
Abstract
Objectives
Central government has been promoting closer integration between the National Health Service (NHS) and local government social services in England for more than five decades. Improved coordination between primary, hospital, community health and social services has been advocated as a cost-effective response to growing care needs in an ageing population. This paper concentrates on one of the principal local care coordination mechanisms: community-based multidisciplinary teams (MDTs) involving NHS and social services staff. It reports local leaders’ perceptions of MDTs’ current and future contributions to more coordinated care and support systems in two integrated care Pioneer sites.
Methods
Thirty-two qualitative semi-structured interviews with 25 local system leaders and operational managers in two contrasting Integrated Care and Support Pioneer areas were conducted between October 2018 and April 2021, as part of a wider evaluation of the Integrated Care and Support Pioneer Programme. Eight of those interviews took place after the start of the COVID-19 pandemic and between lockdowns. Interviews were analysed thematically.
Results
Local leaders in both areas broadly shared a vision of integrated care in which MDTs were essential mechanisms for coordinating improvements in health and wellbeing, especially for older people who are frail, experience falls and have long-term health conditions. Organisational differences between and within sites influenced local decisions about the purpose and structure of MDTs, but, despite such variations, interviewees identified similar challenges to implementation. Staff turnover, often linked to funding uncertainties, and the lack of shared information systems, were among the most frequent operational challenges noted. System leaders valued national policy frameworks as potential enablers of integrated care but also recognised the role of local contexts in shaping local implementation decisions. Interviewees highlighted benefits emerging from multidisciplinary working, including its potential to deliver more holistic care, fewer instances of work duplication, speedier access to care and enhanced home care provision. However, they were concerned such benefits were not always captured by commonly used performance indicators and thus the value of MDTs could be under-estimated.
Conclusions
Local contextual variables and local understandings of these variables appeared to be the main influences on variations in local responses to national expectations of improvements in care integration. Local leaders in both areas broadly shared a vision of integrated care in which MDTs provided essential mechanisms for securing interdependent improvements in both the health and wellbeing of local populations and improvements in workforce job satisfaction.
Introduction
Central government has been promoting closer integration between the National Health Service (NHS) and local government services in England for more than five decades. 1 Vertical and horizontal integration across primary, hospital, community health, social care and other services, such as those provided by the community and voluntary sectors, has been justified on the grounds that the population is living longer and with more long-term conditions that often require managed access to different types of treatment, care and support simultaneously or in succession. 2 Between 2013 and 2018, the Department of Health in England initiated the Integrated Care and Support Pioneer Programme to promote coordination between services. 3 The programme comprised 25 volunteer Pioneer sites, selected through a competitive bidding process, to provide examples of successful health and social care integration which could be rolled out at speed across England.
The Pioneer Programme was initiated by the Coalition Government of 2010-15, which followed its predecessors in emphasising the importance of integration both to extend person-centred care and to increase cost-effectiveness. Following the passage of legislation in 2012 to reshape the NHS, the government published Integrated Care: Our Shared Commitment 4 outlining both an overall strategy for integration, and also the intention to establish pioneer sites to lead its development across England.
The document was heavily influenced by prior development work conducted by National Voices, a coalition of health and social care charities operating to meet a wide range of health and social care needs. Initially commissioned by the NHS, in the light of evidence that the existence of multiple definitions of integration was a significant barrier to change, National Voices was commissioned to develop a narrative about integrated care so that the public and professionals could share a common and meaningful understanding of what it looked like from the perspective of individuals and carers in language that everyone could identify with. This exercise produced the first nationally accepted definition of integrated care as ‘person-centred, coordinated care’ and a narrative for good practice in integrated care based on a series of ‘I’ statements such as ‘I can plan my care with people who work together to understand me and my carer(s), allow me control, and bring together services to achieve the outcomes important to me’. 5 Today, integration of this type remains the organising principle for the Integrated Care Systems in England2,6 and is supported by the Better Care Fund (BCF), a mechanism for pooling resources between the local NHS and local government to enable the provision of more integrated services. 7
One of the most widely employed methods for integrating care has been multidisciplinary teams (MDTs) offering individualised case management and support to promote independent living and reduce need for either acute hospital or residential care.8,9 We provide elsewhere in the supplement more details on the Pioneer programme and MDTs. 10 In this paper, we focus on 11 community-based MDTs in two of the 25 Pioneers and how they developed over six years (2015-2021). This time span is a relatively long one for studies of integrated care and included the challenges those teams faced during the COVID-19 pandemic (which we report elsewhere in this supplement). 11
This research builds on earlier work focused on the initial wave of Pioneer sites. 12 We report elsewhere in this supplement on the barriers to service integration and evaluation. 13 This paper reports on another component of the MDT evaluation, namely the perspectives of leaders with strategic and/or senior operational responsibilities on the origins, roles, tasks and operation of MDTs. We explore how local system leaders in those sites understood the potential and actual contributions of MDTs to person-centred, coordinated care and support.
