
Abstract
Background
When critical illness survivors are discharged home, they encounter a myriad of physical, emotional, cognitive, and socioeconomic challenges which can endure for an extended period of recovery. Given the extent of patient need, family members often assume the role of informal caregivers. The work inherent in this role can significantly compromise their own health, which can, in turn, influence the nature and trajectory of recovery for the survivor.
Purpose
This study aimed to describe the role of informal family caregivers in patient recovery from critical illness following hospitalisation, in the context of publicly-funded healthcare and where there were no critical care follow-up or aftercare programmes.
Methods
Guided by a qualitative, interpretive description approach, in-depth semi-structured interviews were conducted with 25 family caregivers of patients recovering from critical illness at home. In total, 29 interviews were conducted: 21 caregivers were interviewed once, and 4 caregivers were interviewed twice. Interview data were analyzed thematically using inductive, constant comparative methods.
Results
The nature of family caregiving was grounded in the patient’s condition, whether it involved slow recovery vs stagnation or decline, and the caregiver’s capacity to engage in care. Caregivers influenced patient recovery by (1) assuming daily living and physical care responsibilities; (2) providing motivational and emotional support; (3) searching for and gathering information; (4) monitoring and supervising health and treatment; and (5) managing medical appointments and advocating for resources.
Conclusions
Family caregivers fulfilled a central role in managing a wide range of needs of survivors, found to be pivotal for their recovery. Policy and practical support are needed to help caregivers fulfil this role alongside meeting their own personal challenges and responsibilities.
Introduction
Survivors of critical illness often endure long-lasting impairments across multiple health and wellbeing domains. The term post-intensive care syndrome (PICS) refers to a constellation of new or worsening impairments in physical, emotional, cognitive, and social health that arise after critical illness and persist after hospital discharge.1,2 PICS may persist for months or years following hospital discharge, encumbering daily activities and diminishing health-related quality of life.1,3 The path to recovery post-discharge can be arduous, with survivors often requiring substantial health service support, including medical resources, home care, mental health services, rehabilitation, and long-term care placements. 4 Emergency department visits and unplanned hospital readmissions are high for survivors, with pooled data indicating a 53% (95%CI: 44%–62%) readmission rate within a year of hospital discharge. 5
Family members often become informal caregivers of intensive care unit (ICU) survivors for extended periods of time. Many family members simultaneously suffer symptoms of post-intensive care syndrome-family (PICS-F), a term encompassing adverse psychological repercussions of critical illness, such as anxiety, depression, acute stress disorder, post-traumatic stress, and complicated grief, experienced by family.2,6 Recent research has highlighted further consequences to family health and wellbeing, loss of employment, and lifestyle interference.7–10 PICS-F might also affect the survivor’s recovery 11 and shape the ability to sustain care in the home. For example, fragile social or unpaid caregiver support has been associated with increased hospital readmission following critical illness. 12 Family members of ICU survivors have reported feeling distressed and unprepared by survivors’ unpredictable recovery trajectory, unmet information and support needs, and difficulty navigating fragmented healthcare.13–15 Emotional, practical, and instrumental support have been identified as important in helping families adapt to the caregiver role.15–17 Researchers have found that relationships are integral to self-management as family members make sense of symptoms through their conversations with one another, assist with everyday illness management in the home, and communicate with healthcare providers, interpreting and implementing provider advice. 18
While a growing body of literature describes PICS-F and the experiences of family caregivers during patient recovery,9,10 the role family caregivers play in a patient’s recovery post-ICU is less well-described. Notably, there is a dearth of evidence examining the role of family caregivers in the context of publicly-funded healthcare and where there are no ICU follow-up or aftercare programmes, such as in the Canadian province of British Columbia. We sought to better understand the role of informal family caregivers in patient recovery from critical illness following hospitalisation, within the context of a larger study aimed at developing explanatory models of post-ICU unplanned rehospitalisation.
Methods
Design
The over-arching study aimed at developing explanatory models of post-ICU unplanned rehospitalisation in British Columbia from interviews with patients, family caregivers, and healthcare providers. This paper reports on research conducted as part of this over-arching study on the specific role of family caregivers in patient recovery, using a qualitative, interpretive description methodology, and family caregiver interview data. Interpretive description is an applied approach to generating evidence with respect to questions relevant to clinical practice. 19 The research team included an interdisciplinary group of researchers, clinicians, stakeholders/decision-makers, and patient partners (individuals who were patients or caregivers with lived experience). The University of British Columbia Behavioural Research and Fraser Health Ethics Boards approved the study protocol (H21-01378).
Participants and recruitment
We recruited family caregivers from a closed 46-bed ICU (where patients are admitted and cared for by intensivists) of a large urban hospital serving a population of 900,000. We used purposive sampling for recruitment; point-of-care providers, including physicians, nurses, and social workers, approached patients during their hospital stay to inform them about the study and the potential of interviewing their family caregivers. The research team telephoned or emailed those patients who had agreed to be contacted within 1 month of their discharge from hospital, seeking their permission to invite a family caregiver to the study, and directly contacted family caregivers identified as substitute decision makers when the patient had been deemed unable to provide consent to contact because of cognitive impairment. Of the 37 family caregivers invited to participate, 25 accepted. Three of these were substitute decision makers at the time of consent. After verbal consent was documented by a research team member, an interview was scheduled for a time and date selected by the family caregiver. Eligible caregivers included a relative, unmarried partner, neighbour, or close friend of patients who had received invasive or non-invasive mechanical ventilation for ≥48 h during their primary ICU admission, were ≥19 years of age and spoke English and were not in receipt of other follow-up services. Family caregivers of individuals receiving palliative care at home or who underwent cardiac surgery or an organ transplant were excluded on the assumption that the patients were receiving related follow-up services.
