
Abstract
Objective
English general practices have been facing ongoing pressures, arising from complicated health care needs and the recent pandemic. To overcome these pressures and reduce the workload of general practitioners, there have been extensive attempts to integrate pharmacists into general practices. A number of literature reviews, often systematic, have partially explored the topic of general practice-based pharmacists (GPBPs) internationally. Our aim was to further explore the employment/integration models of GPBPs and their actual activities and impact, concepts that have not been thoroughly investigated by previous reviews.
Methods
Two databases were searched from inception to June 2021 for studies published in the English language. Results were independently screened by two reviewers to establish eligibility for inclusion. Original research studies, or protocols where results had not been released at the time of search, that reported on services provided by pharmacists with some sort of integration into general practices were included. The studies were analysed using narrative synthesis.
Results
Searches identified 3206 studies in total, of which 75 met the inclusion criteria. The included studies were highly heterogeneous in terms of participants involved and methodologies employed. Integration of pharmacists into general practices has occurred in several countries, with funds originating from multiple sources. Several employment models for GPBPs were described – for example, part-time and full-time work and/or coverage of multiple or single practices. GPBP activities, with some exceptions, were comparable between different countries, with medication reviews being the most common task globally. GPBP impact was identified through both observational and/or interventional research methods, by pursuing a large variety of measures (e.g. activity volume, contact with patients, perceptions/experiences, and patient outcomes). Independent, quantifiable outcomes from GPBP activities were all positive but were of varying statistical significance.
Conclusions
Our findings suggest that GPBP services can lead to positive, quantifiable outcomes, mainly in relation to medication use. This shows the usefulness of GPBP services. The findings of this review can help policy makers decide how best to implement and fund GPBP services, and how to identify and measure GPBP impact.
Introduction
English general practices (known as ‘family practices’ in some countries) have been under significant workload pressures stemming from an ageing population with complicated health care needs. 1 The recent pandemic further added to general practice workloads by generating extra tasks, including aiding the recovery of people physically or mentally affected by the pandemic, supporting patients on waiting lists for health care services, and contributing to the vaccination programme. 2 In response to unmanageable workloads, general practitioners (GPs) are increasingly retiring early or switching to part-time employment patterns.3,4 As a result, there have been persistent shortfalls in the numbers of GPs.3,5
To tackle the workforce and workload pressures in general practices, there has been an extensive drive (begun in 2015) to integrate pharmacists into general practices. As part of a recent initiative to merge general practices in primary care networks, National Health Service England has endeavoured to fully sponsor the employment costs for hiring approximately 26,000 primary care staff by 2023/24 including additional general practice-based pharmacists (GPBPs).6,7 Primary care networks are collaborative structures linking primary care with hospital, social, and voluntary services, serving 30,000 to 50,000 people. It is anticipated that each of the approximately 1250 primary care networks will have about six pharmacists by 2023/24, thus elevating the population of GPBPs in England to about 7500. 8 Similar to England, extensive attempts to integrate pharmacists into general practices have taken place in Scotland, Wales, and Northern Ireland.9,10,11
Formal integration of pharmacists into general practices is a relatively new concept in England. To demonstrate the value pharmacists add to the general practice setting and thereby justify their inclusion amongst the primary care team, National Health Service England has proposed a number of approaches over the years. These have included numerical and survey-based key performance indicators (i.e. quantifiable measures to track the progress of services or organisations in relation to process or outcomes), electronic activity codes to capture pharmacist activities, and non-pharmacist-specific measures relating to structured medication reviews, care in nursing homes, and cancer detection.12,13,14 Pursuing these impact identification plans, however, has been complicated by variations in pharmacist roles. There have been reports of GPBPs being resistant to the changes, dissatisfied with the available central measures (i.e. they regard the central measures as inappropriate for capturing GPBP impact), as well as inconsistencies in how pharmacist impact is ultimately identified between different practices.15,16,17
A number of systematic and non-systematic literature reviews have explored, to a certain extent, the topic of GPBPs around the globe. The reviews by Tan et al., Hazen et al., Anderson et al., Hayhoe et al., Ibrahim et al., Alshehri et al., and Khaira et al.18,19,20,21,22,23,24 collated outcomes from GPBP activities. The reviews by Benson et al., 25 as well as, to a lesser extent, those by Ibrahim et al. and Khaira et al.,22,24 investigated the types of activities carried out by GPBPs. One umbrella review 26 also looked at existing systematic reviews, some of which reported on pharmacist services in primary care settings in general, rather than general practices specifically.
But none of these reviews described the different efforts of integrating pharmacists into general practices internationally or the methods used for identifying and measuring their impact. Moreover, although some of the reviews mentioned above considered the outcomes of GPBP activities, the described outcomes were not based solely on independent measures. Objective, independent measures might translate to different findings from those approaches that are subjective or self-reported for a given research topic/phenomenon.27,28 Further, some of the previous reviews related to GPBP services for specific conditions and/or certain patient populations only,22,23 or to GPBP services in very restricted geographical areas. 24 In addition, the identified range of GPBP activities (in the review by Benson et al. 25 ) also included student activity and potential roles, rather than focusing only on existing pharmacist services taking place in reality.
Thus, the overall aim of this rapid review was to shed more light on existing integration and employment models, actual roles, and impact of GPBPs. The specific questions this review set out to answer were as follows: • What attempts have been made internationally to integrate pharmacists into general practice? • What is the range of activities carried out by GPBPs? • What methods have been used to identify the impact of GPBPs on practices and patients? • What are the independent, quantifiable outcomes from GPBP activities discovered as part of impact identification methods?
