
Abstract
This paper introduces an evaluation of community-based, integrated health and social care multi-disciplinary teams (MDTs), primarily serving older people with long-term conditions, undertaken as part of the wider evaluation (2015-2022) of the Integrated Care and Support Pioneer Programme in England (2013-2018). To explain the context within which the MDT evaluation was undertaken, we first outline a brief history of health and social care integration policy in England, describe the Pioneer Programme and the requirements of the national ‘longer-term’ evaluation of the Pioneers. We then explain our rationale for focusing on MDTs, describe our conceptual framework of MDT functioning and provide a brief description of the evaluation design and methods, highlighting four overarching challenges we faced in undertaking it. We then briefly describe the individual papers that constitute the current supplement.
Keywords
Health and social care integration policy in England – a brief history
Many countries are seeking to better integrate different components of their health care services, as well as their health and social care services. 1 As in many other countries, the systems of health services and long-term adult social care established in 1948 in England were built on separate structures for finance, service eligibility and provision. Since then, the relationships between the two sectors, the former managed hierarchically from central government and the latter administered through elected local government, have been recurrent policy concerns.
Concerted efforts to improve coordination between the universal, largely free at the point of use National Health Service (NHS), funded from general taxation, and local social care services which are means-tested and funded from a mix of general and local taxation together with user payments, began during the 1970s, based on forms of collaboration or partnership. Since the 1974 re-organisation of the NHS, there has been a long procession of initiatives to promote integrated working through statutory requirements, financial incentives, formal planning arrangements and service delivery based on multi-disciplinary teamwork. 2 Common approaches employed since 1974 have included: shared geographical boundaries for NHS and local government; financial incentives and pooled budgets; local statutory forums designed to coordinate planning and commissioning by individual agencies; and pilot projects designed to identify and spread good practice. 3
Stokes et al 4 identified a set of meso-level interventions designed to facilitate integrated service delivery at the patient level, most commonly in the shape of multi-disciplinary teams (MDTs) in the community. Community-based MDTs in England are typically established to provide more integrated or holistic care for patients than would otherwise be the case, and aim to encourage inter-professional collaboration and care coordination. They are often based around general practitioner (GP) practices. They bring together professionals and other staff from the primary, community and acute health care sectors, adult social services, and the local community and voluntary sector to co-ordinate care for, and, in some cases, provide care directly to patients and their informal carers. They encourage their members to exchange information about caseload patients (e.g. health status and wellbeing, concerns about social, family and other issues, etc.), share ideas, and make decisions on how best to intervene and deliver appropriate services, with the aim of preventing and reducing patients’ health and care problems, unnecessary GP consultations, hospital and nursing home admissions, and premature deaths.
These meso-level approaches focus on building links between formally separate organisations with distinct statutory accountabilities to avoid political controversies that would result from more radical proposals such as either the NHS taking over adult social services from local government or the NHS becoming the responsibility of local government. This political context has, so far, limited the extent to which health and social care service commissioning (planning) and delivery can be integrated around individuals whose needs frequently transcend organizational and professional boundaries.
Integrated care pilots to identify and spread good practice rose to prominence in the 2000s with a series of nationally initiated and locally crafted programmes. These were: Partnership for Older People Projects (2005); Integrated Care Pilots (2009); Integrated Care and Support Pioneers (2013); the Better Care Fund (2014); Care Act (2014); NHS Five Year Forward View (2014); New Models of Care (Vanguards) Programme (2015); Integrated Personal Commissioning Pilots (2015); Sustainability and Transformation Plans/Partnerships (2015); Primary Care Home Model (2015); Devolution of responsibility for health care funding and commissioning (Devo Manc) (2015); Accountable Care Systems (2017); and the NHS Long Term Plan (2019). This series gradually led to the emergence of Integrated Care Systems and Partnerships. This culminated in legislation in the 2022 Health and Care Act which placed 42 Integrated Care Systems on a statutory basis. 5 Each has an Integrated Care Board responsible for planning and aligning all the health and care services in geographical areas with populations of 500,000 to three million.
