
Abstract
Objective
This scoping review aimed to map the literature on knowledge mobilization (KMb), the reciprocal exchange of knowledge and expertise among key partners to bridge research and practice, in the childhood cancer community, identifying key needs, barriers, facilitators, and alignment with the knowledge-to-action (KTA) framework.
Methods
A comprehensive search was completed across Medline, Scopus, and ERIC. Data on study characteristics, KMb categories, barriers/facilitators, and KTA approaches were extracted and analyzed.
Results
A total of 2522 unique articles were identified, of which 77 met the inclusion criteria (1988–2024). Most studies were conducted in high-income countries (n = 54, 70.1%), with 5.2% from lower-middle-income countries (n = 4) and none from low-income countries. Collectively, 27,888 professionals and 50,786 patients were included in the studies. Four key categories resurfaced for KMb needs in this community: information and communication; medical management; training and education; and supports. Categories related to barriers and facilitators for effective KMb include information complexity and standardization; technical challenges to KMb; staff resistance and engagement; resource limitations; cultural and social factors; caregivers’ and parents’ values; and time constraints. While 76.6% of studies (n = 59) proposed KMb interventions, fewer than 20% (n = 14, 18.2%) offered evidence of sustaining knowledge use over time.
Conclusion
The state of the literature indicates that the childhood cancer community faces complex KMb needs and barriers. Future research and innovation should focus on patient and family engagement, address socioeconomic and cultural disparities, and explore how technology can enhance KMb, practice, and policy.
Keywords
Introduction
Globally, more than 1000 children are diagnosed with cancer every day, and as low as 20% survive in low- and middle-income countries. 1 In Canada, pediatric cancers accounts for ∼2% of all cancer diagnoses, with an estimated 3950 cases annually among children and adolescents, and young adults. 2 Advances in treatment have significantly improved one-year survival to 93% and five-year survival to 84% in high-income countries between 1992 and 2017. 2 Despite these improvements in high-income countries, childhood cancer remains a profound challenge for children and their families, especially in low- and middle-income countries. Healthcare professionals, researchers, policy-makers, and pediatric oncology community members also face the ongoing difficult task of translating rapidly evolving evidence into practice to deliver the highest standards of care. 3 Knowledge mobilization (KMb) is a reciprocal exchange of knowledge and expertise among key partners, which is essential to bridge research and practice, 4 helping to ensure improved care. There is an increasing global focus on leveraging KMb activities to enhance practice and policies. 4 It is estimated that cancer outcomes could be improved by 30% by optimally applying up-to-date evidence-based knowledge to practice. 5 KMb in the pediatric oncology context may include, but is not limited to, mobilizing new treatment protocols, evidence-based symptom management strategies, psychosocial support interventions for patients and families, and emerging evidence on survivorship care.
KMb covers a range of activities for producing and using research, such as synthesis, dissemination, transfer, exchange, and co-creation between researchers and users. 6 However, despite this increasing attention, the process of mobilizing knowledge to achieve meaningful impact remains slow and unpredictable. 4 General challenges to KMb include a lack of resources, a lack of KMb skills, and a disconnect between organizational mission and actual practices. 4 Conceptual models, such as the knowledge-to-action (KTA) framework, have been used to help accelerate KMb in healthcare,3,5 with particular recent interest in pediatrics. 7 First, the KTA framework helps knowledge move through the knowledge creation cycle, which consists of three steps: knowledge inquiry, synthesis, and production tools.3,5 Second, the action cycle helps apply knowledge in seven steps encompassing initial problem identification to sustain knowledge use.3,5 In the context of the childhood cancer community, there is a lack of understanding regarding the current state of KMb, including the specific needs, barriers, and facilitators that influence this process.
The primary aim of this scoping review was to map the existing state of KMb, including the needs, barriers, and facilitators, documented in the empirical literature for the childhood cancer community, helping set the stage for informing policies, improving practice, and advancing research aimed at improving outcomes and quality of life for children with cancer and their families. The secondary aim of this review was to assess the current literature's alignment with the KTA framework.
Methods
The Arksey and O’Malley 8 and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses scoping review (PRISMA-ScR) 9 checklist guided this scoping review (Supplemental 1, Table 1).8,9
Information sources and search strategy
A review of major medical and education databases, including Medline (OVID), Scopus, and ERIC (EBSCO), were conducted in consultation with a research librarian. For each database, specific terms were used to address the concept of KMb, pediatrics, and cancer (Supplemental 2, Tables 1 to 4). The first concept of KMb included allied concepts of knowledge translation, knowledge transfer, knowledge brokering, knowledge management, knowledge utilization, and knowledge action or dissemination. The second concept included terms of neoplasm, cancer, and oncology. The third concept included the search terms pertaining to childhood and pediatrics. Medical Subject Headings (MeSH) terms and exploded commands were employed where applicable to optimize the search. In addition, a reference sampling technique was used to ensure thoroughness. The initial search strategy was conducted on 7 June 2024. The search strategy was repeated on 1 February 2025 to help identify salient new literature.