Methods
A rapid review is defined as ‘a form of knowledge synthesis that accelerates the process of conducting a traditional systematic review through streamlining or omitting a variety of methods to produce evidence in a resource-efficient manner’.29(p80) We therefore selected this rapid review approach to produce timely results and inform the current implementation of GPBP services in the UK and overseas.
This study was carried out in accordance with the guidance for rapid reviews produced by the Cochrane Rapid Reviews Methods Group. 30 This consists of 26 recommendations, in relation to designing, conducting, and writing up rapid reviews, as informed by a scoping review and extensive consultations with representatives from Cochrane entities. The objectives of and criteria for this review were developed collaboratively by GDK and NP, with the rest of the authors having input in reviewing decisions made and proof reading.
Search strategy
To identify studies eligible for answering the objectives of this review, two databases (PubMed and Web of Science) were searched. The performed searches covered the period from inception of the databases until 11 June 2021. Search strategies were developed in collaboration with a subject librarian and involved the use of certain keywords, including ‘pharmacist’, ‘pharmacists’, ‘general practice’, and ‘family practice’. All search terms were combined by employing the Boolean operators ‘AND’ and ‘OR’ as appropriate. The precise search strategies are described in S1 in the online supplement. Reference lists of the included studies were also searched for additional relevant studies.
Selection of studies
Study types
Any study reporting on original research, with a formal data collection method but regardless of the study design, was deemed eligible for inclusion in this review. We also included protocols for research studies in cases where results of the actual studies had not been released at the time of the search. All studies must have been published in peer-reviewed journals, written in the English language, and could have originated from any country across the globe. Letters to the editor, editorials, commentaries, experiences, special features, reports, research briefs, and systematic or any other type of literature review were excluded.
Participant types
There were no restrictions to the type of participants considered for this review. As such, to be included, studies could have involved any type of stakeholders in the implementation of GPBP services, such as patients, various health care professionals, and managerial or administration staff. There were no limits in relation to the kind of diseases patient participants experienced and/or GPBP participants dealt with.
Service types
We employed the definition of ‘integration’ by Shaw and Couzos. They described ‘integration’ as ‘any intervention that involved co-location of pharmacists within PHC [primary health care] settings and/or pharmacists who worked as part of multidisciplinary and/or interdisciplinary healthcare teams using a range of integrative processes’.26(p404)
Therefore, to be included in this review, studies must have involved the provision of pharmacist services in a community-based, general practice or family practice or primary care clinic setting. The actual tasks could have been undertaken either within the practice or remotely (e.g. patient homes or nursing homes or research sites). In any case, services should have been provided by pharmacists with some sort of integration into general practice but regardless of employment model.
We excluded studies describing the activity of student pharmacists in general practice or those examining the potential, rather than existing, activities and roles for GPBPs. We also excluded studies concerning pharmacist activity within community pharmacies, various types of clinics (e.g. memory clinics, occupational health clinics, and ambulatory care clinics – hospital-based services offering same day care to patients), outpatient settings that apart from primary care services also provided specialist care, and family medicine residency programmes. Finally, we excluded pharmacist-led educational projects and technological tools or manufacturer initiatives in general practice, as well as jointly delivered interventions (e.g. clinics carried out by GPBPs and nurses).
Outcome types
This review synthesised all methods that had been employed, by the time of our searches, to identify pharmacist impact in general practice. However, the specific outcomes discovered as part of these impact identification methods had to be based on independent, quantifiable measures. Outcomes of GPBP activities based on stakeholder opinions, including patient self-reporting or assumptions (e.g. cost savings computed to longer period of times than what was actually measured), were not presented in this review. The quantity of GPBP activities or interventions or patient encounters, including the duration of GPBP activities or encounters, was also not viewed as outcomes to present in this review.
Screening process
The title and abstract of all identified studies were screened by one reviewer (GDK) and studies that were outside the topic of GPBPs were excluded. All remaining, potentially relevant, studies were extracted to a reference management software. After removing duplicates, full texts were retrieved and independently read by two reviewers (GDK and NP) to establish whether inclusion criteria were met. GDK read all full-texts, whereas NP read a random sample of 50% of the full-texts. Both reviewers met regularly to discuss their findings and resolve any disagreements that arose. A list of studies fully satisfying the criteria was mutually agreed amongst the two reviewers.
Data extraction and synthesis
GDK independently extracted data from all included studies (see S2 in the online supplement). Details extracted included the study type and aim, the study population, information on the programmes of implementing GPBP services, the activities of GPBPs, the methods used for identifying GPBP impact, and key findings relevant to the objectives of this review. NP screened all extracted information, and its consistency and presentation were refined through discussions between GDK and NP.
No quality assessments for risk of biases were performed, as our purpose was to capture the broader picture in terms of integrating pharmacists into general practices globally rather than simply synthesising a narrow body of high-quality literature. In other words, as the primary purpose of this review was to synthesise the characteristics of GPBP models in relation to employment and impact identification, evaluating details about these models as being ‘present’ or ‘not present’ did not require any quality assessment techniques.