Data collection
Six team members with qualitative interviewing training conducted in-depth semi-structured interviews with 25 family caregivers between April 2022 and September 2023. A total of 29 interviews were conducted; 21 caregivers were interviewed once, and 4 caregivers were interviewed twice. Twenty-six interviews were conducted virtually (via Zoom Video Communications, Inc.), and three interviews were conducted in person. Depending on patient and family caregiver preferences, the interviews were conducted either individually or with the patient and family caregiver together. Interview guides encouraged elaboration on aspects of illness and recovery raised by participants and were developed based on preliminary insights identified during ongoing analyses. 19 That is, as interviews were conducted, interviewers and team members discussed their reflections on the data during weekly meetings, identifying important insights and aspects worthy of further exploration in subsequent interviews. Interviews were audio-recorded, transcribed verbatim via online software (TemiTM), de-identified and checked for accuracy by the research team. Interviewers took field notes following each interview, capturing their overall impressions and emphasizing or noting unique aspects of participants’ experiences.
We focused on gathering interview data high in information power, an approach to determining sample size distinct from data saturation. Information power suggests that the more information the sample holds for the study, the fewer participants are needed. 20 We considered the sample and data high in information power due to the wide variation in participants’ characteristics (e.g., sociodemographic data, patient diagnosis, and the nature of the patient-caregiver relationship) and the diverse experiences they described, as well as the richness of participants’ accounts and the high quality of interview dialogue. Self-reported sociodemographic data were collected via Zoom following the interview or self-report through a Research Electric Data Capture (REDCap) survey link. We extracted medical data from patient charts.
Data analysis
Our analysis involved input from the research team, was guided by interpretive description methodology, and used software for data management (NVivoTM version 12) and diagramming (MiroTM). We inductively developed a coding frame based on the interview transcripts that included several codes related to family caregiver roles and responsibilities. We then conducted an inductive analysis of the family caregiver transcript data related to the family caregiver roles and relationships codes. This involved identifying transcript segments that reflected emergent patterns, diversities, and examples in the data and comparing and contrasting data across family caregiver participants. The data coding process was characterised by inductive, active, and iterative steps rather than being centred on inter-coder reliability. All six team members who conducted semi-structured interviews were involved in data analysis, including data coding, and contributed to weekly team meetings and team reflections on additional insights from recent interviews (which were largely captured in field notes), the adequacy of the coding and coding frame, comparisons of data across participants, and preliminary groupings of data and then thematic patterns. Sociodemographic and medical data were analyzed descriptively to provide a comprehensive profile of the sample. As the analysis progressed, the research team actively participated in open dialogue and discussions, facilitating an interpretive analysis enriched by the varied viewpoints of our patient partners and clinical stakeholders. We report the study findings following the Consolidated Criteria for Reporting Qualitative Research guidelines and checklist. 21
Findings
Family caregiver characteristics.
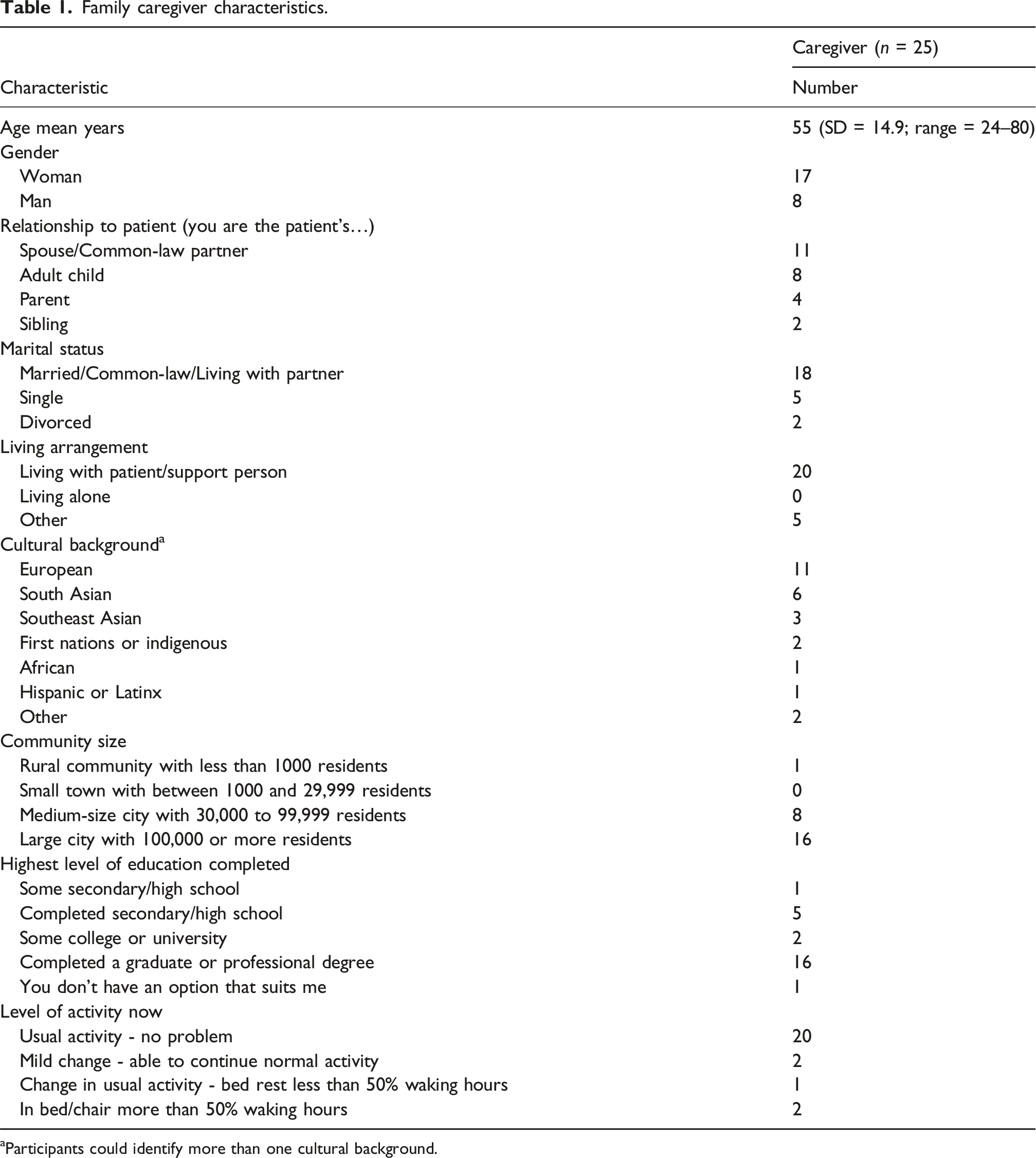
Participants could identify more than one cultural background.
