
Abstract
Objective
To describe the disruptions in care experienced by persons with Multiple Sclerosis in Italy due to the COVID-19 pandemic and the self-reported impact on their health and wellbeing.
Methods
A cross-sectional online survey was completed by 2722 persons with Multiple Sclerosis, after Italy instituted a national lockdown in response to the pandemic.
Results
Persons with Multiple Sclerosis reported that the pandemic caused broad disruptions to usual health and social care services, which impacted on their health and wellbeing. Disruptions in care were consistently associated with negative self-reported impacts on the expected progression of the disease, on out-of-pocket expenditure and on carer’s stress. Psychological consequences were associated with interruption to usual psychological support, and concerns about the safety of care delivered in person.
Conclusions
The quality of life of persons with Multiple Sclerosis depends greatly on prompt access to a broad range of health and care services. Negative psychological impacts reported by persons with Multiple Sclerosis with less severe disabilities show that accessible integrated services are crucial for maintenance of their wellbeing. Most persons with Multiple Sclerosis with more severe disability experienced negative impacts on perceived health. Their carers compensating for lack of social input resulted in care overburden. As continuity of care is crucial for persons with Multiple Sclerosis, as well as for persons with chronic conditions in general, strategies must be in place to ensure it is included in future pandemic response plans.
Keywords
Introduction
Multiple Sclerosis (MS) is an autoimmune neurodegenerative disease affecting almost three million people worldwide, including one million in Europe and 127,000 in Italy.1,2 MS is the most common non-traumatic cause of disability in young and middle-aged adults.1,2 An effective response to the needs of persons with MS (PwMS) requires multidisciplinary management and access to a broad range of services, including pharmaceutical therapy (both disease-modifying and symptomatic), regular specialist examinations, diagnostic tests, rehabilitation therapy, psychological support, social care and inclusion services.3–6
Ensuring that the needs of PwMS are met is generally challenging for health systems.7,8 Non-urgent health care has been delayed in most health systems during the COVID-19 pandemic, both to secure health care capacity to treat COVID-19 patients and to contain nosocomial spread. 9 Social distancing and restrictions on movement imposed in many countries has often meant limited or no access to home and semi-residential social care, as well as to medication.
MS care is mostly aimed at delaying its unpredictable progression, at promoting PwMS’s functional independence and at managing and preventing complications. Discontinuities in care, alongside increased risks of complications in case of infection for those receiving disease-modifying therapy, 10 may affect perceived health and psychological wellbeing of PwMS. Mental health is in fact a crucial aspect of their health and wellbeing, as depression and anxiety are common comorbidities while psychological stress can trigger relapses in patients with relapsing/remitting MS (RRMS).11,12
In February 2020, Italy became the first western country to face a COVID-19 outbreak. The country imposed a national lockdown, which ran from March 9 to May 4, 2020. 13 Soon after the lockdown began, the Italian Multiple Sclerosis Society (AISM) recorded a surge in contacts to its hotline and web platforms from concerned patients affected by disruptions in services and generally unsure about how to mitigate any health consequences. Based on these reports, AISM developed a questionnaire to gain insight into emerging issues that would inform its response by way of its voluntary workforce and its advocation of local and national policy.
Data were analysed to explore the health system’s ability to meet patient needs during the pandemic. The association of service disruptions with self-reported impacts was examined to describe the risks posed by these service discontinuities, providing further insight into the value of care for PwMS.
Methods
Questionnaire
The questionnaire was developed by a multi-professional team of experts, including AISM and academic staff, and was rapidly piloted with a few PwMS who work at AISM. The research team balanced the need to investigate several domains of the life of PwMS with minimizing the burden on participants, who in completing the survey may experience fatigue and difficulty concentrating (common symptoms of MS). For this reason, as well as the need to tailor questions to capture pandemic-related impacts, use of existing validated scales was deemed not appropriate.
