
Abstract
Objectives:
To assess clinicians’ knowledge, attitude and associated factors towards patients’ early mobilization in intensive care units in the tertiary hospitals in Northwest Ethiopia.
Methods:
A multi-centre, cross-sectional study was conducted at the tertiary hospitals in Northwest Ethiopia from April to June, 2022. Data were collected by using self-administered, structured questionnaire; ordinal logistic regression analysis was performed and associations were described in adjusted odds ratios.
Results:
A total of 304 clinicians were included (response rate of 89.7%). The proportions of poor, fair and good knowledge towards early mobilization in intensive care unit among clinicians were 16.8%, 57.9% and 25.3%, respectively; while that of negative, fair and positive attitude were 16.4%, 60.2% and 23.4%, respectively. Factors associated with better knowledge were being a physiotherapist (adjusted odds ratio = 2.9, confidence interval = 1.2–6.7), having a total work experience >5 years (adjusted odds ratio = 4.6, confidence interval = 1.7–12.1), having an intensive care unit work experience >5 years (adjusted odds ratio = 2.8, confidence interval = 1.1–6.8), previous in-service training (adjusted odds ratio = 1.8, confidence interval = 1.1–3.0) and reading guidelines (adjusted odds ratio = 1.9, confidence interval = 1.1–3.2). Better attitude was associated with in-service training (adjusted odds ratio = 1.9, confidence interval = 1.2–3.1), attending early mobilization courses (adjusted odds ratio = 1.8, confidence interval = 1.1–3.0), presence of mobilization advocators (adjusted odds ratio = 1.7, confidence interval = 1.0–2.8), good knowledge (adjusted odds ratio = 2.6, confidence interval = 1.2–5.8) and fair knowledge (adjusted odds ratio = 2.5, confidence interval = 1.3–4.8).
Conclusion:
Most of the clinicians had demonstrated fair knowledge and attitude towards early mobilization in intensive care unit. However, there were significant proportion of clinicians who had poor knowledge and negative attitude. We recommended active engagement of physiotherapists and experienced clinicians in intensive care units. Clinicians need to have self-learning habits and attend regular training/courses related to early mobilization in intensive care unit.
Introduction
Early mobilization needs interdisciplinary team approach from active range of motion to full range of ambulation. 1 It starts as early as the first or second day of admission to intensive care unit (ICU) and involves timely progression through a series of simple activities to full ambulation. 2 It is classified into passive and active mobilization. Passive mobilization usually includes patients changing different positions, suctioning by physiotherapist and changing diapers. 3 Active mobilization includes ambulation and physical exercises with or without assistance.4–6
Prolonged immobilization is independently associated with serious complications such as pressure ulcers, pneumonia, deep vein thrombosis, delirium and ICU-acquired weakness.7–9 Early mobilization was found to improve physical and cognitive functions, decrease mechanical ventilation time, ICU and total hospital stay and overall healthcare cost.10,11
Early mobilization is a safe and feasible intervention that results in physiological and functional improvements in ICU. Despite its benefits, early mobilization is not widely implemented in ICUs. The rate of early mobilization was 19.2% in mechanically ventilated patients and 23.5% in non-mechanically ventilated patients. 12 Previous studies documented that only 37% and 24% of ICU patients had bedside mobilization.13,14 Commonly reported perceived barriers to early mobilization in ICU were lack of mobilization protocol, inadequate training and knowledge and negative attitude and culture among ICU clinicians.15–19 There was limited research-based evidence on early mobilization in ICU in low-income countries. Therefore, the objective of this study was to assess clinicians’ knowledge and attitude and associated factors towards patients’ early mobilization in ICUs in tertiary hospitals in Northwest Ethiopia.