Eligibility criteria
Inclusion criteria included English or French language, peer-reviewed empirical literature of primary studies with no date restriction pertaining to KMb in pediatric oncology. All facets of KMb were included, including synthesis, dissemination, transfer, exchange, and co-creation. All umbrella terms that fall under KMb were also included, such as knowledge translation, knowledge transfer, knowledge brokering, knowledge management, knowledge utilization, and knowledge action or dissemination. Exclusion criteria included non-primary literature, such as reviews, commentaries, editorials, conference proceedings, expert census, ongoing studies, study protocols, and gray literature, such as textbooks, pre-prints, or graduate theses. Translational medical findings focusing on laboratory biological advances were excluded. Further details are outlined in Supplemental 2, Table 1.
Data charting and data items
A reviewer (SM) evaluated each study for eligibility using the Covidence Systematic Review Software (Veritas Health Innovation, Australia). 10 The screening process consisted of an initial review of titles and abstracts, followed by a detailed examination of the full text for studies meeting the inclusion criteria. Consistent with the medical education literature, a second reviewer (AT) verified a portion of the papers with the goal of 90% or better agreement in full-text. 11 Any disagreements were resolved through direct discussions and consensus. For studies deemed eligible, data extraction was conducted by one reviewer (SM). Extracted data included the study title; publication year; country; country income status based on World Bank classification 12 ; study design; study aims; oncology sub-field by disease type or population type, where applicable; sample size and characteristics; recruitment methods; knowledge intervention, tools and instruments; knowledge needs identified; key findings of studies; key partners addressed; barriers and facilitators to KMb; recommendations from authors; and sustainability considerations. The extracted data were analyzed descriptively using Microsoft Excel (Microsoft, United States) 13 and synthesized narratively using content analysis. 14 Each study's alignment with the KTA framework was assessed using the KTA framework knowledge creation and action cycles (Supplemental 3, Table 1). 3
Role of the funding source