Participants
On March 18, nine days after the national lockdown began, the questionnaire was launched as an online survey. It was promoted on AISM’s website and through AISM’s newsletter. In previous online surveys, PwMS with severe symptoms had lower participation rates than did other respondents. 7 To increase their representation in this survey, PwMS with more severe disabilities were contacted by staff from AISM’s local branches. PwMS completed the questionnaire with AISM staff over the phone.
Analysis
Analysis was performed on the 2722 questionnaires completed (of the 4396 started) up to April 15, 2020.
Considering how greatly need varies amongst PwMS depending on their level of disability, 7 the analysis looked separately at four groups based on a self-assessed adaptation of Expanded Disability Status Scale (EDSS) used in published studies. 7 The groups were: minimal disability (self-EDSS < 4, n = 1343), mild disability (self-EDSS >=4;<6, n = 701), moderate disability (self-EDSS >=6;<7, n = 427), severe disability (self-EDSS>=7, n = 251).
The analysis aimed to examine associations between experiencing disruptions in care due to the pandemic and self-reported outcomes, including health status, psychological wellbeing and additional out-of-pocket expenditure (Table 1). More specifically, the disruptions experienced were treated as the exposure, and the outcomes of interest were compared between exposed and non-exposed. Exposure and outcome variables were transformed into dichotomous variables when necessary, and z-tests for independent proportions were used to assess statistical significance of differences in outcome percentages among exposed and non-exposed. Only the associations that were significant in at least three of the four disability-based groups were included in the results. Data were analysed using MS Excel.
Disruptions in care experienced due to the pandemic and self-reported impacts included in the analysis.
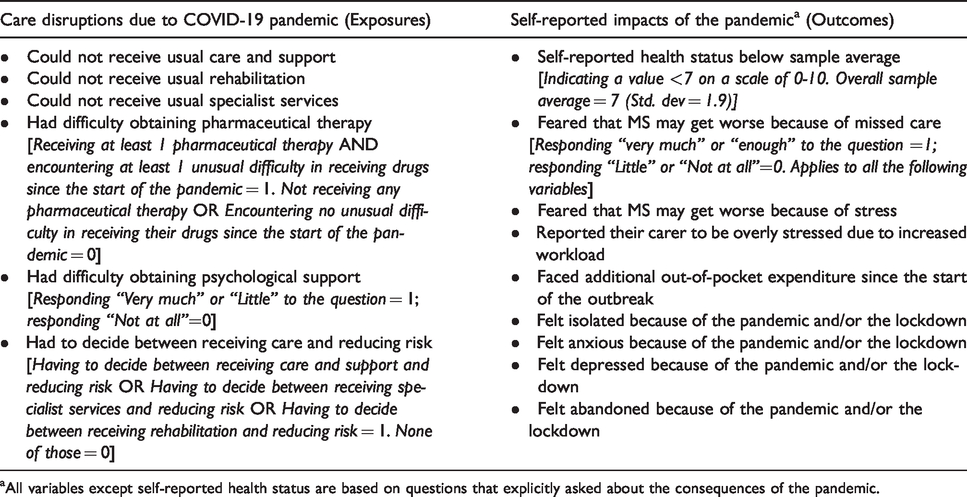
aAll variables except self-reported health status are based on questions that explicitly asked about the consequences of the pandemic.
Results
Sample characteristics and reported disruptions in care
Despite the voluntary nature of participation, the sample was broadly representative of PwMS in the general population on several characteristics (Table 2). All but four respondents were aged 18 or over (three were 17 and one was 16). Gender ratios reflect national and international prevalence data.14,16 These included a lower female ratio among PwMS with the most severe disability. 17 Average age was consistent with previous research, 7 with most diagnoses being received between age 20 and 40 and with the diseases being progressive in nature.1,2 The geographical distribution of respondents reflected the most recent sub-national prevalence estimates of MS, 2 ensuring representation of all areas of the country.
Characteristics of the sample and care disruptions experienced during the pandemic.
