
Abstract
Trauma, socio-economic, cultural and structural issues are associated with poor outcomes for most health conditions and may also make research participation difficult and onerous, perpetuating intervention-generated inequalities by generating evidence from those least in need. Trauma-informed and resilience-informed approaches to care may help address these concerns across health and social care research. These approaches take an empowerment-based response to adversity, and are suitable for integration and extension as Trauma and Resilience Informed Research Principles and Practice (TRIRPP) for studies beyond the topics of resilience and trauma. Four TRIRPP aims were identified: addressing the adversity context that may underpin the lives of research participants and the phenomenon under study; improving study accessibility and acceptability for individuals and populations facing adversity; recognising and addressing traumatisation in potential participants; and recognising and promoting resilience. Recommendations include interview participant control of recording devices, over-sampling of under-represented populations in population surveys, and actively seeking to engage disenfranchised individuals in patient and public involvement from design to dissemination. The practice of research has the power to address adversity and trauma or to perpetuate it at both an individual and a societal level. It is feasible and worthwhile to integrate trauma-informed and resilience-informed approaches across research topics and designs. Further work should extend the TRIRPP recommendations and evaluate their use.
Introduction
Poor health is linked to the social inequalities that arise from inequities in power, money and resources, 1 with high rates of trauma in general populations impacting health and access to interventions. 2 The majority of health outcomes, and many of the ‘risk behaviours’ known to precipitate them such as substance use, are associated with social inequalities and trauma, 3 and it has been argued that ‘Given population prevalence estimates of sexual violence and other traumatic experiences, it is worth considering whether standards for ethical research practice in general should be guided by trauma-informed (TI) principles’.4(p.4769) Those facing greater adversity also have fewer emotional, financial, time and other resources to access health and social care and to act on public health information. 5
These associations remain largely unaddressed in research methodologies and ethics, yet they are important because adversities can also affect willingness and ability to engage with research, such that societies’ most disenfranchised may be less likely to experience good health and to participate in the studies which inform health care decisions. This has been referred to as ‘academic capitalism’, which describes the structural academic drivers that favour studies of ‘tame populations’ willing and able to participate quickly and efficiently. 6 Without careful attention to study design, there is a propensity to recruit ‘tame individuals’ from within populations of interest. Those whose lives are shaped by different forms of adversity may find those adversities to act as disenfranchisements, reducing their ability to participate in health and social care research, and undermining their ability to undertake preventive health actions or access health care. Structural injustices are also seen in attitudes towards research, for example, lack of trust forming a barrier to research participation by those from racially minoritised populations. 7 This reflects a broader distrust of institutions and the legacy of research such as the Tuskegee experiment in the USA. 8
Lack of participation by those facing greater adversity may lead to ‘intervention-generated inequality’, meaning that health inequalities are worsened when interventions are inadvertently developed to be most inclusive of those facing least adversity. 9 This is both a methodological concern, primarily due to sample bias and non-generalisability of findings, and an ethical concern as this practice breaches the ethical principle of justice as the right to access health care and participate in research. 10 Although intervention evaluation may addresses social inequality, 11 earlier stage guidance on study design and execution is needed to minimise the likelihood of intervention-generated inequality occurring in the first place.
At the same time, the ethical principles of beneficence, non-maleficence and autonomy 10 may also be violated where those facing the greatest adversity do take part in research and for whom participation may be more onerous and uncomfortable, and potentially distressing. 12 Different forms of adversity are likely to create different challenges. For example, those experiencing regular infringement of their rights may feel less empowered to assert their needs regarding study information, data collection, withdrawal and dissemination. Others may have to make greater personal sacrifices in order to participate for a variety of personal or practical reasons and might find the process anxiety provoking, in particular those facing abuse in their homes or workplace for whom there is no clear and easy exit strategy. Without due care to such factors, communities and individuals may be less likely to take up future offers to participate in research and more likely to feel harmed by participation.
Research topic and design may also affect the ability and willingness to participate in research, and the experience of doing so. For example, online participation will exclude those without internet access but be more acceptable for anonymously researching populations or topics characterised by illicit, sensitive experiences, for example, parents with problematic drug use.
