
Abstract
Objectives
Integrated neighbourhood teams (INTs) are central to health system reforms in England, aiming to deliver local, coordinated, and personalised care. Understanding the factors that influence their successful functioning is crucial for informing local policy and practice. This rapid evidence synthesis aimed to answer the research question: What factors influence service integration and delivery by INTs operating across health, care, and voluntary sector organisations?
Methods
In February 2025, we searched Medline and Cumulative Index to Nursing and Allied Health Literature (CINAHL) for relevant UK-based primary research and international evidence syntheses published within the last 10 years. The database searches were complemented by searches in Google Scholar and the Google search engine. Eligible studies reported evidence on factors shaping the successful functioning of local and neighbourhood-level integrated teams. Data were rapidly synthesised qualitatively.
Results
Database searches identified 5139 articles (4954 after duplicates were removed). Of these, 26 were eligible for inclusion, comprising nine primary studies and 17 evidence syntheses published between 2015 and 2025. The findings were highly consistent. Key factors supporting INT functioning included a clear, shared vision; effective leadership; strong working relationships based on trust and mutual respect; clarity on interprofessional roles and responsibilities; appropriate and sustained resources and funding; opportunities for staff learning and development; co-location, dedicated time for multidisciplinary team meetings; and interoperable information technology systems to support data sharing.
Conclusions
There is strong agreement on key relational and organisational factors that support INT functioning. Our practical framework can be used to support policymakers, commissioners, and professionals when planning and implementing INTs.
Background
Health systems are increasingly integrating across health care, social services, and other sectors to improve population health and reduce inequalities.1–4 In England, health system policy reforms in 2022 embedded cross-sector collaboration at a local level in the National Health Service (NHS). The country was formally organised into 42 Integrated Care Systems (ICSs), autonomous, area-based partnerships responsible for delivering services tailored to local needs. 5 In 2025, the Department of Health and Social care instructed ICSs to reduce operating costs by approximately 50% by October 2025, 6 raising concerns about their capacity to support local, neighbourhood-level care integration as set out in the government’s new NHS 10-Year Health Plan. 7 A central ambition of ICSs was to address health and inequalities by devolving planning and decision-making to a geographical ‘place’ level (populations around 250,000–500,000) within a system, and by establishing integrated neighbourhood teams (INTs) that coordinate care across local primary, secondary, community, mental health, social care, as well as voluntary, community, faith, and social enterprise (VCFSE) organisations8,9 at the neighbourhood level (populations around 30,000–50,000). 10
Despite strong policy momentum, there is no universally agreed definition of ‘integrated care’ or ‘integration’. 11 Models of integration range from organisations operating independently but coordinating their efforts, to formal collaborations with shared governance, to full integration under a single unified organisation. Ambiguity in the definition of integrated care, and the range of potential models, creates challenges for the implementation and evaluation of integrated care. In turn, this has hindered efforts to draw clear conclusions about effectiveness and cost-effectiveness. 11 While some evidence from high-income countries suggests that integration improves the quality of care, patient satisfaction, and access to care, the effects on healthcare use and costs are limited.12,13
Despite mixed evidence of effectiveness, integrated care remains a policy objective and INTs are central to plans to deliver integrated care at a neighbourhood level.7–9 Understanding the evidence on factors that impact the successful functioning of integrated, multi-agency team models of care, such as governance structures, leadership, funding arrangements, and the local context9,14–17 is important for integrated teams seeking to achieve service integration and delivery.
This rapid evidence synthesis (RES) was undertaken at the request of a local partner in North West England, who sought evidence to inform implementation of their local INTs model. The composition of teams in this model varied across the neighbourhoods, depending on local population needs, but typically involved primary care networks, adult social and mental health care services, and community nursing, who collaborated to share resources and information. This approach aligned with national models of INTs,8,9 which encompass vertical (e.g., primary care-led initiatives) and horizontal integration (e.g., social care- and VCFSE-led models). In this way, INTs are distinct from intermediate and transitional care models. 18
The goal of this RES was to rapidly synthesise evidence on how INTs can most effectively deliver integrated care at the local- and neighbourhood-level. Our research question was: What factors influence service integration and delivery by INTs operating across health, care, and voluntary sector organisations?
Methods
We followed a RES approach 19 to produce a qualitative evidence synthesis. RES provides a rapid, structured method to synthesise evidence, supporting evidence-informed decision-making under time constraints. 19 RES are undertaken to provide a ‘good enough’ answer to inform decisions (where the alternative is often no use of research evidence at all) using a systematic, streamlined process that enables the replicable and transparent delivery of evidence in weeks, rather than months or years. 19 RES methods are flexible and adaptive, depending on the evidence request, 19 and in this case involved working closely with a key partner to iteratively co-produce a review protocol (which is unregistered but available from the authors upon request) tailored to local needs.
We searched Medline (Ovid) and Cumulative Index to Nursing and Allied Health Literature (CINAHL; EBSCO) on 14th February 2025, complemented by searches in Google Scholar and the Google search engine. We used search terms (e.g., integrated care, integrated health, patient care planning, integrated delivery of health care, function*, success*, barrier*, hinder*, facilitator*, enabler*, implementation, evaluation*) based on components of the research question and adapted from existing relevant umbrella reviews of this literature 14 (see Online Supplement 1). We searched the reference lists and conducted forward citation searching of the most relevant articles. We excluded articles not published in English and those that were not available in full-text. We did not exclude articles based on publication status.