Methods
Study design, period, and area
A multi-centre cross-sectional census was conducted from April 2 to June 20, 2022 at five tertiary hospitals in Northwest Ethiopia: University of Gondar Comprehensive Specialized Hospital (UOGCSH) at Gondar town, Tibebe Ghion Comprehensive Specialized Hospital (TGCSH) in Bahirdar city, Felege Hiwot Comprehensive Specialized Hospital (FHCSH) in Bahirdar city, Debre Markos Comprehensive Specialized Hospital (DMCSH) at Debre Markos town and Debre Tabor Comprehensive Specialized Hospital (DTCSH) at Debre Tabor town.
This study included all physicians, anaesthetists, nurses and physiotherapists who were working in adult surgical and medical ICUs at the five tertiary hospitals in Northwest Ethiopia during the study period; 339 ICU clinicians were working:135 at UOGCSH, 58 at TGCSH, 46 at FHCSH, 58 at DMCSH and 42 at DTCSH. UOGCSH and DTCSH had two ICUs (one medical and one surgical), whereas FHCSH, TGCSH and DMCSH had one mixed medical–surgical ICU. All except students, volunteers and clinicians on leave were excluded from this study.
Variables and operational definitions
The outcome variables were knowledge and attitude towards early mobilization. The independent variables were sociodemographic factors, work-related factors and ICU setting-related factors.
We define early mobilization as a range of bodily movements carried out by healthcare provider as part of care for patients admitted to ICU, which may include active or passive movements. 20
Knowledge: According to Bloom’s cutoff points, scores between 80% and 100% (11–13 out of 13) were considered as good, scores between 60% and 79% (8–10 out of 13) were considered as fair and scores below 60% (⩽7 out of 13) were considered as poor.21–23
Attitude: According to Bloom’s cutoff points, scores between 80% and 100% (48–60 out of 60) were considered as positive, scores between 60% and 79% (36–47 out of 60) were considered as fair and scores below 60% (⩽35 out of 60) were considered as negative.21–23
Data collection tools and procedure
Ethical approval was obtained from the Ethical Review Committee of School of Medicine, University of Gondar and official permission was obtained from each hospital administration. Written informed consent was obtained from each study participant and confidentiality was ensured. Data were collected with an English version of structured, self-administered questionnaire which was validated and its internal consistency was reported as 0.9.21,24 The knowledge domain contained 13 YES or NO questions to assess health professional’s levels of knowledge regarding early mobilization in ICU. Within the knowledge domain, the participants responded to any choices they thought might be correct. Each correct answer was scored as 1, and each incorrect answer was scored as 0. Thus, the total score of knowledge for each study participant ranged from 0 to 13, and a higher score indicated good knowledge. The attitude domain contained 12 questions which were measured by a five-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree and 5 = strongly agree). A negative question was scored in the reverse direction. Each question or item was scored, and the final attitude score ranged between a minimum of 12 and a maximum of 60.
Statistical analysis
The data were entered by EpiData version 4.6 and exported to SPSS version 26 (IBM Corporation, New York, USA) for analysis. Descriptive and ordinal logistic regression analyses were performed to determine associations. Independent variables with p-values < 0.2 in bivariate regression analysis were entered in the final multivariate regression analysis. Independent variables with a p-value < 0.05 in the final model were considered statistically significant and the strength of association was shown in adjusted odds ratio (AOR) at 95% confidence interval (CI).
Results
Sociodemographic characteristics
A total of 304 clinicians were included in this study with a response rate of 89.7%. Of the total, 82 (27.0%) were physicians, 80 (26.0%) were anaesthetists, 104 (34.2%) were nurses and 38 (12.5%) were physiotherapists. The median age of the clinicians was 29 years (interquartile range (IQR) = 27–33) (Table 1).
Sociodemographic characteristics of ICU clinicians (N = 304).