Regardless of topic sensitivity or study population, requirements for participation may present difficulties for individuals facing adversity, including trauma, who are within the sampling frame but whose trauma or adversity experiences do not define the sampling frame or the topic of interest. Thus, the conventions of research may in themselves be traumatic for, or excluding, of some who fall within the eligibility criteria for a study. 13
This concept paper sets out the rationale, conceptual basis and overview of the Trauma and Resilience Informed Research Principles and Practice (TRIRPP) framework, as a tool to address inclusivity and participant experience.
Existing work to enhance research inclusion and experience
Patient and public involvement and co-production
There are several approaches that seek to enhance inclusion and participant experience in health research. In England, these include cultural competence training for health services delivery and randomised controlled trials (RCTs) to redress low study participation from black and minority ethnic communities. 14 In many countries, health research funders have championed patient and public involvement (PPI) to improve the acceptability, accessibility and relevance of health and social care research. For example, in our own work of women with problematic drug use, PPI led to improved access (targeting advertisements to public toilets known for drug use) and a more positive participant experience by removing from the survey questions colloquial terms for sexual activity that were deemed offensive. 13 Concerns remain however that PPI enlists contributions from the most enfranchised and focuses on researchers’ agendas, that is, conducting impactful research, rather than principles of justice or social equity. 2 A trauma-informed and intersectional approach to PPI has been suggested to ensure health inequalities are not reproduced in PPI and that instead seldom-heard groups and individuals can influence research design. 2
Research co-production has also gained traction in recent years, co-producing knowledge through partnership working between academia and communities at all stages of the research. Overlapping with approaches such as user-led research, participatory, strengths, assets-based and action research, co-production aims to ensure that the experience not only of research participation but of conducting the research is an empowering and positive experience and which includes the voices of those whom the research seeks to benefit. 15 Co-production is well-suited to intervention development aimed at particular communities and populations defined by a health condition or type of adversity. However, larger-scale quantitative studies, such as general population surveys and RCTs, may not be well-suited to co-production and may be particularly vulnerable to PPI and study participation from ‘tame populations’, thus perpetuating intervention-generated inequalities.