The intervals between each of the pilots shortened over time and, increasingly, one was overtaken by a successor even before the earlier programme had run its full course, possibly because of the impact of the severe restriction of public spending (known as ‘austerity’), which began in 2010 in the aftermath of the financial crisis of 2007-08 and continued throughout the period. Austerity created a so-called ‘integration paradox’ - that is, an environment in which the need for better coordination and joint working between the NHS and long-term care sector grew just as budget constraints encouraged individual agencies and services to place tighter limits around their roles and responsibilities to maintain financial viability, thereby preventing sought for cross-organisational working. 6
Government enthusiasm for these initiatives remained despite the largely pessimistic assessments of integrated care progress and prospects in the period. For example, early in the Coalition Government of 2010-15, the Commons Health Select Committee concluded that ‘little by way of integration has been achieved over [a] 40 year period’. 7 The then Coalition’s re-launch of integration starting in 2010 fared no better with the National Audit Office concluding in 2017 that ‘nearly 20 years of initiatives to join up health and social care by successive governments has not led to system-wide integrated services’. 8 Rigorous academic evaluations of previous initiatives had not shown reduced costs or fewer emergency hospital admissions.9–11 Stokes et al 12 reviewed the research evidence on horizontal integration between health services and social services (including long-term care) available around the time that the Pioneer programme was announced (see below) and concluded that there was no conclusive evidence of integrated services or joint working (including MDTs) improving organisational, clinical or efficiency-related outcomes, but that they could lead to improved patient and carer experiences.
Such evidence indicated that the hope that care integration - including more care outside hospital, closer to where people live - would help people manage their multiple long-term conditions better and at lower cost largely remained out of reach. One possible explanation for this was the tendency for integrated care initiatives to be small-scale and unsupported by wider systemic changes. However, it was acknowledged that systemic change (e.g. integration of the governance and management of health and social services organisations) would have to overcome substantial political, legal and organisational obstacles. 12 Another possible reason for the lack of success were the austerity-related cuts previously mentioned. These particularly affected the funding of local government, including its social care budgets, which reduced the number of individuals that could be supported, either to prevent hospital admissions or to allow patients to be rapidly discharged after a hospital stay. (The term ‘patient’ is used in this paper and in the remainder of the supplement to include social services’ users and NHS patients).
This view does not mean that no progress was made to wrap health and care more effectively and efficiently around the needs of individuals and families. However, the clearest and best documented progress tended to be confined to local centres of excellence, such as Torbay in the 2000s. 13 Such progress has rarely been spread or sustained. This is the environment in which the Pioneer programme operated.
Integrated Care and Support Pioneer Programme (2013-2018)
The Integrated Care and Support Pioneers were 25 volunteer local health and care geographic sites that were selected through open competition in two waves by the then Department of Health (DH). Chosen from over 100 applicants, Wave 1 consisted of 14 sites announced in November 2013, with the second wave of 11 areas announced in January 2015. The programme had a five-year official lifespan. The successful sites were intended to be those judged to be the most advanced areas of the country in terms of having the potential to move NHS and adult social services towards a deeper and more effective form of horizontal coordination between services in the community, and thus better local delivery of health and social care services. They were expected to involve health, social care, public health, other public services (e.g. housing) and the voluntary sector. 14
The DH had called for the ‘most ambitious and visionary’ local areas to become integration Pioneers to drive change ‘at scale and pace, from which the rest of the country can benefit’ 14 and applicant sites had to demonstrate that they could satisfy six criteria, covering: an ability to articulate a vision of its innovative approaches to integrated care; a plan for whole system integration; a commitment to integration across the range of relevant local stakeholders; the capability and expertise to successfully deliver a transformation project at scale and pace; a commitment to share lessons across the sector; and an ability to demonstrate that its vision and approach was, and would continue to be, based on a ‘robust understanding of the evidence’. 14 The programme was based on the principles set out in Integrated care and support: our shared commitment 15 in which the DH and 12 national patient and service user partner organisations committed to ‘urgent and sustained action(p6)’ with the ambition of making integrated care and support ‘the norm’(p8) by 2018. The definition of integrated care which the programme was to pursue was: ‘I can plan my care with people who work together to understand me and my carer(s), allow me control, and bring together services to achieve the outcomes important to me’. 16 The plans and work of the Pioneers were intended to be inspired and guided by a series of ‘I-statements’ (e.g. I tell my story only once. I am always kept informed about what the next steps will be. The professionals involved with my care talk to each other. We all work as a team) crafted by the National Collaboration for Care and Support, 15 which consisted of NHS and patient organisations, including National Voices, a coalition of health and social care charities.
