
Abstract
Objective
Physician gender may be a source of differences in communication between physicians and their patients, which may in turn contribute to patient satisfaction and other outcomes. Our aim was to review systematically research on gender differences in the length, style and content of communication with patients.
Methods
Seven electronic databases were searched from inception to September 2010 with no language restrictions (included MEDLINE; PsychINFO; EMBASE; CINAHL; Health Management Information Consortium; Web of Science; and ASSIA). ‘Grey’ literature was also searched. Data extraction and quality assessment was carried out in accordance with Cochrane Collaboration guidelines by at least two reviewers. The review uses mainly narrative synthesis due to the heterogeneous nature of the studies, with only data on consultation length being pooled in a random effects generic inverse variance meta-analysis.
Results
Searches yielded 6412 articles, of which 33 studies fulfilled the inclusion criteria. Studies were heterogenous and of mixed quality. Conflicting results are reported for many communication variables. There is some evidence that female physicians adopt a more partnership building style and spend on average 2.24 min longer with patients per consultation (95% CI 0.62–3.86) than their male colleagues.
Conclusions
Greater patient engagement by female doctors may reflect a more patient-centred approach, but their longer consultation times will limit the number of consultations they can provide. This has implications for planning and managing services.
Introduction
As the proportion of women in medicine draws towards parity, long-standing questions about whether male and female doctors communicate differently with patients are important and timely. Biological deterministic theories which suggested that men and women differ as a result of biological sex differences have largely been replaced by theories which suggest gender differences in behaviours may arise due to an interaction between personal characteristics and wider social and cultural forces that have historically affected men and women differently.
The communication that takes place during medical consultations is integral to the care that patients receive and research suggests that it may relate to a number of patient outcomes including patient satisfaction, recall, treatment adherence, understanding of information and health outcomes. 1,2 Additionally, doctor–patient communication may influence the length of consultations, which may ultimately affect the clinical activity rates of doctors, timely given the current emphasis on productivity and value for money in health care organizations internationally. If women and men do communicate differently, there may be important lessons related to tailoring the training of men and of women and implications for improving the quality and quantity of consultations.
In an earlier meta-analytic review, Roter et al. 3 found that female doctors engage in more positive talk (such as encouragement), ask more psychosocial questions, discuss more about emotions and demonstrate more partnership building behaviours. More recently, researchers have found that female doctors’ communication was rated as more empathic than men. 4 The length of medical consultations has been researched more extensively with regard to differences between male and female doctors, with several studies reporting that women conduct longer consultations than men. 3,5 Differences in consultation length may contribute to apparent differences in the activity rates of male and female doctors, as reported in Canada 6 and in the UK, 7 although these findings do not consider the nature or quality of the consultation.
While there is extensive research on gender differences in communication during medical consultations, most studies are small and few have appraised their quality or synthesized the findings. Our aim was to update and extend the review by Roter et al. 3 by considering gender differences in the length, style and content of medical communication, with meta-analysis of gender differences where appropriate.
Methods
Search strategy and inclusion criteria
We used a larger literature base than that used by Roter et al., 3 with no language or data restrictions. Seven electronic databases were searched from their inception until September 2010: MEDLINE (Ovid SP) (from 1950); PsychINFO (Ovid SP) (1967); EMBASE (Ovid SP) (1980); CINAHL (Ebsco) (1982); Health Management Information Consortium (Ovid SP) (1983); Web of Science (ISI Web of Knowledge) (1900); and ASSIA (CSA Illuminia) (1987).
Two key journals that had published a number of articles related to this topic area (Social Science and Medicine; Patient Education and Counselling) were hand searched for 2009 and 2010 to check the quality of indexing terms used in the databases. The System for Information on Grey Literature in Europe (SIGLE) was used to search ‘grey’ literature, and the reference lists of review papers and all included studies were checked for further studies.
Studies were included if they: collected and presented interpretable primary data; studied doctors, including those in training; involved patients (studies using simulated patients were excluded); measured communication using independent observers, audiotape or videotape; and tested for an association between doctors’ gender and at least one interpretable communication variable. Studies involving medical students, psychiatric consultations and studies restricted to length of visit were excluded.