Study eligibility criteria.
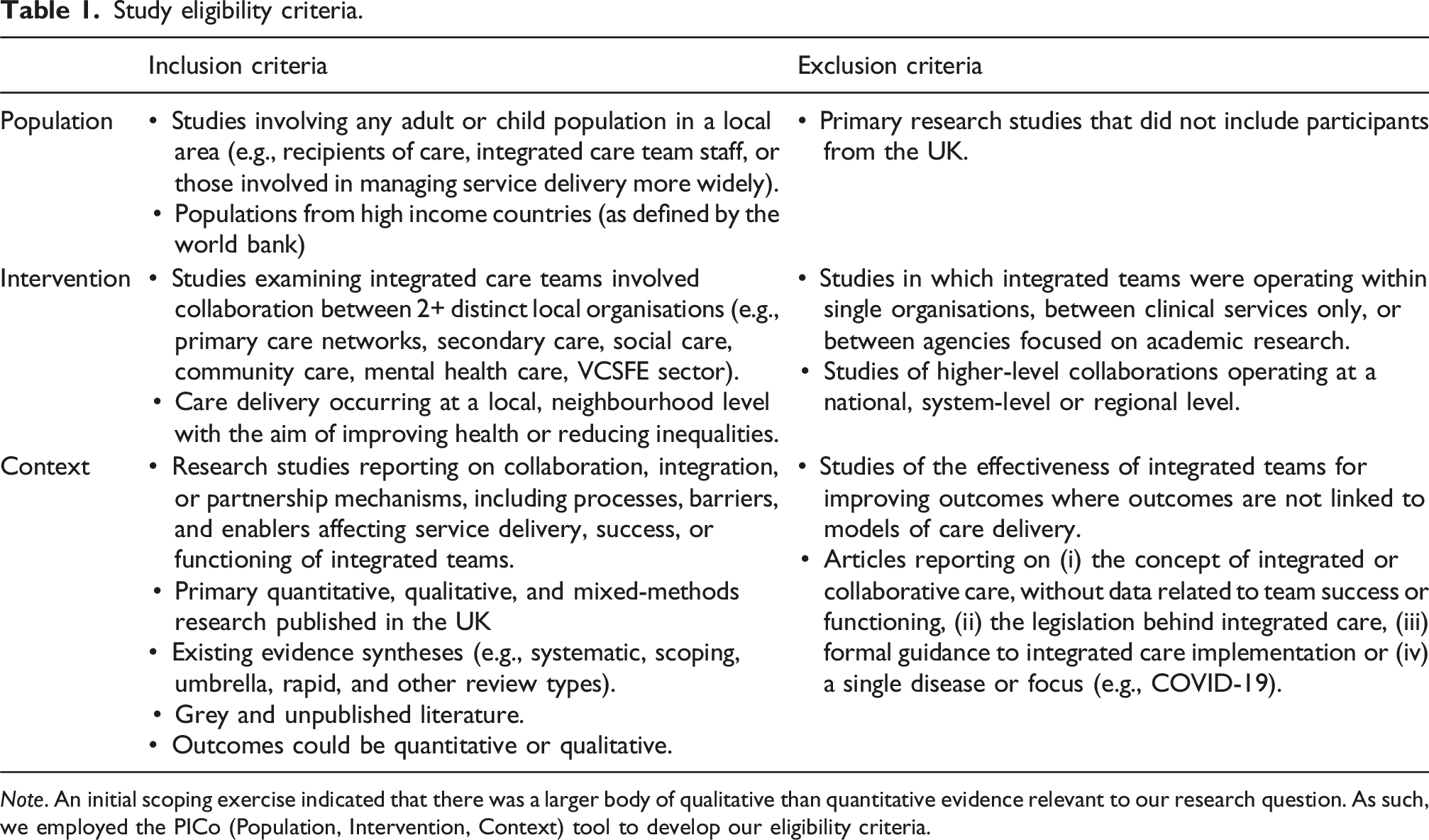
Note. An initial scoping exercise indicated that there was a larger body of qualitative than quantitative evidence relevant to our research question. As such, we employed the PICo (Population, Intervention, Context) tool to develop our eligibility criteria.
In line with RES methods, 19 we did not conduct a formal ‘risk of bias or certainty’ appraisal of each piece of underpinning evidence. Typically, RES methods leverage existing critical assessments (e.g., from systematic reviews) and provide a GRADE (Grading of Recommendations, Assessment, Development and Evaluation) 20 assessment of certainty for individual effectiveness outcomes. 19 Appraisals by studies included in this review were inconsistent; they were either not performed or only performed on an ineligible subset of evidence (e.g., studies of the effectiveness of integrated care on health and other outcomes). Thus, it was not possible to produce an overall quality appraisal. However, studies that had conceptually rich and contextually thick (vs poor and thin, respectively) 21 findings were given greater weight in the synthesis.
One author [HAL] extracted relevant data from the eligible primary studies. Two authors [HAL, SR] independently extracted relevant data from the eligible evidence syntheses (65% of included articles) and came too agreement through discussion.