Overall, co-production and PPI make important contributions to improving inclusivity and participant experience in research. However, a broader framework of research principles and practice may widen the mechanisms by which we can address these issues, encompassing co-production and PPI within.
Existing work to adapt trauma-informed and resilience-informed approaches to care for research purposes
Trauma-informed approaches to care and research
Recommendations for a trauma-informed approach to research about sexual violence.
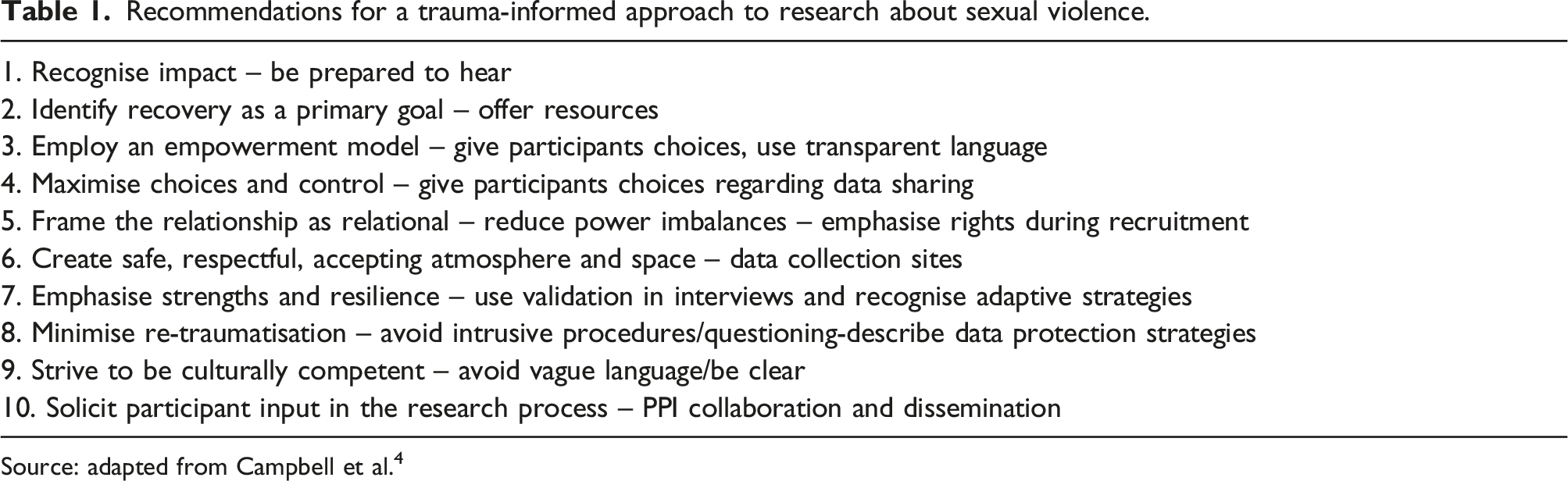
Source: adapted from Campbell et al. 4
For research on topics other than trauma, encouraging and enabling disclosure of traumatic experience, as recommended in some TI approaches, 19 might be impractical however for example, in large-scale surveys and unethical, for example, where no immediate support is available. Campbell et al. have provided recommendations for general population surveys of trauma-related phenomena that may be suitable to other quantitative designs and topic areas, such as delaying recruitment for those who are recently traumatised, and unobtrusive means of study withdrawal or skipping triggering questions. 4
Resilience-informed approaches to care and research
Resilience is conceived of as positive phenomena or activities in response to adverse contexts, acknowledged and fostered through resilience-informed (RI) approaches. 15 Resilience-informed approaches may similarly be of benefit when adapted to improve inclusivity and experience in research. However, conceptually, resilience places the onus on individuals to adapt and cope, 15 which would allow those in power to ignore the underlying social inequalities. ‘Resilience for Social Justice’ (RSJI) has been developed to address these concerns with the intention to ‘encompass this potential for marginalised people to challenge and transform aspects of their adversity, without holding them responsible for the barriers they face’.15(p.1)
The RSJI approach has been applied to research on the topic of resilience, with the core features set out in Table 2. 15
‘Practical moves’ for a RSJI informed approach to research on resilience.
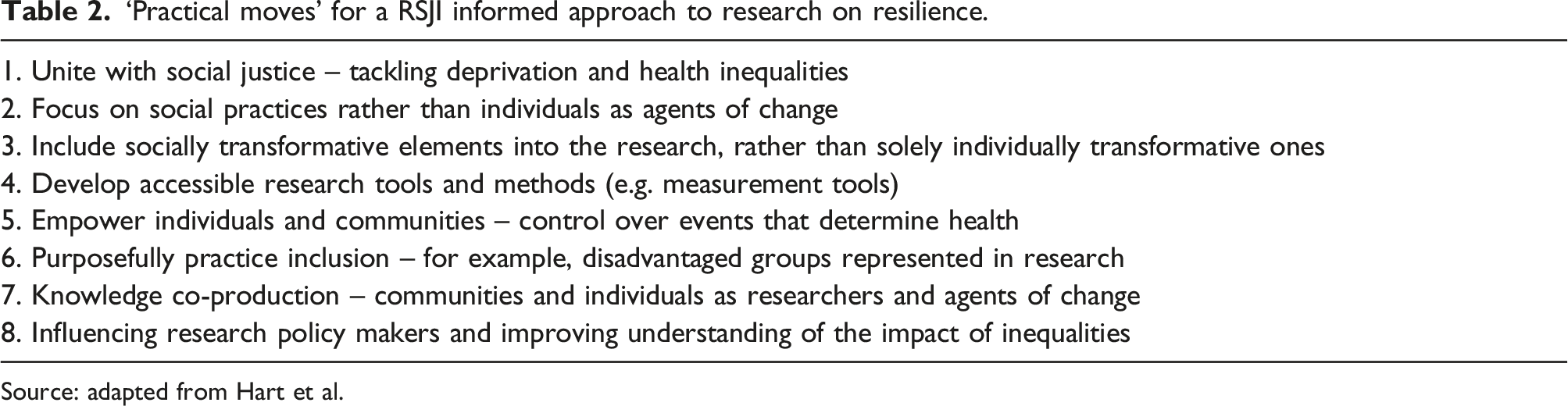
Source: adapted from Hart et al.