This review was conducted in the context of the KMb Group on behalf of the ACCESS (Accelerating Childhood Cancer Experience, Science & Survivorship) network, supported by the ACCESS Secretariat and the Canadian Institutes of Health Research (CIHR funding reference number 184352). The ACCESS group allowed for a research stipend for research members (SM, SAC, and GL) and performed an initial peer review of the manuscript prior to publication. Two of the study authors (SAC and GL) are persons with lived experience of pediatric and young adult cancers. The principal investigator is a Junior 2 Research Scholar, Fonds de Recherche du Québec – Santé (FRQS).
Results
Characteristics of studies
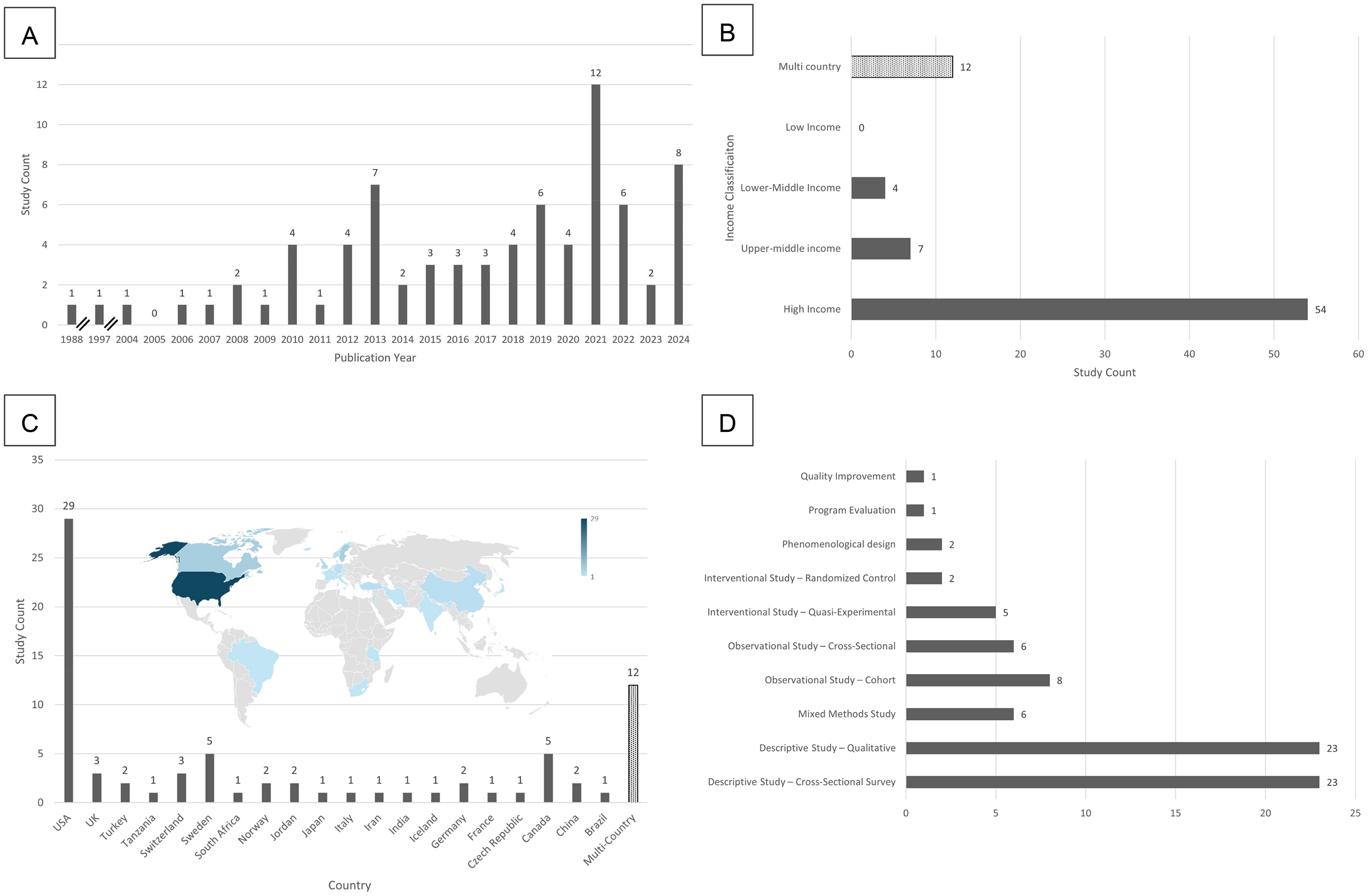
A total of 2522 unique articles were identified across three databases and reference sampling, following duplication removal by Covidence Software (Figure 1). Of these, 77 studies published between 1988 and 2024 met the eligibility criteria and were included in this analysis (Supplemental 4, Figure 2a).15–91 The year following the start of the COVID-19 pandemic (2021) witnessed the most scholarly articles published than any other year (n = 12, 15.6%).33,35,37,55,63,64,66,68,70,73,75,86 Collectively, the studies included 27,888 professionals, 50,786 pediatric patients, 1467 parents or caregivers, and 247 families (Supplemental 3).15–91 A total of 201,298 written website or social media content and 149 videographic content found on video-sharing platforms were included in the primary articles.23,31,39,40,51 Fifty-four studies (70.1%) were conducted in high-income countries,16,19,21,23,2527–31,33,35,37–45,47–50,52–59,61–64,67,70–74,77–81,83–85,87–89 followed by upper-middle (n = 7, 9.1%)18,26,32,60,82,90,91 and lower-middle income countries (n = 4, 5.2%)36,65,75,86 (Figure 2b). 12 There were no studies from low-income countries. Twelve studies were multi-country collaborations (15.6%) (Figure 3c).15,17,20,22,24,34,46,51,66,68,69,76 Over a third of the studies were published in the United States (n = 29, 37.7%),19,21,25,28,30,33,3537–41,44,45,50,52,55,59,61–64,67,70,71,74,78,85,87 followed by Canada (n = 5, 6.5%)29,80,81,83,84 and Sweden (n = 5, 6.5%).16,43,47,72,89 Over half of the studies were descriptive in nature (n = 46, 59.7%), particularly cross-sectional surveys (n = 23, 29.9%)24–26,29,30,34,37,38,42,46,48,50,52,56,57,59,63,65,71,75,78,80,91 and qualitative studies (n = 23, 29.9%) (Figure 2d).16,18,19,21,27,33,3639–41,51,53,54,64,69,70,76,79,81,82,87,88,90 Fourteen studies were observational (18.2%), namely prospective or retrospective cohorts (n = 8, 10.4%)17,23,47,49,58,83,85,86 and cross-sectional (n = 6, 7.8%).31,44,5566–68 Seven studies were interventional (9.1%), quasi-experimental (n = 5, 6.5%),32,43,45,77,84 and randomized control (n = 2, 2.6%).20,89 Six were mixed-methods studies (7.8%).28,35,61,62,72,73

PRISMA flow diagram. 96
Study characteristics (n = 77).

