
Abstract
Older black people in South Africa stay a part of an extended family structure well into old age, irrespective of the family’s ability to provide the necessary care. South Africa’s (SA) underdeveloped infrastructure creates an increasing cause for concern as the size of the country’s older population is growing. The result is a persistent and wide-reaching disparity in access to sufficient geriatric care for older people, especially across racial lines, due to the former Apartheid regime and change in traditional African family contexts. The affiliated study formed part of a larger research project. A qualitative descriptive design was employed to describe the experiences, perceptions and attitudes of older black women regarding long-term care (LTC). Data were collected through two focus-group discussions and analysed thematically. Against the historical background of South Africa, an Ubuntu worldview, and a shift to a more modern African society, it became evident that formal LTC is inaccessible, and that informal LTC can no longer be provided by the younger generation and other extended family members. Among the participants, these two factors create significant ambivalence in having their future needs met.
Introduction
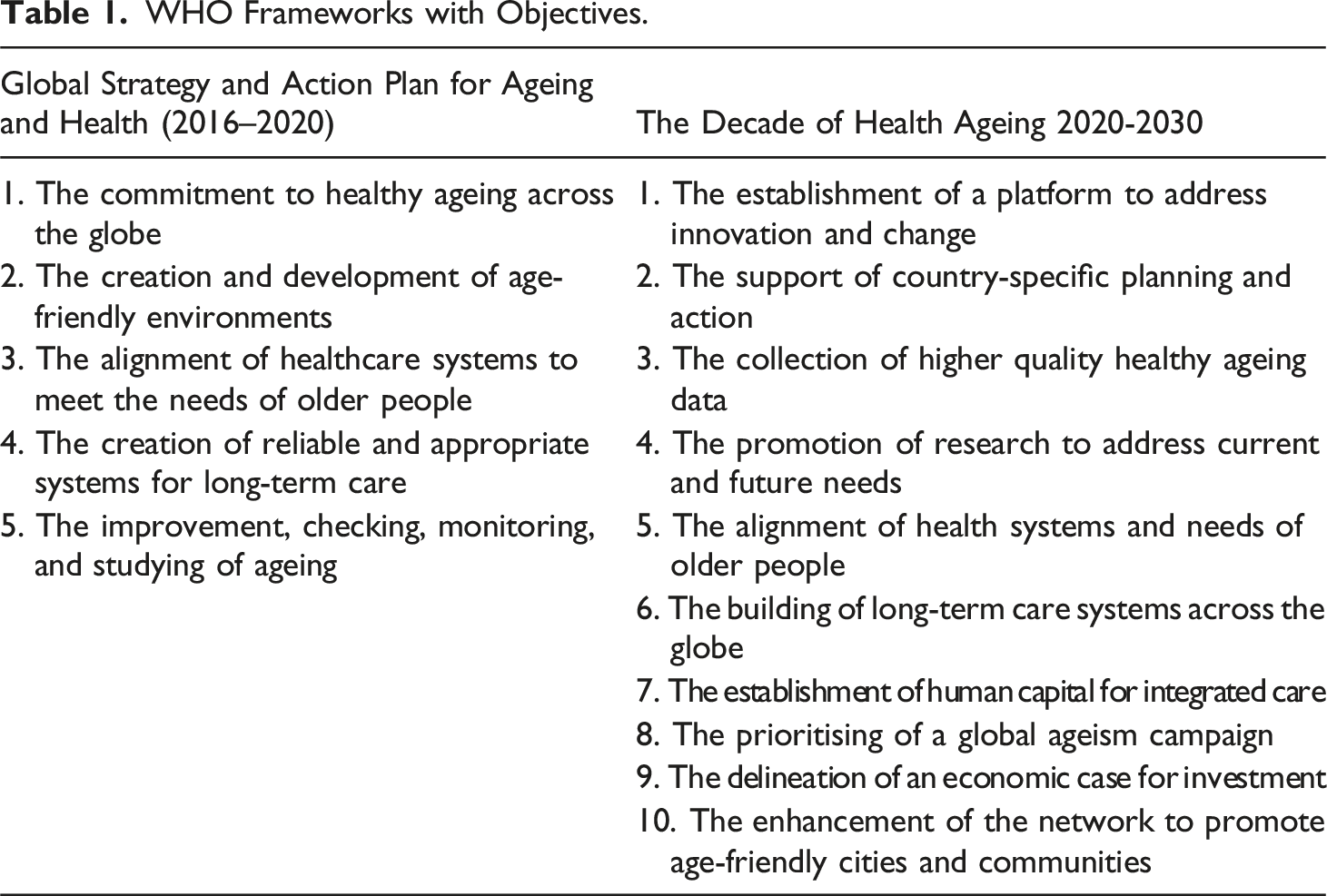
WHO Frameworks with Objectives.