Work and ICU-related characteristics
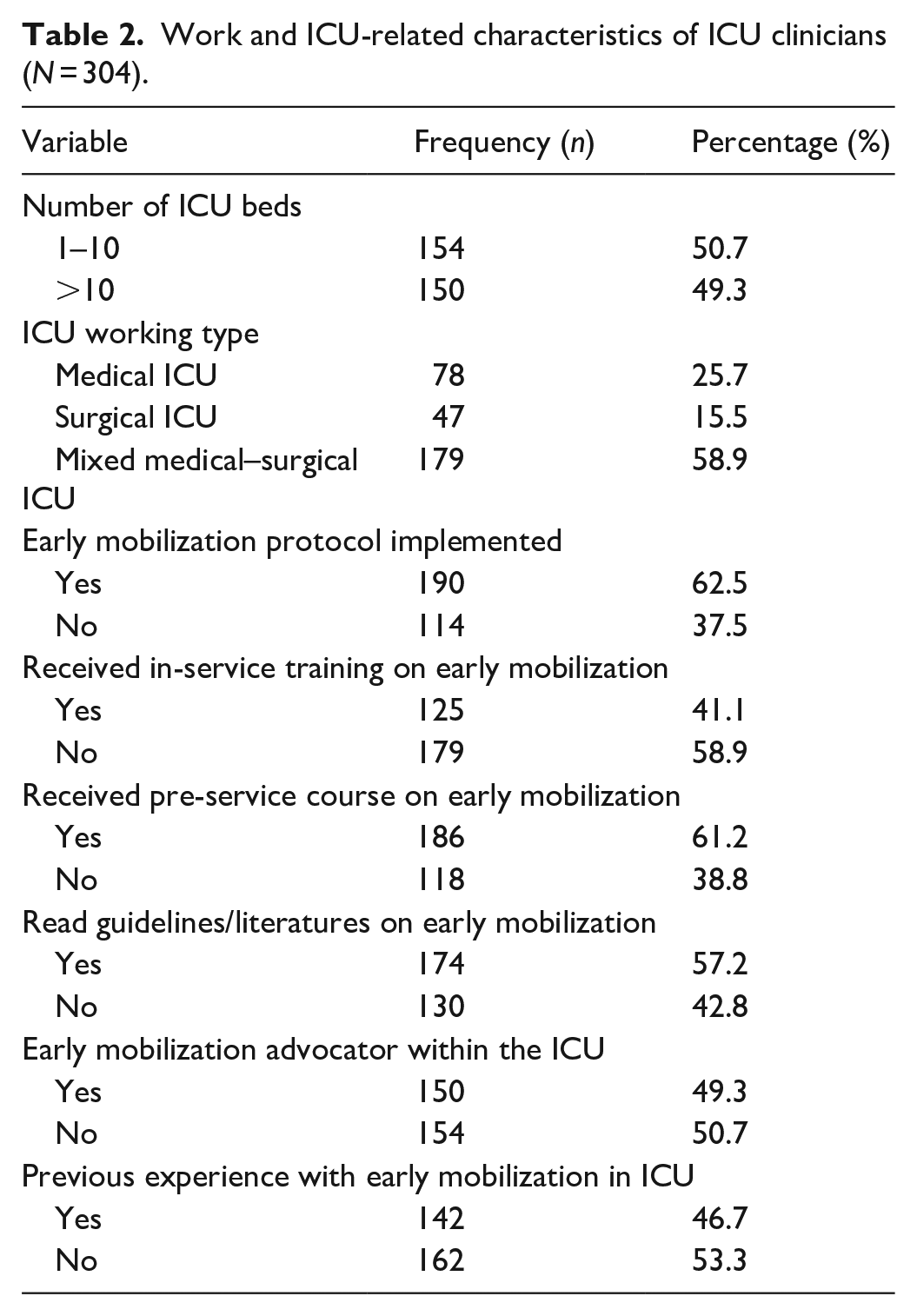
More than half of the clinicians (179, 58.9%) were working in mixed medical–surgical ICUs. The majority (179, 58.9%) did not take any in-service training related to early mobilization. One hundred and eighty-six (61.2%) clinicians had attended a course related to early mobilization during pre-service education. One hundred and seventy-four (57.2%) clinicians had the experience of self-reading of guidelines/literature related to early mobilization in ICU while 162 (53.3%) had no previous experience with early mobilization in ICU (Table 2).