An integrated framework of TRIRPP
Resilience for Social Justice approaches have not been applied to research beyond the topic of resilience or study designs that do not easily lend themselves to co-production or intervention development, while TI approaches have been largely confined to qualitative research methodologies; 18 yet both are likely to be suitable for wider use. I here propose an integrated framework of TRIRPP, which is applicable to a wide range of topics and methodologies to improve inclusion of the voices of the most disenfranchised and traumatised into our understandings of, and response to, adverse health outcomes.
Rationale for Integration
As noted, TI and RI approaches take an empowerment-based approach, and each explicitly acknowledges the concept foregrounded by the other. More specifically, TI approaches seek to foster resilience 16 to reduce, recover from or avoid trauma, 19 while RI approaches position trauma as part of the adversity context from which resilience may emerge. 15 Giving both concepts equal salience in principles, practice and title was a deliberate act by the author, aiming to raise awareness of the importance of addressing both resilience and trauma in research processes, rather than foregrounding one or the other. This decision was born of the author’s lived experience as a researcher and a single-parent with post-traumatic stress disorder (PTSD), carer responsibilities and socio-economic challenges. Using quantitative and mixed methods approaches to the sensitive topic of sexual and reproductive health and associated psychosocial issues over 20 years, fostered awareness of how trauma often underpinned people’s experiences and perceptions, and the need for a framework from which to innovate research practice improvements. Personal experience highlighted the challenges of participating in and conducting research and of using services. The stark difference in experience where one’s resilience as well as one’s trauma are recognised and respected was a significant driver in the decision to make both concepts salient in the framework’s name and approach.
The TRIRPP framework
The aims of TRIRPP are as follows: • To identify, acknowledge and address the adversity context which may underpin the lives of research participants and the research phenomenon under study. • To improve study accessibility, acceptability and participation from disenfranchised and/or traumatised individuals and populations. • To recognise and address the likelihood of trauma experiences among research participants and researchers and seek to avoid re-traumatisation. • To recognise and promote the resilience of research participants and researchers.
A key assumption of TRIRIPP is the notion that the research context itself can attenuate, exacerbate or present new adversities such that ‘an individual’s needs for special protections in the research context depend…on the particular features of the research project and environment in which it is taking place’.21(p.47)
Without careful attention, the research context may re-traumatise or disincline participation from those with trauma or those who face chronic adversities, while also being a site that can maintain and foster resilience by transforming aspects of adversity. Research practices, regardless of topic and methodology, might easily accommodate an assumption of underlying trauma, acknowledging this possibility in the treatment of all participants and those in the sampling frames from which participants are recruited. Trauma and Resilience Informed research Principles and Practice therefore invites the researcher to consider the fine details of contexts and processes through which activities such as recruitment, data collection and dissemination are conducted.
Developing the TRIRPP framework
The development of the TRIRPP framework involved, first, an exploration of the concepts of resilience and trauma to identify areas of congruence and dissonance and develop an integrated understanding to underpin the framework. Second, I reviewed the principles and activities of TI and RSJI approaches for use in the TRIRPP framework. The third phase of testing and refinement of the framework is the subject of ongoing work.