Thematic analyses on knowledge mobilization in childhood cancer (n = 77).
We systematically coded each study to indicate whether it encompassed all cancer types (general pediatric oncology) or focused on a specific disease subtype or area of expertise. The largest proportion of studies (n = 37, 48.1%) addressed general pediatric oncology (Table 1).15,17,19,21,22,24,25,27,29,30,35,37,41,43,44,4850–52,56–62,65,67,71–73,75,77,81,87–89 Six studies focused on the field of pediatric palliative care and pain management (n = 6, 7.8%).34,36,38,74,80,84 Studies on survivorship and late effects of childhood cancer accounted for 6.5% (n = 5).42,49,69,78,85 Four studies focused on adolescent and young adult (AYA) oncology (5.2%).18,20,33,76 Pediatric cancer psychology and mental health accounted for 5.2% (n = 4).28,45,46,83 Studies with a caregiver focus encompassed 3.9% (n = 3).82,90,91 Other notable areas of focus include leukemia (n = 3, 3.9%),32,39,40 lymphoma (n = 2, 2.6%),53,54 central nervous system tumors (n = 2, 2.6%),16,47 COVID-19 (n = 2, 2.6%),66,68 and oncology system informatics (n = 3, 3.9%) (Table 1).55,64,70 Over three-quarters of the studies proposed a KMb intervention (n = 59, 76.6%), and 18 (23.4%) did not specify a specific intervention.16,18,19,2325–27,29,30,33,37,39–42,87,88,90
Pediatric oncology knowledge mobilization (KMb) focus areas (n = 77).

KMb needs
Four primary categories for KMb needs emerged from the analysis with varying levels of emphasis (Figure 3a; Supplemental 5, Table 1). Information and Communication (n = 59, 77%) was the most common category,16,18,1921–24,27,30–32,35,37,39–42,44–48,50–52,55–72,74–79,81–83,85–91 followed by medical management (n = 20, 26%),15–18,21,25,33,34,36,42,43,53,54,58,59,69,79,80,84,88 training and education (n = 18, 23%),20,25,2628–30,34,36–38,53,54,63,64,75,79,80,84 and supports (n = 16, 21%).26,28,32,39,46,49,5171–76,82,83,87
Information and communication
Five sub-categories were identified: a need for multiple and accessible information formats; the importance of up-to-date and accurate pediatric oncology information; the necessity of clear and culturally appropriate communication; the need for better diagnosis communication; and the call for centralized and harmonized data sharing. Akkawi El Edelbi et al. 16 highlighted the need for written instructions, movie clips, and oral communication delivered to the parents and caregivers in their native language, with repeated, non-conflicting messages to reinforce understanding of drug management. Baker et al. 19 stressed the importance of providing information to patients and their parents using multiple methods, avoiding medical jargon, and allowing adequate time for decision-making. Cederved et al. 89 noted that providing radiotherapy education to children via gamification helped reduce anxiety. The demand for up-to-date and accurate information in the pediatric oncology field was also noted. Berg et al. 22 discussed the need for mobile-accessible, real-time information to support treatment decision-making for patients and parents. Bejjani et al. 21 highlighted the need for accurate oncology-related information between professionals during the COVID-19 pandemic. Bahrami et al. 18 emphasized the importance of clear, gradual information-sharing based on an adolescent's cognitive capacity. There is also a need to improve the communication of diagnoses to patients and their families. Bahrami et al. 18 stressed the importance of transparent and gradual information-sharing about diagnosis. This extends to the long-term implications of diagnostic findings, including late effects—a gap highlighted by Mayer et al. 61 and McClellan et al. 62 Mohan et al. 65 highlighted the need for culturally appropriate communication when revealing a cancer diagnosis to patients and families. The need for centralized and harmonized data sharing emerged as a sub-category. Ma et al. 55 called for centralized, harmonized, and accessible systems to improve the flow of clinical information across electronic medical records and help develop harmonized databases of clinical, outcome, and genomic data. McLeod et al. 64 further emphasized the need for harmonized genomic data to enhance research and clinical operations.