Data extracted from the included studies mainly consisted of descriptive information. The presence of descriptive elements, along with the fact that outcomes to be presented were heterogenic, meant that any meta-analyses could not be performed. We therefore selected a narrative synthesis approach to organise and present the extracted data. Narrative synthesis allowed us to ‘go beyond the act of simply describing and summarising the main features of included studies…enabling investigation of similarities and differences between studies, and exploration of relationships within the data’.31(p201)
Results
Selection of studies
The original search resulted in 3206 studies in total. After screening titles and abstracts and removing duplicates, 295 studies were deemed potentially relevant. Full-texts were retrieved and read for all 295 studies. Seventy-five studies were regarded as eligible and included in this review. Figure 1 provides a detailed overview of the study selection process, including the precise reasons behind the exclusion of full-texts. Flow diagram outlining the selection process of studies for the rapid review.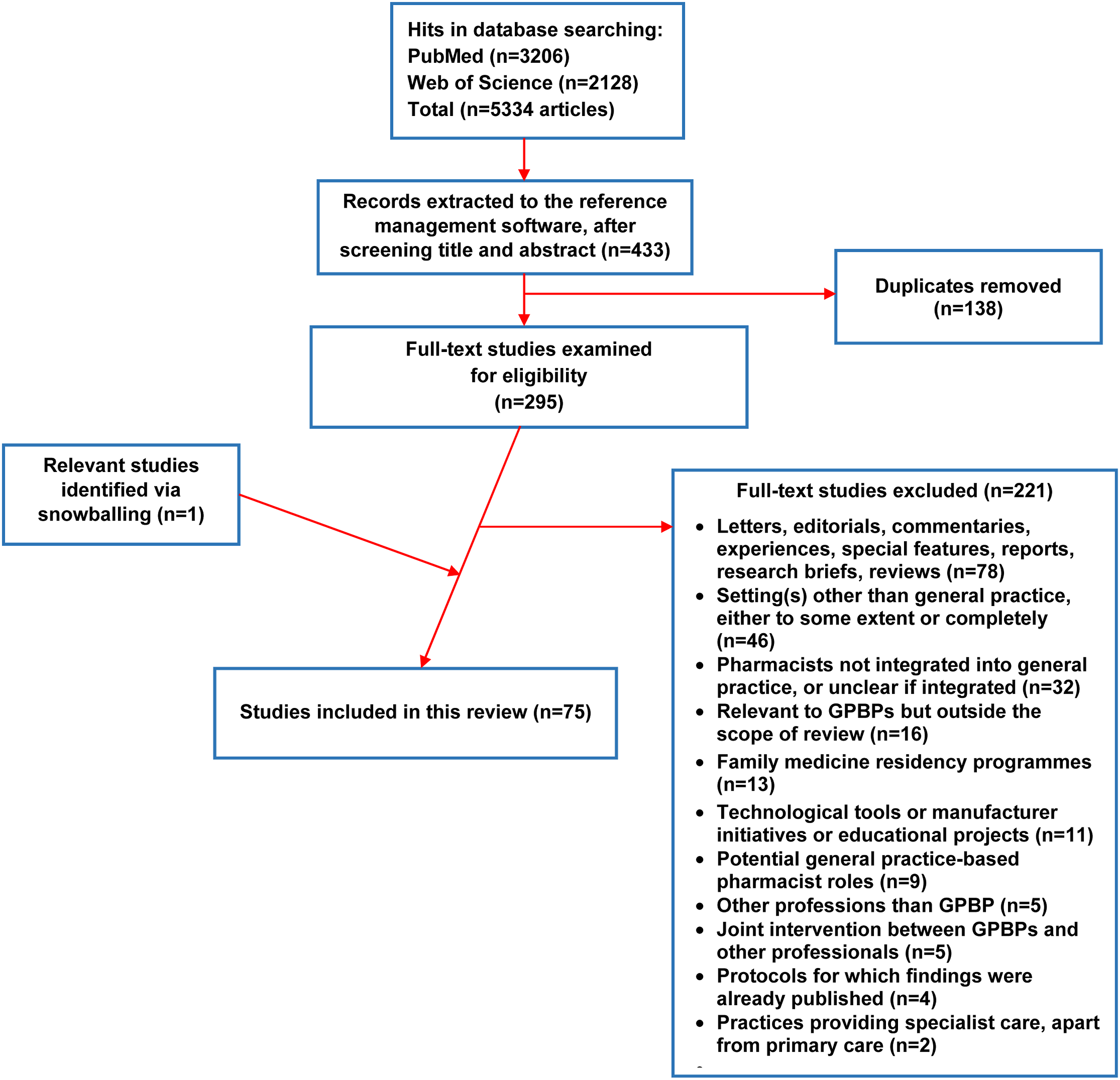
All included studies are summarised in S2 in the online supplement. The reference numbers in brackets below refer to the enumeration of the included studies as listed in S2 in the online supplement.
Characteristics of included studies
Of the 75 included studies, 73 described original research (1–19, 21–67, and 69–75) and two were protocols for research studies for which findings had not been released by the time of the search (20 and 68). Twenty-five studies originated from the UK (1, 8, 9, 11, 18, 33, 38, 42–45, 47–50, 52–54, 56, 60, 62, 63, 67, 69, and 75), 19 from the US (10, 14–17, 19, 29–32, 34, 39, 41, 51, 55, 59, 61, 64, and 73), 13 from Australia (2, 4–6, 21–23, 26, 46, 68, and 70–72), nine from Canada (3, 7, 24, 25, 27, 28, 57, 58, and 74), four from the Netherlands (36, 37, 65, and 66), three from the Republic of Ireland (13, 20, and 40), and two from New Zealand (12 and 35). Studies were highly heterogeneous concerning the type of participants involved (e.g. pharmacists, patients with varied conditions, GPs and other practice staff, scheme commissioners, and training leads) as well as the designs and methodologies described (e.g. observational research, controlled trials, pilot studies, surveys, qualitative studies, and mixed-methods research). Around 80% of the included studies were published in the last 10 years, of which 75% were published from 2018 onwards.