Our research questions comprised: (1) How did the MDTs originate and what were their principal objectives? (2) How were the teams structured, staffed and resourced? (3) What functions did they perform and how did they relate to the wider health and care system locally? (4) What implementation difficulties emerged and how were they overcome? (5) What would successful MDTs look like and what evidence was being collected about their performance?
Methods
Our evidence was obtained from interviews and local documentary sources. The documents comprised local papers outlining integration strategies, the role of MDTs within the context of such strategies, and formal proposals to establish MDTs (including roles, staffing, location and funding, together with reviews of their operation where these existed). The documents were mostly consulted in advance of the interviews and, indeed, assisted in the structuring of topic guides. Others were identified during the course of interviews and obtained thereafter. Together with our observations of team meetings, reported elsewhere, 14 we conducted 32 semi-structured interviews with 25 local system leaders and operational managers in two Pioneers, utilizing a snowballing technique to build the sample. The interview schedules (see S1 and S2 in Supplement A) and documentary analyses were based on the research questions, informed by policy and practice literatures on MDTs, as well as the early evaluation of the Pioneers and the initial findings of the longer-term evaluation. Noting the apparent ubiquity of MDTs in the early evaluation, 15 we sought to map MDTs’ forms and functions, to establish how far we were dealing with similar or different approaches to multidisciplinary working and how far such differences could be seen as locally designed bespoke adaptations to particular features of local contexts.
The interviews took place between October 2018 and April 2021, including eight interviews conducted between lockdowns during the COVID-19 pandemic. The interviewees occupied a range of roles, including primary care managers, urgent care managers, community team leaders, heads of service, clinical leads, directors of adult social services, directors of public health, and commissioning managers. Some managers were also directly involved in MDTs as GPs or community matrons. Approximately one-third of the respondents were local authority social services employees.
The interviews were conducted by GW, ND and LT and transcribed verbatim. Transcripts were coded in NVivo 12 by three researchers (LT, AP, LR) using an analytical framework initially developed by GW and LT. The framework was informed by the initial research questions, interview schedules and awareness of some of the apparently most critical issues encountered during interviews. Once the dataset was coded, the analytical team (AP, LR, MAD, GW, NM) met regularly to discuss the key findings and themes identified in the narratives. Quotes used in the results section are denoted by the site of the participant (P1 and P2) but to preserve anonymity, individuals’ roles are not identified.
Two contrasting Pioneer sites
Pioneer structure and MDTs model in the study sites.
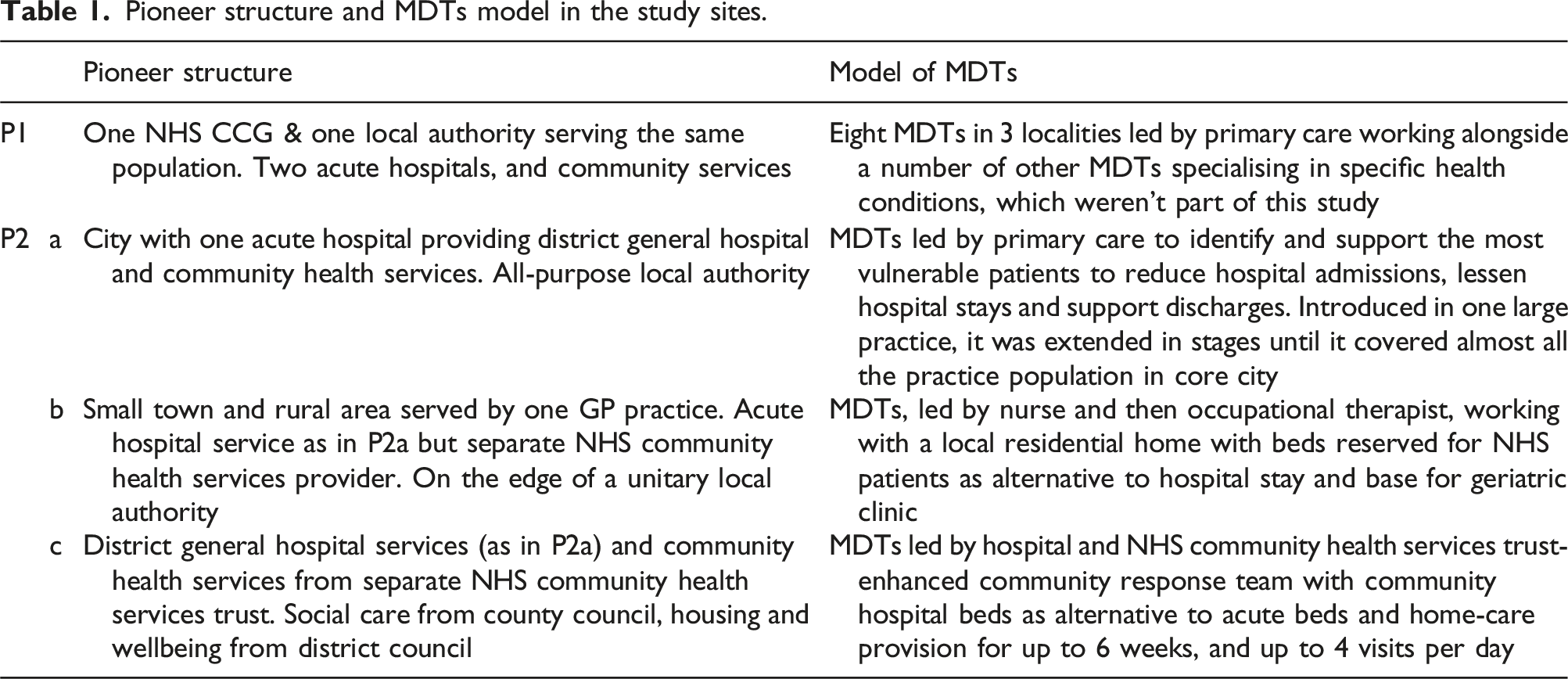
P1, located in a unitary authority within a larger conurbation, had a socially and economically diverse population with notable inequalities in mortality and morbidity. P1 had the simplest geographical and functional context, as its NHS Clinical Commissioning Group (CCG) responsible for organising the delivery of NHS services and local authority responsible for local social and other services shared the same population.