Four groups of terms were included in the search strategy: terms for doctors; patients; communication; and gender. Free text terms were combined with MeSH headings to produce a comprehensive search strategy. To refine the search and reduce the number of ineligible hits, the Boolean operator ‘not’ was used to restrict the searches to studies that did not include nurses or midwives. No study design filters were used. Full search strategies for each database are available upon request from the authors.
Two of three investigators screened independently the 6412 titles and abstracts according to pre-specified inclusion criteria (Figure 1). Two hundred twenty-four full text articles were then retrieved and reviewed independently by two investigators, yielding a final pool of 33 relevant studies. Disagreements were resolved through discussion, with arbitration with the third reviewer where necessary. Cohen’s Kappa was calculated to test the inter-rater reliability of the study selection process and revealed high agreement between reviewers (0.81, p < 0.001).
PRISMA flowchart of study selection process.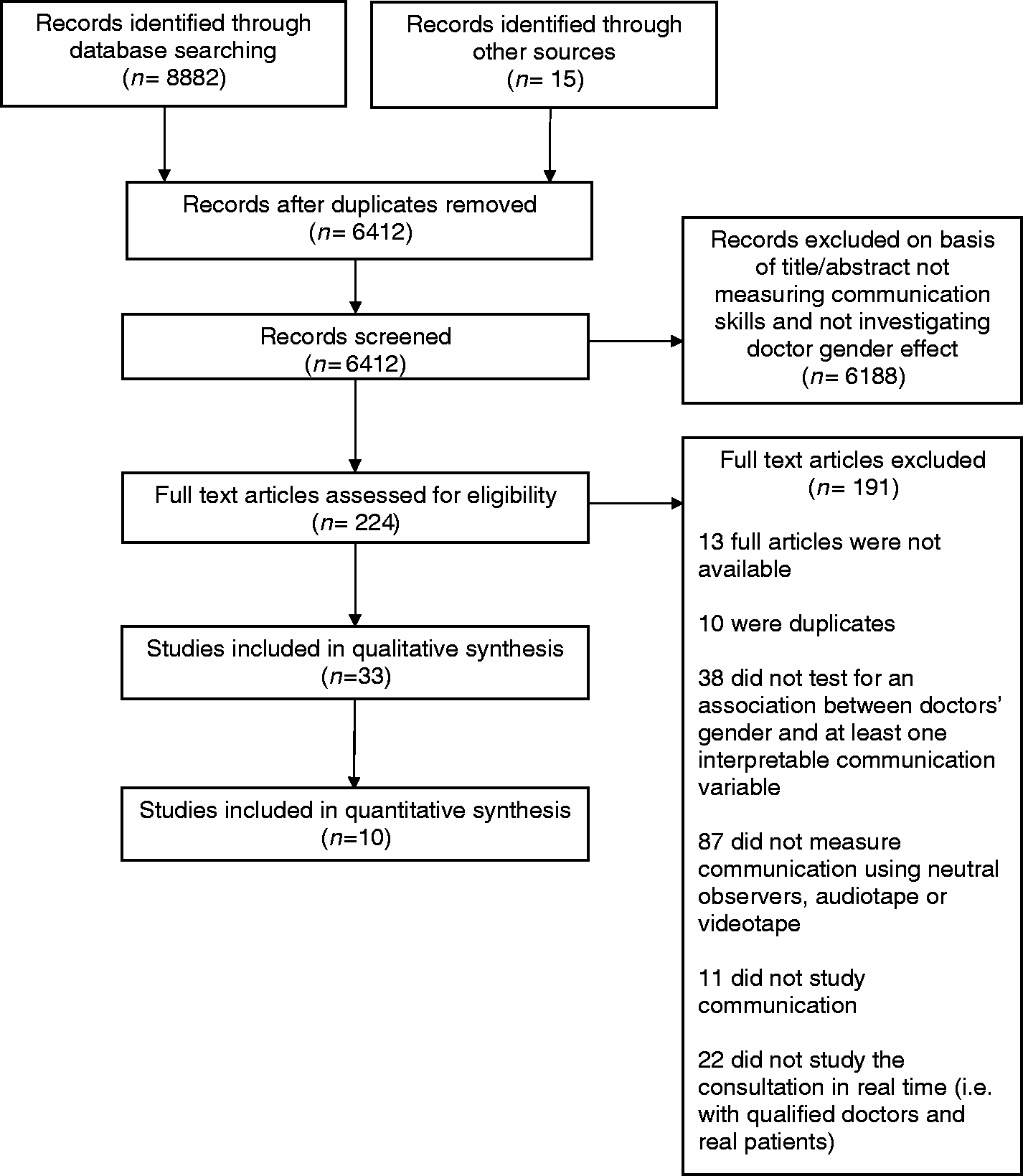
Data extraction and quality assessment
Two investigators extracted data independently for all studies using a form based on the Cochrane collaboration guidelines for data extraction in non-randomized studies, 8 and refined so that it was specific to the topic.