The informal family caregiving role appeared to be contextually grounded in the patient’s condition, whether it involved slow recovery vs stagnation or decline, and the caregiver’s capacity to engage in care. Caregivers influenced patient recovery by (1) assuming daily living and physical care responsibilities; (2) providing motivational and emotional support; (3) searching for and gathering information; (4) monitoring and supervising health and treatment; and (5) managing medical appointments and advocating for resources (see Figure 1). Roles of caregivers in patient recovery.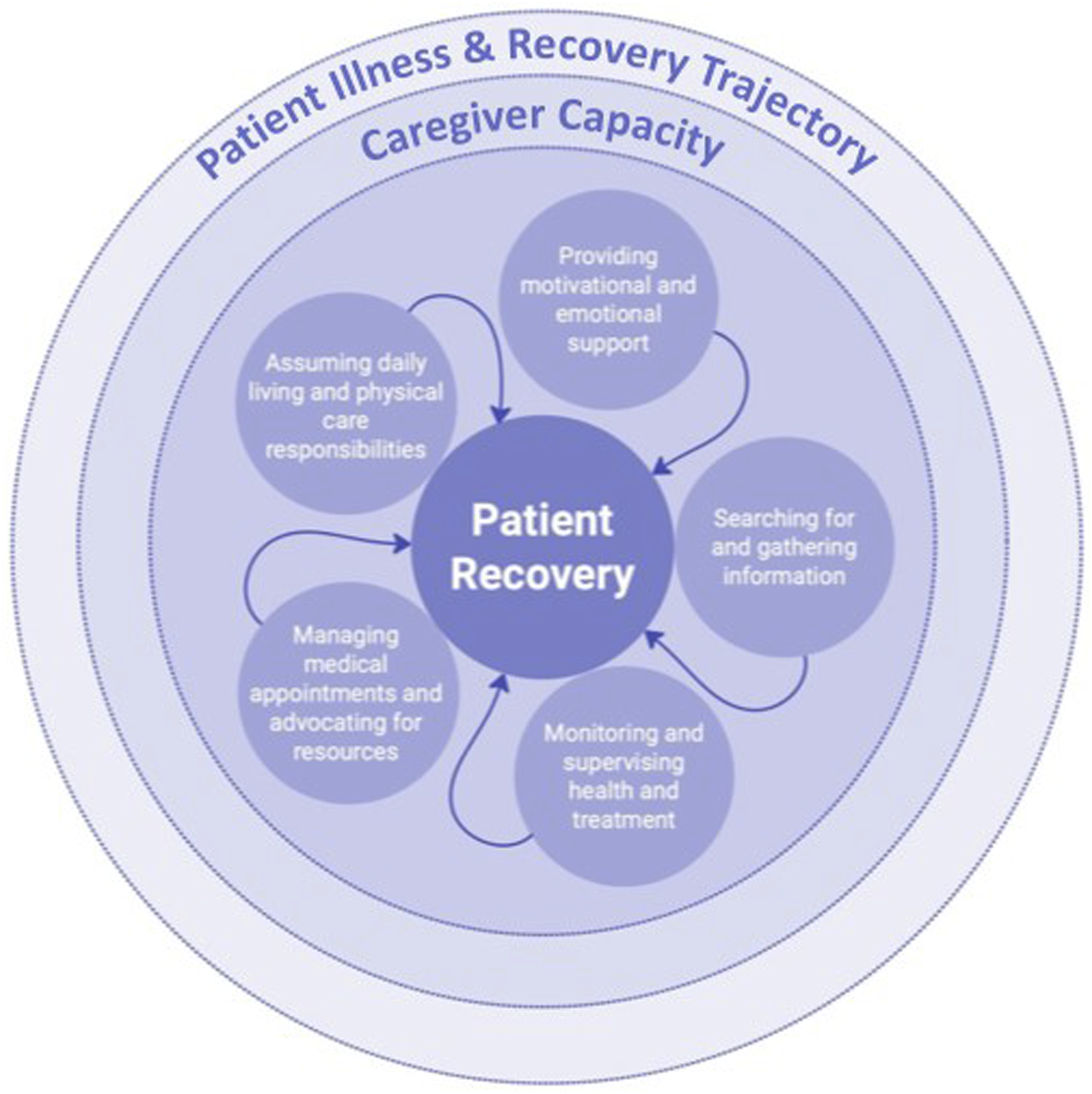
Caregiving in context
Divergent patient trajectories: Slow recovery versus stagnation or decline
There were different patient trajectories, with some slowly recovering at home, while others experienced stagnated or worsening health, necessitating emergency care or hospital readmission. With caregiver support, some patients gradually regained health and functionality, noticing a slow return to their prior daily activities over time. As weeks and months passed, patients progressed from requiring constant care for a wide range of needs including basic hygiene and mobility to needing less assistance. For example, a caregiver described how her husband slowly returned to performing personal tasks without assistance or instruction: “Finally, he started to measure his blood sugar. He got a new glucometer a few months ago and he hasn't used it before. Then, the regular walks. Before, I was nudging him. ‘Okay. Let’s go, let’s go.’ Now, he does it by himself. So, it’s really comforting to see that he’s doing these things for himself, that he doesn’t need anyone else to tell him.” (60-year-old woman caring for her 63-year-old husband admitted to ICU with gastrointestinal bleed)
Despite caregiver support, other patients’ health and functioning plateaued at home, remaining stagnant at the level observed at hospital discharge. Rather than experiencing improvement, these caregivers and patients seemed forced to accept a new normal characterised by ongoing illness and impaired functioning. Additionally, caregivers often found themselves grappling with declines in their loved one’s health during the initial months at home post-discharge, unsure of the causes or how to address setbacks. For some, this led to frequent ambulance calls, emergency department visits, and hospital readmissions. Many caregivers conveyed feeling trapped in a cycle of perpetual emergencies and stuck in a situation demanding constant care and vigilance. As one 69-year-old sibling caregiver expressed: “We escaped death again twice in six months; what can we do to stop this kind of cycle?”
Patient medical characteristics.
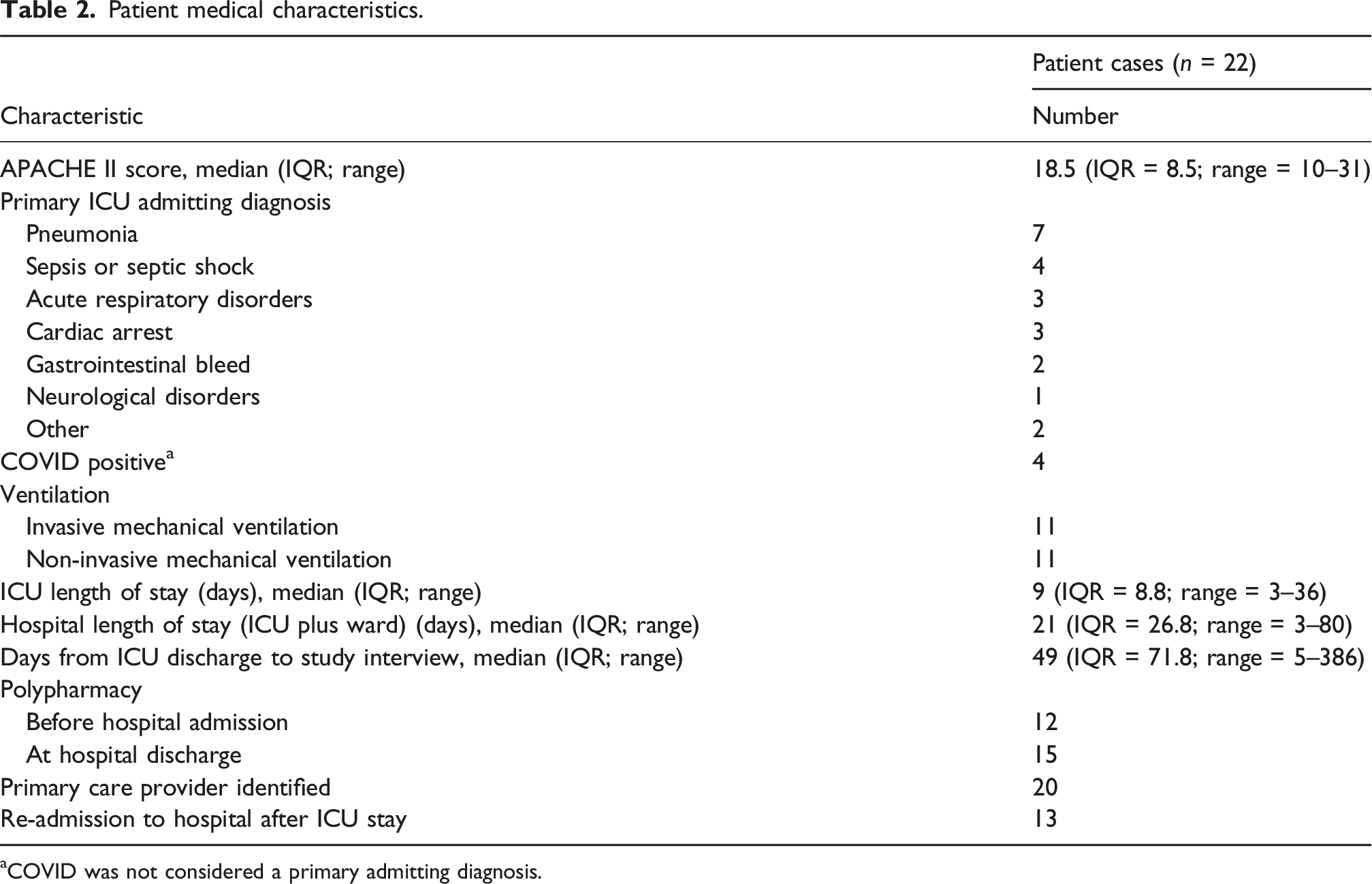
aCOVID was not considered a primary admitting diagnosis.