Long-term care (LTC) is defined as ‘activities undertaken by others to ensure that (older) people with a significant on-going loss of intrinsic capacity can maintain a level of functional ability consistent with their basic rights, fundamental freedoms, and human dignity’ (WHO, 2015, p. 127). LTC not only supports the idea of healthy ageing but places the responsibility of LTC provision on appropriate systems that include home, community, and institutional care (Rudnicka et al., 2020). An existing body of research emphasises the importance of LTC for older people and ageing with dignity and maintaining basic human rights (Aboderin, 2005, 2012; Aboderin & Ferreira, 2009; Joubert, 2005). Despite this, there is a lack of research on the normative experiences of those within formal and informal networks of care, especially in developing countries such as South Africa. Here it should be noted that other developing countries won’t necessarily share the same attitudes and perceptions of LTC as LTC for older South Africans competes with many other pressing policy priorities, which are often related to the lasting effects of Apartheid, and HIV and Aids (Lloyd-Sherlock, 2019; Nabalamba & Chikoko, 2011).
South African disparities and formal long-term care
The South African older population is estimated at 5.4 million, which accounts for 9.1% of the entire population (see Statistics South Africa, 2011). From these statistics, it is estimated that South Africa’s formal LTC facilities are mainly used and accessed by older white individuals (Lloyd-Sherlock, 2019), even though this racial group only represents a significantly smaller portion of the total older population (Stats SA, 2011). In contrast, the larger and majority black population of South Africa does not have access to formal LTC facilities due to various socio-economic factors which impede healthy ageing (Lloyd-Sherlock, 2019). Moreover, it is evident that black individuals born in the early Apartheid years (1948 – 1958), who faced major social and economic inequalities, still struggle with access to quality geriatric care (Ananias & Strydom, 2014; Hosegood & Timæus, 2006; Lloyd-Sherlock, 2019; Stats SA, 2011). Within the South African context, unpaid family care by female relatives, unregulated formal LTC services, and privileging of older white individuals as a result of the former Apartheid system, impede healthy ageing and the quality of formal and informal LTC in South Africa (Lloyd-Sherlock, 2019). Within poverty-stricken environments, it is also documented that problems result from familial care structures (see Cohen & Menken, 2006; Kautz et al., 2010; Ramashala, 2001; Schatz & Gilbert, 2014). There is also a continued discourse in the body of research on South Africa’s older population in which it is suggested that LTC-models should be reconsidered – as care should take place within families and extended families (Aboderin, 2005; Hoffman, 2016; Schatz & Seeley, 2015).
Families and informal long-term care
Aboderin (2005) describes the family as an organisation accountable for caring for older people in the African context. This is rooted in the beliefs of filial obligation as assimilated by an Ubuntu worldview. Motho ke motho ka batho babang or umuntu ngumuntu ngabantu, which translates to ‘I am a person through other persons,’ is the guiding principle under which Ubuntu functions (Broodryk, 2008). The moral theory underlying Ubuntu represents an understanding of what it is to be human in both a familial and a communal context; it tries to capture the essence thereof, and what is essential for human beings to find fulfillment and to grow (Shutte, 2001). It emphasises community and life within a community and enhances solidarity as individuals, their community, and the world are considered connected (Chuwa, 2014). Van Niekerk (2013) explains that the concept of Ubuntu is invoked to capture an assemblage of traditional African morals and ethics, such as humanness (Broodryk, 2008; Shutte, 2001), group solidarity, reciprocity and sharing, caring, compassion, respect, and other values that ensure quality community life, such as responsiveness and participation (Broodryk, 2008; Chisale, 2018). These values encompass the characteristics of informal care provision for older individuals from an Ubuntu perspective (Chisale, 2018). Informal long-term care can thus be divided into two key categories, namely family-based and neighbourhood-based care that is driven by ‘responsiveness’ and ‘participation’ as fundamental elements of African traditional values, i.e. familial and communal response and participation when someone is in need of care (Chisale, 2018). In post-Apartheid South Africa, President Nelson Mandela drew on Ubuntu to create a consensus, a degree of reciprocity and values which are shared (Hailey, 2008). It has been part of a process in which concepts of morality and citizenship have been shaped in post-Apartheid South Africa (Swartz, 2006; as cited by Hailey, 2008). As such, the principles underlying Ubuntu as a theory of morality has informed many policies, for instance the South African Older Person’s Act 13 of 2006. The Act prioritises community-based care, support services, and familial care and suggests that the family should be central to the care process of older individuals. This further promotes the central position of older people in the structure of South African families (Malherbe, 2007). However, Lloyd-Sherlock (2019) uncovered that the discourse regarding the older black population who has access to adequate informal LTC from family members appears wanting and oversimplifies cultural differences across racial groups. The structure of the South African family has changed over the past decade and attention is increasingly being placed on individual accomplishment and the nuclear family, as opposed to a focus on the individual providing for extended family (Amoateng et al., 2007; Golijani-Moghaddam, 2014; Mokomane, 2012; Seekings, 2009; Walsh, 2015).
