019.
Study design and patient selection
This is a retrospective, observational study involving randomly selected fifteen (15) patients who suffered either OHCA or a witnessed cardiac arrest soon after arrival in the ED and underwent prolonged resuscitation. We used Microsoft© Excel 2016 for data entry and analysis. Dichotomous variables were reported as Yes and No while continuous variables were presented as medians with interquartile ranges. We defined prolonged resuscitation as more than 30 min of resuscitation efforts after commencement of first CPR, either by a bystander, paramedics or in the ED. We defined a sustained ROSC 6 as a palpable carotid pulse for more than 30 s as analysed by the physician-in charge with a measurable blood pressure irrespective of vasopressor or inotropic support with the patient not having another cardiac arrest in the next 20 min. We analysed various pre-hospital characteristics and durations related to the cardiac arrest and interventions in the field by SCDF. Other patient related factors were analysed too. The ED resuscitation events and interventions were analysed as well. Prolonged downtime was defined as cases where the duration between arrest and first CPR or arrival of EMS was more than 15 min. 7 Selected inpatient interventions and patients’ progression data were recorded and analysed too. A central institutional review board (CIRB) approval was applied for, which deemed that a CIRB review was not required for this study.
Results
Pre-hospital, ED and In-patient interventions and measures: sustained ROSC and nil ROSC.

aIncludes one OHCA patient, who had witnessed arrest by SCDF en-route to hospital.
b1 OHCA patient who received defibrillation shocks during resuscitation was not administered Amiodarone post-ROSC.
c4 patients were consulted for E-CPR, but none eventually received E-CPR.