Medical management
Three sub-categories were identified: the need for improved care and transition planning; the necessity of addressing gaps in symptom management; and the importance of involving families and patients in care decisions to enhance medical management outcomes. Nandakumar et al. 59 and Marchak et al. 69 emphasized the importance of transition processes and accessible survivorship care plans. Bloomhardt et al. 25 and Finley et al. 36 stressed better management of symptoms like chemotherapy-induced nausea and vomiting, and pain. Involving families and patients in care decisions emerged as a key sub-category for improving medical management outcomes, with Gilljam et al. 43 and Gibson et al. 88 underscoring the importance of family and patient engagement throughout the management of childhood cancer.
Training and education
The major sub-categories identified in the literature highlight the need for provider-specific education and skill development. Bloomhardt et al. 25 highlighted the importance of educating healthcare providers on clinical practice guidelines for managing chemotherapy-induced nausea and vomiting based on provider perception. Clayton et al. 29 and Chong et al. 30 highlighted a need for training healthcare providers in fertility preservation practices, particularly for adolescent patients. Finley et al. 36 emphasized improving education on effective pain management practices. Similarly, Widger et al. 84 and Ehrlich et al. emphasized the importance of enhancing overall training in pediatric palliative care. Lie et al.53,54 highlighted the need for educating general practitioners (GPs) on late effects and comprehensive follow-up care. Frederick et al. 37 emphasized improving sexual health education and communication practices among providers. McGrady et al. 63 called for tools for providers to facilitate sexual education discussions.
Support
Two sub-categories were identified: the need for KMb for enhanced emotional and psychosocial support for parents and families; and the importance of improved communication strategies to better support pediatric cancer patients and their caregivers. Gage-Bouchard et al. 39 emphasized targeted emotional support for parents. Weidman et al. 83 stressed the need for better peer-support resources and personalized emotional support. Lau et al. 51 highlighted the importance of supportive-style messages for pediatric cancer patients and families across social media platforms, such as Twitter. Schroeder et al. 75 pointed to the need for accessible communication tools in lower-middle-income countries, such as mobile cell phones, as a tool to support patients and caregivers.
KMb barriers and facilitators
Seven primary categories emerged from the analysis with varying levels of emphasis (Figure 3b; Supplemental 6, Table 1). The main categories included information complexity and standardization (n = 61, 79.2%),16,1925–28,30–34,36–42,46–72,74–86,89–91 technical challenges to KMb (n = 26, 33.8%),16,17,28,3343–46,49,53–55,59,61,62,64,66,68,70,71,75,76,79,80,85,88 staff resistance and engagement (n = 19, 24.7%),15,17,18,22,23,25,30,35,36,43,47,48,56,57,63,69,73,74,87 resource limitations (n = 11, 14.3%),15,33,34,38,44,51,58,73,74,86,88 cultural and social factors (n = 11, 14.3%),15,18,23,52,65,67,73,81,82,87,90 parent and caregiver values (n = 9, 11.7%),18,19,24,37,45,63,79,80,82 time constraints (n = 8, 10.4%).19,28,29,35,37,77,78,84
Information complexity and standardization
Two sub-categories were identified as barriers to KMb: the lack of standardized and consistent information across healthcare providers and settings; and the challenges associated with communicating complex medical information while preventing misinformation. Akkawi El Edelbi et al. 16 highlighted contradictory information from different healthcare professionals and a lack of standardized protocols. Clayton et al. 30 and Hoven et al. 47 emphasized limited awareness and variability of existing guidelines, which affect the consistency of care delivery. Information complexity and the risk of misinformation pose significant challenges to effective communication and mobilization. Gage-Bouchard et al.40,41 and Moreira et al. 66 emphasized the proliferation of misinformation, often due to a lack of expert mediation of online resources. Baker et al. 19 identified therapeutic misconceptions and emotional stress as barriers to understanding complex medical information. Ringner et al. 72 pointed to overwhelming information and the lack of structured delivery, leading to crisis reactions and emotional stress among patients and families. Cederved et al. 89 highlighted that gamification may be an appropriate strategy for knowledge dissemination directed at children.
Technical challenges
Two sub-categories were identified: digital access and literacy barriers that limit KMb; and technical and privacy-related challenges affecting data integration within the childhood cancer community. Moreira et al. 66 and Muda and Rashid 68 discussed the challenges of varying internet access levels and the need for digital content that is tailored to recipients, including specific populations and contexts. Schroeder et al. 75 noted low literacy rates and varying phone capabilities as significant obstacles to accessing information. Issues integrating data across systems, technical complexities, and privacy-related barriers impact KMb in the childhood cancer community. Ma et al. 55 and McLeod et al. 64 identified data integration challenges and the need for robust legal data-sharing agreements to address technical complexities.