Quality assessment, using an established instrument, 9 was also conducted independently by two reviewers and any disagreements were resolved through discussion and arbitration with the third reviewer.
Data synthesis
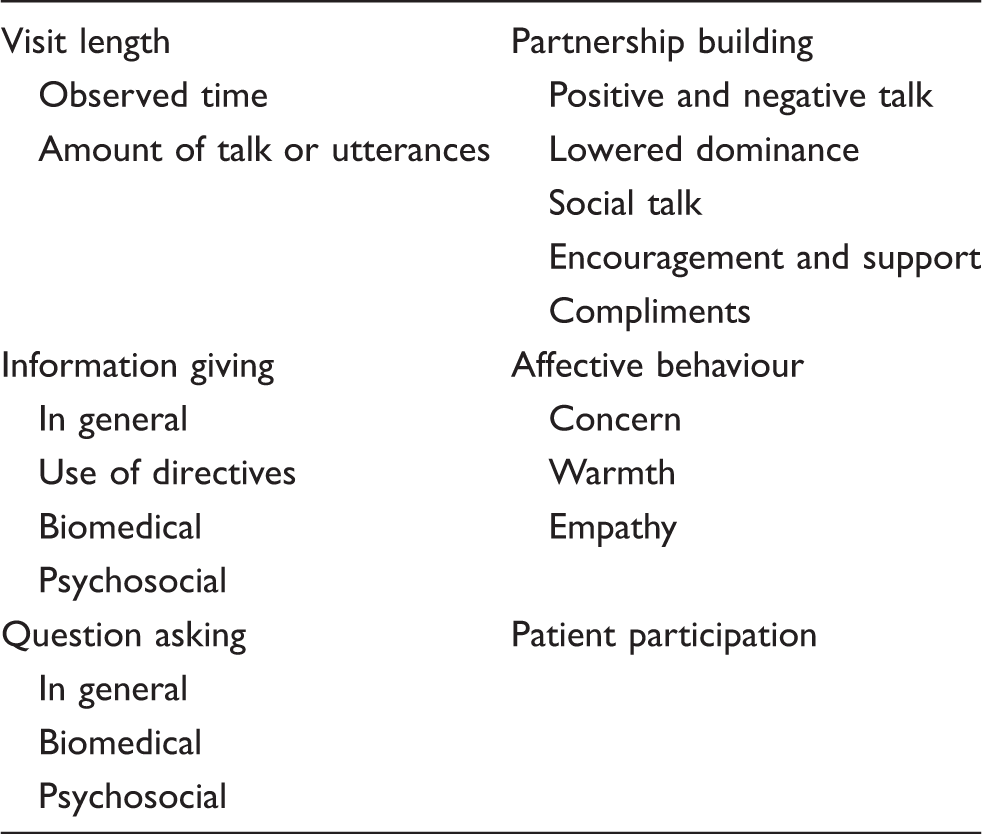
Conceptual groupings of physician communication categories (adapted from Roter et al. 10 ).