Caregiver accounts of their experiences made it apparent that the patient’s return home from the hospital was particularly daunting when the patient experienced multiple setbacks and both patient and caregiver felt overwhelmed by the prospect of managing the situation without adequate support. Some of the caregivers described occasions on which they felt they had reached their limit. For example, a 44-year-old daughter caregiving for an 80-year-old father who had been admitted to ICU with hospital-acquired pneumonia described reaching a breaking point after her father fell down the stairs and was re-admitted to hospital: “I explained to the paramedics that it’s just too much. I told him, look, I can’t do this. I cannot take care of him here. My mom can’t. So, something needed to happen.... So, basically that’s our experience where the person’s health is not very good and you are trying to get the help you need, but it’s not really happening. And I don’t really know how to just get it across that he’s not medically fit to be in a house.”
Similarly, as the patient’s health declined, many caregivers faced increasingly intense physical, emotional, and mental demands, leading to a gradual erosion of their own well-being alongside that of the patient.
Variation in caregiver capacity
The capacity to engage in caregiving appeared to vary greatly across participants and was influenced by many factors, including competing life priorities, work and childcare responsibilities, living arrangements, the availability of others to assist in caregiving, and financial resources. Several caregivers found themselves attempting to cope with the additional demands of declining health of a parent and care for their own children, without additional help or support; these situations often led to a sense of caregiver burnout. Caregivers who indicated they had an effective and comprehensive support network seemed less burdened; however, even in situations of strong support networks, caregiving was characterised as demanding and accompanied by serious caregiver strain. Some explicitly stated they worried about “burnout” whereas others described more general feelings of being overwhelmed, exhausted, hopeless, defeated, and even apathetic: “At first, I was [frustrated and disappointed]... then eventually, I didn’t care.”
Participants suggested that the more extensive their support network, the better-equipped caregivers felt to cope with the failing health of their loved one. When family members divided up roles, supported each other, problem-solved together, and maximized the expertise of different family members, caregivers fared better in terms of health and well-being than those who were more isolated with less support. In one family, the primary caregiver was the wife of a 67-year-old man who had been admitted to the ICU with congestive heart failure. Three daughters assisted their mother by splitting up caregiving tasks, with one daughter explaining how all three were needed to manage their father’s care; they had all taken time off work or school to help. However, even with that degree of family support, one of the daughters exclaimed: “It’s stressful... we can’t do it all.”
She went on to explain that, at times, conflict erupted in the allocation of responsibilities of care, a situation which was not characteristic of this particular family before the father’s illness.
Participants with smaller family support networks experienced more difficulties coping with the demands of caregiving. For instance, in one family, a 58-year-old daughter assumed the care of her 85-year-old mother but also shared how angry she was with her estranged sister, who was unwilling to help. In other interviews, family caregivers mentioned how they needed to rely on friends, neighbours, and community acquaintances or, in some instances, consider moving their loved one into assisted living for the support they needed. Some caregivers characterised the patient as relatively isolated, as indicated by a sister-caregiver who said of her 59-year-old brother: “[he] doesn’t have other people in his life.”
In these instances, there were no additional caregivers or supportive individuals to lean on and the enormity of caregiving often fell to one person.
Caregiver roles and the influence on critical illness recovery
Assuming daily living and physical care responsibilities
Most caregivers provided hands-on care for daily activities such as showering, teeth brushing, or dressing due to the patient’s ongoing fatigue, muscle weakness, and complex medical issues. Caregivers described these everyday activities as some of the most challenging, but necessary, aspects to support patient recovery. A daughter-caregiver shared how her days were spent: “Basically, trying to get her up and get her into the shower, or trying to get her up to get her to eat. Trying to get her up to use the bathroom. Trying to get her up to do anything.” (50-year-old woman caring for her 76-year-old mother admitted to ICU with sepsis)
Transferring patients with limited mobility from bed to wheelchair to bathroom was extremely challenging for older, frail, or smaller caregivers, and such physically demanding tasks characterised their days. In addition to physical care and hygiene, caregivers assumed full responsibility for all household duties such as cooking, cleaning, and shopping, many of which may have been shared before the illness. A husband-caregiver commented on the amount of effort it took to be a caregiver and continue to work outside the home: “I have to do everything, every single thing I have to manage, but I’m not used to this. Before, [patient name], she [did] everything for me. I just got to work and come home. That’s it. That was my job. But now I have to do everything. It's hard for me to manage.” (44-year-old man caring for his 38-year-old wife admitted to ICU with preeclampsia)
Caregivers felt pressured to manage daily care, household responsibilities, and their own careers, and most reduced or eliminated social and leisure activities to conserve time and energy. A daughter-caregiver remarked that she felt so burdened by the numerous responsibilities that: “I felt like I didn’t have a life anymore.”