The concepts of trauma and resilience
Both trauma and resilience are constructed as responses to contexts of adversity. Trauma can be understood as a failure of context; that is, the impact on neurology and sense of self of overwhelming adverse experiences not adequately contained by the individual, the environment or those around them. 22 The corollary of this is that social support provides the best protection against developing trauma responses, such as PTSD, to adverse events and contexts. 22 Resilience conversely, is a positive response to adverse contexts. While some RI approaches focus on ‘internalised resilience’ (psychological attributes and behaviours of individuals), 15 the RSJI approach conceptualises resilience as ‘overcoming adversity, whilst also potentially subtly changing, or even dramatically transforming, (aspects of) that adversity’.15(p.10) As discussed above, this conceptualisation comprises ‘moves’ practiced at the level of organisations and communities as well as individuals. Importantly, TI and RSJI approaches both foreground the importance of relationships and social context; neither trauma nor resilience can be understood, fostered or attenuated without recognising the interdependence of context and individual. 23 They also focus on empowerment and address cultural issues, to define meaningful outcomes in the case of RSJI 24 and to recognise cultural legacies and context (TI). 16
Conceptualisations of trauma may differ between the resilience and trauma literature. The latter recognises both singular events and cumulative incidents and adversities as trauma-inducing, such as in the case of complex/childhood PTSD. In contrast, resilience literature has increasingly moved away from conceptualising chronic adversity as itself traumatic; in order to simplify resilience research, there has been a tendency to conceptualise trauma in relation only to singular ‘potentially traumatic events’ (PTEs), the effects of which may be avoided or attenuated through resilience. 25
The high degree of congruence between TI and RSJI approaches makes them suitable for integration and expansion, using the TRIRPP framework. The TRIRPP framework seeks to acknowledge the complexity and multiplicity of trauma and resilience, recognising in particular that both can co-exist in contexts of adversity 24 and taking the position that resilience emerges (and can be fostered) in the contexts of both trauma arising from PTEs and trauma arising from contexts of chronic adversity.
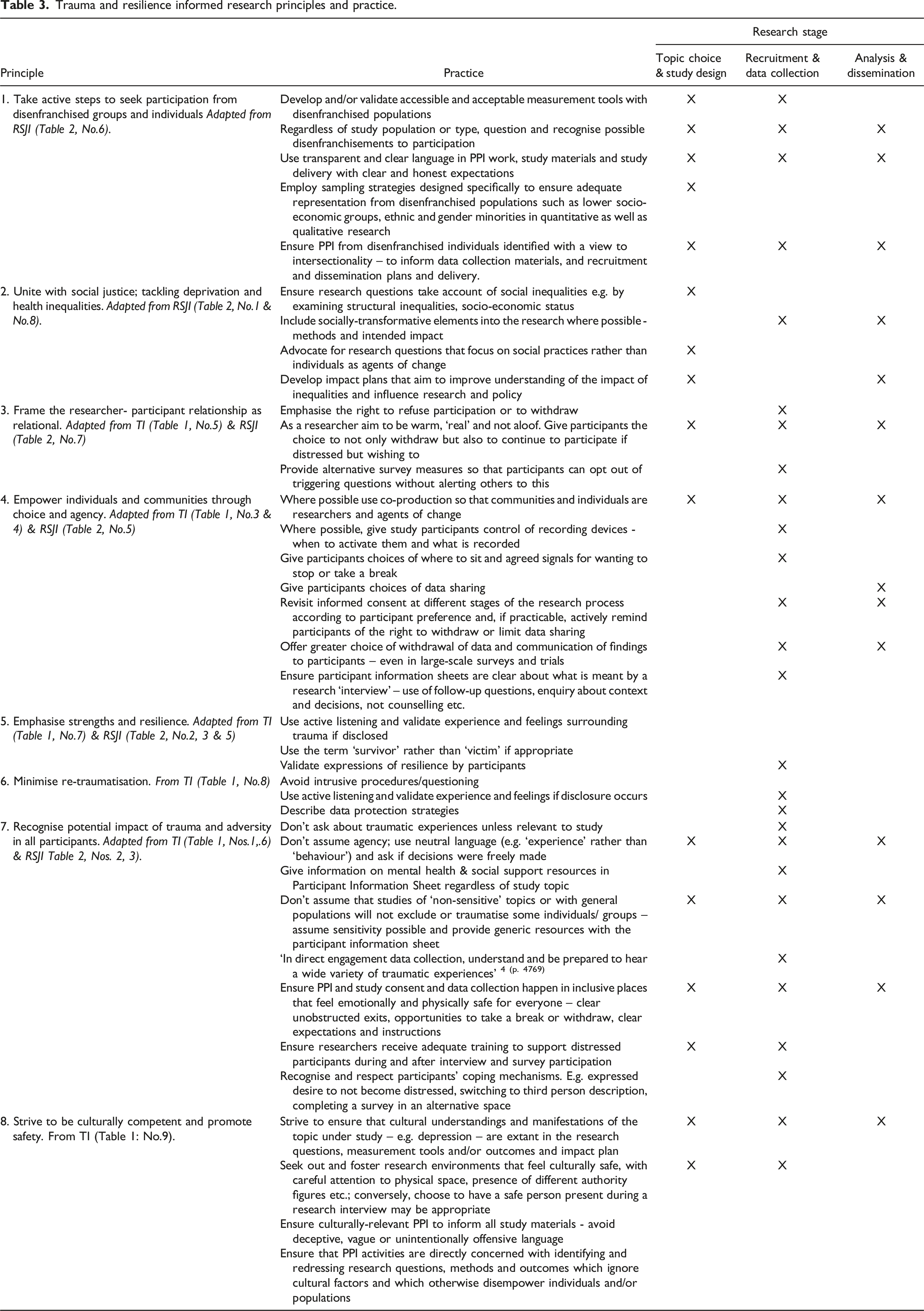
Reviewing the principles and practices of TI and RSJI approaches to research
Trauma and resilience informed research principles and practice.
Discussion