We used primarily a narrative synthesis, pooling data in meta-analysis only on the effect of doctors’ gender on length of visit. The mean difference in visit length between male and female doctors and the standard error of this difference were calculated for each study. If an overall estimate of effect was not reported in the study, then we extracted summary data and calculated an unadjusted effect estimate. Some studies reported mean differences but did not report the standard error of this difference. Where necessary, we calculated these values from other data presented in the study using the methods outlined in the Cochrane handbook. A random effects generic inverse variance meta-analysis was used to estimate the overall pooled measure of effect of physician gender on visit length. All analyses were conducted in Stata version 9, using the metan command.
Results
Studies included
Thirty-three studies were included, and the characteristics of included studies can be found in Appendix 1 (web-only; see hsr.sagepub.com/supplemental). The majority were undertaken in the US (22/33) and in primary care (20/33). Most studies involved a variety of patient groups, with only a handful concentrating on specific patient groups or specialties. Studies used a wide variety of tools to measure communication, ranging from specific patient-centredness tools to those that are designed to measure a variety of communication outcomes, such as the Roter Interaction Analysis System (RIAS). 10 RIAS was the most frequently reported method of communication measurement and was used in 11 of the 33 studies. The number of doctors who participated was positively skewed, with more studies of small sample size (median 27, inter-quartile range 17–49.5).
Quality assessment
All studies had two or more ‘weak’ ratings which translates to a ‘weak’ overall quality rating. Details of the quality assessment ratings for each study, excluding the ratings for ‘study design’ and ‘blinding’ which were rated weak for all of the included studies are shown in Appendix 2 (web-only; see hsr.sagepub.com/supplemental). There were difficulties in undertaking the quality assessment, mainly due to limited reporting in the original studies which means that the majority of quality criteria were classed as ‘weak’ due to lack of information. For example, it was difficult to assess the likelihood of selection bias in the studies as they did not describe a sampling framework or provide demographic characteristics of the study population. The majority of studies did not therefore satisfy quality assessment criteria for potential selection bias.
For the majority of studies, it was also not possible to assess whether potential confounders had been accounted for, and most studies did not describe whether there were any important differences in the characteristics of consultations (e.g. patient age, gender or health status) between male and female doctors. There were five studies that were considered as ‘strong’ in this category as they employed appropriate statistical techniques to account for 80–100% of potential confounders. 11 –15 Blinding of observers or raters to doctors’ gender is difficult in this field as often studies used audio recordings or tape recordings. Two studies 14,16 used transcriptions of consultations to code the data, which would theoretically allow the coders to be blind to doctors’ gender; however, these studies do not report whether this was undertaken. Compared to the other quality assessment criteria, studies tended to undertake more rigorous data collection methods. The majority of studies used existing observational tools that had been described elsewhere, and several assessed the inter-rater reliability of different coders.
In only one measure (length of consultation) was measurement thought homogenous enough to justify statistical pooling in a meta-analysis (Appendix 3, web-only; see hsr.sagepub.com/supplemental). Other measures of communication were thought to be too heterogeneous for meta-analysis to be valid.
Visit length
Fifteen studies measured the relationship between doctors’ gender and length of consultation. Of the seven studies that found a statistically significant difference between men and women, five found that female doctors held longer visits 5,12,17 –19 and two showed the opposite effect, 13,20 although one of these was based on data from multiple consultations with just one male and one female doctor. 20
Ten studies were included in a random effects meta-analysis to pool the data on visit length.
5,11
–13,17
–19,21
–23
Four were excluded because they did not present sufficient data,
15,24
–26
and one was excluded because it included observations with only two doctors.
20
Across the 10 included studies, in an average, consultation, female doctors spent over 2 min more with patients compared to male doctors (coefficient 2.24, 95% CI 0.62–3.86, p = 0.01) (Figure 2). However, tests for heterogeneity demonstrate the high variability across studies included in this meta-analysis (X
2 = 28.67, df = 9, p < 0.001, I
2 = 68.6%).