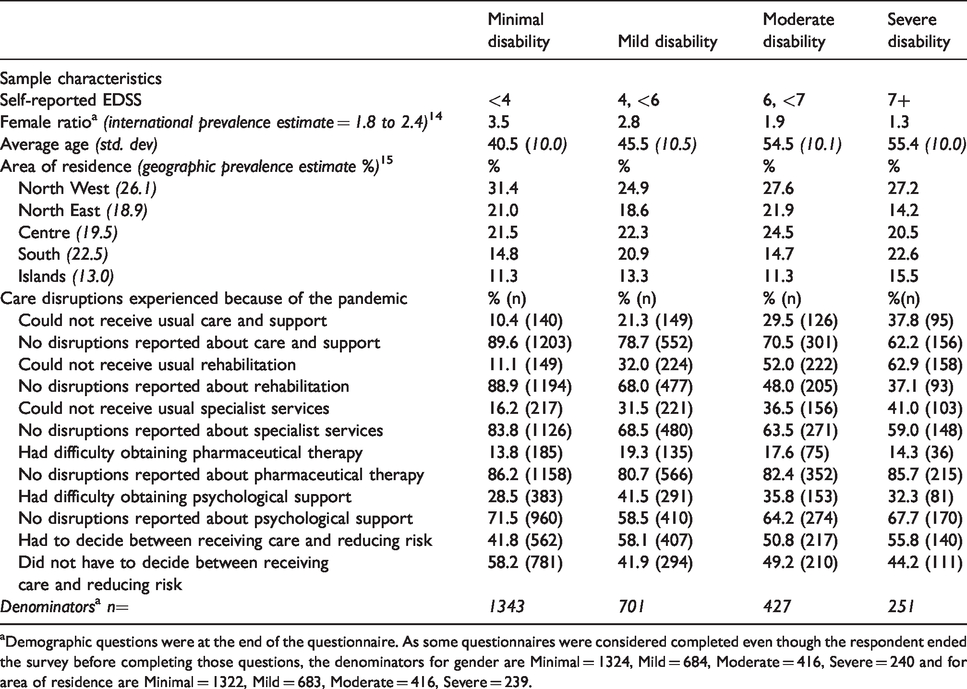
aDemographic questions were at the end of the questionnaire. As some questionnaires were considered completed even though the respondent ended the survey before completing those questions, the denominators for gender are Minimal = 1324, Mild = 684, Moderate = 416, Severe = 240 and for area of residence are Minimal = 1322, Mild = 683, Moderate = 416, Severe = 239.
As noted in Table 2, the proportions of PwMS that experienced disruptions in care varied across the four groups in most instances, as PwMS with more severe disability (included in the moderate and severe disability groups) experienced a higher proportion of lack of usual care and support, rehabilitation and specialist health. All four groups experienced similar proportions of problems in obtaining pharmaceutical treatment and difficulties in receiving psychological support. Nearly half of all respondents across the four groups indicated that they had to decide between receiving care and protecting themselves from risk of infection.
Self-reported health and fear of MS getting worse
As detailed in Table 3, a higher proportion of PwMS with more severe disability reported experiencing worse self-reported health status (above 75% in both the moderate and severe, 54.9% in the mild and 16.5% in the minimal disability group). They were also afraid in higher proportions that their MS could progress because of interruption to usual care. Conversely, the percentage of participants reporting fear that their MS could progress because of stress was higher in the mild disability group (58.2%).