d1 of three patients did not have any pre-existing CKD prior to the cardiac arrest event.
e5 patients did not have any brain imaging done, 1 patient had no HIE on CT Brain but had HIE on MRI Brain subsequently, 3 had nil HIE on the CT Brain and 1 had ICH.
Pre-hospital, ED and in-patient interventions and measures: survivors and non-survivors.
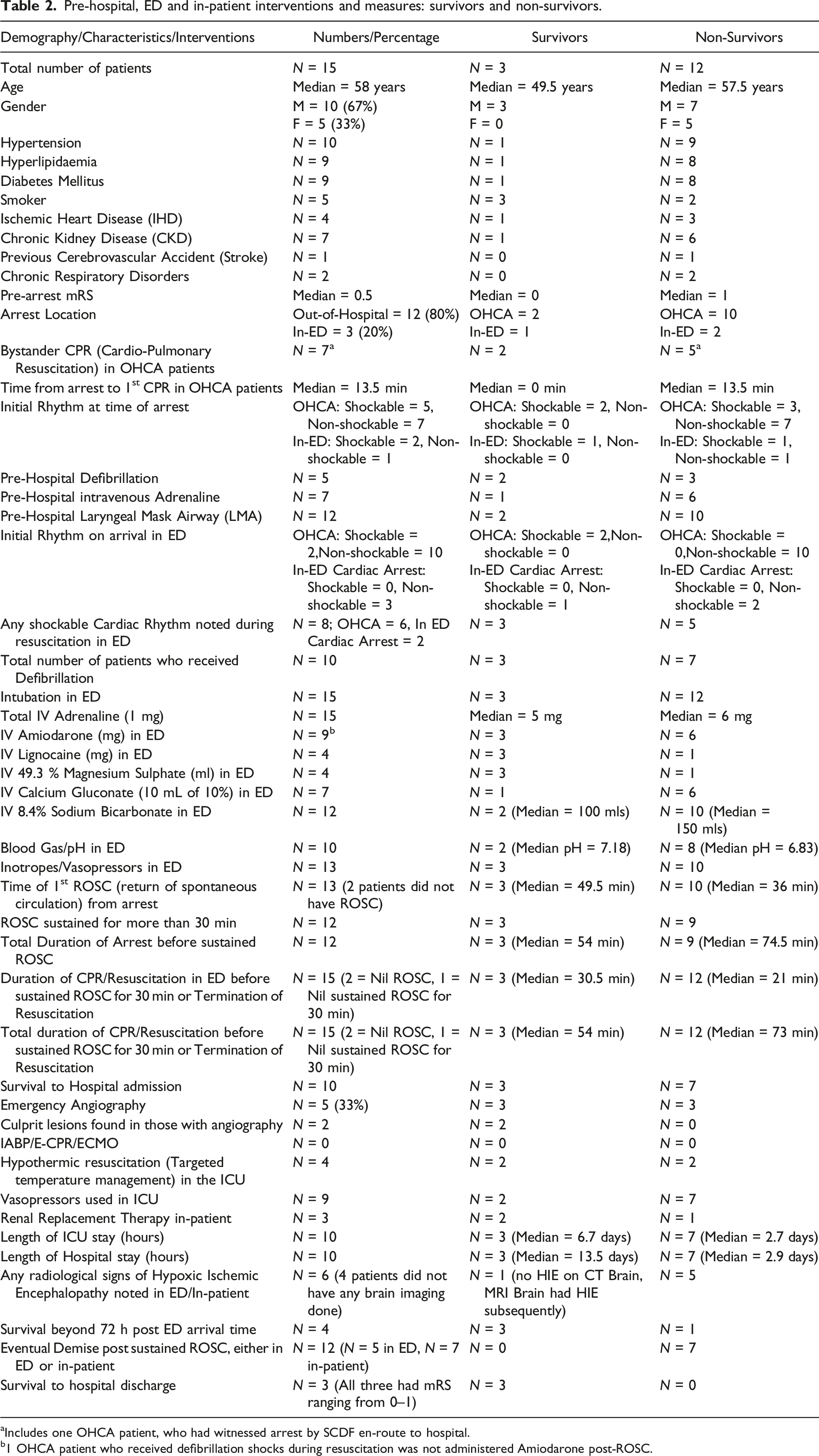
aIncludes one OHCA patient, who had witnessed arrest by SCDF en-route to hospital.
b1 OHCA patient who received defibrillation shocks during resuscitation was not administered Amiodarone post-ROSC.
Ten patients had hypertension, nine patients had diabetes mellitus (DM), nine patients had hyperlipidaemia (HPL), 7 patients had existing chronic kidney disease (CKD), six patients were known smokers, 4 patients had previous ischemic heart disease (IHD), 2 patients had previous chronic respiratory illness like Asthma, COPD, and Bronchiectasis and 1 patient had previous cerebrovascular accident (CVA). All patients had pre-arrest mRS of 0–2, except one whose mRS was 4 pre -arrest. Higher proportion of patients in the sustained ROSC group had pre-existing major co-morbidities of smoking, hypertension, Hyperlipidaemia, Diabetes Mellitus (DM), Ischemic Heart Disease, and Chronic Kidney Disease. All the survivors were smokers while higher proportion of the non-survivors’ group had prevalence of other co-morbidities like hypertension, DM, HPL, CKD, and others.
Three patients had cardiac arrest after arrival in ED, where CPR was started immediately, while the remaining 12 patients has out-of-hospital cardiac arrest and 5 out them did not receive any bystander CPR. A total of 10 out of the 15 patients had shockable rhythms either initially or during the resuscitation process out of which 7 had an initial shockable rhythm and in the remaining 3, the initial rhythm was either systole or PEA.