Forest plot of visit length.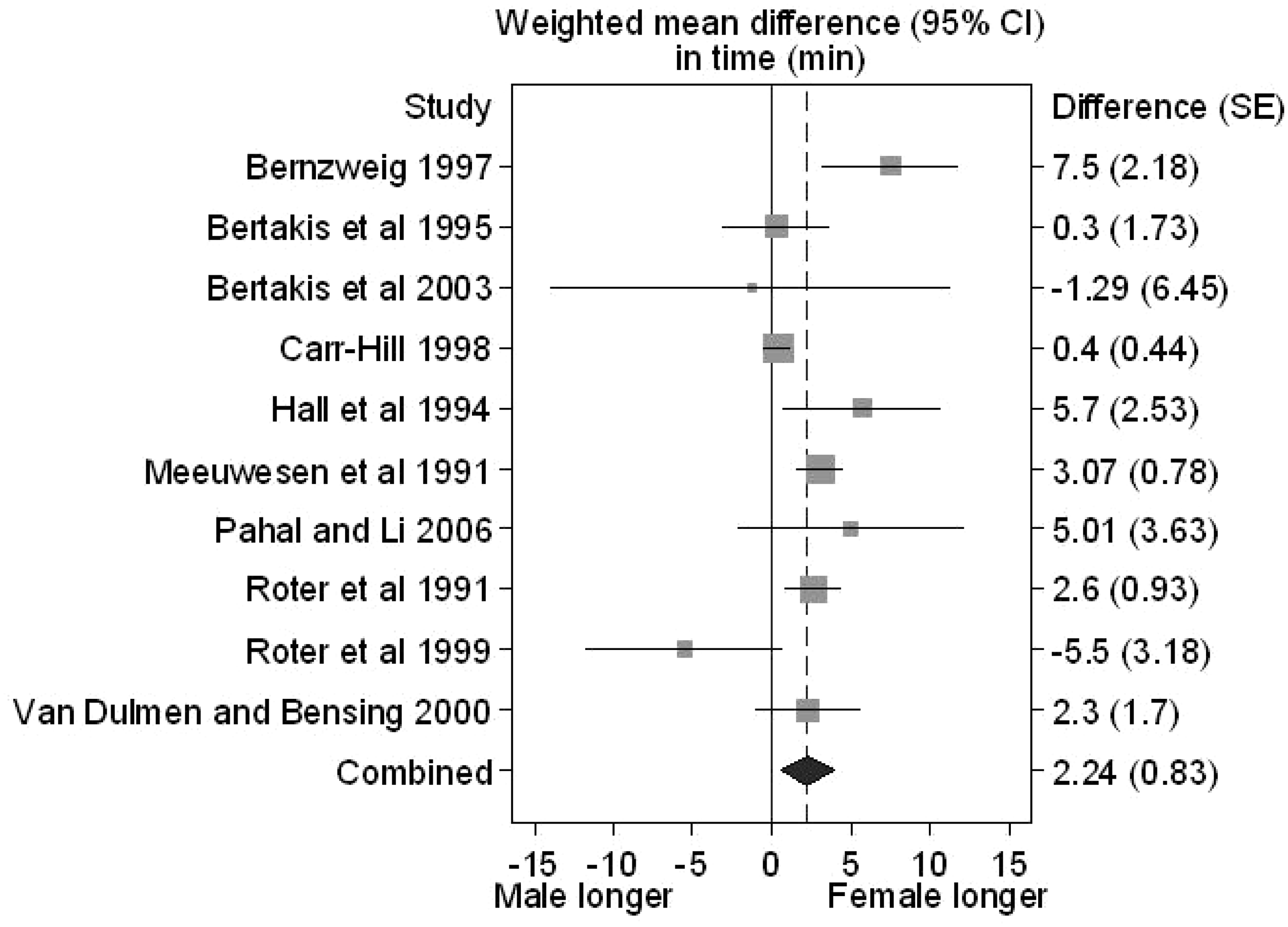
Information giving
Fourteen studies assessed this aspect of medical communication and reported mixed findings. We explored potential gender differences in overall information giving and use of directives, as well as considering psychosocial and biomedical information separately. No clear picture emerged. Overall information giving and use of directives show little difference between male and female doctors, but it may be that male doctors provide more biomedical information, 18,27 although this did not apply to providing preventive biomedical information, which appears to be provided more frequently by women. 21,22 Female doctors may also be more likely to provide psychosocial information. 12,21,27
Question asking
Thirteen studies investigated the effect of doctor’s gender on the questions that are asked during medical consultations. Again there are conflicting results. The majority of studies of general questioning showed no difference between male and female doctors, the exception being psychosocial questioning. In two studies that explored this, the authors reported more psychosocial questions from female doctors. 5,27
Partnership building, affective behaviour and patient participation
Many studies measured these aspects, and more consensus is apparent, although a diverse range of factors were measured. The majority of studies suggest that there are gender differences, with female doctors showing more partnership building behaviours generally. For example, women may exhibit more facilitating and rapport building behaviours such as encouragement, attentive silences and verbal encouragement (‘mm-hmm’). In studies using direct observation or videotape, there was more non-verbal (nodding, smiling) positive communications. 5,12,17,28,29 In addition, female doctors are reported to show lowered levels of dominance during consultations and a more submissive tone of voice towards the end of a consultation. 5,18,30 Studies of affective behaviours such as concern, warmth and empathy have also tended to demonstrate more of these behaviours in female doctors. 19,24,31,32 The effect of doctors’ gender on the amount of patient participation is unclear. Studies found either no difference, 15,33 –35 or more patient participation in consultations with female doctors. 13,24
Discussion
Female doctors spend on average over 2 min longer with patients in their consultations, though this must be interpreted with caution because of the heterogeneity of the studies and the poor quality of many of them. Nevertheless, the potential impact this small difference in time per patient could result in large differences over a working day. This is consistent with other studies that have found gender differences in doctors’ clinical activity. 6,7