Integrating pharmacists into general practices internationally
Efforts to integrate pharmacists into general practices have taken place in several countries since the late 1990s. GPBP services have been implemented, to a large degree, through short-lived programmes lasting from 4 months to a few years (10, 13, 15, 19–24, 29, 30, 36, 37, 39, 40, 46–49, 57, 58, 60, 65, 66, 68, and 70–73). The UK is the only country with established nationwide programmes so far. In other countries, efforts to integrate pharmacists were restricted to specific geographical locations and/or were of a small scale in terms of number of general practices and pharmacists involved (3–7, 10, 12–17, 19–32, 34–37, 39–41, 46, 51, 55, 57–59, 61, 64–66, 68, and 70–74).
A number of funding sources for GPBP services were reported (2–6, 8, 11–13, 21–24, 28, 32, 34, 35, 38–50, 54, 57–62, and 67–72). Funds originated from general practices themselves (including from billing patients), local primary care or other clinical structures, universities (in cases where there was some affiliation between practices and local universities), specific research teams (where grants were obtained to integrate pharmacists into general practice for a certain time period and study their impact), and governments. It is therefore apparent that a common funding model for GPBPs is absent, either inside the same country or globally. However, in general, programmes led and funded by governments appear to lead to larger numbers of GPBP posts, with the highest numbers being in Canada and the UK.
A large variety in the models of employment and integration also exists. In most studies, pharmacists were reported to work part-time in their general practice-based role spending the rest of their working time on parallel affiliations such as community pharmacy, hospitals, specialist services, and other clinical and non-clinical bodies, including academia (2–6, 10, 11, 13, 15, 19, 20–24, 28–31, 38–41, 46, 48, 49, 51, 57–59, 67, 68, and 70–72). Full-time employment in general practice-based roles was less common and was present in the ‘Pharmacotherapy Optimisation through Integration of a Non-dispensing pharmacist in a primary care Team’ programme in Netherlands, in one local effort in the US, in the Canadian province of Ontario, in New Zealand, and in the UK (but only after the large governmental schemes commenced in 2015) (1, 12, 27, 35–37, and 64–66).
In some cases, pharmacists were directly employed by practices (13, 20–23, 28, 36, 37, 40, 49, 65, 66, 68, and 70–72), whereas elsewhere pharmacists were officially hired by other structures (e.g. private companies, primary care structures, clinical bodies, specialist services, and universities) and integrated into general practices (3, 11, 12, 24, 25, 27, 35, 38, 47, 57–59, and 62). Coverage of multiple practices (i.e. one pharmacist serving a number of general practices) was a common phenomenon (1, 4–6, 10, 11, 13, 16, 17, 20, 27, 35, 40, 47, 48, 60, 63, and 67), but instances of pharmacists being located in one practice exclusively were also described (1, 3, 7, 19, 26–28, 34, 35, 40, 41, 55, 59, 61, 73, and 74). General practice-based pharmacists were either directly accessible to patients, as a choice equal to the GP and other health care professionals in general practice, or patients were invited to a pharmacist consultation (either directly by GPBPs or through referrals by other professionals) if they met certain criteria.
Activities carried out by GPBPs
Common GPBP activities, as presented in the included studies (listed in alphabetical order).
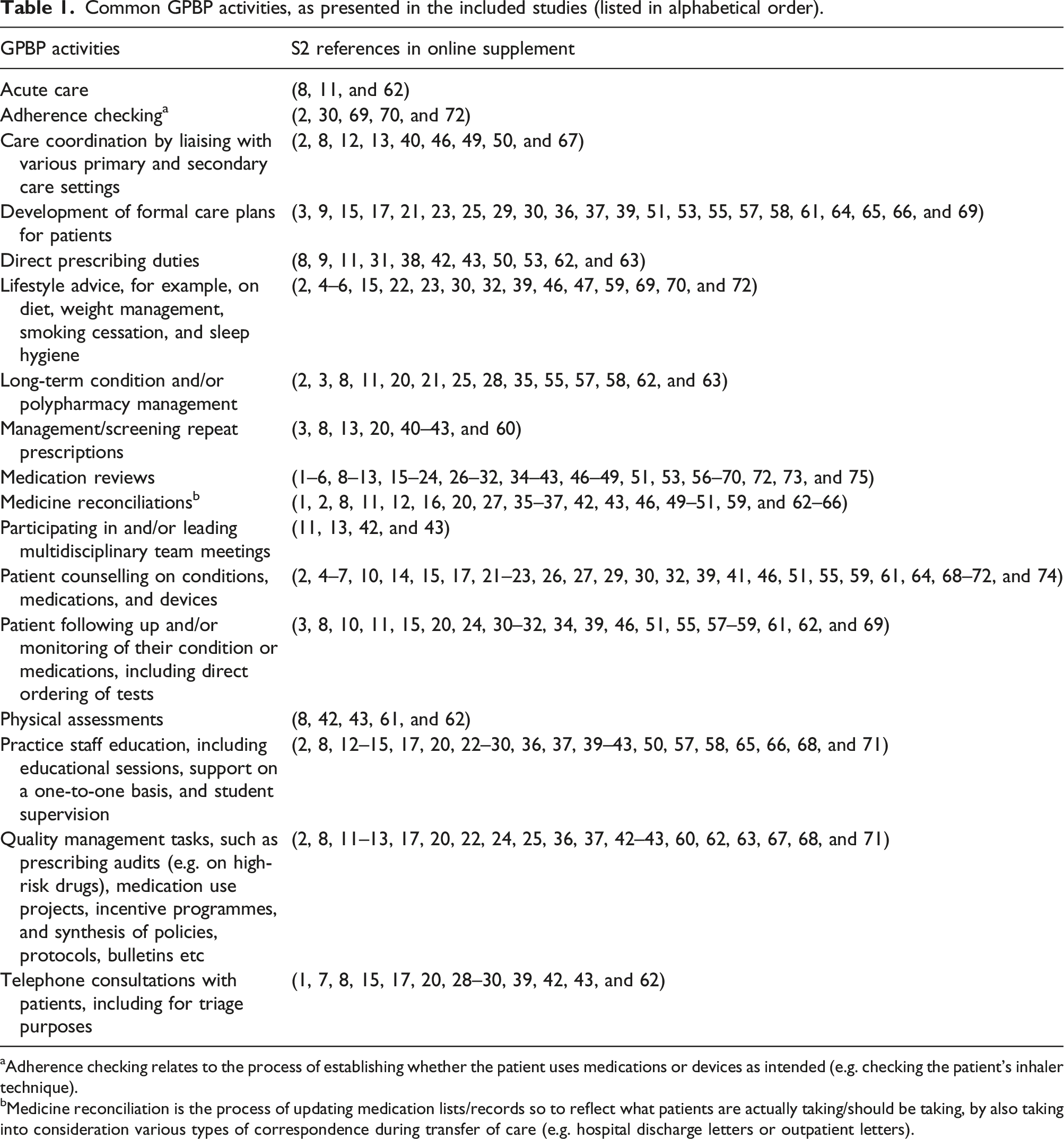
aAdherence checking relates to the process of establishing whether the patient uses medications or devices as intended (e.g. checking the patient’s inhaler technique).
