
Abstract
Deploying knowledge brokers to bridge the ‘gap’ between researchers and practitioners continues to be seen as an unquestionable enabler of evidence-based practice and is often endorsed uncritically. We explore the ‘dark side’ of knowledge brokering, reflecting on its inherent challenges which we categorize as: (1) tensions between different aspects of brokering; (2) tensions between different types and sources of knowledge; and (3) tensions resulting from the ‘in-between’ position of brokers. As a result of these tensions, individual brokers may struggle to maintain their fragile and ambiguous intermediary position, and some of the knowledge may be lost in the ‘in-between world’, whereby research evidence is transferred to research users without being mobilized in their day-to-day practice. To be effective, brokering requires an amalgamation of several types of knowledge and a multidimensional skill set that needs to be sustained over time. If we want to maximize the impact of research on policy and practice, we should move from deploying individual ‘brokers’ to embracing the collective process of ‘brokering’ supported at the organizational and policy levels.
Background
The gap between research evidence and its use in clinical practice, often described as a ‘know-do gap’, 1 is well documented. 2 One of the ways of bridging this gap is the creation of knowledge brokering roles, such as knowledge transfer associates, diffusion fellows, or knowledge exchange officers. Knowledge brokers are individuals that bridge a gap in social structure and help knowledge flow across that gap by enabling translation, coordination and alignment between different perspectives and facilitating transaction between previously separated practices. 3 They may come from a range of backgrounds, including clinical professions, 4 managers 5 and researchers. 6 The knowledge brokering role has been described as complex, diverse and contextual, 7 with brokers operating as ‘knowledge managers’, ‘linkage agents’ and ‘capacity builders’. 8 In the context of health care, they are expected to promote interaction between researchers and practitioners, enabling the mobilization of research evidence into clinical practice9,10 and policy making.2,11
Following the pioneering work of the Canadian Health Services Research Foundation, 1 knowledge brokering has turned into an ‘industry’, with knowledge brokers increasingly employed by collaborative research partnerships, inter-organizational networks and other organizations.7,9 Many commentators view the knowledge broker as an unquestionable enabler of evidence-based medicine, enhancing the flow of knowledge between researchers and practitioners. 11,12 There are calls for use of brokers at the national level and even internationally, across European health systems. 12 At the same time, there is growing evidence about the unintended consequences of deploying knowledge brokers in health care,3,9,13,14 which are often overlooked.
Without questioning the theoretical foundations of knowledge brokering as an ‘organic’ way of bridging the gap between separate communities of practice, 15 we aim to provide an analysis of its ‘dark side’, which can be defined as a set of secondary consequences of a purposive intervention that run counter to its objectives, 16 and suggest a way forward. Rather than presenting a formal literature review, we draw on a broad range of recent empirical studies that discuss the challenges and unintended consequences of deploying knowledge brokers in the public sector, as well as on our personal experiences as practitioners of knowledge mobilization in healthcare. We believe that highlighting these issues is useful for informing future research into knowledge brokering as well as for maximizing its positive impact on policy and practice.
Tensions between different aspects of knowledge brokering
Aspects of knowledge brokering and skills required for their realization.