P2 was more organisationally complex. Its CCG boundaries encompassed one entire local authority (which we have designated P2a) and parts of two others (P2b and P2c), with social services responsibilities. Its population was approximately 30% larger than P1. These administrative and geographical complexities resulted in a higher number of stakeholders with organisational interests to advance and defend as well as higher transaction costs of communication and coordination.
Both the CCG and NHS acute hospital in P2 faced significant financial challenges, absorbing senior management time and potentially fostering blame and cost-shifting behaviours across organisational boundaries. The local authorities also experienced financial constraints, and developed their financial and service responses to funding gaps largely independently of each other and of the NHS.
The national Better Care Fund played a crucial role in supporting the development of multidisciplinary teams (MDTs) for older people in both sites, particularly influencing MDTs’ structures in P2. As in many other locations, 16 CCG leaders utilized the BCF to incentivise NHS primary and community health care providers to collaborate more closely with the three local authorities. Competitive joint bids were sought from primary care, social care, and other partners in each area to establish centralized community services, enhance multidisciplinary collaboration, and facilitate community-based care as an alternative to hospital admission or to enable earlier discharge from hospital. Initially seeking a single preferred model, the CCG funded bids from each area, intending to adopt the most successful as its longer-term standard approach.
Results
The results are organised to address each of the research questions set out above.
Origins and initial objectives of MDTs
Despite the many differences between the two Pioneers, local system leaders in P1 and P2 had largely similar understandings of the guiding principles informing their integration initiatives. Those in P1 referred to the long local history of a person-centred ethos in health and social services which had enabled a ‘natural progression’ to Pioneer status: We became a Pioneer because we were already thinking about these things, and so that informed our submission to be awarded Pioneer status really … [P1 has] always been … ahead of the game in that respect, we’ve had some quite visionary clinical leads … We’ve had a real, very person and patient-centred view of how we should be optimising care for our patients. (Interviewee 2, P1)
The principal objectives of integrated care in P1 were described as being based on the ‘I’ statements developed by National Voices,
5
with their emphasis on proactively identifying unmet needs and reducing acute admissions and lengths of stay by improving care outside hospital. While the ‘I’ statements were rarely identified by name, interviewees tended to frame MDTs’ aims in terms consistent with their content. In addition, local system leaders reported that they soon realised that improvements in care could only be met by addressing wider social determinants of health: It became quite clear relatively fast that housing was a major driver for people’s health and wellbeing, and so … we worked with the local authority to develop a role which was kind of like where a social worker worked within the housing department as well, so it was a bit of a joint role, housing and social care … within the team. That really enabled us to … have an impact on addressing the housing issues that were so often a concern for patients. (Interviewee 1, P1)
This approach reflected the emphasis in P1’s Pioneer bid that ‘the focus of our integrated care programme is to improve health and wellbeing at a wider population level, as well as coordinate care better for the more intensive users of services … taking a whole system approach’ to population health (internal document).