bMedicine reconciliation is the process of updating medication lists/records so to reflect what patients are actually taking/should be taking, by also taking into consideration various types of correspondence during transfer of care (e.g. hospital discharge letters or outpatient letters).
In general, reported GPBP activities were quite comparable between different countries. One exception was smoking cessation services, which were only specifically mentioned in Australian studies (2 and 46). Other exceptions were the management of high-risk drugs and engagement with incentive programmes, which were only reported in the UK (8, 11, 42, 43, and 62). Examples of incentive programmes included the Quality and Outcomes Framework (a programme for English, Welsh, and Northern Irish general practices that incentivises clinical excellence) and the Quality, Innovation, Productivity and Prevention scheme (a combination of programmes in England to ensure that money is spent in a way that maximises the quality of care and benefits for patients).
Provision of acute care, physical assessments, and direct ordering of laboratory/clinical tests were also reported in the UK-based studies, as well as at some local schemes in the US (8, 11, 31, 32, 42, 43, 59, 61, and 62). Although the management and/or screening of repeat prescriptions were amongst GPBP tasks in several countries (3, 8, 13, 20, 40–43, and 60), direct prescribing and authorisation of repeat prescriptions were reported only in the UK and in the US (at a much smaller extent) (8, 9, 11, 31, 38, 42, 43, 50, 53, 62, and 63). Overall, UK GPBPs appeared to work more independently from GPs than other countries, where pharmacist input ended with a number of recommendations awaiting approval and implementation by GPs.
Methods used for identifying GPBP impact
Common methods used for identifying GPBP impact, as described in the included studies (listed in alphabetical order).
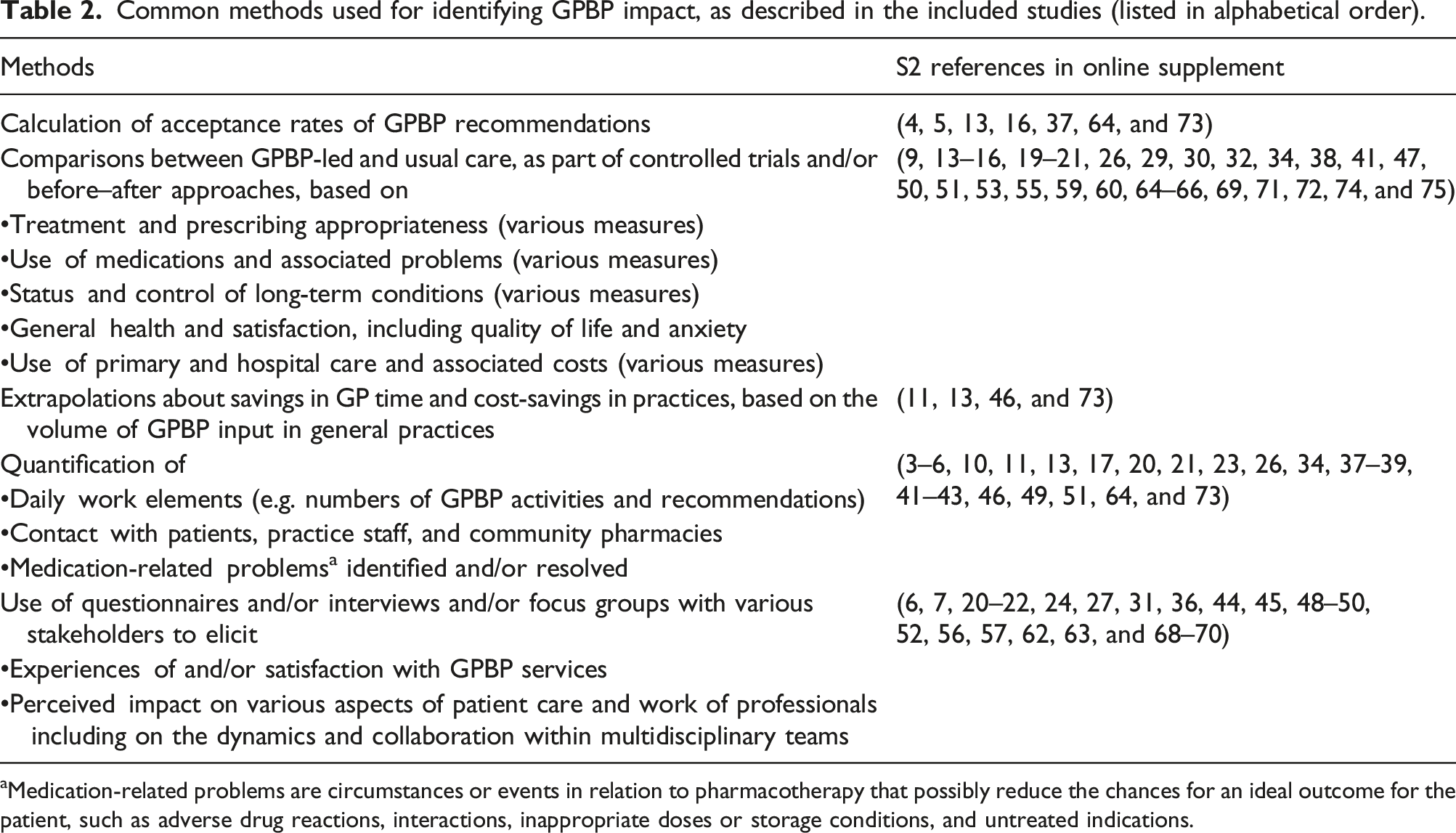
aMedication-related problems are circumstances or events in relation to pharmacotherapy that possibly reduce the chances for an ideal outcome for the patient, such as adverse drug reactions, interactions, inappropriate doses or storage conditions, and untreated indications.