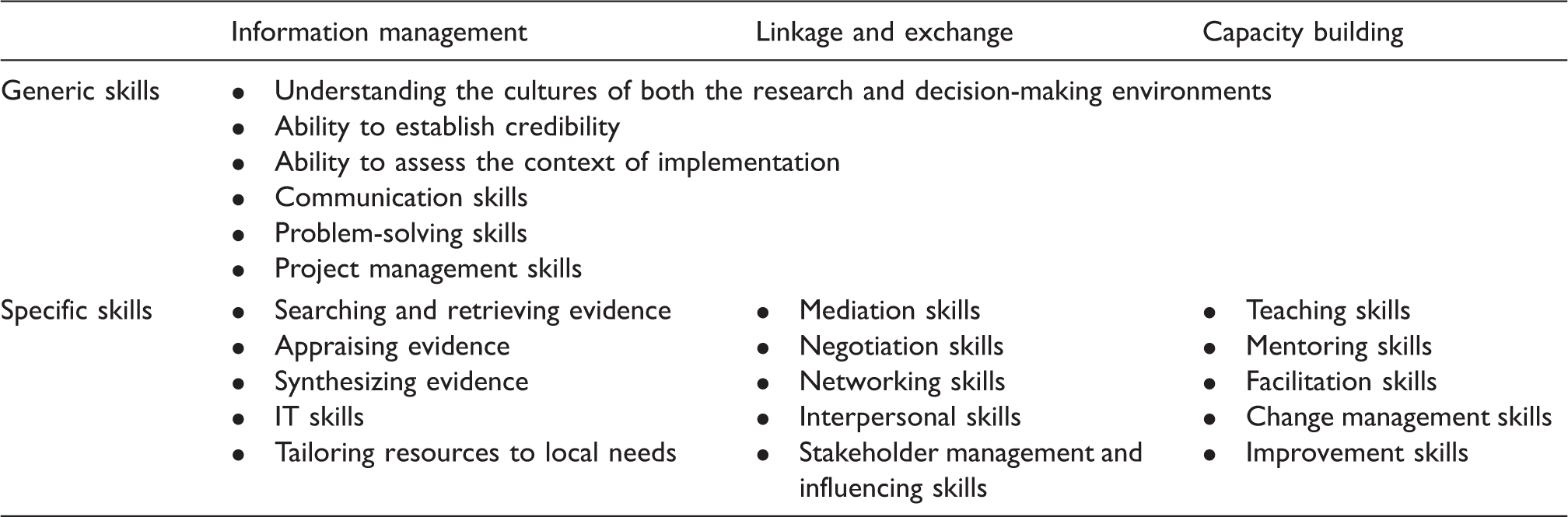
In an ideal world, these aspects of brokering are expected to complement each other, but in reality there are often tensions between them.3,17 Linkage and exchange and, particularly, capacity building may receive less attention because these activities are often more time-consuming, resource-intensive and difficult to capture than information management. Due to their focus on codified knowledge, information management activities are more amenable to standardization, with their measurable outcomes often being directly aligned with performance targets at local and national level. 3 Within a capacity building role, knowledge brokers possessing clinical expertise may be at risk of switching from ‘facilitating’, i.e. enabling their peers to mobilize evidence in practice, to ‘doing’, when they implement change on their own, with limited learning within a health care organization. 3 In one of the recent studies, specialist nurses seconded as knowledge brokers found it much easier to conduct an electronic audit of primary care chronic disease registers (which can be classified as ‘information management’) themselves than enable clinicians to change their practice based on the result of the audit. As a result, the formal objectives of the improvement project, aligned with the clinical performance targets, were met but it is questionable to what extent the expert knowledge of specialist nurses was transferred to primary care clinicians and to what extent the resulting improvement was sustainable. 18
Tensions between different types and sources of knowledge
According to Gabbay and le May, 19 rather than relying on clinical guidelines in their decision-making, doctors use clinical ‘mindlines’ – collectively constructed, internalized, tacit guidelines which are mainly informed by their own clinical experience as well as by informal interactions with their peers, patients, local opinion leaders and pharmaceutical representatives. It is therefore not enough for knowledge brokers to have a good understanding of research evidence codified in the form of guidelines, protocols and pathways. Regardless of their professional background, they also have to possess at least some clinical knowledge in order to understand the implications of evidence for clinical practice and acquire credibility with practitioners, managerial skills enabling them to effectively connect with and influence people and manage projects, and contextual knowledge about cultures, policies, processes and people in the health care context. 5 Similarly, recent research has shown that ‘knowledge’ being brokered is not limited to codified research evidence but represents ‘bundled action proposals’, 2 involving actionable ideas about how clinical guidelines (scientific knowledge) could be applied in practice (clinical knowledge) taking the features of the health care context (contextual knowledge) into account. 3
The need to balance different types of knowledge originating from multiple (and often competing) 2 sources raises important practical questions. How to make sure that knowledge brokers take into account both written, explicit knowledge of evidence with the unspoken, taken-for-granted knowledge of the ‘mindlines’? What skills are most important for a knowledge broker? Clinicians deployed as knowledge brokers are likely to possess credibility, knowledge of guidelines and understanding of the health care context. 20 At the same time, they may not be very familiar with managerial techniques 21 and, as discussed above, can easily switch from ‘facilitating’ to ‘doing’, undermining the idea of bridging the gaps between different groups. In addition, nurses and allied health professionals may struggle to broker clinical knowledge to doctors.3,5 Managers, on the other hand, lack clinical expertise and may struggle to appraise evidence, which can limit their credibility with clinicians.5,20 Finally, researchers have a vested interest in the process of research production, with their priorities often being markedly different from those of the practitioners 22 or commissioners of research, 23 and may fail to recognize the complexities of clinical care and health care policy making. 6
Tensions resulting from the ‘in-between’ position of brokers
It is exactly the in-between, intermediary position of knowledge brokers that enables them to bridge gaps and connect previously separated communities. 1 It also helps them better understand the perspectives held by the multiple groups and organizations they are working with, acting as a ‘catalyst for change’ in the practices of knowledge recipients. 8 Occupying an intermediary position requires maintaining a certain degree of neutrality and equanimity in navigating contextually sensitive environments, dealing with conflicting perspectives and negotiating feasible responses to diverse stakeholder needs.8,9 Knowledge brokers have been described as individuals who belong to and are being seen as credible in several communities. 15 When it comes to mobilizing evidence into practice, they should therefore be able to relate both to the world of research and the world of practice.