Staff resistance and engagement
Three sub-categories were identified: staff resistance due to a lack of confidence and comfort in implementing new practices; professional discomfort and negative attitudes toward knowledge sharing; and limited training and familiarity with guidelines, all of which hinder effective KMb. Staff resistance to implementing new tools or practices may stem from a lack of confidence, comfort, or perceived competence. Nandakumar et al. 69 highlighted a lack of confidence in primary care providers, which led to a reluctance to implement new practices. Rutert et al. 73 identified initial resistance to interdisciplinary collaboration as a barrier to improving knowledge flow. Professional discomfort, misconceptions, or negative attitudes hinder engagement and effective knowledge sharing. Bahrami et al. 18 emphasized the negative attitude of medical teams toward information-sharing with patients and their families, partly influenced by local cultural and contextual factors. Staff engagement is limited by a lack of familiarity with guidelines, and insufficient training opportunities affect KMb. Sawin et al. 74 cited insufficient palliative care and end-of-life communication training, leading to emotional burdens on staff and limiting their engagement.
Resource limitations
Insufficient infrastructure, physical resources, and logistical issues hinder KMb. Ehrlich et al. 34 noted limited resource access, particularly in low- and middle-income countries. Financial considerations also play a role in KMb. For example, Dornisch et al. 33 identified insurance coverage challenges and operational barriers, including the complexity of healthcare network structures, as obstacles to effective KMb.
Cultural and social factors
Variations in cultural norms, health perceptions, and communication preferences may hinder or help KMb. Watt et al. 81 identified cultural differences in health perceptions and the reluctance of healthcare providers to discuss complementary and alternative medicine. Liu et al. 90 highlighted the stigmatization of cancer-related cognitive impairment and its subsequent KMb efforts directed towards parents. Hierarchies and social dynamics within families and institutions affect information-sharing. Wegner and Pedro 82 described institutional power dynamics and cultural caregiving expectations as barriers to caregiver support and KMb. Rutert et al. 73 emphasized resistance to interdisciplinary collaboration due to institutional constraints and social dynamics within teams.
Parents’ and caregivers values
Parents and caregivers play an important role in facilitating KMb's role in the care of their child, and supporting their capacity to embrace KMb is essential. Values and priorities may differ between treating teams and families. Bilodeau et al. 24 found that parents may undervalue research results focused on quality of life, prioritizing immediate health outcomes instead. Relationships and dynamics between healthcare providers and parents may also influence KMb. Frederick et al. 37 noted that the presence of a parent or guardian during consultations sometimes created perceived discomfort for providers and patients, reducing the prioritization of sexual health discussions.
Time constraints
Insufficient time for comprehensive training or delivering knowledge affects the quality and consistency of mobilization. Widger et al. 84 pointed out variability in training implementation, with limited time for advanced module delivery. Svavarsdottir and Sigurdardottir 77 highlighted the challenge of time constraints for children undergoing active treatment, highlighting a need for brief yet effective communication interventions.
KTA framework
The 77 included studies were synthesized and mapped using the KTA framework (Figure 4; Supplemental 7, Table 1), encompassing the knowledge creation cycle and the action cycle. In the knowledge creation cycle, 26.0% of studies (n = 20) demonstrated comprehensive knowledge synthesis,15,20,34,38,44,51,5557–59,63,64,66–68,73,77,79,84,86 and 36.4% (n = 28) provided knowledge tools to facilitate implementation. 15 20–22,24,27,36,38,43–46,55,57–59,63,64,66–68,73,77,79,84–86,89 In the action cycle, 73 displayed the first step of problem identification (n = 73, 94.8%). Over a third of studies implemented knowledge interventions (36.4%, n = 28)15,17,20,28,3234–36,38,43–46,55,57,59,63,64,66–68,73,77,79,84–86,89 and monitored knowledge use (35.1%, n = 27).15,17,20,32,35,36,3844–46,51,55,57,59,61,63,64,66–68,73,76,77,79,84–86 However, only 18.2% (n = 14) of studies provided evidence of sustaining knowledge use over time.15,17,20,32,36,38,44,55,59,64,67,68,73,86 Overall, the synthesis of this primary literature revealed a misalignment across studies in how KMb is enacted within the childhood cancer community. While many studies effectively identified key needs and concerns, these often focused on the early stages of the KTA framework, specifically, the knowledge creation step of knowledge synthesis and the action cycle step of problem identification. Consequently, this reflects preparedness for action rather than the active mobilization or sustained application of knowledge. A smaller proportion of studies addressed subsequent steps, such as implementing, evaluating, or sustaining KMb interventions. This indicates that while awareness of knowledge gaps is well-documented, the formal study of the translation of synthesized evidence into practice or policy remains limited in comparison.