We produced a rapid qualitative synthesis of the findings, informed by narrative synthesis methods, 22 which primarily uses words and text to summarise and explain findings from multiple studies and can involve thematic analysis to code data and develop descriptive themes. 22 We took a pragmatic approach to ensure timely and contextually relevant findings, prioritising relevant primary research studies from the UK to reflect the local health, care, and policy context, supplemented by international evidence from existing evidence syntheses. To expedite the synthesis, we considered the UK primary evidence first on the basis that it was more likely to be directly relevant to our partner’s request and thus more transferrable than evidence from reviews (typically reporting high-level summaries from a wider body of evidence). We extracted only the most relevant primary study findings, including those with potential relevance (i.e., when compared with findings from other studies). This was an iterative, interpretative process, and all study findings were reviewed several times amongst the wider research team.
We then undertook high-level (not line-by-line) coding of key factors influencing service integration and delivery by integrated teams. Coding was performed at the theme-level (rather than sentence-level within themes). Codes were catalogued and tabulated, grouped based on similarity, and given overarching descriptive theme names. 22 We produced a preliminary written narrative to describe the themes.
We then incorporated evidence from eligible reviews by extracting and coding review findings to identify overlap with the primary study evidence. Review findings were integrated with primary research evidence, effectively reinforcing the primary level evidence and providing further detail. We revised the narrative to include the review level evidence.
Results
Search results
The searches returned 5139 articles (of which 4954 remained after duplicates were removed). Following title and abstract screening, 84 full-text articles were identified (see Online Supplement 2). One author [HAL] screened all full text-articles, while a second author [SR] screened a subset of 26 (31%) articles.
In total, 26 studies met the inclusion criteria. These comprised nine primary studies (including one unpublished)17,23–30 and 17 evidence syntheses (including one unpublished).14–16,31–44 The eligible evidence syntheses included six umbrella reviews and 11 reviews of primary evidence (i.e., systematic, rapid, and scoping reviews) from a range of high-income countries. All reviews reported evidence narratively or qualitatively.
All nine primary studies reported recent evidence on local integrated care teams based in the UK. Of these, only one qualitative study explicitly reported evidence on integrated neighbourhood teams (which were in the process of co-locating). 23 The remaining primary studies reported qualitative and process evaluation evidence on other integrated care models, including a general national scheme (Integrated Care and Support Pioneers Programme – hereon Pioneers Programme17,24,25), general local initiatives,26–28 and more specific schemes on integration for frailty 29 and between primary and social care. 30
Data synthesis
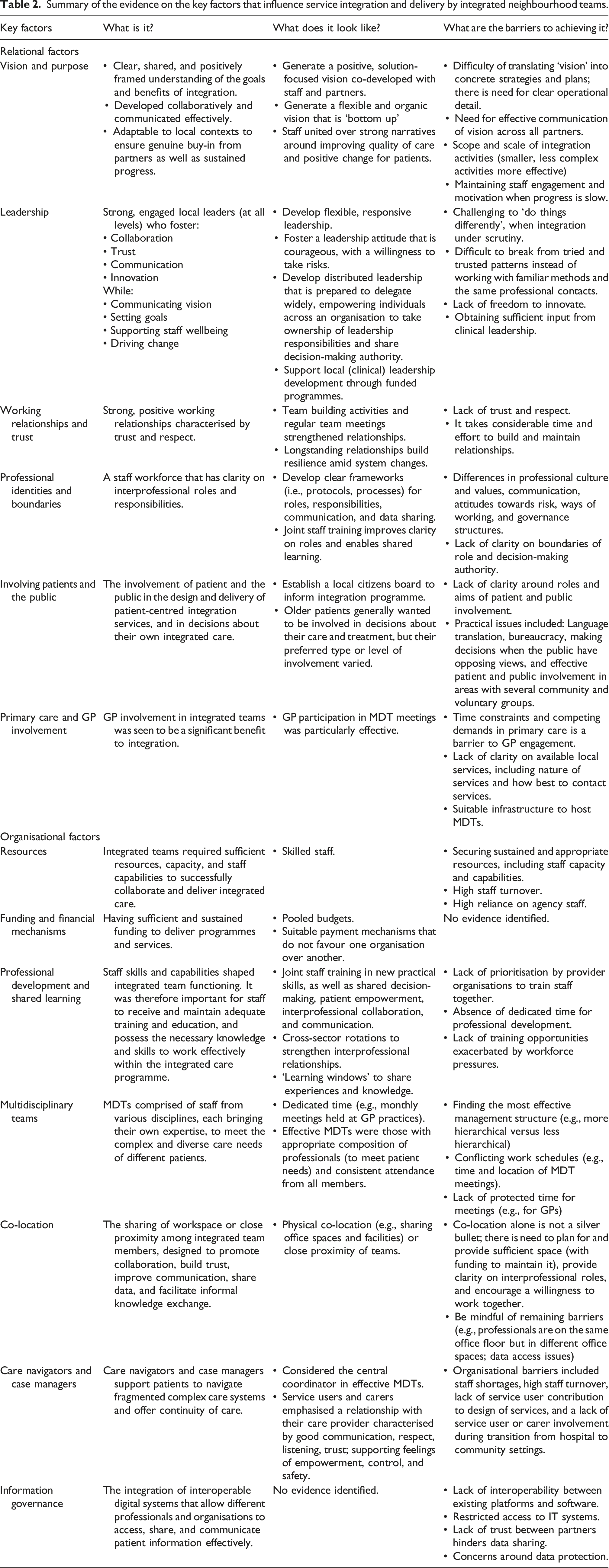
There was strong consistency in the research on key factors that were considered to influence integrated team functioning (Box 1), which are grouped under two overarching factors: ‘relational factors’ and ‘organisational factors’. These factors are described below. A summary of the evidence is presented in Table 2
• Vision and purpose • Leadership • Working relationships and trust • Professional identities and boundaries • Involving patients and the public • Primary care and GP involvement
• Resources and capacity • Funding and financial mechanisms • Professional capacities, development, and shared learning • Approaches to integrated working ◦ Multidisciplinary team meetings ◦ Co-location ◦ Care navigators, care coordinators and case managers • Information governance: IT systems and data sharing Summary of the evidence on the key factors that influence service integration and delivery by integrated neighbourhood teams.Box 1. Factors that influence service integration and delivery by integrated neighbourhood teams operating across local health and care organisations
Relational factors
Organisational factors
Relational factors
The first overarching factor is the critical role of relational issues in integrated teams, in terms of the interpersonal dynamics between team members and collaborating organisations, which affect how effectively individuals and teams work together.