Amongst the 15 patients, 13 (87%) achieved ROSC, out of which 12 (80%) had sustained ROSC for equal to or more than 30 min, 67% survived to hospital admission, and eventually 3 (20%) survived to hospital discharge, and all three survivors had mRS 0–1 at hospital discharge. Median total CPR duration (until either sustained ROSC or TOR, including by-stander CPR, SCDF CPR and ED CPR) for all the 15 patients was 46 min (IQR: 40–62.5 min), 44 min (IQR: 39.75–61.25 min) for those with sustained ROSC, 48.5 min (IQR: 45–56.5 min) for those without sustained or no ROSC and 54 min (IQR:52.5–66.5 min) for those surviving to hospital discharge and 45.5 min (IQR:39.75–54.75 min) for those who demised with or without ROSC. Median overall CPR duration in ED was 40 min (IQR: 38.5–42.5 min), 45.5 min (IQR: 12.75–68.25 min) for those with sustained ROSC, 28.5 min (IQR: 26–34.5 min) for those without sustained or no ROSC and 30.5 min (IQR: 21.5–31 min) for those surviving to hospital discharge. The longest observed total duration of CPR was 115 min in any subject, while the shortest total CPR duration was for 31 min. The longest duration of resuscitation among survivors was on a 52 year-old-man who had ROSC at 68 min and he was discharged with a favourable neurological outcome. In the sub-group of those with non-shockable rhythms (n = 5), all the patients had sustained ROSC while amongst those with shockable rhythms (n = 10), 70% patients had sustained ROSC. None of the patients, who experienced an out of hospital cardiac arrest had ROSC prior to arrival in the ED. The median time from arrest to initiation of 1st CPR effort was 13.5 min for all the patients while it was started immediately without any time loss in the three patients who survived to hospital discharge. Two of these three patients had OHCA while one of them arrested after arrival in the ED. Ten out of 12 patients with sustained ROSC survived to hospital admission and 4 of these 10 survived well beyond 5 days after ED arrival time. Eventually, three survived to hospital discharge and all three of them had good neurological status upon discharge (mRS: 0–1).
Five patient underwent emergency coronary angiography post ROSC but only 2 of them had an identifiable culprit coronary artery lesion. All patients in the sustained ROSC group required vasopressors and inotropes while one amongst the non-stained ROSC group was initiated on it. Eighty percent of the patients were administered intravenous sodium bicarbonate, out of which 10 were from the sustained ROSC group while 2 were from the non-sustained ROSC group.
The cause of death was determined to be Ischemic Heart disease in 1, Pulmonary embolism in 2, Valvular heart disease in 1, Pneumonia with concurrent acute myocardial infarction (AMI) in 1, AMI and diabetic keto-acidosis in 1, bleeding gastrointestinal tract in 1 and intracranial haemorrhage in 1 patient while in the remaining no cause of death could be ascertained immediately.
Discussion
The appropriate duration of resuscitation in cardiac arrest patients is usually a balancing act between clinical and ethical considerations. The core issue behind considering a prolonged duration of resuscitation is physician prognostication which is based on many factors including but not limited to age, initial rhythm, any by-stander CPR, pre-arrest co-morbidities and ADL (activities of daily living) status. There may also be some concerns about the stewardship of scarce emergency department resources, manpower, and specialised support services like angiography, extra corporeal life support (ECLS), intensive care unit, etc. However a cut-off duration beyond which resuscitation is likely to lead to unfavourable outcome is not yet determined and it may unlikely exist. Some guidelines advocate ≥20 min of resuscitation8,9 whereas others require structured assessment after three cycles of CPR and rhythm analysis (about 6 min). Many a times clinicians may arbitrarily use resuscitation duration in the absence of ROSC to justify TOR. We found in our study that the all three survivors with good neurological outcomes had longer time-to-ROSC (median 49.5 vs 36 min in non-survivors) in contrast to the study by Grunau et al. 10 Reynolds et al showed that longer CPR duration in selective subjects may be independently associated with favourable functional status, 11 and 90% of subjects with good functional outcome had ROSC within 20 min, and 99% within 37 min. On the other hand, Yoshikazu et al. 12 have demonstrated that CPR duration was independently and inversely associated with a favourable 1-month neurological outcomes. In this study, the critical prehospital CPR duration for OHCA was 35 min in patients with initial shockable rhythms and pulseless electrical activity, and 42 min in those with initial asystole. Welbourn et al. 13 have also mentioned in their study that that there is generally a better neurological outcome with a shorter duration of CPR in survivors of cardiac arrest. Prolonged resuscitation efforts when applied for subjects with an initial shockable cardiac rhythm, witnessed and public location of the cardiac arrest, and bystander CPR and defibrillation, the likelihood of survival with a favourable outcome of mRS 0–3 increases, 11 but decreases significantly with increased EMS response time and patient’s age. In a study examining in-hospital cardiac arrests, Goldberger, et al. 14 reported longer attempts at resuscitation associated with higher rates of ROSC and survival to discharge, which was independent of the measured patient characteristics. Four variables 15 are independently associated with prolonged CPR attempts: younger age, pre-existing heart disease, occurrence of transient return of spontaneous circulation, and access to the ED.