Based on the historical background of the country and the changing of traditional views within black families, LTC in South Africa may be considered a modern-day challenge (Lloyd-Sherlock, 2019). Moreover, not much is known about the South African family’s capability to provide care to older persons (Aboderin & Hoffman, 2015; Joubert, 2005; Van Aardt & Roos, 2016). It is, therefore, important to understand the nuances of care for older people, especially older black people in South Africa, which is rooted in the country’s current socio-economic realities as well as the consequences of Apartheid and the modernisation of traditional values. Research also suggests that where familial care has been employed, the majority of care provision is left in the hands of female relatives (Akintola, 2004; Joubert, 2005; Lloyd-Sherlock, 2019; Uys, 2002). This study endeavoured to explore and describe older black women’s perceptions and attitudes of formal LTC, led by the following research question: What are older black women’s perceptions and attitudes of long-term care? This understanding describes the nuances of older black women who were directly influenced by Apartheid within a community where beliefs encourage families to provide care irrespective of the ability of families to do so.
Methods
Research context
The study presented is an affiliated study that forms part of a larger research project entitled: ‘The future of long-term care for vulnerable older adults in Sub-Saharan Africa: A South African case study’. The larger research project formed part of an international initiative to explore and understand formal LTC for vulnerable older people in Sub-Saharan Africa (SSA). The larger research project explored formal LTC through three related, but different, phases and data were collected in South Africa and Malawi. The overall aim of the larger research project was formulated as follows: To understand how formal provision of LTC for vulnerable older adults (aged 50+) in Sub-Saharan Africa can be reconciled with informal care provision to plan interventions that can mitigate the risk of unmet care.
Study design
The affiliated study employed a qualitative research approach with a qualitative descriptive design. The approach aided in exploring and describing the perceptions and attitudes of LTC among older black women. This design provided the framework to collect a detailed summary of events written in the everyday language situated in the context of those events, that both the researcher and, importantly, the participants can agree on (Sandelowski, 2000, 2010).
Procedure and data collection
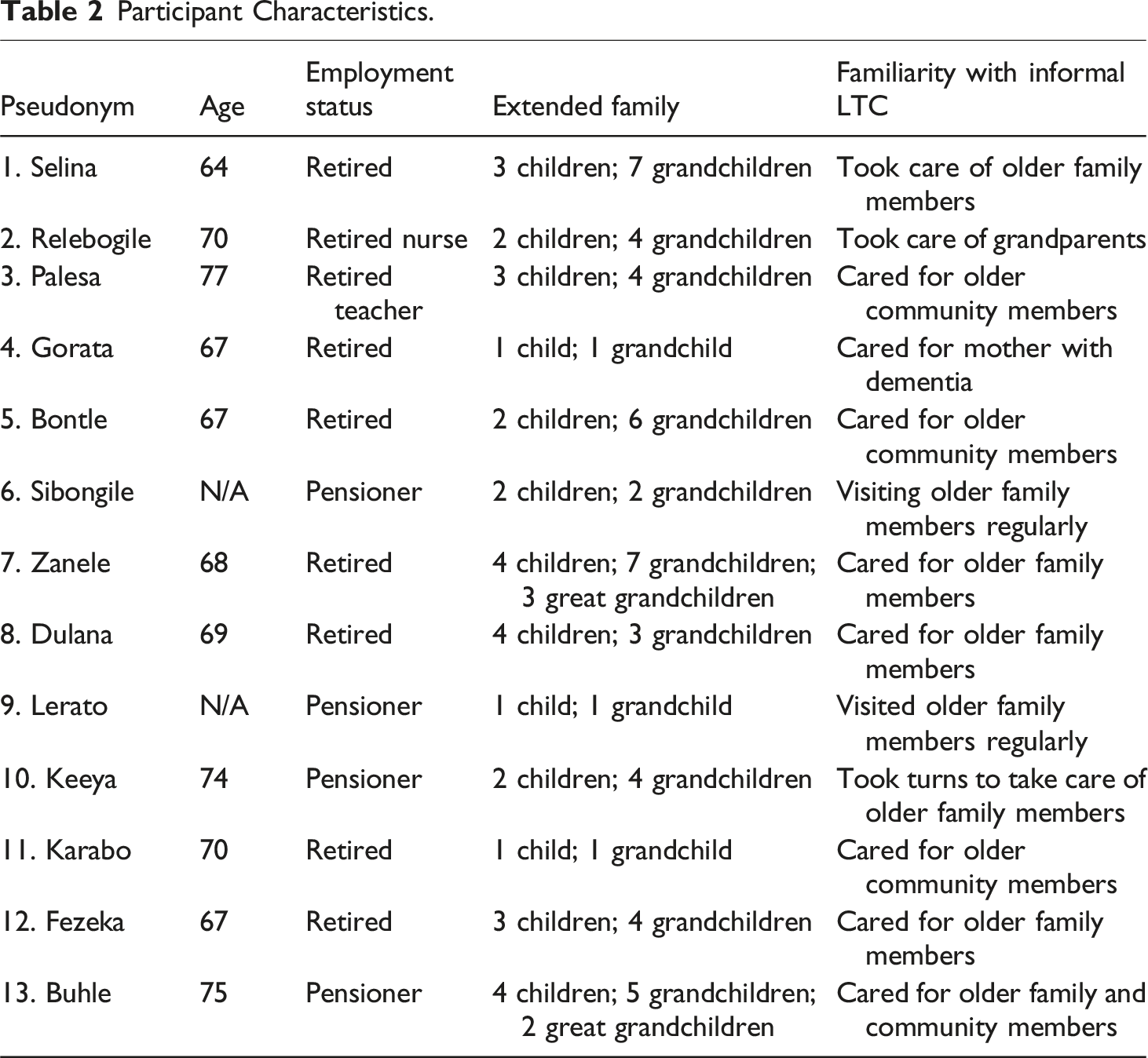
The participants (n = 27) were older women who were directly affected by the Apartheid era and currently reside in an area (Orlando, Soweto, South Africa) that gave rise to anti-Apartheid freedom fighters. These women were on the receiving end of racial discrimination, disadvantage, and marginalisation (Ananias & Strydom, 2014; Hosegood & Timæus, 2006; Stats SA, 2011). The participants were introduced to the research team before discussing the research process wherein the participants suggested a group discussion instead of individual interviews. These discussions were conducted in English, to which the participants agreed and consented. Consequently, the