Work and ICU-related characteristics of ICU clinicians (N = 304).
Knowledge on early mobilization in ICU
Of the total, 51 (16.8%) had poor knowledge (CI = 12.8–21.4), 176 (57.9%) had fair knowledge (CI = 52.6–63.5) and 77 (25.3%) had good knowledge (CI = 20.4–30.6) on early mobilization in ICU. The median knowledge score was 9.0 (IQR = 8.0–10.8). The minimum and maximum scores were 4 and 13, respectively. The knowledge levels differ across professions as 18 (22.0%) physicians, 21 (26.3%) anaesthetists, 21 (20.2%) nurses and 17 (44.7%) physiotherapists had good knowledge (Figure 1). The knowledge levels differ across each institution, 26.2% in UOGCSH, 17.3% in TGCSH, 11.9% in FHCSH, 36.8% in DMCSH and 32.3% in DTCSH had good knowledge (Figure 2).
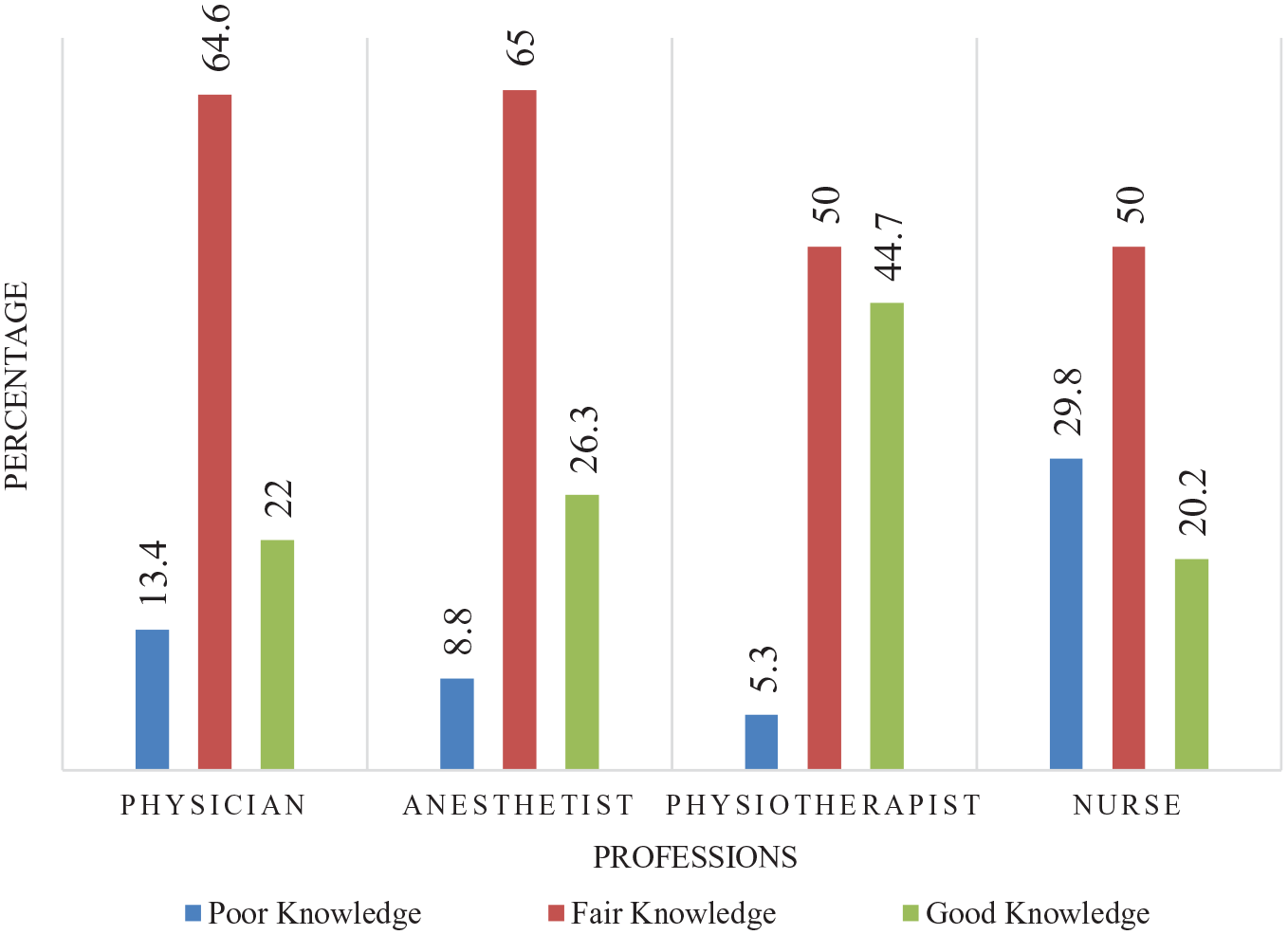
Knowledge of clinicians among professions (N = 304).
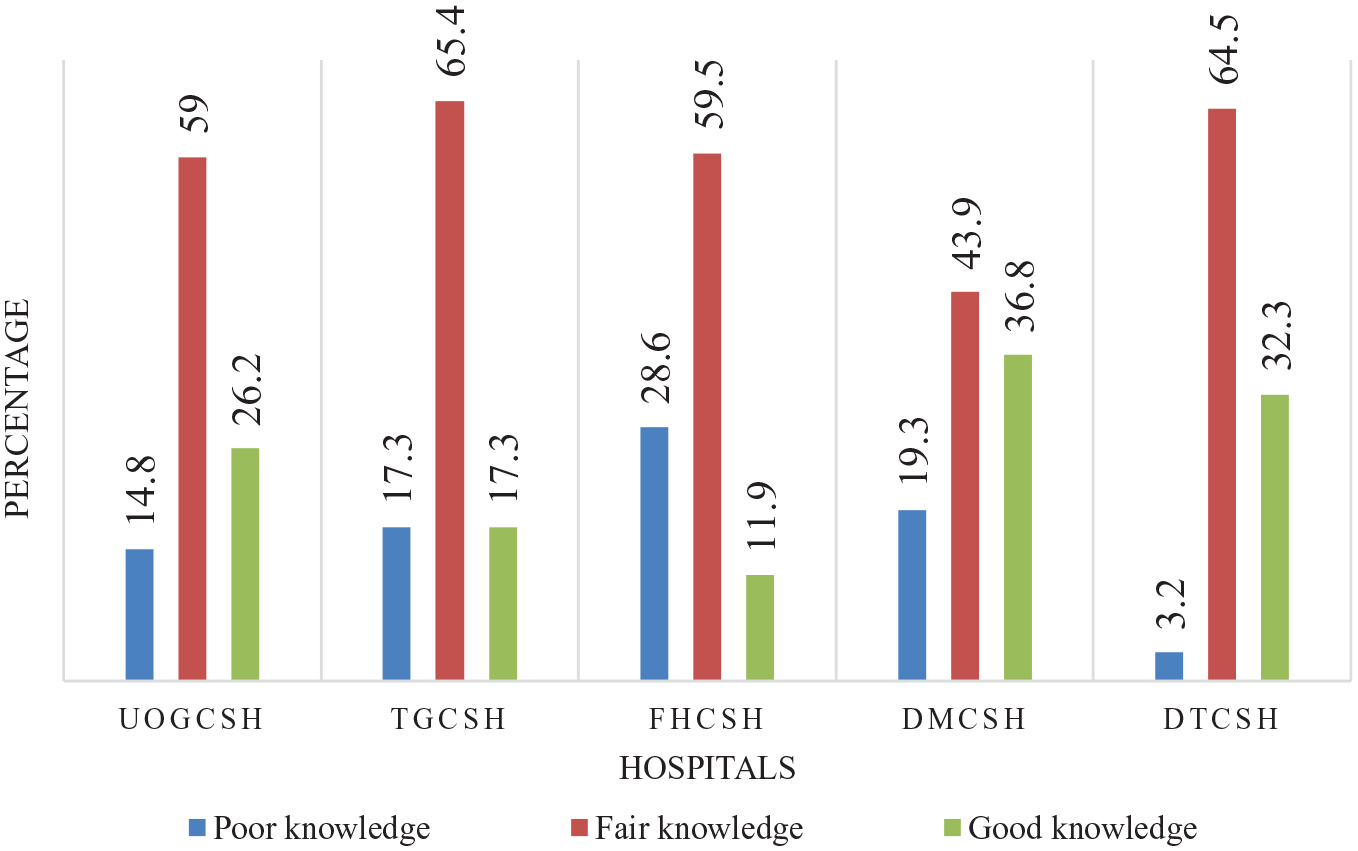
Knowledge of clinicians among hospitals (N = 304).