At the same time, ‘in-betweenness’ is characterized by a high degree of ambiguity and instability. First, there is an inevitable tension between the ‘in-betweenness’ and embeddedness. The latter is required for developing a deep understanding of the context and gaining credibility but may involve prioritizing one of the communities and its interests. 9 For instance, deployment of researchers as knowledge brokers can reinforce the boundary between the producers and users of research, creating the ‘us and them’ situation. 24 Second, rather than belonging to both communities, knowledge brokers are at risk of being perceived as belonging to neither. In some of the recent studies, individual knowledge brokers report hostility and scepticism from other professionals, and can occasionally feel isolated and incompetent among them.4,14 Finally, brokering can be a low priority for organizations which prefer to allocate most resources to their ‘core’ business, giving little support, reward and recognition for intermediary roles.12,13 Knowledge brokers often experience lack of role clarity and guidance,13,14 with no established career path, and limited opportunities for promotion.9,17,25
Unintended consequences
Delegating brokerage to specially designated individuals makes mobilization of knowledge into action highly contingent on their individual preferences, connections and skills. This may result in bottlenecks and blockages in the flow of knowledge, and prevent the development of brokering as an important organizational capability. 26 Organizations can also experience difficulties recruiting and retaining knowledge brokering staff. Clinicians, managers and researchers may choose to abandon their brokering responsibilities in favour of more traditional roles giving them a higher degree of credibility and job security.4,21,25 This raises questions about continuity and sustainability of change: if a broker leaves, his or her knowledge and skills can be lost to the organization.4,9
Sustainability can also be compromised if ‘knowledge’ is narrowly seen as ‘research evidence’ (What evidence is to be brokered?) with little attention being paid to other forms of knowledge (What contextual knowledge and managerial skills do knowledge recipients need to mobilize research evidence in their day-to-day practice? How to broker different forms of knowledge to this target group in this setting?). 27 Failing to adequately address these questions can result in a loss of credibility, damage engagement with practitioners and significantly decrease the impact of research evidence on decision-making. All these factors can lead to a situation where the brokered evidence is made available (‘transferred’ or ‘translated’) to knowledge recipients without being taken up (‘mobilized’ or ‘implemented’) in practice. In other words, knowledge brokers may be at risk of failing to broker knowledge, with the latter being lost in the ‘in-between world’.
From individual ‘brokers’ towards collective ‘brokering’
Addressing the tensions in knowledge brokering by adopting a team-based approach.