In P2, the key principles underlying integration were those of patient-centredness and enabling people to live independently at home longer through better collaboration between health and social care. However, as one of the senior NHS staff involved in the Pioneer bid frankly admitted, they had started from a very low base of understanding about social care and the voluntary sector, including how they operated in practice: You didn’t know anything about any of those services. I thought the voluntary sector were people who collected money outside [named supermarket] and that’s how they got all their money. With social services, I thought they were the people on the phone who just said, ‘No.’ So, there was a very, very steep learning curve. (Interviewee 1, P2)
With a target population of frail and older people, the purpose of multidisciplinary working was also defined by interviewees in P2a as meeting growing demand by extending the range of care delivered in the community. In health, this involved developing wider familiarity with what was locally available by creating a directory of services that could be used to help the patients: When I first started, it was explained to me that, as a part of my role, we want to engage with the third sector more and we want to increase referrals to the third sector as a way of giving better quality care and also reducing pressures on the team. I was tasked with coming up with a directory of services … It was a great learning tool for me to find out what was out there. (Interviewee 12, P2)
Organisation of MDTs
In P1, several MDTs were established as ‘test and learn' sites prior to the Pioneer and expanded within a locality model of integrated care. These sites involved eight GP practices in three geographical areas, each implementing different meeting approaches: face-to-face, video conferencing, and targeting specific professionals for specific case discussions. The pilots also aimed to enable core teams of professionals (including GPs, nurses, social workers and mental health specialists) to test collaborative ways of working to achieve seamless, coordinated, and proactive care. Interviewees noted improvements in rapid response, long-term case management, proactive care, and patient self-management.
After initial piloting, P1 adopted face-to-face meetings as its preferred model (Table 1) and, by the onset of the COVID-19 pandemic, had established eight MDTs covering all practices. While teams were initially organised according to practice preferences, the final structures were based on population and geographical boundaries: That bit of work needed to be more defined than simply having a kind of weekly or fortnightly MDTs’ meeting, so we did a lot of work over the last 18 months on looking at what size of population we would want the [MDTs to cover] … There was some equalizing between the population sizes and the number of practices, and then also getting them more geographically aligned as well. (Interviewee 3, P1)
When our evaluation began, initiatives complementing the MDTs’ work were already underway (e.g. services to identify people living with moderate frailty who might benefit from early intervention and prevention initiatives). As reported elsewhere,
14
MDTs met weekly and membership included administrators, GPs, senior nurses, voluntary sector representatives, local authority representatives, social prescribers and mental health professionals. While the MDTs’ membership was described as ‘fairly static’, not all of these groups attended with the same frequency. There were also perceived to be gaps in team membership: I think probably the area where we’ve struggled the most to get consistent input is from the mental health teams … We could have had a pharmacist in the team … there are a lot of really good reasons that you could have done that, but we didn’t. You could have had an OT in the team, and we didn’t. So, you’re always drawing a bit of an artificial line. (Interviewee 5, P1)
In P2, three models were established as different approaches to integrated care (Table 1). As such, they reflected the different histories, service systems, needs and development opportunities in each of the three P2 sub-areas. This approach demonstrated that, as in P1, commissioners saw the implementation of multidisciplinary working as a developmental process. They did not possess a prior blueprint for MDTs of either national or local design. Rather they were seeking to try out different approaches and develop local ‘ownership’ of whichever seemed to work best locally.