Impact of disruptions in care on self-reported health status and expectations on progression of MSa
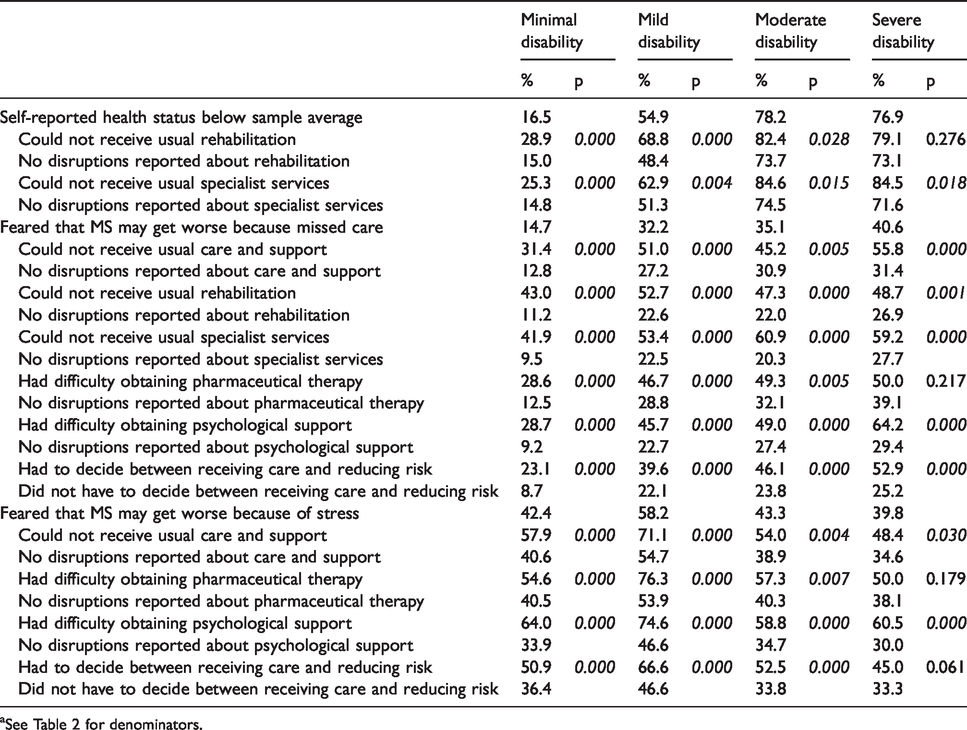
aSee Table 2 for denominators.
The analysis showed that several care disruptions were significantly associated with worse health status and fear of MS progression in most groups. Not receiving usual care and support, rehabilitation, specialist services were strongly associated with fear of progression due to missed care across all four groups. A large difference in percentages with this outcome was observed between those who experienced these disruptions and those who did not. Missed rehabilitation and missed specialist health care were associated with a self-reported health status below the sample average in most groups, while difficulties in obtaining psychological support were mostly associated with the fear that stress could cause MS progression.
Carer’s stress and additional out-of-pocket expenditure
As shown in Table 4, higher proportions of PwMS in the moderate and severe disability groups reported that their carer was overly stressed from the additional care workload caused by the pandemic (almost two out of three respondents in the most severe group). Similarly, out-of-pocket expenditure was reported in higher proportions among these PwMS than in the other groups.
Impact of disruptions in care on carer’s stress and additional out-of-pocket expenditurea
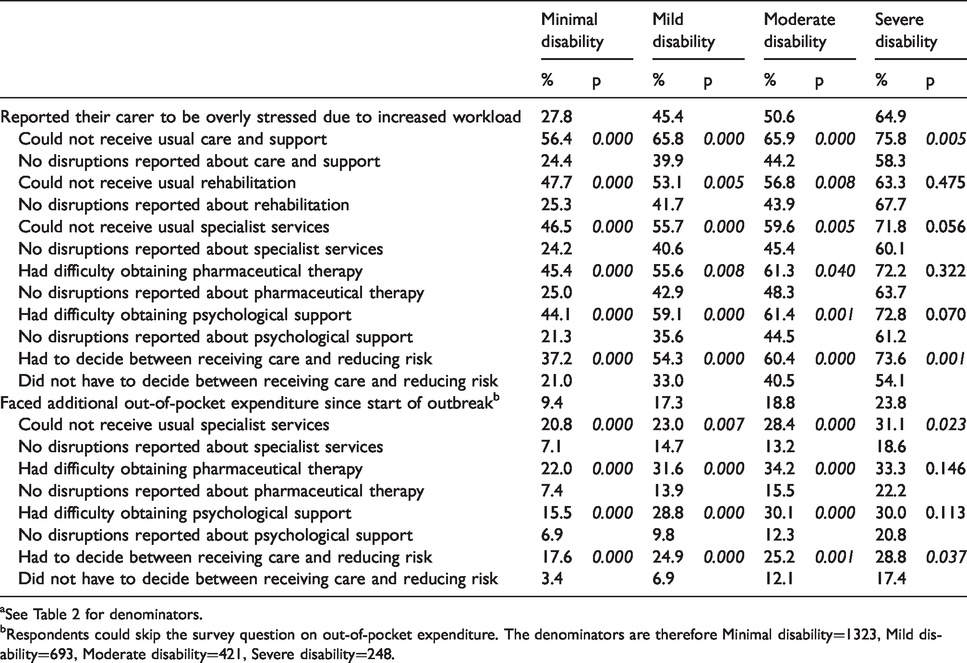
aSee Table 2 for denominators.