Independent, quantifiable outcomes from GPBP activities
Independent, quantifiable outcomes from GPBP activities, as reported in the included studies (listed in alphabetical order).
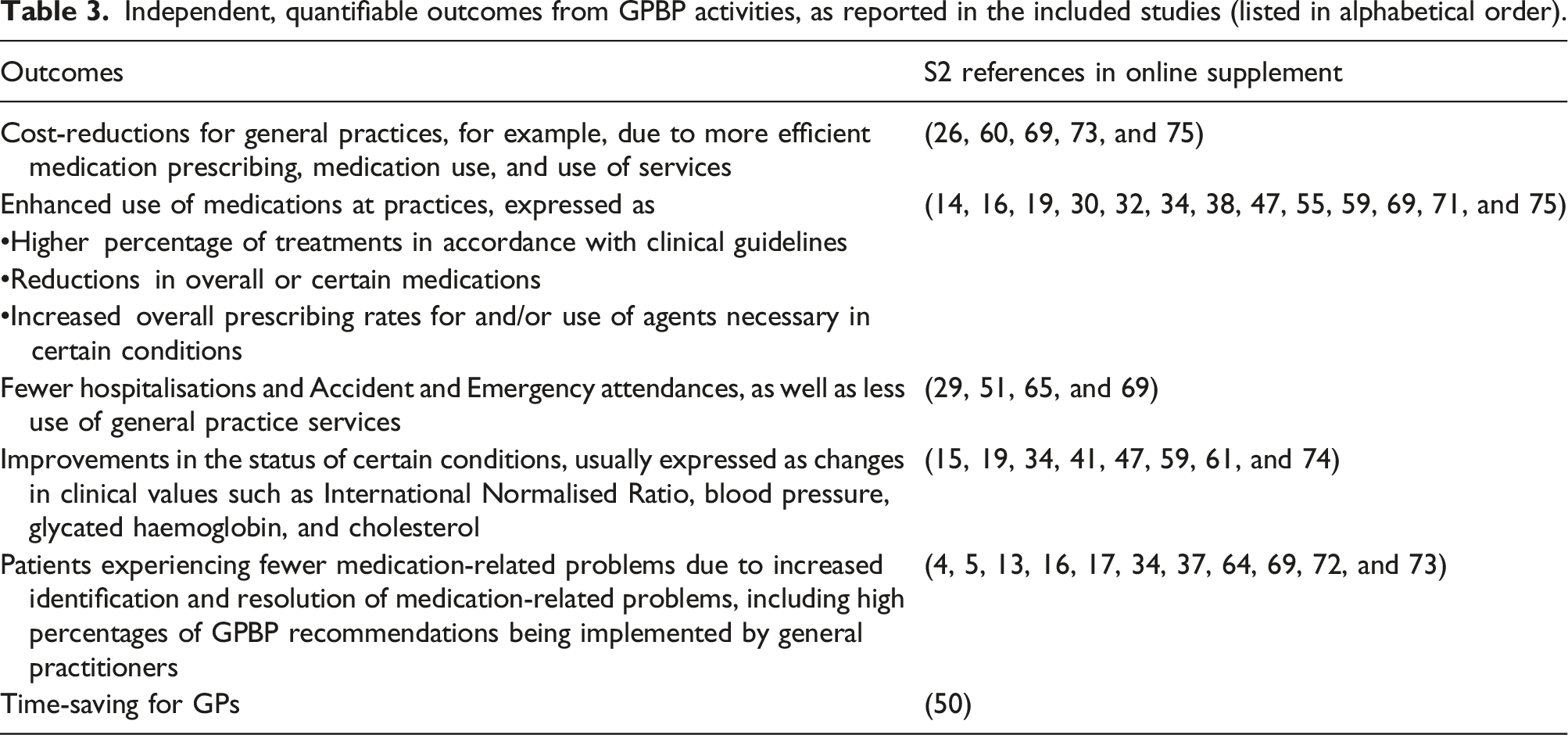
The significance of the measured differences fluctuated, with statistically significant changes in some cases (14–16, 29, 30, 32, 34, 51, 59–61, 69, 71, 72, and 74) and non-statistically significant differences and/or differences of unclear statistical significance elsewhere (19, 26, 38, 41, 47, 50, 51, 55, 64, 65, 69, and 75). Some studies found that GPBP introduction made no difference in terms of the achievement of clinical goals for long-term conditions (15, 16, and 34), use of primary and secondary care (51, 64, 69, and 75), quality of GP prescribing (66), and costs (65). However, no studies described any negative outcomes for patients and practices following pharmacist integration. Overall, we can say then that the outcomes of GPBP activities were largely positive.