Vision and purpose
The evidence highlighted the importance of a clear, shared, and positive vision of integration and its potential to improve services.14–17,23,25,27,30–33,35 This vision must be co-developed and clearly communicated across all levels (from leadership to frontline teams) to ensure ‘buy in’ and be flexible to suit local contexts.17,23,25,33,35 One study noted that a top-down approach hindered progress, instead stressing the need for bottom-up engagement. 11
However, translating vision into actionable strategies was a notable challenge. 17 While frontline staff often understood the overarching goals, many felt the vision lacked operational clarity and communication.10,12 The Pioneers Programme evaluation echoed this, finding the vision had not reached all providers in the local system. 17
Shared values created a sense of unity amongst local partners and team members (e.g., a commitment to reducing health inequalities).14,35,38 Healthcare professionals were more engaged in integrated programmes with strong narratives around improving quality of care, 17 but their motivation was difficult to sustain. Slow results from integration activities led to frustration and disengagement. 17 Differences in values could fundamentally undermine integration efforts. 14 Strategies to develop shared values and understanding included staff involvement in policy-making and ongoing training. 32
Two studies emphasised the importance of starting integration efforts with smaller, manageable initiatives guided by clear vision and purpose.16,28 Overly ambitious programmes often stalled progress. 28 Focusing on a few well-executed actions and setting short-term milestones helped demonstrate progress and maintain morale.
Leadership
Effective leadership was widely identified as essential for successful local service integration.16,23,28,29,31–33,35 Strong local leadership fostered pivotal enablers of successful integration, such as: • Communicating shared vision and purpose. • Setting clear, measurable goals. • Building trust, motivation, and commitment. • Promoting collaboration and staff wellbeing. • Scaling innovation from pilot projects. • Establishing governance structures for faster change.
A systematic review of NHS initiatives called leadership the most critical factor, noting its central role in enabling all other key factors. 31
Effective communication between leaders and frontline staff ensured guidance and support for those working on the ground. Leadership was necessary across system levels – from senior management to clinical, front-line, and local team leaders. 31
One study described leadership in INTs as requiring courage, wisdom, and a willingness to take risks, due to the challenges and complexity of multi-agency integration. 23 It was acknowledged that such leadership was challenging, particularly when integration was under close scrutiny. 23 Strategic level staff promoted a vision of distributed leadership (i.e., empowering individuals across organisations take ownership of leadership responsibilities and share decision-making authority) to support collaboration and innovation. Strategic-level staff highlighted the need for senior leaders to shift budgeting and delegation practices to support integrated care models. 23 However, in practice, team members cited challenges including unclear authority, limited decision-making power, and leaders reverting to ‘tried and trusted’ traditional (i.e., less flexible) styles. Some teams lacked the freedom to innovate, cited as a barrier in the Pioneers Programme. 16
Clinical leadership in primary care, including primary care engagement, was seen as highly beneficial. 28 In one evaluation, a charity partner initiated a separately funded primary care ‘emerging leadership’ programme, which was considered a catalyst for the professional development of those leading integrated care. 28 However, staff noted tensions between management- and clinically-led models, and questioned whether there was sufficient clinical leadership and that integration efforts are driven by and supported within primary care. 28
One review challenged the emphasis on leadership in integrated care, citing limited evidence for its impact and for interventions that build leadership skills. 15 This review argued that less visible, more nuanced factors play a greater role in shaping integration, such as professional hierarchies, tensions, biases, and political agendas. Leaders are expected to navigate these hidden complexities with clear, sensitive communication, which was believed to be a significant challenge. 15
Working relationships and trust
The evidence strongly emphasised the importance of building and maintaining effective working relationships across organisations and professions.16,17,24,29,32,33,35 Integrated teams were deemed more successful when partners had strong, trusting, and respectful relationships.14,31–33 Developing a shared vision relied on these relationships, enabling open communication, mutual understanding, collaborative problem-solving, and alignment on goals and roles. 17 Building and maintaining such relationships required significant time, effort, and goodwill.17,24,34 Longstanding relationships provided stability and resilience amid changes in staff, systems, and commissioning.14,17,32,36 Whether positive or negative, pre-existing relationships shaped how partnerships developed 14 and were especially important where no prior connections existed. 17 However, relationships were reportedly difficult to establish, due to (dis)trust between staff and professional, cultural, and communication differences. In the Pioneers Programme, engaging new providers was challenging, and these efforts were often overshadowed by other priorities and targets. 17 Asking providers to share the ‘risk and reward’ marked a major shift from previous models (in which providers aimed to gain reward and avoid risk), and some providers were excluded from key discussions, leading to tension, reduced trust, and barriers to collaboration. 17
Professional identities and boundaries