Despite the high level of national engagement across a wide range of organisations that had generated the concept of a ‘pioneer’ programme and the vision for integration embodied by the ‘I-statements’, what the Pioneers were required to do to produce more integrated care and support was left largely to each local Pioneer in its bid document. The Pioneer programme was therefore substantially shaped by the local history of integration and, to a large degree, by integration aims, plans, initiatives, and anticipated system level outcomes (e.g. reduced hospitalisation rates) of improved integration already in place locally prior to sites becoming part of the programme. The programme was not organised around testing one or more defined, innovative ‘interventions’ prescribed by the DH to integrate the health and care system.
Each Pioneer area was to be given access to expertise, support and constructive challenge from a range of experts (e.g. from NHS Improving Quality, the Local Government Association, the Leadership Academy and Public Health England). However, unlike the pilot programme that followed and overlapped, the New Care Model Vanguards, the Pioneers received no additional funding for service delivery or local evaluation and only a very modest UK£90,000 to pay for an inception-phase project manager. Each was supported by an account manager from NHS England who had responsibility for a group of Pioneers, and had access to an online information-sharing platform and regular Pioneer conferences.
The Pioneers represented a diverse range of urban, rural, deprived and affluent areas across England, and comprised 83 local authorities (LAs) and 66 NHS clinical commissioning groups (CCGs) in 25 sites, amounting to 25% of all LAs and 31% of CCGs, and covering 30% of the English population.
Longer-term Pioneer evaluation (2015-2022)
Following a largely qualitative ‘early’ evaluation of the first 14 Pioneers,6,17 we undertook the longer-term evaluation of all 25 sites comprising three so-called work packages (WPs). It aimed to assess the extent to which the Pioneers were successful in providing ‘person-centred coordinated care’, including improved outcomes and quality of care, in a cost-effective way, and to identify what worked best in delivering quality integrated care in different contexts. WP1 (Process and (limited) impact evaluation of all Pioneers) aimed to: understand service changes and the experiences of those in Pioneers; identify facilitators and barriers to integrating services and how such barriers are overcome; and examine changes in key indicators of the extent of care coordination and its consequences at Pioneer level compared with non-Pioneers. The Pioneer level findings have been published elsewhere.18–21 WP2 (Mixed method economic and impact evaluation of specific integration initiatives in a sub-set of Pioneers) aimed to: conduct impact and economic evaluations of systemically important integration initiatives undertaken by Pioneers by relating the resources used to the benefits for patients in terms of user experience, and health and/or social care-related quality of life; and understand how and why these initiatives’ impacts were affected by different contexts, through an integral qualitative component in each cost-effectiveness analysis. The aims of WP3 (Working with sites and policy makers to test findings and conclusions from the evaluation, and disseminate learning from the evaluation to stakeholders) were: firstly, to synthesize the emerging findings from WPs 1 and 2 to assess the extent to which the performance of integration initiatives (WP2) could be related to the approach taken at a higher level by the host Pioneer (WP1) and the contribution of individual initiatives to the overall performance of the Pioneer; and, secondly, to derive and spread practical insights from the evaluation as a whole, and encourage reflection and learning among Pioneers, policy makers and others.
The then DH’s 22 Invitation to Tender for the evaluation specified that: (1) the successful research team would assess the impact of the Pioneer programme on ‘users’ and carers’ experience and outcomes, on the overall quality of care and support, on the care provider market, and on the wider health and care system’; 22 (p13) (2) the programme and its constituent initiatives should be subject to outcome and cost-effectiveness evaluation, using comparative or controlled research designs; and (3) the research team would work closely with DH in the early stages of the longer term evaluation, and build on the previous early evaluation’s findings, 6 to scope methodological challenges and assess the feasibility of delivering a ‘robust’ outcomes and cost-effectiveness evaluation. The DH acknowledged that delivering this scale and scope of evaluation would be challenging.