Discussion
Our rapid review found that the integration of pharmacists into general practices has occurred in seven countries, through a variety of employment and funding models. GPBPs engage in many activities and roles that, with some exceptions, are comparable across different countries. A wide spectrum of methods was used to identify GPBP impact, as part of observational and/or interventional research designs. Independently measured, quantifiable outcomes from GPBP activities were reported in less than a half of the included studies. All of these outcomes were positive but were of varying statistical significance.
There was a wide variety of research methodologies employed. This heterogeneity is partly a function of the inclusion criteria for this rapid review (which were rather broad) but could also be due to different stages in the development and implementation of GPBP services across different countries. When assessing health care interventions, formative methodologies (focusing on strengths and limitations of implementation strategies) tend to be used in early days of implementation, whereas more summative approaches (focusing on outcomes) are usually preferred in later stages of assessment. 32 As the UK has had pharmacists in general practice the longest and in the highest numbers, it is no surprise that a great number of the included literature (a third of the studies) came from the UK.
There was a large variation in models of employment and integration for GPBPs, and in health care systems and/or funding between countries. No GPBP presence was found in certain regions of the developed world – for example, the Middle East and Eastern parts of Europe. Based on the included studies, it was not possible to determine what the best model for integration of GPBPs was. There was also no variation in outcomes arising from differences in GPBP models (e.g. full- or part-time posts or employment by different bodies linking to any more or less favourable outcomes). The only common theme in the literature was that governmental schemes translated to larger financial investments, more GPBP posts, greater longevity of the role, and a larger extent of full-time employment in general practice for GPBPs. Pharmacists’ presence full-time in single general practices was previously found beneficial for patients in terms of accessibility to services33,34,35 and might be worth considering when GPBP employment is desired.
As full integration leads to positive, patient-related outcomes and improvements in patient-centred, pharmacy services, 19 several strategies have been considered internationally to support the integration of GPBPs into the primary care team. Examples include ensuring certain GPBP attributes (e.g. ability to build relationships with staff and patients, non-judgemental attitude, resilience, and clinical skills) are practised when working in general practice, employing GPBPs in practices that had previously worked with a pharmacist and thereby understood pharmacist capabilities, having a system enabling patients to self-refer to the pharmacist, and drawing on GPBP experience of the local community, through either previous local work or cultural orientation programmes and/or interactions with local community pharmacists. 36 Successful GPBP integration was often found to depend on the availability of shared information systems (i.e. GPBPs working on same clinical record systems with the rest of the practice team), 19 as well as on GPBPs bringing medication-related expertise into general practices and reconciling interprofessional tensions with other members of the practice team (caused by overlapping tasks) (36).
GPBP activities were wide-ranging and generally confirmed roles described in previous reviews.22,24,25 The fact that medication reviews were the most common task for GPBPs is unsurprising as it has been reiterated (by GPs and pharmacists themselves) that the focus of GPBPs should/could be the performance of complex, clinical medication reviews in line with pharmacist expertise and training.37,38,39,40,41 The larger degree of independence of UK GPBPs in their work might be attributed to their being able to independently prescribe (if qualified to do so), which allows pharmacists to directly make patient- and medication-related decisions. 42 In contrast, in other countries pharmacists are not able to prescribe or can only do so under very specific conditions.
Since the advent of the recent pandemic, face-to-face medication reviews with patients in the general practice setting have largely been conducted virtually. 43 This was not commonly encountered in the included studies. As a result, there is a chance that virtual GPBP services might diverge from services provided in person in terms of how their impact needs to be identified, also bearing in mind the intricacies of studying the use of technology in health care, 44 and of determining outcomes. Associating specific activities with GPBP impact is an area of ambiguity (e.g. what GPBP actions exactly are responsible for certain positive outcomes?).
There has not been a common method for identifying GPBP impact, either within the same nation or across countries. A large number of measures have been employed to capture GPBP impact globally, such as activity volume, contact with patients, perceptions/experiences, and patient outcomes. An e-Delphi study found that funding acquisition for general practices was the most likely area for GPBPs to show a difference (42). Most of the included studies in this review, however, reported quantitative differences in relation to the use of medications (4, 5, 13, 14, 16, 17, 19, 30, 32, 34, 37, 38, 47, 55, 59, 64, 69, 71–73, and 75) rather than financial benefits, following pharmacist presence in general practice.
Quantitative improvements in clinical indicators (e.g. blood pressure, International Normalised Ratio, cholesterol, and glycated haemoglobin) were also described in the included studies (15, 19, 34, 41, 47, 59, 61, and 74). However, these findings only constitute a snapshot of these clinical indicators. Differences in clinical indicators do not necessarily translate to impact over respective long-term conditions, especially since GPBP integration and associated studies often lasted for short time periods and full control of long-term conditions might require a longer time period. It is also unclear if GPBPs would have more influence on any particular clinical indicator as listed above.