The BCF provided both the incentive and opportunity for bids to be developed with each of the three adult social services departments to which the CCG related. The CCG was looking for MDTs combined with intermediate care beds and one point of access to services outside hospital: The funds were based on the Better Care Fund … The then clinical chair of the CCG had a vision that he wanted three different [approaches to out of hospital care] piloted … At the time we felt it was to see which worked the best … so it felt as though there was a bit of competition between us at the beginning, although there was an awful lot of shared learning as time went on over those first few years. (Interviewee 1, P2)
P2a was described by most local system leaders as the most proactive of its three schemes. Participants (e.g. Interviewee 11, P2) highlighted the crucial leadership role of a specific GP, who had initiated the project and who was widely respected for being able to work effectively across services and sectors. A care and support sub-team in P2a provided an immediate response to patients leaving hospital, until longer term support could be mobilised. The sub-team also identified and approached vulnerable patients at home and connected them with community and voluntary sector resources. The strength of the sector reflected the local authority’s long-term investment in building community capacity through, for example, its Local Area Coordination programme. In contrast, a key focus of P2b lay in offering more beds, regular geriatric clinics and end-of-life planning for care home residents. Lastly, P2c was initiated by, and led from, the integrated NHS Acute and Community Health Services Trust with input from the GPs and other professionals. One of those involved in its design and establishment provided a perspective on its development: One of the first things we did when I came into post was held a half-a-day workshop session with representatives of most of the practices down in [P2c] - consultant geriatrician, somebody from our community services … We got everybody in a room and said, ‘Okay, we’ve got this pot of money that’s coming. It needs to be about stopping people going into hospital unnecessarily, because that’s where savings are going to come out to pay for it; it needs to drive more integration both between different parts of health and health and social care; and it needs to reflect what’s the population challenge in P2c; and it needs to be owned by all of us.’ (Interviewee 4, P2)
However, there were some concerns about the costs of this model among commissioners and providers. A provider leader recognised that: When we look at the national audit of intermediate care, our skill mix between registered and unregistered [staff] is absolutely at the top end ... The strength is it’s a cost-effective model … You’ve got the right people going in, who’ve got the skills across all of them to deliver the care plan, rather than a professional going in who just does their bit and then somebody else does [theirs]. (Interviewee 4, P2)
The integrated NHS Acute and Community Health Services Trust suggested that differences between the local authorities in P2a and P2c in commissioning reablement services were an impediment to providing an integrated model of intermediate care. Reablement services were contracted out in P2a, but provided inhouse in P2b. As a result, in P2a the Trust was working closely ‘with the private reablement provider, (in) a much stronger one-team approach to intermediate care and reablement … [including] jointly triag[ing] all the referrals’ (Interviewee 4, P2). But a similar ‘one team’ delivery model in P2b was more difficult, because the NHS thought the local authority saw the development of ‘an entirely joint intermediate care and reablement service’ as a challenge to the local authority’s control of inhouse services and a possible threat to its continuing responsibilities for providing reablement services.
Functions of MDTs
One of the more fundamental differences between the two Pioneer sites lay in the populations they targeted, which in turn helped shape the functions adopted by their MDTs. From the beginning, an explicit function of the P1 MDTs was to support GPs responding to complex cases with multiple needs. As well as older people, patients discussed in MDT meetings included people living with disabilities, mental health problems, and continuing social needs. In anticipation of such demand, two senior social workers were recruited with housing and social care experience to lead the local authority representation on the MDTs: It’s addressing the complexity the patients face in terms of having to deal with multiple organisations … They’re getting care from the local authority, from different NHS providers, from private providers, and we’re trying to bring that together, slowly, complicatedly, bit-by-bit. (Interviewee 8, P1)
The establishment of the MDTs created the possibility of a more proactive approach to addressing those complexities: There was this opportunity to take a more proactive approach … with people who we think are going to go off their feet, and we’re just beginning to see things that aren't working right, and allowing clinicians to use their own acumen to identify those people who might be a risk. (Interviewee 1, P1)
In contrast, MDTs across P2 were more explicitly focused on older people with complex long-term conditions, bed-bound patients and care home residents. Thus, they engaged more exclusively with the wider care system for older people. One of the local system leaders in P2 described how the team in P2a had established itself as a reliable point of immediate contact: If your GP phones the community response team [a mainstream team outside the MDTs] they will get somebody who might say, ‘Well I can't go today.’ So even if they’ve got carer capacity, they can't send a carer because they have to have a nurse or a senior person assess them first … So, we are now on CCG’s sort of page of care in the community. We are, ‘Phone the [P2a MDT’s name] first.’ We’re the first go-to team. (Interviewee 1, P2)
Further, local system leaders in P1 and P2c noted unintended positive effects of their integration initiatives. These included the spillover effect of MDT staff having some unused capacity to provide care to people in their own homes.