Knowledge to action framework analysis (n = 77).
Discussion
This scoping review explored the existing state of KMb in the childhood cancer literature, including KMb needs, barriers, and facilitators, to help guide future policy planning, practice, and research. Seventy-four empirical studies involving 27,888 professionals and 50,786 pediatric patients were included in this review. The key KMb needs in the pediatric childhood community can be clustered around the need for accessible, multifaceted communication, improved KMb focused on medical management and care coordination, enhanced staff training (especially in palliative care, late effects, and fertility preservation), and expanded psychosocial knowledge support. While most studies (n = 59, 76.6%) proposed specific KMb interventions, barriers to effective KMb included the complexity and lack of standardization of information, technical challenges, staff resistance and engagement, resource constraints, cultural and social dynamics, time limitations, and caregiver-related factors. Despite widespread identification of KMb problem areas (n = 73, 94.8%), only around one-third of studies implemented and monitored KMb strategies (n = 27, 35.1%), and fewer than a fifth provided evidence for sustaining knowledge use over time (n = 14, 18.2%).
KMb trailblazers
Although the primary KMb literature in the childhood cancer community focuses on gaps and limitations, each barrier is an opportunity for KMb's success. Remarkable initiatives illustrate how key gaps identified in this review may be addressed in practice, mobilizing knowledge to clinicians, patients, and families. The Cure4Kids learning platform, an online medical education website by St Jude Children's Research Hospital with over 22 million content hits, has demonstrated full implementation of the KTA framework, including sustainability over two decades, in addition to an iterative quality improvement process.22,67 Beale et al. 20 effectively addressed KMb directed towards pediatric oncology, providing educational videogames, and demonstrating them as an effective vehicle for health education in adolescents. Cederved et al. 89 helped demonstrate that KMb via gamification prior to radiotherapy helps decrease anxiety in children. Others, such as Ma et al. 55 and McLeod et al., 64 have set the stage for a large-scale data-sharing ecosystem, helping KMb within the clinical and research spheres. Agulnik et al. 15 showed the successful implementation of knowledge tools across 36 pediatric centers. Collectively, amongst others, these successful initiatives underscore the transformative potential of full KMb in pediatric oncology by catalyzing educational advancements, facilitating robust data-sharing frameworks, and establishing sustainable practices that may inform future innovations. Their success may be partly due to engagement with the later stages of the KTA cycle, including knowledge implementation, evaluation, and sustainability planning, rather than stopping at the early steps of knowledge creation or action. While secondary literature, commentaries, pilot projects, and special reports provide valuable insights, expanding empirical research on these approaches could generate more generalizable evidence and support broader adoption across the childhood cancer community. Future studies could particularly benefit from action research methodologies to further explore KMb facilitators and provide robust validation and evaluation of interventions.
KMb barriers
Previous studies have assessed the barriers and facilitators in KMb activities within larger multi-disciplinary academic institutions in low- and middle-income countries.92,93 Barriers included a lack of knowledge of how to conduct effective KMb, limited financial and time resources, limited staffing and training support, inadequate institutional guidelines and structures promoting KMb, and limited leadership engagement. Our findings of the KMb needs in the childhood cancer community are analogous, but with the added complexity of the developmental abilities of the pediatric patient, the caregiver's and parents’ dynamics, and sociocultural factors.
KMb interventions
The CHILD-BRIGHT Network, a patient-oriented network funded by the Canadian Institutes of Health Research under Canada's Strategy for Patient-Oriented Research focused on children and youth with brain-based developmental disabilities and their families, provides a list of KMb strategies and intended outcomes with an evaluation of their state of the evidence using validated tools for intervention assessment. 94 The overarching categories included media strategies, online platforms, 1:1 support, presentations, training, and written materials. Of the 61 KMb strategy-to-outcomes listed, 19 were evaluated as effective. Among many, these included: videos with visual and/or oral components for decision-making and communication about pain; e-learning, mobile apps, patient portals, and toolkits to facilitate behavior change; and decision aids to improve participation in decision making and overall knowledge. The childhood cancer community may benefit from a similar guidance document evaluating the grade of recommendation of KMb interventions for pediatric patients, parents, and the public to address the needs and barriers identified in this scoping review study.