Weiser et al 16 showed that, patients with PEA with initial electrical frequency >60/min were associated with 30- days-survival rate of 22% and a good neurological outcome. In general, non-shockable rhythms such as pulseless electrical activity (PEA) and asystole are thought to have a low chance for survival (overall 0.5–2.5%) compared to shockable arrest rhythms with up to 30% survival. 16 Minimum co-morbidities and initial shockable rhythms are some of the most powerful independent predictors of good survival outcomes10,17 after a cardiac arrest event and in our study patients with initial shockable rhythms at the time of arrest demonstrated better survival outcomes.
Eighty percent of our study patients were administered intravenous 8.4% Sodium Bicarbonate (median dose of 150 mls) during resuscitation. AHA 2020 ACLS guidelines 18 does not recommend routine use of sodium bicarbonate in cardiac arrest and the evidence for use of Sodium Bicarbonate in prolonged resuscitation efforts is not very compelling and it may not necessarily lead to ROSC or good neurological status 19 post ROSC. Vukmir et al. 20 in their study in 2006, showed that bicarbonate administration was associated with a trend toward improved outcome in prolonged cardiac arrest with approximately hundred percent increase in survival over those who received placebo (32.8% vs 15.4%). In contrast to this, Shin Ahn et al., 19 in their study performed in 2015 involving 50 patients, showed that the use of sodium bicarbonate improved acid-base status, but not the rate of ROSC and did not account for any difference in good neurologic survivals. Mclean et al. 21 in their 2021 study involving 225 patients concluded that sodium bicarbonate in acidotic cardiac arrest patients did not result in increased rate of ROSC compared with those without prearrest acidosis.
In our study lignocaine was used for refractory shockable rhythms after exhausting usage of about 450 mg of Amiodarone. The ARREST 22 and ALIVE 23 trials were the pioneer randomized studies, which provided the strongest evidence in favour of amiodarone in OHCA due to shockable ventricular arrhythmias. In a study by Huang et al. 24 involving patients with shockable rhythms during cardiac arrest, 1-year survival rates were improved with use of amiodarone and/or lignocaine, as opposed to non-treatment while Mcleod et al. 25 showed that Amiodarone and lignocaine were associated with improved survival to hospital admission, but not necessarily to survival to hospital discharge and neurologically intact survival. Various studies23,26,27 have shown that in Ventricular Tachycardia (VT) and Ventricular Fibrillation (VF) patients, amiodarone improved survival to hospital admission, but there was no significant difference in the rate of survival to hospital discharge when compared to lignocaine. 28 Khan et al. 29 showed that while there were no statistical differences between amiodarone and lidocaine in terms of survival to hospital admission, lidocaine was significantly better than amiodarone in improving survival to hospital discharge. This is a relatively novel conclusion and needs further validation. Outcomes from non-shockable-turned-shockable OHCA is poor but not invariably fatal and although not statistically significant, estimates for survival were greater after amiodarone or lidocaine use than placebo. 30
Magnesium is used most commonly for polymorphic VT and Torsades-de-pointes (TdP) and is thought to be helpful in refractory VF and pulseless VT cardiac arrest patients, due to its role in regulating sodium, potassium and calcium flow across cell membranes,31,32 although studies by Allegra et al. 33 , Srisurapanont et al., 34 and Hassan et al. 35 showed no statistically significant difference in ROSC, survival to hospital admission and hospital discharge with good neurological outcome after the use of intravenous Magnesium Sulphate compared to placebo.
The hypothesis for Calcium usage and administration in a cardiac arrest is that acidosis causes hypocalcaemia, and reversal of hypocalcaemia may lead to a potentially viable cardiac function. Harrison and Amey 36 showed that intravenous Calcium Chloride had a 5.6% successful ROSC rate amongst the 480 pre-hospital cardiac arrest patients with three long term survivors and all the patients with ROSC had electromechanical dissociation (PEA) rhythms. Stueven et al. 37 mentioned that a subset of patients with widened QRS complexes or ischemic changes may benefit from the use of calcium in cardiac arrest. On the other hand, Kette et al. 38 in their systemic review concluded that there is no evidence that the administration of calcium during cardiopulmonary resuscitation improves survival from cardiac arrest irrespective of the presenting rhythm. Vallentin et al. 39 in their OHCA trial concluded that administration of calcium compared with saline did not significantly improve sustained ROSC. Seven patients in our study were administered intravenous calcium gluconate and all of them had OHCA along with a sustained ROSC later on. Four of these patients had non-shockable (PEA or Asystole) rhythms.