The question that had the highest rate of correct answers (284, 93.4%) was ‘early mobilization practice can improve patients’ respiratory function’, followed by the question ‘the term “mobilization” refers to physical activity of sufficient intensity to produce physiological effects such as increased blood circulation’ (270, 88.8%). The least correctly answered question was ‘the range of motion exercise (active or passive) is sufficient to maintain muscle strength in critically ill patients’ (103, 33.9%), followed by the question ‘early mobilization refers to active rehabilitation and passive exercise that are limited in bed’ (111, 36.5%) (Table 3).
Responses to knowledge questions by ICU clinicians (N = 304).

ABCDE: Airway, Breathing, Circulation, Disability, Exposure; EM: Early Mobilization; ICU: intensive care unit.
The likelihood of physiotherapists to have better knowledge was three times higher than that of nurses (AOR = 2.9, CI = 1.2–6.7). Clinicians who had total work experience >5 years were found to be five times more knowledgeable than those who had <2 years of experience (AOR = 4.6, CI = 1.7–12.1). Furthermore, the odds of having better knowledge were four times higher among clinicians who had a total work experience of 2–5 years than those who had <2 years of exposure (AOR = 4.1, CI = 1.7–9.9). Similarly, clinicians who had ICU work experience of >5 years were found to have three times better knowledge than those who had <2 year of ICU work experience (AOR = 2.8, CI = 1.1–6.8).
Clinicians who had taken in-service training were twice more knowledgeable (AOR = 1.8, CI = 1.1–3.0). In addition, those who had attended a course related to early mobilization during pre-service education were twice more knowledgeable (AOR = 2.1, CI = 1.2–3.6). Similarly, those who have the experience of self-reading of guidelines/literatures related to early mobilization were twice more knowledgeable (AOR = 1.9, CI = 1.1–3.2).
The odds of having better knowledge among clinicians who had positive and fair attitude were 3.3 (AOR = 3.3, CI = 1.4–8.0) and 3.2 (AOR = 3.2, CI = 1.5–6.9), respectively (Table 4).
Ordinal logistic regression model: knowledge of clinicians on early mobilization (N = 304).

CI: confidence interval; ICU: intensive care unit.
Bold values are statistically significant.