KMb gaps in the childhood cancer community
The KMb findings associated with this study are predominantly from high-income settings, which limits generalizability to low-resource environments. In 2018, the World Health Organization (WHO) and St Jude Children's Research Hospital began their collaboration by committing US$15 million to launch the Global Initiative for Childhood Cancer, which now supports over 50 governments in developing local cancer programs and aims to raise survival rates to 60% by 2030. 95 This is historically one of the largest investment in the childhood cancer community aimed at low- and middle-income countries. 95 More research on KMb interventions in these settings is needed to support this important goal with evidence-based strategies. Additionally, these strategies must be grounded in cultural and social sensitivity, highlighting the importance of culturally appropriate KMb in these settings, all while emphasizing patient, family, and community engagement.
Limitations
This review has several limitations. Consistent with other studies in medical education, this scoping review included one reviewer in the screening process, given the aim, time, and resources allocated. 11 Methodological heterogeneity and inconsistent reporting precluded subgroup analyses (e.g. based on study design, population characteristics, or KMb intervention type). A grey literature search was not conducted to retrieve blogs, textbooks, or thesis works. Including a grey literature search may uncover emerging or unpublished findings, offering broader insights and reducing potential publication bias. Indeed, KMb practices may be occurring in pediatric oncology but are not captured in the formal primary literature. There was a paucity of empirical data focusing on policy-makers and their role in KMb in the childhood cancer community. Another limitation of our findings is the lack of consistent reporting of KMb facilitators in the literature, highlighting a publication bias toward problem-focused studies emphasizing barriers and knowledge gaps. Consistent with the scoping review methodology, a formal critical appraisal of the included articles was not undertaken. This approach aligns with the primary goal of scoping reviews, which is to map the breadth of existing literature rather than to assess study quality. 8 This review provides a time-bound assessment of the current state of KMb in pediatric oncology. As practices and frameworks in KMb continue to evolve, the findings of this study should be interpreted within the context of the timeframe in which the review was conducted.
Future research should assess patient and family engagement in KMb and understand disparities in access to knowledge in different socioeconomic and cultural groups, helping reach underserved populations. It is also essential to explore how to ensure sustainability in KMb processes, as well as to investigate the role of technology-enabled KMb—including artificial intelligence—and its impact on KMb practice and policy.
Conclusion
This scoping review highlights the complexity and multifaceted nature of KMb in the childhood cancer community, highlighting the needs and barriers to effective KMb. Despite ongoing efforts to improve the flow of reliable, evidence-based information, significant gaps persist, particularly in the action cycle of knowledge. Effective KMb will require sustained, culturally appropriate collaboration among healthcare teams, patients, caregivers, and policymakers to tackle the needs and barriers to KMb.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251397433 - Supplemental material for Knowledge mobilization in childhood cancer: A scoping review and content analysis
Supplemental material, sj-docx-1-dhj-10.1177_20552076251397433 for Knowledge mobilization in childhood cancer: A scoping review and content analysis by Sarah Moussa, Emily K Drake, Sonia Angela Castiglione, Geneviève Laporte, Michel Duval, Argerie Tsimicalis and in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251397433 - Supplemental material for Knowledge mobilization in childhood cancer: A scoping review and content analysis
Supplemental material, sj-docx-2-dhj-10.1177_20552076251397433 for Knowledge mobilization in childhood cancer: A scoping review and content analysis by Sarah Moussa, Emily K Drake, Sonia Angela Castiglione, Geneviève Laporte, Michel Duval, Argerie Tsimicalis and in DIGITAL HEALTH
Footnotes
Acknowledgements
We thank McGill University's Research Librarian team for supporting the search strategy. We thank the Knowledge Mobilization Group on behalf of the ACCESS (Advancing Childhood Cancer Experience, Science & Survivorship) network, supported by the ACCESS Secretariat and the Canadian Institute of Health Research (CIHR Funding Reference No.: PDC 184352).
Author contributions
The research protocol was established by SM, EKD, and AT, with guidance from the McGill University Research Librarian. SM led the acquisition and analysis of the data along with EKD. All authors had access to all the data in the study. SM, EKD, and AT interpreted the data. SM drafted the manuscript, and EKD, SAN, GL, MD, and AT revised it critically for important intellectual content. The ACCESS (Advancing Childhood Cancer Experience, Science and Survivorship) network peer-reviewed the manuscript prior to publication. All authors reviewed the reviewers’ comments and provided important intellectual content based on their clinical expertise. All authors read and approved the final version to be published. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This review was conducted in the context of the Knowledge Mobilization Group on behalf of the ACCESS (Accelerating Childhood Cancer Experience, Science & Survivorship) network supported by the ACCESS Secretariat and the Canadian Institutes of Health Research (CIHR funding reference number 184352).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data generated or analyzed during this study are included in this published article and its supplementary information files.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.