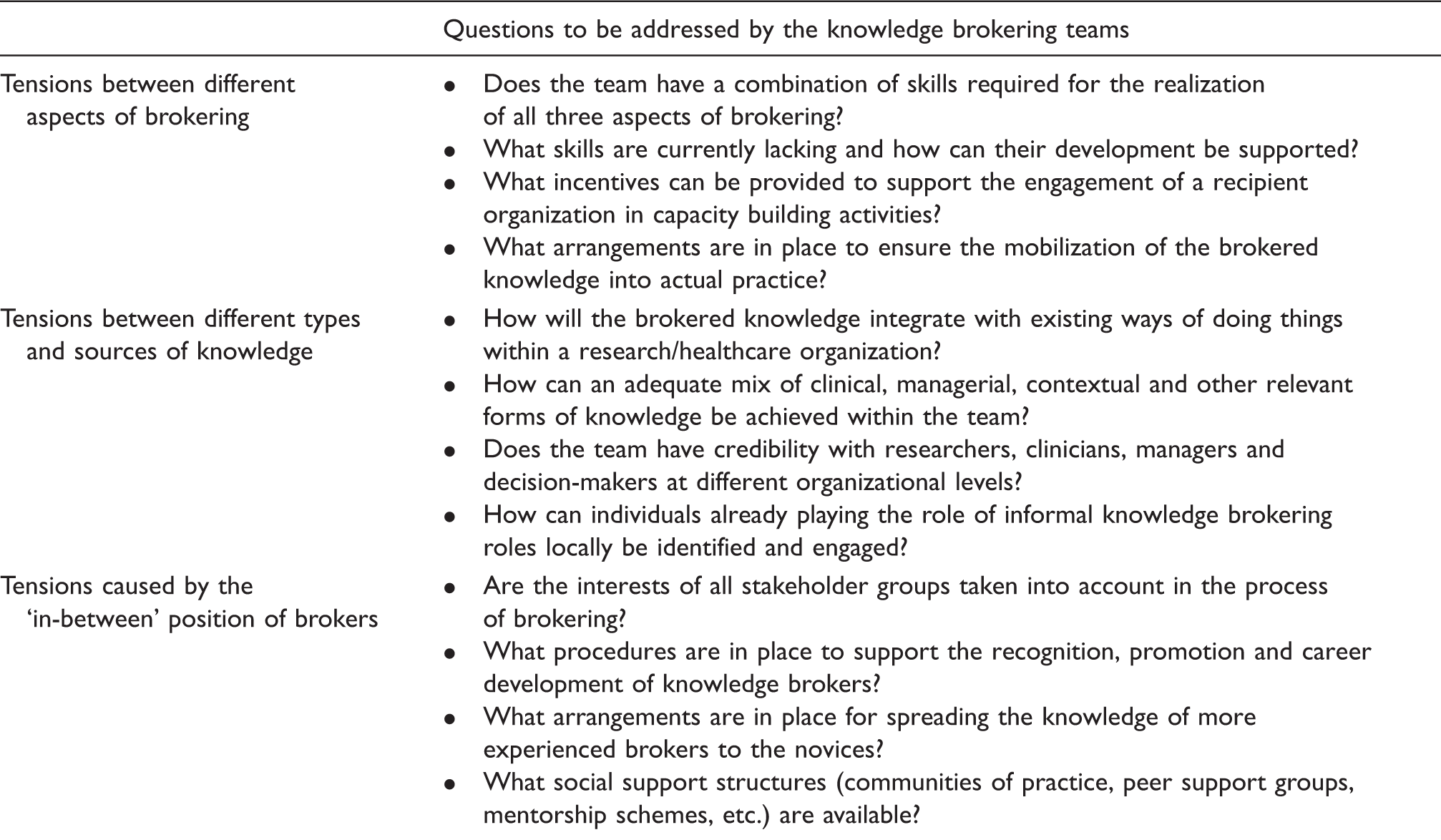
The first step in this direction is to foster brokering teams composed of people with different professional backgrounds and having complementary skills. These skills should combine those needed for successful information management, linkage and exchange, and capacity building with broader clinical, managerial and contextual knowledge. This may be achieved by the involvement of academics, clinicians, managers, information scientists and service users. 10 The composition of the knowledge brokering teams should enable them to gain credibility not only with multiple professional groups but also at different organizational levels. This would require an active engagement of knowledge recipients in the process of evidence-informed organizational change, which is likely to be contingent on the alignment between the content of a knowledge brokering intervention and the priorities of the recipient organization. 3
Second, organizations deploying knowledge brokers should recognize brokering as part of their ‘core’ business, providing a range of learning, development and promotion opportunities to staff occupying the ‘in-between’ roles. 9 Supporting the knowledge brokers’ communities of practice and creating regional or national forums for staff occupying intermediary roles can help alleviate their sense of isolation and enable peer-to-peer learning. As an alternative to full-time brokering posts, knowledge brokering activities can also be supported as part of a wider, more traditional professional or managerial role. In addition to the formalized knowledge brokering roles that will need time to acquire sufficient credibility, it is also crucial to identify those representatives of the managerial, clinical and/or research communities that are already playing the role of informal knowledge brokers locally. Such informal brokers often operate in ‘broker chains’, 5 engaging with which can enable an integration of formalized and informal brokering activities and increase the sustainability of evidence-informed change in the recipient organizations.