Integrated working involves bringing together professionals with different philosophies and values. There was strong emphasis in the evidence of the potential impacts of professional and cultural differences on integrated team functioning.14,17,23,27,32–34,38 Many positive accounts of interprofessional collaboration were shared, with staff anticipating mutual benefits for practitioners, patients, and service users. 23 Staff recognised the value of being able to provide information about another profession’s services to better support individuals and to determine when it was appropriate to involve other specialists. 23
However, interprofessional collaboration was often framed around its challenges and barriers. These included differences in working practices, language, conceptions of health, and a lack of mutual understanding and trust between different professions (e.g., health and social care) 23 with use of different terms (such as “patients” vs “citizens”) hindering communication. 34
There were gaps in understanding the varying roles and responsibilities of different professions. Both health and social care groups felt the other lacked a full understanding of their roles and governance structures. This applied to both traditional and emerging roles (e.g., care navigators). 26 Professionals also struggled with role boundaries, concerns over accountability, and discomfort being managed by those unfamiliar with their codes of practice or evidence-based standards.17,23,26
Evidence suggested that differing attitudes to risk (e.g., around patient discharge and referrals) could hinder trust and shared responsibility. Professions were critical of each other’s approach to risk management. For example, social care staff were perceived as more comfortable with higher-risk situations than health professionals, 23 while other professions suggested that GPs’ focus on risk management sometimes resulted in less patient-centred solutions. 17
Clarity around roles and responsibilities was considered essential for integrated programme success.14,33–38 A lack of clarity was linked to power struggles, underused services and skills, and confusion over decision-making authority.32–34 Staff believed it was important to be comfortable in the scope of their role and respectful of the role of others. 33 To improve clarity on roles and responsibilities, the evidence supported developing clear collaboration frameworks, protocols, and hosting joint staff training.14,32,34,39 Clear roles also reportedly helped coordinate patient care (e.g., by clarifying responsibility for physical health in patients with mental illness). 39 However, one study noted that some flexibility in roles could support multidisciplinary team (MDT) functioning. 14
Team-building activities and regular team meetings were believed to foster team functioning through increased understanding, trust, and a shared purpose, which in turn supported case management and information-sharing. Without these, integrated working was hindered. 32 Focusing on the patient perspective helped reduce tensions between professional groups and supported collaboration. 17
Involving patients and the public
Several studies discussed the importance of involving patients and the public in designing and delivering integrated care15,17,28,36,40 and in decisions about their own integrated care.37,41 Co-production with communities was seen as a key facilitator. 15 Pioneer Programme sites involved patients and the public to varying degrees. 17 The establishment of a local citizen board enabled active participation in decision-making. 28 However, team members raised concerns about whether these boards were truly representative and whether citizens’ roles were sufficiently clear. 28
In the Pioneer Programme, patient and public voices were seen as valuable in building the case for integration, although broader public involvement was less common. 17 Challenges to engagement included language issues during multilingual meetings, bureaucratic processes, unclear expectations of public contributors, and difficulty managing public expectations, especially in areas with many community and voluntary groups. Some believed it may not always be appropriate to directly involve patients and the public in service design, while others highlighted the overall benefits.17,40
Healthcare professionals highlighted how involving frail older patients and carers in care decisions improved the quality of care.37,41 Their participation was perceived to help tailor care and treatment plans, hospital discharges, and follow-up support. Limited involvement of service users and carers in care decisions hindered effective transitions of care between hospital and community settings for older patients. 41 However, time constraints were a barrier to effective engagement during transitions of care. 41 These findings mirror those of a review of older patients’ views on integrated care, which found most wanted involvement in decisions about their care, tailored to their needs and preferences. 42 While many expected a person-centred approach, they often felt this was not reflected in practice. Some preferred GPs to make decisions, especially about referrals, while others wanted to be informed and make their own choices. 42 Opportunities for decision-making were seen as more limited when dealing with specialists or during hospital discharge planning. 42
Primary care and GP involvement
GP involvement was widely regarded as a significant enabler of integration,17,23,25,29,37 especially participation in INT meetings. 23 However, GPs viewed integration as adding to an already overwhelming workload,29,30 which reduced motivation to collaborate and take on new responsibilities without clear benefits.29,30 These challenges were heightened in areas with many small or single-handed practices, which had limited infrastructure to host MDT meetings and capacity for strategic and development roles. 17
A significant barrier identified by GPs and practice managers was the lack of clarity about local services – what exists, who provides it, and how to access it. 30 Outdated provider contact details often forced staff to rely on patients for information, ultimately slowing communication, referrals, and collaborative working. Under time pressure, GPs tended to stick to familiar care decisions and referral options, missing opportunities to fully utilise available local resources. 17
Organisational factors
The second overarching factor related to organisational issues, involving the structural, procedural, and systemic elements within and between organisations that affect integration efforts and team functioning.