Implementation difficulties
Local system leaders in both sites acknowledged the importance of gaining active stakeholder support, fostering new professional relationships, and cultivating shifts in organisational cultures to promote integrated care. Interviewees highlighted the significance of securing frontline staff commitment through negotiation, and a focus on individual needs and outcomes. For example, in P1 some GPs initially expressed scepticism about dedicating time to discussing patients from practices other than their own and raised concerns that framing MDTs’ goals around early hospital discharges might not align with their principles of good practice. MDTs had to overcome such resistance: It’s actually about better care and a better patient experience. I think the pitching of it as, ‘Let’s get patients out of hospital,’ [means] it’s not always clear to GPs why that is necessarily a good thing. (Interviewee 2, P1)
In P2, some interviewees said NHS acute trusts’ scepticism about the feasibility of reducing the number of hospital admissions was prompted by the trusts’ perception that such plans would simply undermine their incomes: I've worked in an acute trust; I know how that works. I have sat down every September for many years and written plans that involved bringing more people into the hospital so we can get more money, so that’s a really difficult mindset to set aside overnight. (Interviewee 3, P2)
The lack of sufficient funding for MDTs was also considered a significant barrier to new plans, especially in securing commitments from social care. In P2, for example, financial pressures had historically generated tensions in relationships between local authorities and the CCG: I think there had been quite a long history of tension between the CCG and the council, some of which will have been around financial pressures and competing priorities ... At a leadership/system level there was not a lot of rapport, and there was some distrust … Everything was a challenge, everything was combat … We’re in a different place now, we’ve got different characters around [e.g. senior leadership], but also actually some of the mechanics are different. (Interviewee 7, P2)
Another financial problem was the reliance on short-term funding, especially from the BCF, for hiring staff at MDTs. Interviewees thought short-term funding affected team dynamics by creating employment uncertainty for some staff, increasing turnover and restricting the development of expertise. Interviewees thought longer-term funding would create greater confidence among frontline staff about the continuing priority for integrated work. Stable and diverse team membership enhanced individual practitioners' knowledge base, improved working relationships, and facilitated efficient communication. Ensuring long-term funding for all relevant staff was deemed especially critical in areas with recruitment and retention challenges, including the rural areas of P2.
Given the importance of strong leadership in building relationships across organisations, changes in leadership were perceived to be particularly problematic, potentially disrupting trust between stakeholders, and continuity of the vision, aims, and objectives of integration: You may get someone who you’ve a good relationship with for five or 10 years and they suddenly leave, and then the next person who replaces them are not as contactable or that working relationship isn’t there. (Interviewee 7, P1)
Additional challenges, also discussed by frontline staff, 17 included difficulties around information sharing resulting from not having a unified clinical records system. Those and other challenges were also affected by the COVID-19 pandemic, which we describe elsewhere in this supplement. 11
Further information on the challenges faced by both sites is given at S3 in Supplement A.
Measuring success of MDTs
Interviewees acknowledged the need to assess the performance of MDTs to secure long-term funding. Local system leaders identified various potential approaches to performance assessment, but also highlighted the challenges that still needed to be addressed: There have been repeated cycles of work, … going on at a CCG and a now [city] level, around monitoring success for all sorts of different interventions, outcomes. What outcomes are we looking for? How do you measure them? Patient experience is one, but it is hard to pin down. I suppose a lot of it is qualitative. I suppose it would be one of the interventions that over time would feed into data like reduced length of stay, reduced readmission rates. (Interviewee 2, P1)
A further potential difficulty in assessing performance was seen to arise from reliance on local (professional) judgements, especially in P1, instead of using more formal patient risk stratification tools. As a result, comparable evidence was not available to review the performance of the teams in P1: I suppose my slight anxiety is that we don’t use a risk stratification tool, so most [MDTs] bring patients from lists, people that have been in hospital, people that they want to discuss. Actually, how do you get evidence that what you’ve done has made a difference? (Interviewee 6, P1)
A particular tension was between the goal of reducing hospital admissions, an initial aim of integrated care, and its appropriateness as an overarching success measure. Interviewees acknowledged the objective of minimizing avoidable hospital admissions through integration, but said adopting it as a performance metric raised concerns. Some system leaders highlighted the subjectivity of clinical opinions in categorising admissions as ‘preventable’ and changing definitions of the term ‘admission’. One respondent said reducing admissions or shortening hospital stays might simply shift the burden of costs from the NHS to social care budgets. Furthermore, hospital staff expressed concerns about jeopardizing the hospital’s financial stability by reducing admissions.