The mundane tasks of laundry and housework piled up such that caregivers noticed they rarely had time to simply visit or be with their patient in a relational capacity.
Some caregivers juggled caring for more than one family member with a health condition. For instance, a 39-year-old mother who acted as a caregiver for her adult daughter who had been critically ill following a traumatic chest injury, also had a son diagnosed with autism and another daughter with marked mental health challenges. This mother described how caregiving over prolonged periods ultimately jeopardized her own health: “I'll get really bad stomach aches from the stress of worrying about everybody, and I just won’t do anything, and I have high blood pressure already. So, it’s hard…I need to be there for everybody else, [so] I can’t be there for myself.”
Overall, many caregivers described feeling exhausted by their complicated roles, without time to rest, recharge or look after themselves. A 53-year-old daughter caregiver explained how the stress of providing daily care resulted in the entire family feeling mentally and physically exhausted. She said: “We all lost an incredible amount of weight because we weren’t eating, we weren’t sleeping. I wasn’t around for my kids.”
This extensive family caregiving effort played a vital role in patient recovery. Having family members, rather than hired support, as caregivers offered reassurance to patients who were uncomfortable with, or did not trust, individuals from outside their family. Familial care also eased patient and caregiver anxiety and distress during recovery. However, participant accounts revealed many instances in which caregivers could not fulfill all physical and household requirements, resulting in inadequate nutrition, mobility issues and falls, missed appointments, and limited social interactions, thereby posing additional challenges to patient recovery.
Providing motivational and emotional support
Many caregivers described relentless efforts to persuade patients to engage in their recovery. For patients whose health plateaued or deteriorated, caregivers had to work hard to convince them to eat and drink, get out of bed, or participate in their recovery. Caregivers’ optimism sometimes contrasted dramatically with the patients’ exhaustion, poor mental health, and lack of motivation. This sense of emotional labour was, itself, a challenge for caregivers to maintain in the face of a conflicting sense of hopelessness or fear coupled with their perceived duty as the emotional anchors for their declining loved ones. Caregivers conveyed difficulty accepting the patients’ low energy and lack of interest in life, as though the patient’s inability to thrive reflected the caregiver’s own failure. A 50-year-old daughter-caregiver expressed frustration with her mother: “She never had the energy to be able to do anything. She always wanted to lie down and not really get up and do anything. And it was really hard to try to get her to get up and do everything.”
In some families, caregivers adopted the role of a taskmaster, giving the patient orders, schedules, and routines despite pushback, which resulted in tension and conflict. A frustrated caregiver described why he ordered his father to continue walking every day: “I need to yell at him because he had to realize that you need to get better. Like, there was a fine point. He started walking for 26 minutes a day from two minutes without sitting down… I tell him what we’re going to be doing and you need to do it.” (39-year-old man caring for his 72-year-old father admitted to ICU with respiratory failure)
In some families, the caregiver seemed to assume a role more like a parent or ‘boss,’ setting rules, giving directions, and gauging progress. A 70-year-old caregiver commented on how she monitored her husband’s condition, not allowing him to go out to the shop alone and ensuring he always wore a mask to protect against infection.
Caregivers also monitored the psychological state of patients, observing their low mood and potential signs of depression. Caregivers and patients struggled to cope when patients showed depressive symptoms, with caregivers increasing their optimism and patients withdrawing further or exhibiting reactivity. A caregiver-mother described how her adult daughter insisted, “I’m good, I’m good,” but then would sometimes “explode” with anger, challenging her own composure. Caregivers felt the need to promote optimism when patients showed signs of poor mental health, including depression, even if they did not share in it themselves. One 70-year-old caregiver shared that she protected her husband from the medical prognosis that indicated his lungs may never heal; instead, she chose to say to him: “You’ll be just fine, we can always ask for oxygen... positive thinking, positive thinking.”
In the case of a survivor’s declining health, there existed a complicated balance between maintaining hope for continued recovery to protect a loved one, whilst knowing such hope was false.
Searching for and gathering information
Caregivers took on the task of searching for and gathering medical information because most families had received minimal details about the patient’s critical illness, recovery expectations, home care instructions, or contact information for assistance. Without information or a comprehensive plan, caregivers described their approach as: “one day at a time.”
After discharge, families often felt abandoned by the hospital system and lacked vital information for identifying and accessing social and community services they identified they needed, such as financial assistance, subsidised living arrangements, physiotherapy, and addiction counselling. A caregiver, whose elderly father had been admitted to ICU for respiratory failure and showed signs of dementia once home, learned about a geriatric assessment clinic entirely by accident. They expressed bewilderment that no one in the healthcare system had given their family information about the clinic that might have been beneficial.
Caregivers described feeling overwhelmed and lacking the knowledge to make the best decisions to support patient recovery or react appropriately when the patient’s health declined. As a 77-year-old mother-caregiver remarked about her 56-year-old son’s worsening condition: “I didn’t have a clue what to do.”
Caregivers reported that communication with healthcare providers during the recovery period was inadequate, with medical information sometimes given by telephone to the patient, or an elderly family member, who was unable to fully understand and relay all the details. Some caregivers felt they needed more medical knowledge to interpret information, with several seeking to fill in gaps with internet searches for medical conditions and treatments. One 39-year-old caregiver suggested that his father’s recovery following an ICU admission for respiratory failure had depended on him learning to interpret his father’s bloodwork, then searching and interpreting disease management information online: “Learning every day. Figuring out his sodium, how to do it... Believe it or not, I didn't give him water because water would kick out the sodium too quickly. So, I ended up giving him Gatorade, and Gatorade started helping balance the GFR [glomerular filtration rate] and the creatinine.”