Female doctors appear to engage in more rapport building behaviours such as encouragement, reassurance, lowered dominance and positive talk and may also exhibit more affective behaviours such as concern, empathy and sympathy. These findings are consistent with an earlier review which suggested that medical consultations with female doctors were more patient-centred. 3 This is also reflected in research outside the field of medicine: Tannen 36 uses the terms ‘report talk’ and ‘rapport talk’ to differentiate between the types of communication of men and women.
Gender differences may be important as communication could be related to patient compliance, satisfaction and health outcomes. Researchers have found associations between a patient-centred communication style and improved adherence and patient enablement, 37 as well as greater ‘efficacy of care’, for example through fewer referrals and diagnostic tests. 38 A systematic review by Stewart 2 suggests that shared decision making, amongst other communication styles, may affect emotional health, symptom resolution and physiological measures. In cancer patients, greater participation and decision making has also been associated with better physiological outcomes and improved quality of life. 39 However, Street et al. 40 stress that research in this field fails to consider the effect of interactions with other health professionals, caregivers, family and friends on health outcomes. In addition, research that assesses the relationship between communication and health outcomes rarely acknowledges wider physiological or social determinants that may affect the health outcomes under study. 40
As regards the limitations of our review, the quality of studies was disappointing. The evidence base is heterogeneous and made up of small studies, often lacking rigorous methods or reporting results only partially. There is a need for more rigorous evidence using larger samples of doctors, clear sampling frameworks and blinding where possible. Appropriate statistical techniques to adjust for clustering effects and confounders should also be employed, along with better reporting of potentially confounding characteristics. The majority of research in this field has been conducted in primary care settings in the US. More research is needed in other health care settings and health care systems.
Given the limited research evidence, drawing policy implications must be undertaken with care. Gender may be one of numerous contributing factors to communication between doctors and patients, and this in turn may affect doctors’ clinical activity and even patient outcomes. Even if there is a consistent gender effect, there may be lessons to learn for medical training of both men and women, or, perhaps more appropriately, of groups of trainee doctors with different instinctive communication styles, regardless of gender.
Footnotes
Funding
KB and LJ are funded by an NIHR Career Development Fellowship. The views expressed in this paper are those of the authors and not necessarily those of the NHS, NIHR or the Department of Health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.