Some of the studies reporting on quantitative outcomes (mainly those accounting for use of hospital services and clinical indicators) found no differences and/or were inconclusive about the benefits of pharmacist integration into general practices (13, 15, 16, 19, 29, 30, 34, 38, 51, 64–66, 69, and 75). The difficulty of GPBPs to make a positive difference in the use of primary and secondary services, due to their dependence on various factors outside pharmacist control, has been echoed elsewhere (43). Where changes in relation to quantitative outcomes from GPBP activities were reported, only some were statistically significant. But even where changes were not significantly significant, GPBPs are still of value for general practices to assist GPs who are under increasing workload pressures in many countries of the Western world. 45 Indeed, GPs in several countries have largely been satisfied with GPBPs and recognised GPBPs’ role in reducing GP workload and increasing GP confidence concerning medication-related matters.46,47,48
With regards to the UK, some studies accounted for some of the formal measures developed to capture GPBP impact (e.g. volume of medication reviews, Quality and Outcomes Framework-related targets for long-term conditions, and Accident and Emergency attendances) (11, 47, 49, and 69). No studies, however, explored GPBP impact on nursing home care and detection of cancer, areas contained in latest measures for GPBPs at a national level.13,14 Although the main goal of recent UK schemes was to alleviate pressures on GPs, just one study set out to independently measure actual reductions in GP workload (50). Overall, only six UK studies reported independently measured, quantifiable outcomes (38, 47, 50, 60, 69, and 75). Despite limited exploration of quantitative outcomes, there have been continuing investments to maintain and expand GPBP presence and roles in the UK, as there are now many positive indications – if not certainty – about the usefulness of GPBPs.
It is therefore questionable whether impact identification processes are still necessary for UK GPBPs and, more generally, wherever large-scale efforts of integrating GPBPs have taken place and/or GPBP services have existed for quite a while. Identifying impact is not a straightforward procedure, as impact is multidimensional, can have more than one cause, and may have a subjective element to it, making it hard to measure numerically. 49
This review did not uncover what the easiest and/or best way to measure GPBP impact is. In the studies it was often reported that randomised controlled trials, for example, are the gold standard for impact research, since randomisation minimises biases by ensuring attribution of measured differences to the intervention of interest. 50 Although such trials might allow for certain outcomes to be followed over time, that may mean the findings are not of great relevance by the time they are published due to the rapidly changing landscape in health care. 51 Randomised controlled trials are also characterised by inherent ‘experimental’ elements that do not necessarily reflect real-world situations. 52 For example, it is difficult to set up an experiment to measure GPBP impact when GPBP work is multidimensional in nature and integrated care is collaboratively provided by GPBPs and general practice teams. As such, there are claims that non-randomised controlled trial quasi-experimental, before–after studies might be more successful in identifying real-world impacts.51,52 Perhaps an easier way to assess the usefulness of GPBPs, as well as any effect of role and/or skillset variation, could be through appraisal processes (i.e. sessions between line manager and employee to evaluate employee’s performance against mutually agreed objectives),53,54 which do not require research expertise and have historically been performed for all clinical staff in general practices.
Limitations
There are three main limitations to the current study. First, because it was not a full-systematic review there might have been additional literature on the topic of GPBPs, indexed in other databases, that was not captured. The fact only studies in English were considered means information about GPBPs published in other languages, and hence about other countries, may have been missed. In addition, it might have been that further details about GPBP models and activities were contained in grey literature reports (e.g. policy documents), which were not included in this review.
Second, the included protocol papers provided detailed information on what the respective study teams aimed to do in relation to employing and identifying GPBP impact. However, the fact that studies were not completed meant that we do not know what the impact of these GPBPs actually was.
Third, the risk of biases in the findings of the review could not be completely eliminated due to the fact no quality assessments were performed and that narrative synthesis is inherently subjective. This means different research teams might reach slightly different conclusions from the same literature. In addition, the fact that clinical endpoints and outcome measures reported in the included studies were not critically appraised (via quality assessment tools) might mean that the trustworthiness of the findings of this review pertaining to measurable GPBP impact might be questioned. However, other reviews that did engage with quality assessments18,19,21,22,23 reported similar (positive) findings to this rapid review in relation to GPBP impact on patients and health care professionals.
Conclusions
Our findings validate the usefulness of GPBP services for patients and practices, by demonstrating positive quantifiable outcomes, especially in relation to medication use. Moreover, this review shows that there are many GPBP models and ways of identifying GPBP impact. Government funding is worth considering when large-scale and long-term integration of pharmacists into general practices is desired.
For countries that want to develop GPBP services, this review provides ideas for how to do this and what evidence might be required to justify pharmacist inclusion in general practice. According to the findings of this review, it is more likely for pharmacist integration into general practices to impact upon medication use rather than use of health care services (e.g. Accident and Emergency attendances, hospitalisations, and consultations in general practice).
Future research efforts should focus on measuring quantifiable outcomes from GPBP activities for which there is ambiguity and/or no conclusive evidence. These include hospital admissions and/or Accident and Emergency attendances, clinical indicators for long-term conditions, and cost-savings. Clinical indicators need to be followed up in the long term to establish whether the GPBP services have a long-term impact. Prospective studies should also attempt to quantify the precise time-savings for GPs, post-implementation of GPBP services, as well as establish any statistically significant associations between GPBP models and improvements in quantifiable outcomes. Such research would identify the most beneficial GPBP models for patients and practices.
Supplemental Material
Supplemental Material - Integration and impact of pharmacists in general practice internationally: A rapid review
Supplemental Material for Integration and impact of pharmacists in general practice internationally: A rapid review by Georgios Dimitrios Karampatakis, Nilesh Patel, Graham Stretch and Kath Ryan in Journal of Health Services Research & Policy
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not required as this is a rapid review of the literature.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.