bRespondents could skip the survey question on out-of-pocket expenditure. The denominators are therefore Minimal disability=1323, Mild disability=693, Moderate disability=421, Severe disability=248.
Most care disruptions were significantly associated with these two outcomes. Regarding carers’ stress, across all four groups particularly large percentage differences were observed between those who missed care and support (56.4%, 65.8%, 65.9% and 75.8% respectively in the minimal, mild, moderate and severe disability) and those who did not (24.4%, 39.9%, 44.2% and 58.3% respectively). Missing usual specialist services and difficulties in obtaining psychological support were associated, also with large percentage differences, with both reported carer’s stress and additional out-of-pocket expenditure in all groups but the severe.
Psychological wellbeing
As shown in Table 5, reported impacts of the pandemic on psychological wellbeing differed less across the four groups. PwMS with more severe disability did not indicate that they felt depressed, isolated or abandoned in higher proportions than those with less severe disability. Rather, lower proportions of PwMS with severe disability reported feeling anxious (38.6%, with percentages ranging between 45.2% and 54.6% in the other three groups).
Impact of disruptions in care on psychological well-beinga
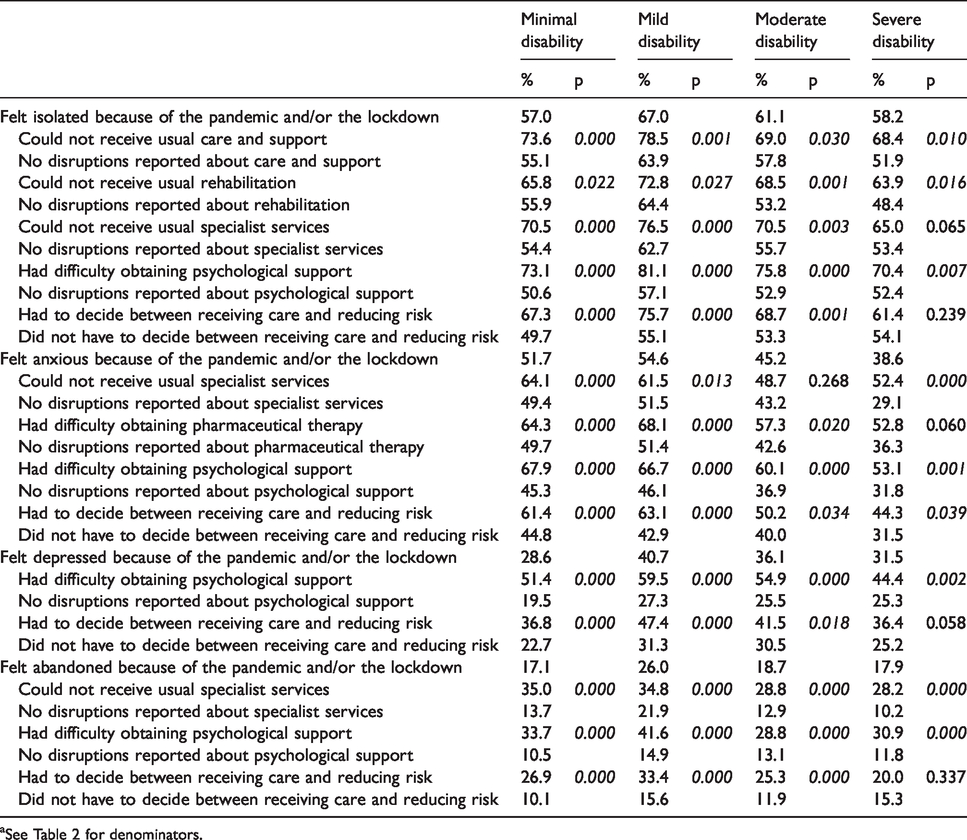
aSee Table 2 for denominators.