Overall, most system leaders considered that applying quantitative performance measures to the work of teams was problematic and suggested qualitative indicators might be more useful. Individual stories of staff working together in integrated ways were viewed by some respondents as having the advantage over ‘hard evidence’ in conveying the benefits of MDTs. ‘Storytelling’ was perceived to be a valuable source of feedback but insufficient to secure the future of MDTs, and needed to be complemented by evidence of their cost-effectiveness: We think we’ve got a reasonable story to tell. The difficulty is that there are lots of interventions that have got good stories to tell and you’ve got a finite pot of cash, so it’s our job to then balance this thing here which has got a reasonable story to tell, which costs X hundreds of thousands versus the next. (Interviewee 5, P1)
Using patient feedback also posed challenges. For example, it was suggested a lack of awareness among patients of the efforts to integrate their care could be seen as evidence of its (in)effectiveness: Our patient perspective is less compelling because if the MDT does its job the patient shouldn't notice any benefit … That said, we know that patients want joined-up care and we’ve had clear messages from patients in a consistent way. (Interviewee 5, P1)
In the absence of consensus around appropriate metrics for assessing the effectiveness and added value of different MDTs, interviewees highlighted softer assessments of perceived benefits. Operational managers emphasized MDTs’ contributions to improved staff communication in individual cases and in fostering a shift from a medical to a more holistic care model.
Building relationships with colleagues across organisations and learning more about their approaches to practice helped mitigate the rigidity of organisational boundaries, thereby fostering trust. MDTs enabled informal conversations that created new avenues for support and learning, contributing to success. Respondents also believed that the MDTs’ environment of trust, respect, and equality reduced staff turnover.
Moreover, MDTs’ work streamlined communication, thereby minimizing duplication, improving access to care, and enhancing home care provision. This improved patient care: We've had people who've had urinary tract infections where our nurses have been out [to the patients’ home promptly to complete an assessment.] We've asked the GP to prescribe, and then the pharmacy has delivered the prescription. And all within two hours … whereas previously they’d have been waiting for a GP to do a home visit after six o’clock in the evening. (Interviewee 1, P2)
Assigning patients just one point of contact was recognized as another benefit of having MDTs in P2a. It gave patients direct access to professionals involved in their care and ensured continuity of the relationship between the patient and the MDT. Some believed the continuity of this relationship made patients more comfortable with the process of hospital admission, discharge and follow-up care. It also meant that the patients did not need to repeat their stories to professionals they were unfamiliar with.
Discussion
This analysis in two of the 25 integrated care Pioneers demonstrates that, within and between these two sites at least, local MDTs’ initiatives varied in terms of team purposes and structures. Nevertheless, interviewees in both Pioneers identified similar challenges in developing sustainable integrated care. They particularly emphasised challenges relating to staff turnover, in turn driven by the short-term nature of development funds for integrated care (the BCF being the prime example) and the lack of shared information systems. These findings are supported by findings from our structured observations of team meetings and interviews with frontline staff, published elsewhere.14,17
System leaders valued national policy frameworks as potential enablers of integrated care, but also recognised the role of local contexts in structuring variations in the objectives and forms of integrated working. These findings also resonate with results from other studies.18,19 Specifically, research on the role of other national policy pilots in England suggests that they create local opportunities for service improvement, especially where national guidelines are sufficiently ambiguous or flexible to accommodate diverse views among local participants. 20 One implication of this is that MDTs’ care is likely to adapt to changing local contexts, as well as national guidelines.
The organisational distinctions between the two Pioneer sites and within P2, along with variations in target populations, significantly influenced decisions regarding the implementation of MDTs, resource allocation, and the establishment of structures, staffing, and objectives. For instance, the presence of three distinct models in P2 directly corresponded to the CCG’s relationships with three different social services departments, necessitating incentives for integrated collaboration within each local care system. In P2, the specific form of each model was shaped by local population needs, service gaps, and stakeholder influences within each system. In contrast, P1 implemented a largely uniform model across the entire CCG and local authority area, with some localized adaptations. Despite these structural disparities, it was evident that local system leaders in both Pioneers shared a common understanding of integrated care as being needs-centred, ensuring individuals access the ‘right care, in the right place at the right time’ through services and support in their own homes.