Momiyama et al. 40 showed that patients with favourable outcome after OHCA had lower lactate and higher pH levels. Our study survivors had median pH of 7.18 compared to non-survivors with pH of 6.83.
In the modern resuscitation era E-CPR and ECMO is being used increasingly particularly in those with favourable factors for a good outcome. The ARREST 22 trial has demonstrated that early ECMO institution during resuscitation of OHCA patients with refractory VF as compared to the standard ACLS treatment significantly improved survival to hospital discharge. None of the patients in this study received an extra-corporeal CPR (E-CPR) or the incorporation of ECLS into the cardiac arrest.
Deakin et al. 41 in their review did not find double sequential defibrillation (DSD) superior to standard defibrillation and there were no differences in terms of neurological outcome, survival to hospital discharge, survival to hospital admission, ROSC, or termination of VF/pVT. There are also no differences between the defibrillation efficacy 42 by using antero-posterior (AP) or sterno-apical (SA) pads’ placement. None of the patients in our study received (DSD).
Principle of futility
An objective criterion for medical futility or the principle of futility 43 was defined in 1990 for interventions and drug therapy as imparting a <1% chance of survival. In practise, this principle is controversial, and the perfect ‘futility-meter’ in a cardiac arrest scenario does not exist, allowing emergency physicians to practise clinical gestalt in making decisions about the length of resuscitative interventions. 44 Some clinicians have advocated the use of POCUS (point-of-care-ultrasound) findings to decide about TOR. The POCUS findings might indicate a particular diagnosis and encourage the continuation of resuscitation, but absence of diagnostic findings is not sufficient in isolation to exclude a particular diagnosis or cease resuscitation. 45 The evidence to support POCUS during cardiac arrest is at best as a diagnostic and prognostic adjunct.
Limitations
There are essential drawbacks in our study like being observational and descriptive in nature, extremely small sample size with possible bias in sample selection. There are no statistical analysis to demonstrate any association between the interventions and the results and our conclusions. The lack of randomisation and being underpowered, also makes our study conclusions less robust. Regardless, we have attempted to establish a positive association between the longer duration of resuscitation and CPR with outcomes of sustained ROSC, survival to hospital admission and discharge, but the relationship may not necessarily be linear and many other factors and interventions may modify the outcomes.
Conclusion
Each elapsed minute of CPR and resuscitation without a ROSC is independently associated with lower odds of favourable functional outcome at hospital discharge. However, those with universally accepted favourable features 11 (shockable initial cardiac rhythm, witnessed cardiac arrest, bystander CPR, minimum or absence of co-morbidities) are more likely to survive with favourable functional outcome after longer resuscitation periods, and warrant early consideration of advanced therapies such as E-CPR, coronary angiography. Resuscitation duration alone in the absence of ROSC should not be used as an ad-hoc criterion for TOR. Also, the treating clinician may possibly bias against the non-shockable rhythm patients to shorter resuscitation durations due to generally accepted overall poor survival rates. Hence, it is quite possible that the overall outcomes may be improved for both shockable and non-shockable rhythm subgroups by prolonging advanced resuscitation attempts. While our study does show that prolonged duration of resuscitation is associated with higher rates of ROSC and survival with better neurological outcomes, further larger studies with robust methodology may be needed to validate these conclusions.
Supplemental Material
Supplemental Material - Characteristics and outcomes of cardiac arrest patients with prolonged resuscitation
Supplemental Material for Characteristics and outcomes of cardiac arrest patients with prolonged resuscitation by Abhay Kant and Yi-En Clara Seah in Progress in Proceedings of Singapore Healthcare
Footnotes
Author contributions
Dr. Seah Yi-En Clara was partially involved in tabulation of the research data and also contributed in patients’ selection for the research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
All supplementary material for this article are available online.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.