The current authors were part of a team that bid for this evaluation work. In our bid, we argued that it was not feasible or meaningful to undertake cost-effectiveness analysis at Pioneer level, given the range and mix of integration initiatives 6 being undertaken across the individual Pioneers. Instead, we proposed conducting cost-effectiveness analyses, with integral qualitative research, of specific integration initiatives targeted by Pioneers at sub-areas and/or population sub-groups, setting out the aims of WP2 as described above. Another important consideration we identified was the extent to which we could evaluate the same or similar interventions across a number of Pioneers to produce generalisable learning. It was also clear to us that there was no support for randomised controlled trials of Pioneer initiatives, and that some form of quasi-experimental design would be required. Our bid was ultimately successful.
Choosing initiatives to evaluate in depth
As described in Durand et al 23 we needed to identify interventions which could be clearly and consistently defined, were of sufficient strategic and systemic significance for health and social care integration and could feasibly be studied using a comparative design involving a matched group of patients not receiving the intervention. As Pioneers were expected to develop ‘person-centred coordinated care’ encompassing local health services, social care, public health, other public services (e.g. housing) and the voluntary sector, 14 we were specifically interested in integration interventions that involved both health and LA adult social care staff. Based on Erens et al 6 and later scoping for the evaluation, a number of potentially discrete integration activities - including community-based MDTs, integrated hospital discharge schemes and new integrating roles (e.g. care navigators) - were considered. Though not unique to the Pioneers, all could be considered strategically important integration activities in the English health and care system.
Community-based MDTs, involving both health and adult social services staff, were chosen ahead of the others for several reasons. First, as in other integration pilot programmes, 20 and consistent with the definition of integration as ‘person-centred coordinated care’, they were, and remained, one of the Pioneers’ most widely reported integration initiatives.6,24 Second, their caseloads often included older people with multiple chronic conditions, a population prioritised by most Pioneers. 6 Third, they brought together professionals from a range of different services, organisations and sectors. Fourth, the scoping work suggested that there might be geographical areas within individual Pioneers which were not covered by MDTs, allowing for the possibility of recruiting matched patients not exposed to MDT care. Finally, as MDTs were likely to differ from one another in some respects, operationally and/or structurally, this suggested scope for comparisons of outcomes not only between MDT and comparator patients but also potentially between different MDT models, subject to statistical power.
Research on the effectiveness of community-based MDTs for either specific (e.g. lung cancer) or more general conditions (e.g. frailty in older people) presents a mixed picture regarding their impacts on outcomes and service delivery.25–31 Stokes et al 12 argue that the case management approach employed by MDTs is a poor option ‘for achieving significant cost reduction.’(p283) However, there is a paucity of economic evaluation of MDTs, and limited research on MDTs incorporating both health and social care professionals, despite some studies suggesting that involving social workers in health care provision can have positive effects on health outcomes and reduce costs.32,33
Our evaluation aimed to be very ambitious in its scope, to provide stronger evidence regarding the costs and benefits of providing integrated or patient-centred care through MDTs than previous studies. By employing a mixed-method, quasi-experimental design, we aimed to be able quantitatively to assess the impact of MDT care on patient experience and health-related outcomes, service use and costs. Qualitative methods would enable an in-depth understanding of patient, informal carer and staff experience, and the exploration of contextual differences between Pioneers and their MDTs, which might explain any observed differences in quantitative outcomes. Furthermore, evaluating MDTs would allow us to explore the interplay of a range of stakeholders (organisations, services, individuals) operating at different levels (macro, meso, and micro) within complex local health and care systems to produce and deliver care that is experienced as patient-centred, against the backdrop of national policy imperatives on integrated care. Care integration involves not only the actions of managerial staff in local strategic organisations (e.g. CCGs and LAs) and frontline staff who organize and/or deliver care, but also patients and their informal carers, who are arguably best placed to define what ‘integrated care’ should look like in practice, and how it should be delivered. Thus, by including a wide range of participants, we planned to give a voice to key actors at all levels of the system. This is relatively unusual in studies of care integration to date.