Geographic and structural challenges in P2 increased transaction costs for commissioners, which impacted providers. Furthermore, due to local geography and organisational footprints, the integrated NHS Acute and Community Health Services Trust faced the challenge of aligning its post-discharge services to the different models of reablement services in the two larger social services areas. This alone made implementing a single MDT model in P2 impractical. However, in P2a, a strong commitment to, and investment in, the community and voluntary sectors, creating opportunities for NHS team members to access resources beyond the statutory sector. This development, not initially part of the envisioned NHS primary care-led model, emerged as primary care leaders became more aware of the community support provided in local communities, partly due to social services' investments in community capacity.
Although we have highlighted the additional transactions costs generated in P2 by geographical and organisational complexity, the structurally less complex P1 site faced its own set of challenges. Indeed, we reported that the types of barriers to integration were broadly similar. The difference was not only that some had to be addressed three times in P2 but also that they might need to be addressed in three different ways with correspondingly greater demands on senior staff resources and capabilities.
Performance assessment posed a frequent challenge. Other evaluations of health and social care initiatives highlight the complexities involved in providing more integrated care as well as the lengthy time periods necessary to develop it.21–23 Further, as implied above, integrated care initiatives and models need to be recognised as ‘emerging from particular as well as common contexts’.23(p.1) Studying the emerging value of integrated care models is likely to be more useful than evaluating them against predetermined outcomes as the intricacies of contextual factors shaping them can have unpredictable consequences. This point is reflected in the evaluation of the North West London local integrated care initiative, which was also part of the Pioneer programme. 3 The external evaluation showed how the rigidly structured management and monitoring of care integration risked focusing attention exclusively on the milestones within the project plan and missing unforeseen changes that happened along the way, which are important in determining the overall effectiveness of large-scale changes in health and care. 24 These arguments resonate with our findings that local system leaders recognised that the challenges of successful performance assessment necessitated mixed methods and flexible data collection strategies.
It is generally accepted that evaluation of the effects of care integration brings significant methodological challenges because integrated care remains hard to define, has been developed in a variety of contexts, and its implementation has been affected by many other factors that help determine population health.25–28 Nonetheless, our interviewees identified clear benefits of integrated working, including being able to provide more holistic care, fewer instances of work duplication, speedier access to care, and enhancement of home care provision.
Limitation
The main limitation of this study is that it relies solely on documentary analysis and interviews in two Pioneer sites. This may be considered a slender base for drawing conclusions about MDTs’ variations more widely and their broader implications for integrated care delivery. Nevertheless, the two Pioneers included diverse integration contexts, spanning inner city conurbation to provincial city, smaller towns, villages, and rural areas. This broad coverage enhances the overall relevance of the analysis of working models of integrated health and social care.
Conclusion
The local leaders in both areas appeared to share a vision of integrated care in which MDTs were essential mechanisms for bringing about improvements in health and wellbeing for local populations. The teams were also reported to have improved workforce job satisfaction and stability. Local contextual variables and local understandings of these variables appeared to be the main influences on local responses to national expectations of improvements in care integration in the shape of MDTs.
Supplemental Material
Supplemental Material - The role and functions of community-based multidisciplinary teams in two integrated care and support Pioneers: Perspectives from local system leaders
Supplemental Material for The role and functions of community-based multidisciplinary teams in two integrated care and support Pioneers: Perspectives from local system leaders by Agata Pacho, Gerald Wistow, Nicholas Mays, Lavanya Thana, Lucia Rehackova, Nick Douglas, Mustafa Al-Haboubi and Mary Alison Durand in Journal of Health Services Research & Policy
Footnotes
Acknowledgments
We wish to thank all of those - patients, informal carers and staff - who participated in the MDT evaluation, and staff at the Pioneer sites who helped to facilitate its implementation. We also acknowledge the contributions of our former colleagues Ties Hoomans and Tommaso Manacorda to the development of our conceptual model of MDT functioning.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is an independent evaluation funded by the NIHR Policy Research Programme (Evaluation of the Integrated Care and Support Pioneers Programme in the context of new funding arrangements for integrated care in England (2015–2022), PR-R10-1014-25001). NIHR played no role in the conduct of the research or preparation of this manuscript. The views expressed are those of the authors and are not necessarily those of the NIHR or the Department of Health and Social Care.
Ethical statement
Data availability statement
The datasets generated and analysed during the current study are not publicly available because they contain information that would identify the research sites, individuals, and/or case-material and it would not be feasible to redact or otherwise anonymise them. The data custodian is Professor Nicholas Mays, London School of Hygiene & Tropical Medicine.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.