Resources and capacity
Integrated teams need adequate resources, capacity, and skilled staff to collaborate effectively.16,24,25,32,36,38,41,43 Shortages in these areas were a common barrier to collaboration and integration, often resulting in increased staff workloads and strain on frontline morale and wellbeing.14,16,24,25,27,38 Staff highlighted the importance of supportive leadership and recognition from management regarding the demands faced by frontline staff. 27
Many Pioneer Programme sites relied on small teams, whose limited time and high staff turnover hindered progress.16,24,25 In larger, more complex Pioneer sites, resources were stretched further by the need to work across multiple clinical commissioning groups and/or local authorities, diverting attention and resources from local initiatives where meaningful change could occur. 17 Key partners struggled to allocate staff time and resources, which stalled momentum. Relying on volunteers required extra recruitment effort. For providers, the volume of integration meetings conflicted with the demands of delivering patient care.
Funding and financial mechanisms
Funding was closely tied to resources and was considered essential for integrated teams to deliver services effectively.29,36,37 A key enabler was sustained funding, which helped to incentivise partner collaborations, ensure sufficient staffing, and support (long-term) planning, 40 with short-term or uncertain funding found to undermine progress.14,16,32 Stable finances were seen as essential for investment in innovation that could yield long-term cost-savings.
Effective integrated working also required collaboration between organisations funded through different mechanisms, with appropriate means in place to transfer funds between partners.31,40 Sharing resources through pooled budgets was considered highly beneficial, allowing access to additional resources and enabling innovative activities.14,17,31,39 This approach encouraged a more unified, patient-centred use of resources, and shifted the focus to meeting patient needs and away from concerns over which sector was funding the care. However, pooled budgets were seen as a ‘big ask’ 17 and could cause problems of fragmentation of service responsibilities. 32 Fair payment mechanisms were also essential. Inequities (e.g., one provider being paid by activity and another via fixed budget) could create imbalances and distort care delivery. 26 Payment methods such as payment by results (PbR) that incentivise activity in hospitals over other providers were cited as barriers to integrated care. 17 The evidence called for financial frameworks that support, rather than fragment, integration, where the inability to integrate financially and unify budgets is seen as a barrier.17,24,25,31,40
Professional capabilities, development, and shared learning
Staff skills and capabilities significantly influenced integrated team performance.32,33,36 Adequate training in areas such as shared decision-making, communication, and interprofessional collaboration was deemed essential.33,37 Practical skills were also needed – for example, nurses involved in integrated health and social care assessments requested training on topics such as discussing personal finances, previously outside their scope. 32 However, health and social care professionals often lacked dedicated time for development and reflection, limiting opportunities for learning. 36 These issues were compounded by staffing shortages, high staff turnover, reliance on agency workers, and ongoing service pressures. 27
Fostering an ethos of learning and self-reflection had positive benefits, particularly long-term collaboration. 14 Staff suggested cross-sector rotations to strengthen interprofessional relationships, but such initiatives were not prioritised by many providers. One study highlighted ‘learning windows’, which were formal and informal opportunities for knowledge-sharing and included reflective practice sessions and local staff engagement events. 27 However, while these were well attended, some staff were sceptical about their lasting impact on cross-sector relationships. 27
Approaches to integrated working
Multidisciplinary teams were key to enabling integrated care.17,26,39,41,44 Approaches varied from single management structures co-located on a single site, to less hierarchical models built on trust and shared values between team members. Monthly MDT meetings at general practices were highlighted as central to effective care coordination.26,39 MDT composition was a crucial factor, requiring diverse professionals to address patients’ complex needs.30,37,40 Teams often included GPs, extended primary care teams, integrated care team professionals, social workers, nurses, mental health professionals, geriatricians, practice managers, and case managers.27,37,39 Team success relied on consistent attendance from all professional groups. Overall, these meetings were viewed as valuable for sharing knowledge and addressing complex patient needs.