Psychological wellbeing appeared to be strongly associated with disruptions in care due to the lockdown. Difficulties in obtaining psychological support and having to decide between receiving care and reducing the risk of infection were significantly associated with all four outcomes investigated here (except having to decide between care and risk reduction in the severe group, only significantly associated with feeling anxious). Not receiving specialist health services was associated with anxiety, feeling abandoned and isolated (percentage differences were significant in all groups except for the severe about feeling isolated and the moderate about feeling anxious). Disruptions in rehabilitation therapy and pharmaceutical therapy were associated respectively with feeling isolated and with feeling anxious (the latter was significant in all groups but the severe).
Significance of results
Z-tests showed that differences in percentages reporting the outcomes between exposed and non-exposed are statistically significant in most instances. Non-statistically significant differences were only observed in the severe and moderate disability groups, whose lower number of respondents reduced the statistical power of the test. Even in those cases, the direction of the difference is in most cases consistent with the hypothesis of an association between care disruptions and negative self-reported impacts.
Discussion
Early results of AISM’s survey about the impact of COVID-19 pandemic on the lives of PwMS in Italy show that, as a result of the pandemic, many reported not receiving their usual level of care. The reasons for this are twofold. First, many providers rescheduled or cancelled appointments. 13 Second, as many PwMS had to choose between receiving care and reducing risk of contracting the virus, it is likely that some eventually chose to avoid face-to-face contact with care staff altogether.
Both PwMS and their carers compensated for this reduction in usual care, but not without personal consequences. In several cases, PwMS resorted to rearranging their care using personal resources. Similarly, the lack of usual care and support often meant additional burden and stress for their carers - most commonly in those of PwMS with severe disability. Previous research shows that the families of PwMS in Italy, especially those of older and most severe patients, often bear a substantial proportion of both the financial and the informal care burden.7,18 Participation of families in the care of persons with chronic conditions is very common in the Italian system, and is known to be a contributor to financial disadvantage and gender inequalities.19,20 This type of care overload appears to have been exacerbated by the pandemic.
The pandemic and the lockdown had apparent detrimental impacts on the self-reported psychological wellbeing of many PwMS. Difficulties in obtaining psychological support were, quite predictably, a factor strongly associated with all outcomes considered here. Not receiving specialist services, usual care and support and rehabilitation therapy were also associated with negative psychological outcomes. The association between care disruptions and apparently unrelated aspects of wellbeing supports evidence promoting a person-centred multi-disciplinary therapeutic strategy in provision for MS.3,4,21 This possibly further underscores the value of a holistic approach to care, as it suggests that missing one component of care can have a knock-on effect in other facets of health and wellbeing.
Early therapy and regular monitoring are crucial in the treatment of MS and in delaying its progression.1,5,22 The prognosis of PwMS with milder disability is therefore dependent on timely receipt of care. This resonates with fears of MS progression being very common among respondents who have missed health care and rehabilitation therapy, not only in the groups with more severe disability, but also in those with minimal and mild disability. Moreover, PwMS at the early stages of the disease are particularly vulnerable from a psychological point of view, 23 not only because depression and anxiety are common comorbidities of MS, but also because they are likely to have been recently diagnosed and thus still coming to terms with their shattered life plans. 24 Therefore, it is perhaps unsurprising that this group of patients indicated in higher proportions that they felt anxious because of the COVID-19 pandemic, as well as the fact that broad consequences were associated with a lack of usual psychological support during this period.