Drawing on and expanding existing TI and RSJI research recommendations, TRIRPP offers a framework from which to approach research with the explicit intention of addressing intervention-generated inequalities, by creating inclusive opportunities for engagement in research for and with disenfranchised and traumatised individuals and populations, including researchers, promoting well-being throughout that process. It does so by seeking to avoid re-traumatisation and promote resilience, and transform aspects of adversity both within and beyond the research context itself. Trauma and Resilience Informed Research Principles and Practice invites us to lay down assumptions that the individuals and populations we seek to engage as participants are not traumatised or face adversity, nor ourselves as researchers. Instead, TRIRPP acreknowledges and works inclusively with this reality.
Trauma and Resilience Informed Research Principles and Practice’s focus on reducing intervention-generated inequalities through research processes is consistent with intervention development models such as APEASE, which are used to assess interventions across a number of criteria including equity, 11 and with Beauchamp and Childress’ biomedical ethics framework. 10 However, TRIRPP also attends to critiques that the ethical principles of autonomy, non-maleficence, and justice cannot adequately address differences in adversity among participants and the populations from which they are recruited without due attention to trauma. 4 Trauma and Resilience Informed research Principles and Practice further addresses the notion of justice by aiming to offer fair opportunity to access health care, participate in the research that underpins it, and transform aspects of adversity. The TRIRPP framework thus reframes PPI as a means of redressing intervention-generated inequalities. This approach to PPI aligns with recent pleas for greater diversity in PPI 26 while moving beyond arguments that it is morally right to include the end users of research in its design 27 or that PPI can improve the rigour of a study. 12 Instead, PPI is conceptualised within the TRIRPP framework as a deeper change to how we conceptualise health research as a social justice activity.
Conceptual issues
Conceptual issues emerged during TRIRPP development concerning the generic meaning of the words ‘recommendations’, ‘principles’ and ‘practices’ and the extent to which they differ from each other. For example, although resilient moves are described as practical, they are applicable variously to topics, impact and research methods and are for the most part congruent with the definition of ‘principle’, although the proposed TI recommendations for sexual violence research more clearly delineate principles from practice. There is a corresponding lack of generic enquiry into the process by which principles are translated into practice. Practice theory may offer a lens from which to notice and address that process, enacted through communities of practice and with attention to the reflexivity embedded in TI research.