While scheduled meetings were valued for improving collaboration, practical barriers limited their success. Communication between primary and secondary care was logistically challenging, often with no standardised method for communication. 30 GPs were busy with patients during the day, while social care staff were working in the community, making joint conversations about patients nearly impossible. 30 The main criticism from GPs was the lack of protected (funded) time for these meetings, meaning GPs were unable to attend. Social care and community care staff struggled to attend due to conflicting schedules and geographic constraints (e.g., meetings in general practices) and, when present, were not always able to contribute relevant information due to limited capacity and high staff turnover.26,30 The use of agency staff further hindered coordination and continuity of care.26,30
Co-location was widely proposed as a key enabler of integrated teams.14,16,23,26,32–34,39 Physical co-location (e.g., sharing offices) or close proximity of teams was believed to strengthen integration, trust, relationships, and collaborative working, and facilitate data sharing. It also created opportunities for informal communication (e.g., ‘corridor conversations’) about patient care. 26 Some staff viewed co-location and being under unified management positively, while others found it unnecessary or counterproductive, depending on local context and team dynamics. Careful planning was required to provide sufficient physical space for co-location (e.g., primary care services to be located in a mental health clinic). 39 In one study, social workers were not co-located with healthcare teams, and faced difficulties due to inadequate workspace and limited access to their own data systems. 27
It was acknowledged that co-location alone was insufficient without investment to support planning and provision of physical space for professional groups to come together. 39 However, simply sharing a space did not necessarily result in cohesive teams. 23 Staff needed to understand their roles and responsibilities and work willingly and collaboratively, 39 emphasising that people (rather than specific ways of working) were essential to successful integrated care. Silos remained when, despite sharing work spaces, professional groups were in different offices, limiting shared learning opportunities. 26 Territorial use of shared space further reinforced silos. 43 This highlighted that successful integration depended on people and relationships, not structural arrangements alone.
Care navigators, care coordinators, and case managers supported patients to navigate complex systems and provide continuity across services.33,39,41,44 Their value was particularly evident in the literature on integrated care for people with severe mental illness 39 and frailty.41,44 As central figures in MDTs, they facilitated personalised care, smoother transitions from hospital to community settings, and access to appropriate information and support. 34 Service users and carers valued the continuity of care offered through one-to-one relationships, characterised by good improved communication, respect, trust, empowerment, and a stronger sense of safety and control. 41
However, the impact of these staff was reduced by staff shortages, turnover (particularly among care workers), and limited involvement of service users in designing services and managing transitions when leaving hospital. 41 Concerns were raised about the limited advocacy power and authority of care navigators, particularly when working across services less familiar with severe mental illness (e.g., dental care for those with severe mental illness). 39
Information governance: IT systems and data sharing
IT interconnectivity and shared platforms were of central importance for effective integration, communication and information sharing.23,26,31,33,36,38 Integration was hindered by restricted access to IT systems and poor interoperability across platforms.32,34,38 General practices and social care teams used different software and lacked methods of transferring patient data, instead relying on emails and calls, causing delays and raising confidentiality concerns. 30 The absence of a unified IT system limited data-sharing among health and social care and partner services (e.g., GPs, mental health providers, emergency services, and social care), all of whom maintained separate patient databases.
Data protection concerns arose around what patient information could be shared and with whom, reflecting low perceived trust between sectors and services. The fragmented approach to data access was seen as a risk to safeguarding and individual safety, with inadequate information sharing impacting staff safety and accuracy of risk assessments for lone-working and home visits. It was recognised that sharing comprehensive data on individuals could reduce unnecessary referrals to other services.
There was a belief that fostering stronger professional relationships could promote trust and confidence in data sharing. Integration was viewed as an opportunity to address these IT challenges, though fully unified systems were considered unlikely in the short term.
Discussion
Integration between health, social care, and other sectors promises to improve population health. We sought to rapidly review the evidence on factors shaping the successful functioning of INTs in achieving service integration and delivery. We identified 26 studies reporting evidence on local and neighbourhood team integration. Our rapid qualitative synthesis of the evidence identified overarching relational and organisational factors, which covered leadership, vision and purpose, relationships and culture, involving patients, the public, primary care and GPs, resources and funding, approaches to integrated working, information governance and IT systems.
In March 2025, it was announced that NHS England will be brought under closer control of the Department of Health and Social Care. 6 The 42 ICSs in England were asked to drastically reduce their operating costs by Autumn 2025, raising significant concerns about the capacity of ICSs to support and sustain neighbourhood integration of care. INTs are a relatively recent policy development within England.8,9 As of July 2025, the UK Government’s new 10-Year Plan places neighbourhood health centres in every community. 7 Our findings suggest that many of the relational and organisational factors commonly highlighted in broader literature (e.g., leadership, vision, trust, and infrastructure) retain their relevance in INTs,8,9,23,45 but staff within INTs need freedom to think for themselves and agency to act, supported by strong local leadership and clear vision. Our synthesis highlights that well-functioning INTs will require steady, sustained resources and funding to support staff retention, reduce reliance on agency workers, incentivise partners, and enable integration progress. In light of the evolving policy landscape, this synthesis informs reflections on how INTs can adapt and ensure the goals of integrated care remain achievable amid systemic financial constraints. Our findings highlight the dual importance of considering both relational (e.g., working relationships) and organisational (e.g., funding) factors in INT functioning.
Strengths and limitations
Our review has several strengths: we identified a substantive body of evidence using an adaptation of review methods designed to provide a very rapid evidence update to support time-sensitive local decision-making. 19 We included peer-reviewed and grey literature, increasing the contextual depth of the synthesis. Two reviewers independently assessed the relevance of evidence for extraction and synthesis and the wider research team reviewed the findings. The included studies reflect contemporary understanding of factors influencing local integrated team functioning. While not exhaustive, we have updated the evidence to identify central themes important to integrated team functioning.