Attitude towards early mobilization in ICU
Of the total, 50 (16.4%) had negative attitude (CI = 12.5–20.7), 183 (60.2%) had fair attitude (CI = 54.3–66.1) and 71 (23.4%) had positive attitude (CI = 19.1–28.6). The median (IQR) attitude score was 44 (39–47). The minimum and maximum attitude scores were 20 and 60, respectively. When comparing professionals, 21 (25.6%) physicians, 23 (28.7%) anaesthetists, 18 (17.3%) nurses and 9 (23.7%) physiotherapists were found to have positive attitude (Figure 3). The attitude levels differ across each institution, 24.6% in UOGCSH, 25% in TGCSH, 19% in FHCSH, 24.6% in DMCSH and 38.7% in DTCSH had positive attitude (Figure 4).

Attitude of clinicians among professions (N = 304).

Attitude of clinicians among hospitals (N = 304).
The majority of the clinicians (157, 51.6%) had agreed that early mobilization should be regarded as a routine care in ICU and 125 (41.1%) had strongly agreed that receiving in-service training related to early mobilization is necessary for critical care ICU clinicians (Table 5).
Responses to attitude questions by ICU clinicians (N = 304).

ICU: intensive care unit.
The odds of having better attitude among clinicians who had received pre-service course and in-service training related to early mobilization were nearly two times more than those who had not (AOR = 1.8, CI = 1.1–3.0) and (AOR = 1.9, CI = 1.2–3.1). Moreover, clinicians who were working in ICUs that had mobilization advocator were nearly twice knowledgeable (AOR = 1.7, CI = 1.0–2.8).
Clinicians who had good and fair knowledge were found to have better attitude (AOR = 2.6, CI = 1.2–5.8) and (AOR = 2.5, CI = 1.3–4.8) than those who have poor level of knowledge, respectively (Table 6).
Ordinal logistic regression: attitude towards early mobilization (N = 304).

CI: confidence interval; ICU: intensive care unit.
Bold values are statistically significant.
Discussion
Early mobilization is essential for physiological and functional recovery. Despite its benefits, early mobilization is not widely implemented in ICUs. 12 This survey study was conducted with a total of 304 study subjects to determine the level of knowledge and attitude and associated factors among health professionals working in ICU towards patients’ early mobilization. Our study showed that the proportions of poor, fair and good knowledge on early mobilization were 16.8%, 57.9% and 25.3%, respectively. The proportion of good knowledge was lower compared to that of previous studies which reported that the proportion of good knowledge was 66%, 61.7%, 58.2% and 50%.19,24–26 Another study has reported 41% poor, 19% fair and 40% good knowledge. 16 However, higher proportion of poor knowledge (59.8% and 34.8%) was also reported.2,27 The proportion of good knowledge was relatively high compared to a previous study that reported 45.2% poor knowledge, 52.3% fair knowledge and 2.5% good knowledge. 21 The possible reasons for the lower proportion of good knowledge in our study might be pre-service and in-service training, measurement tools and composition of study participants in-terms of profession.
Physiotherapists were three times more likely to have good knowledge as compared to nurses. Supporting our finding, previous studies have reported that physiotherapists demonstrated good knowledge on early mobilization and its benefits,19,28 and might be explained by the nature of the profession as physiotherapy focuses on physical activities.