Thus, for many, caregiving required considerable self-education about medical conditions and relevant supports. However, as a caregiver participant who herself happened to come from a “medical family” said, “You still had no clue what to do. I mean, other than what we know ourselves, it was left to be intuitive. I don't think people have enough intuition to come out of ICU and the stressors that ICU have in your lives.” (67-year-old woman caring for her 68-year-old husband admitted to ICU with COVID-19 and indolent lymphoproliferative disease)
Lack of information and communication left many caregivers feeling they were improvising day by day based on information they gathered themselves.
Monitoring and supervising health and treatment
Caregivers constantly monitored, and informally assessed, the patient’s health, and recovery or decline. They tracked diet, swallowing, weight fluctuations, mobility, blood pressure, breathing issues, oxygen levels, and body temperature, among many other measures, always on alert for changes. At home without professional guidance, caregivers worried about any deviation in readings or symptoms, often being highly vigilant in their surveillance due to uncertainty about what such changes might mean. A mother-caregiver described the anxiety inherent in not knowing: “One thing that’s been a challenge is all her stitches, because there’s a lot of care involved in taking care of those, and they didn’t really give us any instructions. So, we’ve just been like winging it and there’s obviously a lot of stress about it getting infected. We don’t know if it looks right or it doesn’t, but then we don’t want to go sit in emergency for six hours for them to tell us, oh no, it’s fine.” (39-year-old woman caring for 19-year-old daughter admitted to ICU with traumatic chest injury)
When changes were noted, caregivers often struggled with deciding whether to continue monitoring symptoms or to call for professional assistance. A 62-year-old woman caring for a husband who had survived a gastrointestinal bleed described noticing how his stomach had “hardened,” and he appeared to be staggering. Uncertain about what to do, the caregiver decided to call for help: “I tried calling the home healthcare lady or the nurse, but she wasn’t available, and I was just kind of waiting for her to call back.”
In these kinds of situations, caregivers were forced to wait, and if symptoms worsened, their only recourse was to call paramedics and face a possible emergency department visit and hospital readmission.
Tracking and administering medications were also a key responsibility for caregivers. In some instances, pharmacists were a helpful resource. Other caregivers reported struggling to address medication side effects and pleaded with healthcare providers to review and modify prescriptions. Sometimes, even a simple task, such as obtaining a medication refill which required a doctor’s approval, could prove highly challenging when healthcare providers were unavailable.
Managing medical appointments and advocating for resources
Arranging medical appointments with primary care providers, specialists, and allied health practitioners was a constant challenge. ICU survivors attempting to recover at home lacked ready access to primary care referrals to specialist physicians and services. Families without a primary care provider were forced to go to a hospital or urgent care centre. When specialist referrals were available, caregivers had to arrange for transport for patients to attend appointments. One daughter-caregiver explained how difficult this could be in relation to her father who was recovering from an ICU admission for congestive heart failure and required a wheelchair: “How do you get him into a car? There’s only one taxi company in [city name] and you have to book them only 24 hours in advance... it was very challenging just to get him to an appointment.” (53-year-old woman caring for her 67-year-old father)
Overall, many caregivers expended a great deal of effort coordinating medical appointments without a designated point person or scheduled follow-up. A daughter-caregiver referred to the situation as a “big goose chase” because she had incomplete medical information about her father, who had been admitted to ICU for a cardiac arrest. Frustrated, she explained: “Now we’re still waiting for follow-ups with two different doctors that we still haven't gotten. He’s been out for almost a month.”
In other situations, the caregiver felt they knew what was needed for the patient to recover at home, but medical professionals disagreed. A daughter-caregiver shared how it took multiple emergencies related to breathing issues before her father was prescribed home oxygen: “We had a hard time getting the oxygen at home. We knew he needed it. We asked them for it. They did one test one afternoon and said, ‘No, he doesn't need it. We're discharging him without it.’ Within a couple of days, we had to call because his breathing was such that he wasn't saturating enough with his oxygen. He ended up having to go back into the hospital. They got him on a breathing app right away. And then I think it was the second, third time that he finally passed the threshold to receive oxygen at home.” (44-year-old woman caring for her 67-year-old father admitted to ICU with congestive heart failure)
Across caregiver interviews, we heard similar accounts of an over-burdened healthcare system that required persistence, skill, and patience to navigate. Characterising the advocacy process of obtaining necessary home support as a “fight,” one daughter-caregiver expressed dismay and frustration with home care: “They would come and say, ‘Well, we can feed him or we can change him. That’s all we can do.’ Well, that’s not what he needs.”
Many caregivers reported similar frustrating experiences of a mismatch between what home care workers were authorized to perform and what supports they felt were needed for recovery. Further, multiple visits a day from different care workers were reported. These rotating schedules made continuity in care impossible, leaving the caregiver to coordinate all aspects of care, as well as filling gaps in support. Families felt at odds with the system: on the one hand, trying to work with the healthcare system to support the patient in recovery, and on the other hand, fighting a system whose failures seemed to be jeopardizing both their own wellbeing and the recovery of their loved one.