Our review has some limitations: we searched a small number of databases, we did not critically appraise the evidence, and we focused extraction on the most relevant data for subsequent synthesis. As such, there may be additional relevant studies and data from included studies, and we are unable to comment on the quality or certainty of the evidence. Further, while our searches identified some grey literature, we did not perform a comprehensive grey literature search. Where possible, we only reported data from individual studies once, but some overlap of findings may still exist across reviews.
Implications
Despite decades of integration initiatives in the UK and internationally, evidence on the effectiveness of integrated care for improving public health remains mixed.12,13 Yet integrated care models, including INTs, remain central to health policy.8,9 This requires a shift in research priorities from assessing whether integration ‘works’ to investigating how best to implement integrated care in diverse local contexts. Understanding what enables or constrains their ability to deliver coordinated and equitable care remains critical.
Our synthesis presents an accessible framework for policymakers, commissioners, health service managers and professionals to use when implementing INTs. While the present RES was undertaken in the context of a single local INT model in England, we argue that the principles identified (e.g., the importance of leadership, shared vision, adequate resourcing) are likely to be highly transferable to other settings. Adaptation to local organisational structures, care system priorities, and commissioning arrangements will be necessary, but these factors provide a practical framework to guide implementation.
Our synthesis highlights key gaps in the evidence. Evidence shows that tension and a lack of understanding between different professional groups can lead to conflict within teams that impedes integration. More research is needed on the INT workforce, 46 including how different professional identities develop and interact within INTs, 47 what supports staff retention and wellbeing in multi-agency settings, and how to support primary care engagement in integrated care models. 48
GP involvement in MDTs was deemed essential for INT functioning, yet workforce demands made this difficult, and those GPs engaged did not always know what local services were available. More research is needed to understand how local GPs can be supported to participate, as integrated care becomes increasingly neighbourhood-based. Given how highly GP engagement was valued, exploring how their involvement in MDTs affects integrated care activities and outcomes should be considered.
Co-location was considered critical to integration initiatives even when other barriers were cited (e.g., siloing, territorialism, separate offices). Research could explore how to optimise shared workspaces and viable alternatives (e.g., virtual) if physical co-location is not possible. More research is needed to understand how patients, the public, and wider communities can be meaningfully involved in INTs – both in decisions about individual care (e.g., participation in MDT meetings) and in shaping the design and implementation of integrated neighbourhood care. Our search for evidence on patients’ and the public’s experiences with local integrated care identified only a small literature.34,41,42 This gap warrants further research.
In line with previous umbrella reviews of this literature, 14 we found limited evidence on how different factors interact, their relative importance in different settings or contexts, and how potential tensions between factors (e.g., central leadership vs local distributed autonomy; differing ways of working between professional groups) are negotiated in practice. This lack of granularity continues to impede our understanding of which collaborations work best, for whom, and in what contexts. Shared staff training was cited as a beneficial way to promote team- and trust-building, but there was often a lack of funding and organisational commitment for this.
Looking forward, there is an opportunity to build on this partnership-based approach by embedding evaluation into ongoing INT implementation efforts – with a focus on exploring the comparative impacts of different approaches to the issues identified (e.g., the impact of GP engagement, or greater levels of patient involvement). Embedding evaluation within implementation can help ensure that the generation of evidence and development of services coexist and evolve together in response to local context and need, even in the absence of definitive evidence on the overall impact of integration on public health. In this way, research can better support local systems to maximise the potential of integration. This type of embedded, responsive approach to evidence generation may help to bridge the gap between research and practice by supporting co-produced learning and knowledge mobilisation. Finally, aligning research activity with the needs of local systems reduces the risk of research waste, as the resulting evidence is more likely to be relevant and usable.
Conclusions
Integrated care remains a central policy imperative in the UK and internationally. This rapid qualitative evidence synthesis identified key relational and organisational factors that are consistently perceived to influence the successful functioning of INTs, offering a practical framework for local policymakers, commissioners, and professionals. In the absence of stronger evidence on the effectiveness of integrated care for improving public health and health inequalities, these contextual insights can support INT reflection, planning, and development efforts.
Supplemental material
Supplemental material - What factors influence service integration and delivery by integrated neighbourhood teams operating across local health, care, and voluntary sector organisations? A rapid synthesis of qualitative evidence from the UK
Supplemental material for What factors influence service integration and delivery by integrated neighbourhood teams operating across local health, care, and voluntary sector organisations? A rapid synthesis of qualitative evidence from the UK by Hannah A Long, Peter Bower, Sonya Rafiq and Sonya Rafiq in Journal of Health Services Research & Policy.
Footnotes
Acknowledgements
We gratefully acknowledge our local public partner for approaching us with a request for evidence to inform their activities, and for their valuable collaboration in co-developing the review scope and protocol. We also thank Professor Jo Dumville and Dr Chunhu Shi for their thoughtful feedback and assistance in developing the review protocol and editing this manuscript.
Ethical considerations
This rapid review synthesises previously published data and does not include new data that require ethical approval.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Hannah Long is funded by the University of Manchester Healthier Futures Research Platform. Professor Dame Nicky Cullum, Professor Peter Bower, and Dr Sonya Rafiq are partially funded by the National Institute for Health and Care Research (NIHR) Applied Research Collaboration Greater Manchester (ARC-GM). The views expressed in this publication are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.