Conceptual framework of community-based MDT functioning
We developed a conceptual framework of community-based MDT functioning (see Figure 1) to underpin the evaluation by focusing and organising the data collected. A rapid review of theories and studies of multi-disciplinary team working in the UK was undertaken. While much of the literature reviewed related to health care settings (e.g. hospitals) where teams did not include social care staff34–37 a study by Raine et al,
38
which examined features of team functioning in the treatment of chronic disease, did. Review findings, combined with Pioneer logic models developed in the early evaluation of the programme based on their integration plans,
6
formed the basis for the framework. The framework provided an overview of the dimensions to be examined in the study, to enable the research team to explore the causal pathways between a dimension and the relevant outcome, and to help us understand the impact of different contexts, MDT operating models and other factors on outcomes in participating Pioneers. The framework was structured as a classic input–process–outcome model, which sees the MDT as an intervention. Our examination of the literature suggested that the ‘intervention process’ box (see Figure 1) could be sub-divided into input, process and output factors related to team functioning. Conceptual framework of community-based MDT functioning, derived from Douglas et al.
45
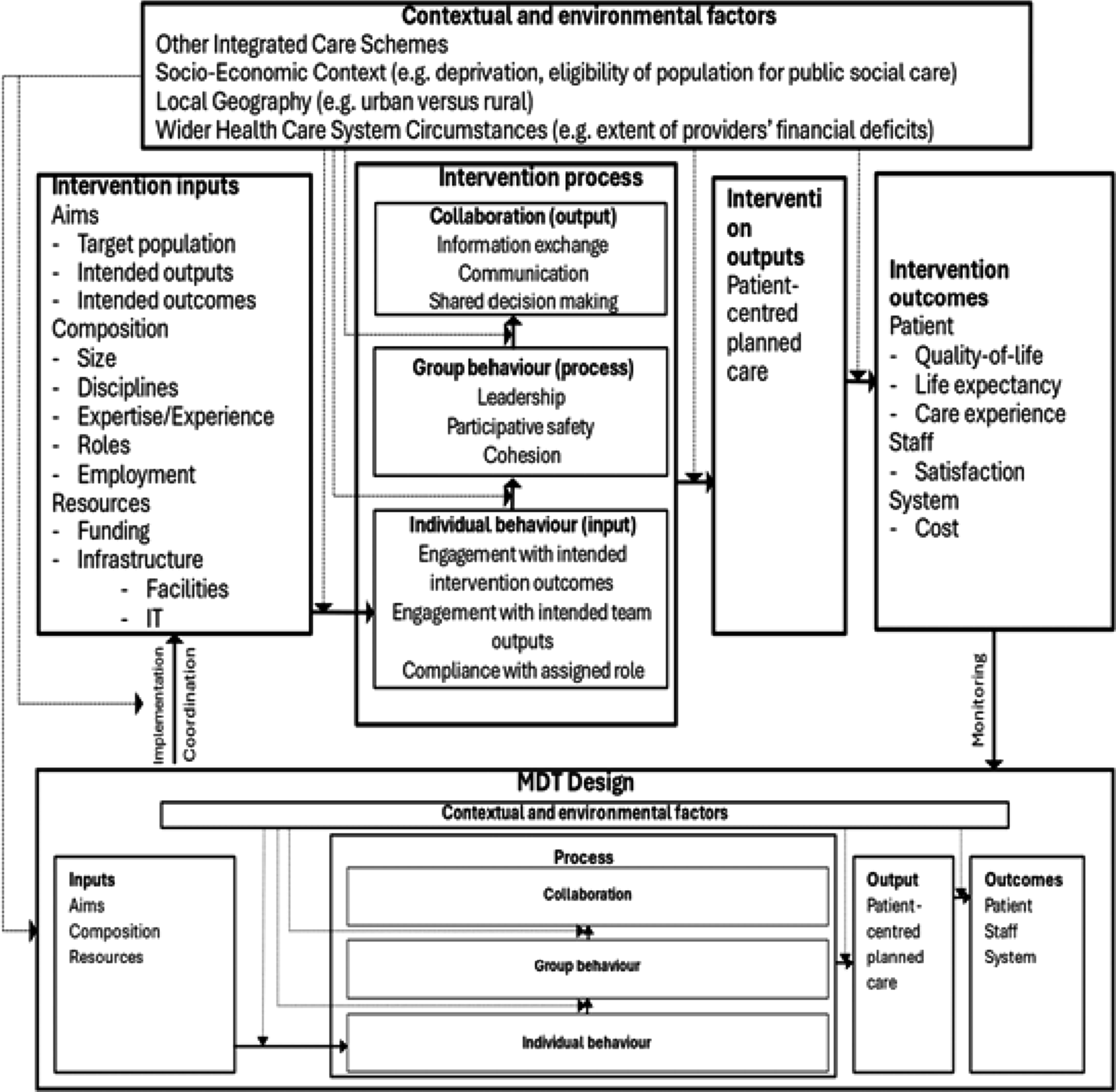
We envisaged that employing a range of different research methods should allow us to explore: • Contextual and environmental factors, including integrated care schemes existing in the area, social deprivation and eligibility for social care of the target population, geography, political and economic circumstances, etc.; • Intervention inputs, including MDT design and evolution; • Intervention processes, including aspects of team functioning associated with collaboration and group/individual behaviours; • Intervention outputs; • Intervention outcomes – including self-reported outcomes for MDT staff (e.g. professional satisfaction), intended and perceived outcomes for patients/service users according to MDT members’ perspectives, as well as self-reported outcomes (e.g. from patient survey and interview data).