Feeling abandoned was reported by lower proportions of PwMS overall, yet those responses flag a profound unease, which was much more common among respondents who could not receive specialist health care and psychological support. These PwMS felt left alone to face the emergency and the uncertainty arising from it without the professionals and providers usually responsible for both their physical and psychological wellbeing.
Many respondents also indicated that they had to decide between receiving care and protecting themselves against the risk of infection. This suggests that, despite the timely publication of guidelines from the Italian Neurological Society 25 and the efforts reportedly made by many MS clinical centres to offer care remotely, 15 respondents could not access expert guidance in deciding what behaviour would be the safest for them, and that many providers could not ensure minimization of risks.
Limitations
There are two main limitations of this study. The first is the self-selecting nature of the sample. This means the sample may not be representative of all PwMS in Italy. However, this study did have a relatively large sample size, which gives us confidence regarding the robustness of the results.
Second, the data are of disruptions and impacts at a single point in time. This reduces the scope for attributing causality, as what came first between disruptions and impacts cannot be established. Plausibility and coherence of the causal pathway strongly support the hypothesis that disruptions are likely to have caused the outcomes. In any case, for the descriptive purposes of this study it is not essential to establish causation with certainty. Either disruptions in care worsen conditions, or PwMS with more pressing needs did not receive an adequate response in the health and care system. Both of these scenarios raise the same concerns and questions from a health and social care policy point of view. Observing that the two were reported by the same PwMS, and not due to chance, is the key finding of this study.
Conclusions
The observed association of care discontinuities with negative consequences for health and psychological wellbeing supports continuity of prompt, accessible, integrated, and multi-disciplinary care for PwMS during times of emergency. As the conditions of PwMS range from full autonomy to severe impairment, findings regarding ways in which the pandemic affected their care and their wellbeing may be generalizable to a larger number of persons with chronic conditions, who are likely to have experienced similar difficulties and impacts. Disruptions in the provision of care, dilemmas between receiving it and strict self-isolation, fear of the clinical consequences of delayed care, anxiety, and possibly feeling left alone in trying to cope, were most likely shared experiences with many other ill and vulnerable people, in many countries around the world during the pandemic. In fact, similar risks posed by the pandemic and by the clinical response have been noted for several other diseases, including other neurodegenerative conditions, 26 diabetes 27 and cancer. 28
Health systems’ responses to COVID-19 have often been dictated by emergency conditions. This was particularly so in Italy as it was the first country hit in Europe and was caught very much by surprise by the outbreak. The race to secure capacity to treat prioritised COVID-19 patients9,13 left little leeway to develop and implement consistent strategies to ensure continuity of care for persons with chronic conditions. At the time of the outbreak, the latest edition (2016) of the Italian national influenza pandemic response plan did not include any such strategies, 29 therefore updating it would be imperative. The reported adoption of remote care in Italian MS clinical centres 15 could be implemented more widely and possibly combined with empowerment and other training programmes for patients and carers.
Alongside improving providers’ preparedness to deliver care in person safely during a lockdown, remote access may improve communication of risks and support care continuity while minimizing need for physical proximity between patients and care staff. Such an approach could be adopted for a broad range of chronic conditions beyond MS. This may ensure that the needs of persons who rely on regular health and social care services 30 are better met in the next stages of the COVID-19 pandemic, as well as possibly in future pandemics and other emergencies.
Footnotes
Authors' note
The study was carried out by AISM using its own resources.
Acknowledgements
The research team wishes to thank all the people with MS that participated in the study, AISM staff who helped them to complete the questionnaire over the phone, and everyone at AISM who contributed, in particular Marcella Mazzoli, Giorgia Franzone, Linda Brozzo and Michele Messmer who provided insight and suggestions in developing the questionnaire. The team also wishes to thank Bob Erens and Lavanya Thana at LSHTM for their help and methodological support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Authors declare that all the research meets the ethical guidelines.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.