This attention to practice may also be useful in identifying and addressing tensions between the aims of a study and the use of TRIRPP practices in study processes. Indeed, tensions between the aims of trauma research and the application of TI principles have previously been described: conflict between participants’ privacy and public availability of data; providing informed consent and trauma-induced difficulty with decision-making; and the need for unbiased population samples versus the need for transparent participant information which may disincline traumatised people from participation. 4 Similarly, employing the TRIRPP practice suggestion of describing the depth of questioning used in research interviews may be at odds with methodological aims by deterring participation and thus biasing sample and findings towards those more comfortable with in-depth questioning. Process and realist evaluation may be helpful in identifying possible tensions and assessing possible impact.
The conceptualisation and focus of TRIRPP may not appear to be novel, as many of its principles and practices have been proposed previously. Some elements of TRIRPP may be seen to deviate from RSJI and/or TI approaches; the framework may be considered at odds with an RSJI approach because co-production is not recommended for studies such as population surveys, and because RSJI authors have highlighted that a focus on vulnerability (akin perhaps to trauma and other deficit-based constructs) ‘is neither constructive nor ethical’.15(p. 5) The RSJI approach also speaks directly to egalitarianism and empowerment as discrete but related concepts; further conceptualisation of TRIRPP in relation to these is needed. Nonetheless, TRIRPP’s focus on tackling inequalities aligns with RSJI values in creating mechanisms by which the marginalised can transform aspects of the adversity they face. 15 Thus, TRIRPP might itself be considered a resilient move.
Areas for TRIRPP development
Consultation and testing work to further refine and expand TRIRPP is planned, incorporating the lived experience of others with trauma and those who conduct research. Trauma and Resilience Informed research Principles and Practice recognises that researchers may themselves face their own trauma and other adversities. The potential impact of qualitative research on researchers has been noted, alongside a propensity to explore topics that hold personal resonance, 2 but less so for quantitative or non-human studies, which may be conducted in social and cultural settings characterised by conflict or climate adversity. A separate TRIRPP publication is planned, applying the framework to improve researcher inclusivity and experience.
Trauma and Resilience Informed research Principles and Practice also offers opportunities for methodological innovation. Quantitative study designs, particularly large-scale RCTs and observational studies, might accommodate more purposive sampling strategies of under-represented groups, alongside nuanced data-sharing preferences. The COVID-19 pandemic has also precipitated a shift towards internet-mediated research, necessitating further development of TRIRPP in this domain.
The cultural aspects of TRIRPP also need further development regarding both cultural competency and cultural safety. Firstly, trauma and resilience can only be understood within cultural contexts and may manifest in ways that do not conform to the Global North’s conceptualisations. 23 Accordingly, TRIRPP needs development with regard to cultural competency to ensure that research contexts are culturally appropriate in supporting participation, minimising re-traumatisation, and promoting resilience. Trauma and Resilience Informed Research Principles and Practice also needs further development in terms of creating cultural safety by changing how research is conducted so that those from racially and other minoritised populations have a positive experience of participation. 28 For example, the notion that research interviews should be conducted with only the interviewer and researcher present may feel unsafe to some, providing an opportunity to revisit and re-assess the rationale for such conventions. Practice recommendations particularly may vary by setting and culture. For example, the recommendation to over-sample disenfranchised groups itself assumes a variation in experience across society. Conversely, in settings framed by widespread poverty or conflict, trauma and resilience may be important concepts for the whole population and regardless of research topic.
Conclusions
The practice of research can either address adversity or perpetuate it, at both individual and societal level and thus challenge researchers to develop new research procedures. 4 Trauma and Resilience Informed research Principles and Practice has the potential to reduce harm and intervention-generated inequalities by strengthening our research practices to be more inclusive and safe; introducing and normalising structures and processes that empower individuals and populations. Evaluation of these potential benefits is needed to establish if TRIRPP meets its aims, to identify and ameliorate inadvertent harms and to extend TRIRPP practices.
Trauma and Resilience Informed research Principles and Practice is founded on the belief that attention to the details of how research is conducted and to broader social contexts may improve the likelihood of participation by those facing greater adversity, and improve their subsequent experience of so doing. In doing so, it reframes health and social research as social justice activities that actively seek to reduce intervention-generated inequalities, using research practice as a means to tackle inequalities through inclusivity, empowerment and safety.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval was not required for this conceptual and methodological article.