In practical terms, we employed the framework to guide our selection of outcome measures (e.g. patient self-reported quality of life), and the development of survey questionnaires and interview topic guides. We also used it as the basis for the non-participant observations of MDT meetings.
MDT study design and methods
For the purposes of the evaluation, a community-based MDT was defined as: including both health and social care professionals, and in some instances, the voluntary and community sector; bringing these professionals together in a shared process of care coordination; and having a caseload that included people aged 55 and over with multiple chronic conditions living in their own homes (i.e., those whom evidence suggests often need complex care coordination and high levels of health and social care resources).39,40
We designed a multi-method, prospective, quasi-experimental impact and economic evaluation of community-based MDTs. The evaluation included: postal surveys of patients and their informal carers, if nominated, designed to measure health status and quality of life; qualitative interviews with sub-samples of both groups
41
; qualitative interviews with local strategic managers involved in integration activity
42
and frontline MDT staff
43
; an MDT staff online survey
44
; and MDT meeting observations.
45
In addition, we planned to obtain (with patient consent) individual level, pseudonymised, routine service use data (hospital, general practice and social care services) to link to our primary questionnaire data. A detailed description of the planned design and methods is provided in Durand et al.
23
That article details the four major, overarching challenges experienced in undertaking the evaluation: (1) commissioner/funder research specification; (2) negotiating with, and recruiting, research sites where the participation of multiple organisations/ services is required; (3) navigating research ethics and governance approvals’ systems; and (4) recruiting MDT and matched non-MDT patients and obtaining their routine service use data).
That paper also gives the steps we took to try to mitigate those four challenges, and the practical impacts they had, including on our ability to recruit a matched control group of patients, and the type and amount of data we were able to collect. The COVID-19 pandemic’s impacts on the evaluation are also outlined. 23 In the event, we were unable to carry out the carefully planned quasi-experimental impact and economic evaluation. We report what we were able to achieve in this supplement.
Participating Pioneers and their MDTs
As described in more detail elsewhere,23,42,45 11 MDTs in two contrasting Pioneers, covering four different MDT operational models, were recruited to the MDT evaluation. Pioneer 1 (P1) was located in a unitary authority in an inner-city, and involved eight MDTs coordinated by NHS administrators, all operating to one model organised around general practices. Pioneer 2 (P2), in a mixed urban-rural area, had three MDTs operating to different models - two general practice-based and one led by an NHS acute hospital trust. P2 encompassed one CCG, one LA in its entirety and parts of two other LAs.
In both Pioneers, the MDTs’ aims included supporting those discharged from hospital and preventing hospital admissions.42,43 While targeting older people, P1’s MDTs also responded to some younger adults with complex needs, and played a largely care-coordinating role, with a focus on supporting GPs. P2’s MDTs focused more specifically on older people, and, as well as co-ordinating and planning care, were also involved in providing direct support to those on their caseloads. In both Pioneers, patients and their informal carers did not attend MDT meetings. The recruitment of contrasting Pioneers and a range of MDT models enabled us to explore how different contextual and MDT-specific characteristics impact MDT functioning and perceived performance (e.g. outputs and impacts on staff and patients), as outlined in the conceptual framework above.