We found that longer total work experience and ICU work experience were associated with good knowledge which is consistent with previous studies,19,29–32 and might be justified by knowledge acquired through experience and the possibility of senior clinicians to have further education training. 33 However, knowledge may fade as time elapsed, especially, in over 10 years.25,28
Taking pre-service courses or in-service training related to early mobilization have doubled the odds of having better knowledge. We found that this finding is consistent with previous reports.21,31–36. Furthermore, clinicians who have the experience of self-reading of guidelines/literature related to early mobilization in ICU were found two times more knowledgeable; and it is comparable to a previous study. 19
Knowledge and attitude are usually interdependent. Our study demonstrated that clinicians who had positive or fair attitude were three times more knowledgeable on early mobilization in ICU and this finding is supporting a previous study. 19
Over 60% of respondents had shown positive attitude to early mobilization in previous studies.25,28 In this study, the proportions of positive, fair and negative attitude towards early mobilization were 23.4%, 60.2% and 16.4%, respectively. Comparably, a previous study has reported 31.4% positive, 60.7% fair and 7.8% negative attitude. 21 However, the proportion of positive attitude was lower than that of a previous study which reported 72%, 61.7% and 87.4% of clinicians had positive attitude towards early mobilization.18,25,37
Clinicians who had received pre-service course or in-service training related to early mobilization were found twice more likely to have better attitude which is consistent with previous studies.21,34,36,38
The presence of early mobilization advocator/champion in ICU has doubled the odds of better attitude among clinicians. Early mobilization advocators in ICU may help to build positive attitude and motivation. 2
Clinicians who had good and fair knowledge were found to have better attitude towards early mobilization. Knowledge is known to guide behavioural changes and our finding is consistent with the other studies.19,25,39
The limitations in this study were inability to determine cause–effect temporal relationships, study was exposed to social desirability bias as respondents may overreport their attitudes and relative weakness of ‘YES or NO’ questions to accurately assess knowledge compared to multiple choice questions. We included all healthcare professionals who were working in ICU, without power analysis of sample size calculation due to limited number of clinicians working in the ICUs. For future researchers, we would like to recommend to study the practice of early mobilization in ICU.
Conclusion
The majority of clinicians had fair knowledge and attitude towards early mobilization in ICU. However, there were still significant proportion of clinicians who had poor knowledge and negative attitude. Being a physiotherapist, total work experience >5 years, ICU work experience >5 years, training and education on early mobilization, self-reading guidelines/literatures and having positive attitude were significantly associated with good knowledge of health professionals. Similarly, training and education on early mobilization, presence of early mobilization advocator within the ICU and having good knowledge were significantly associated with positive attitude of health professionals towards early mobilization in ICU. Therefore, we recommended active engagement of physiotherapists and experienced clinicians in ICUs. We also urge clinicians to have self-learning habits and hospital administrators to prepare regular training and courses related to early mobilization in ICU. We have also demonstrated interdependence between knowledge and attitude.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231172348 – Supplemental material for Clinicians’ knowledge and attitude towards early mobilization in intensive care units in Ethiopian tertiary hospitals: A multi-centre study
Supplemental material, sj-docx-1-smo-10.1177_20503121231172348 for Clinicians’ knowledge and attitude towards early mobilization in intensive care units in Ethiopian tertiary hospitals: A multi-centre study by Tasew Kelemu Dagnachew, Yophtahe Woldegerima Berhe, Salh Yalew Mustofa and Wubie Birlie Chekol in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to acknowledge the University of Gondar Comprehensive Specialized Hospital, Tibebe Ghion Comprehensive Specialized Hospital, Felege Hiwot Comprehensive Specialized Hospital, Debre Markos Comprehensive Specialized Hospital, Debre Tabor Comprehensive Specialized Hospital and the data collectors. We also want to show our special acknowledgement to Hui Zhang from Pecking Medical College, Beijing, China and Frances Lin from University of the Sunshine Coast, Queensland, Australia for sharing data collection tools.
Author contributions
TKD has conceptualized the study and objectives and developed the proposal. YWB, WBC and SYM criticized the proposal. All authors had participated in data management and statistical analyses. YBW and TKD have prepared the final article. All authors read and approved the final article.
Availability of data and materials
Data and materials used in this study are available and can be presented by the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by University of Gondar and Debre Markos University with no conflict of interest. The support did not include publication charges.
Ethics approval and consent to participate
Ethical approval was obtained from the Ethical Review Committee of School of Medicine, University of Gondar (approval number: SOM/1404/2022); and official permission was obtained from each hospital administration. Written informed consent was obtained from every participant after a brief explanation. Confidentiality was ensured by removing identifiers and locking the questionnaires after data collection in a secured area.
Informed consent
Written informed consent was obtained from all subjects before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.