Knowledge brokering in the broader policy context
The growing investment in inter-organizational knowledge mobilization networks and collaborative research partnerships, such as the Collaborations for Leadership in Applied Health Research and Care (CLAHRCs) in England, creates favourable conditions for fostering collective knowledge brokering arrangements. 27 The CLAHRCs have built a cadre of experienced knowledge brokers, acting as ambassadors of knowledge mobilization, and contributing to a new culture of inclusive and impactful research.25,27 Their knowledge brokering functions are often shared among the members of multiprofessional teams,10,25 with a growing recognition of the broader networks in which the brokers are embedded. 25,27 At the same time, collaborative research partnerships are often seen as external ‘academic machines’, 27 with their fragmented design and focus on research production occasionally reinforcing the boundaries between the generation of evidence and its application. 22 Given the recognized need to develop the internal knowledge mobilization capacity of health care organizations, the impact of collective brokering structures could be further strengthened by a broader inclusion of research users in the processes of brokering and co-production, aiming at mobilizing knowledge that would be useful for their particular local situations.
The realization of this shift would face a number of deep-seated structural macro-level obstacles identified in the previous analyses of efforts to promote knowledge exchange between research and practice.2,17,23 An increasing emphasis on performance management and the divergence of priorities between the academia and the ‘real world’, especially in the context of limited resources, represent powerful institutional pressures leading to the marginalization of knowledge brokering and other boundary bridging interventions in public sector organizations. Knowledge brokering is a costly and resource-intensive strategy 8 ; implementing it properly and making it ‘everyone’s business’ requires substantial organizational commitment and investment. Unless the broader policy context is modified accordingly, with the introduction of incentives stimulating the strategic, reflective and long-term engagement of researchers and practitioners in knowledge mobilization activities, knowledge brokering is likely to remain confined to specialized intermediary organizations and fail to realize its full potential in bridging the ‘know-do gap’.
Conclusion
Deployment of knowledge brokers is widely promoted as an enabler of evidence-based practice, with relatively little attention paid to its ‘dark side’. This analysis shows that knowledge brokering is a multidimensional process involving the use of several types of knowledge and skills. Its impact on the mobilization of research evidence into decision-making and clinical practice may be affected by a number of tensions, some of which reflect the inherent complexity of knowledge and brokering while others stem from the ‘in-between’ position occupied by brokers. We suggest that creating isolated knowledge brokering roles is not enough to produce sustainable impact on the ‘know-do gap’ and advocate shifting from individual ‘brokers’ to collective ‘brokering’, implemented by multiprofessional teams and supported at the organizational and policy levels.
Our analysis also opens a number of new directions for empirical research. While the literature is pre-occupied with cataloguing various activities and tasks performed by individual knowledge brokers, 8 we call for exploring the mechanisms, practices and consequences of brokering as a multilevel process involving individuals, teams and organizations. How do knowledge brokering teams and organizations deal with the multiple tensions described in this essay? How do successful ‘broker chains’ operate? What happens to new evidence, ideas and connections after they are introduced by brokers? How do brokers enable the recipient organizations to absorb and utilize knowledge? How do knowledge brokering practices evolve over time? Given the diversity, complexity and contextual nature of brokering, we need to systematically identify and critically explore those cases where knowledge brokering interventions had a positive and sustainable impact in order to understand what makes these interventions effective in particular settings.
Footnotes
Acknowledgements
The authors thank Dr Vicky Ward, Dr Robin Urquhart and two anonymous referees for their helpful comments on the earlier versions of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received funding from the National Institute for Health Research Collaboration for Leadership in Applied Health Research and Care (NIHR CLAHRC) Greater Manchester. The views expressed in this article are those of the authors and not necessarily those of the NHS, NIHR or the Department of Health.