Discussion
In our findings, the experiences and roles of caregivers were influenced by variations in patient health and recovery trajectories. Prior research has described distinct subtypes of critical illness survivors.22,23 For example, Ferrante et al., 22 identified three distinct functional trajectories among 754 older adults post-ICU: minimal disability (21%), mild to moderate disability (28%), and severe disability (51%). Iwashyna 23 proposed three critical illness recovery trajectories: the Big Hit, where patients experience an acute loss of function during their critical illness from which they gradually recover; the Slow Burn, where patients experience new, persistent, and more rapid decline; and Relapsing Recurrent, where patients experience acute exacerbations and then partial recovery. Our findings show the implications of different recovery trajectories on caregivers. Particular strain was felt by those caring for patients who faced stagnating or worsening health, with fear and uncertainty experienced when the assumed norm of a steady recovery was not apparent.
Family caregivers of critical illness survivors assist with activities of daily living and management of emotions, development of self-management strategies, and identification and engagement of additional support from family, friends, and formal support services.10,24 Others have highlighted the encouragement and coaching provided by caregivers to critical illness survivors,10,24,25 which appears somewhat akin to the motivational support in our study. However, a novel finding in our study was how motivational support caused frustration and could be highly taxing, especially for exhausted caregivers, and contributed to interpersonal tensions. We have further elaborated the intensity and extent of caregiving and the caregiver burden.
Our study uniquely revealed variations in caregivers’ capacity to provide care and further evidenced the value of social support.7,13,26 Caregivers juggling additional employment and family responsibilities, with limited or fragile social support, conveyed significant struggles. Conversely, shared caregiving and greater social support reduced the risk of caregiver strain, and so seemed to have the potential to enhance patient recovery.
Implications
Strategies to support caregivers could reduce caregiver strain and so promote patient recovery. Strategies that begin in the ICU could include involving caregivers in discharge planning, assessing the home environment, their capacity to provide care, providing written information and anticipatory guidance. Information and guidance could include ICU diaries, plain language discharge summaries, medication education, information on PICS and PICS-F, and recovery expectations. In the absence of formal recovery programmes, access to healthcare team throughout recovery should be supported by guidance on accessing primary, specialist, and emergency care, as well as community support such as physical therapy, social work, counselling, respite care, and financial resources.16,20,27
Helping families identify their established and potential support systems before and after patient discharge may also reduce poor outcomes. 24 Peer support programmes are particularly promising.11,28,29 For example, caregivers who participated in a peer-supported, multidisciplinary programme for patients and caregivers, demonstrated improvements in anxiety, carer strain, and insomnia compared to caregivers who did not participate. 11 Peer- or professionally-led support may further facilitate the sharing of information and resources to address caregiver strain and offer a means through which caregivers can receive validation of their role and encouragement of self-care.
The limited healthcare and community support for caregivers reflects a broader caregiving crisis in Canada and globally, and a lack of change to improve discharge planning and support beyond hospitalization. Strengthening primary care could improve care coordination and help connect patients and families to necessary resources and specialties. Patients and families need timely and consistent access to functional community care, including home care, rehabilitation, mental health resources, and social support. Wider healthcare system transformations to better meet the needs of patients and caregivers beyond hospitalization will require a significant shift in political and healthcare system leadership. More focused policy interventions could include mandating caregiver involvement in hospital discharge planning, expanding paid caregiving leave, and financial relief through tax credits and caregiver stipends. Enhanced access to respite services, counselling, and support groups for patients and caregivers could improve mental health. Continuity of care could be improved by standardizing evidence-based transitional care processes, implementing dedicated transition or discharge coordinators across acute and community settings, mandating post-discharge follow-up for high-risk patients, and increasing investment in community programs.
Strengths and limitations
Our sample only captures some caregiver experiences, features of our sample include patients with a relatively high illness severity compared to typical post-ICU studies, given the median ICU stay of 9 days and median hospital stay of 21 days. This likely contributed to the extent and complexity of the caregiving described. Recruitment occurred during the COVID-19 pandemic, and the related strain on the healthcare system may have affected participants’ experiences and our findings. Caregivers who declined to participate cited exhaustion and feeling overwhelmed. Our reliance on virtual interviews limited participation to those with phone or internet access. Despite these limitations, our study benefited from a diverse range of family caregivers and the details they shared, offering insights for other post-ICU contexts.
Conclusions
Given the extent of support required for patients to recover at home following critical illness, informal family caregiving directly influences patient recovery. However, the demanding and complex nature of this caregiving contributes to substantial caregiver strain. Strategies to support family caregivers will be key to the recovery of critical illness survivors. Mechanisms of support must be initiated in the hospital, extended throughout the recovery trajectory, effectively aligned with community resources, and coordinated.
Footnotes
Acknowledgments
We would like to thank Bernard Lynch, Miki Tsui, our other patient and caregiver partners on our Critical Illness Survival Patient Advisory Board, Hiroki Sato, our other multidisciplinary research team members, and our participants for their support on this project.
Ethical considerations
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by The University of British Columbia Behavioural Research and Fraser Health Research Ethics Boards (H21-01378 approved on 19 September 2021). Informed consent was obtained from all subjects involved in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Institutes of Health Research (AWD-016294). A.F.H. holds a Scholar Award and S.C. a Trainee Award from Michael Smith Health Research British Columbia.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: R.C.A. has received Honoraria from Edwards Lifesciences and HLS Therapeutics Inc. R.C.A. is on the Advisory Board for Renibus Therapeutics Inc. All honoraria and board membership are for work unrelated to this manuscript. S.C. has received honoraria from Baxter Healthcare Corporation for work unrelated to this manuscript. No other authors have any potential competing interests to disclose.