Contents of the supplement
The remainder of this supplement sets out the findings of the extensive qualitative research that it was possible to carry out on two Pioneers’ MDTs.
Durand et al 23 (Evaluating health and social care integration in England’s Pioneer programme: the challenges of undertaking research in service delivery and research regulatory systems that are not fit for purpose) describes the four overarching challenges encountered in undertaking the MDT evaluation and the adaptations that we had to make to the study design and methods. It also outlines lessons for research commissioners and funders, national and local research governance and ethics bodies, policy makers and researchers.
Pacho et al 42 (The role and functions of community-based multi-disciplinary teams in two Integrated Care and Support Pioneers: perspectives from local system leaders) focuses on the role and tasks of the MDTs in the two participating Pioneers, as viewed by local strategic health and care leaders. It covers how the MDTs originated and what their principal objectives were; how they were structured, staffed and resourced; what functions they performed and how they related to the wider care system; stakeholder views on what MDT success would look like; and the evidence being collected locally about MDT performance.
Thana et al 43 (Frontline staff perspectives on multi-disciplinary team working and the effectiveness of integrated service delivery: findings from the Evaluation of the Integrated Care and Support Pioneers in England) presents findings from semi-structured interviews with frontline integrated care MDT staff. Perspectives on the evolution of the original MDT aims, the constitution of teams, the meaning of ‘team’ and individual professional identities within the context of wider networks, the business of meetings, and barriers and facilitators to MDT working, as well as the benefits for both patients and staff are explored.
Durand et al 41 (The views of older patients on community-based multi-disciplinary team caseloads and informal carers about health and care services in two Integrated Care Pioneer sites in England) reports the findings of qualitative interviews with MDT caseload patients and informal carers about their views of health and care services, including perspectives on whether their needs were being met in a way that allowed them to live as they would wish, and how co-ordinated their care was. After the start of the COVID-19 pandemic, interviewees’ views about its impact on their health, care and support needs, and on service delivery were also explored.
Rehackova et al 46 (The impact and legacy of COVID-19 on community-based multi-disciplinary teams organising integrated health and social care for older people with long-term conditions: findings from the Evaluation of the Integrated Care and Support Pioneers in England) reports on the perspectives of strategic leaders, operational and frontline MDT staff. It considers how the MDTs in the two Pioneers had responded to the pandemic; strategic and frontline staff’s views of their roles and professional relationships within MDTs currently and in the future and how they might organise themselves to coordinate and deliver care post-pandemic; and the potential longer-term impacts of the pandemic on the local health and care systems in which the MDTs function.
Durand et al 47 (Evaluating the role of community-based multi-disciplinary teams in integrated health and social care in England: overview of findings from the Pioneer evaluation and their implications for health and social care integration) brings together and compares findings from the individual papers, as well as considering the implications of those findings for our conceptual framework of MDT functioning (Figure 1). It draws out general implications for the continuing development of the role and operation of community-based MDTs, and for policy and research on health and social care integration more broadly.
Footnotes
Acknowledgments
We wish to thank all of those - patients, informal carers and staff - who participated in the MDT evaluation, and staff at the Pioneer sites who helped to facilitate its implementation. We also acknowledge the contributions of our former colleagues Nick Douglas, Ties Hoomans and Tommaso Manacorda to the development of our conceptual framework of MDT functioning.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is an independent evaluation funded by the NIHR Policy Research Programme (Evaluation of the Integrated Care and Support Pioneers Programme in the context of new funding arrangements for integrated care in England (2015–2022), PR-R10 -1014–25001). NIHR played no role in the conduct of the research or preparation of this manuscript. The views expressed are those of the authors and are not necessarily those of the NIHR or the Department of Health and Social Care.
Ethical statement
Data availability statement
The datasets generated and analysed during the current study are not publicly available because they contain information that would identify the research sites, individuals, and/or case-material and it would not be feasible to redact or otherwise anonymise them. The data custodian is Professor Nicholas Mays, London School of Hygiene & Tropical Medicine.