research team followed the methodological principles of focus group discussions. Patton (2002) explains that focus groups are aimed at collecting high-quality data within a social context. This data collection method allows for the collection of data that captures nuances at both group and individual levels (Phillippi & Lauderdale, 2018). Furthermore, the guiding principle of ‘I am a person through others’, sheds some light on the meaning-making process of individuals with an Ubuntu worldview; that is, the meaning participants add to their experiences, perceptions and beliefs happen through co-construction. By employing focus group discussions, participants were placed in a situation where co-construction was possible, arguably allowing them to comfortably explore initial ideas and add more value and nuance to their own and each other’s perceptions. This ultimately contributed to thick descriptions of the phenomenon. The focus group discussions were completed using open-ended questions and were recorded with the participants’ permission. The initial starting point of discussion was ‘what long-term care means to you’.
Participant Characteristics.
Data analysis
Data were analysed using thematic analysis. According to Braun and Clarke (2006), thematic analysis is focused on identifying, organizing, and describing patterns found in data. Furthermore, thematic analysis provides a rich, detailed, and nuanced account of the data and experiences of participants (Braun & Clarke, 2006; Clarke & Braun, 2013). Common threads across the entire set of interviews were identified by following six steps proposed by Braun and Clarke (2006): Firstly, becoming familiar with the data by reading and re-reading it to identify meaningful patterns. Secondly, generating initial codes by reviewing the patterns deemed meaningful to identify important and interesting aspects of the data. Thirdly, searching for appropriate overarching themes by analysing and reviewing the codes. Fourthly, reviewing the themes whereby main themes were identified and refined. This step also included reworking and/or creating new themes. Penultimately, interpreting, defining and naming the themes. Lastly, producing the report. To contribute to the trustworthiness of the process, verbatim quotes from the dataset are provided to support each theme. The entire process continued until the research question was answered and data saturation was reached.
Ethical considerations and trustworthiness
The Health Research Ethics Committee (HREC) of the North-West University, approved the affiliated study: NWU00239-15-S1. To enhance the quality and integrity of the presented study and larger research project the authors employed the following strategies as outlined by Cohen and Crabtree (2006) and Shenton (2004). All unclear data during the familiarisation process of the data analysis were discussed with the initially appointed data collector. All methodological aspects from the larger research project and affiliated study are discussed and disclosed. The findings were continuously discussed with the second author (CP) and the appointed data collector to ensure that the findings were objective and without personal bias, personal motivations, and interests.
Findings
Older Black Women’s Perceptions and Attitudes of Long-Term Care.
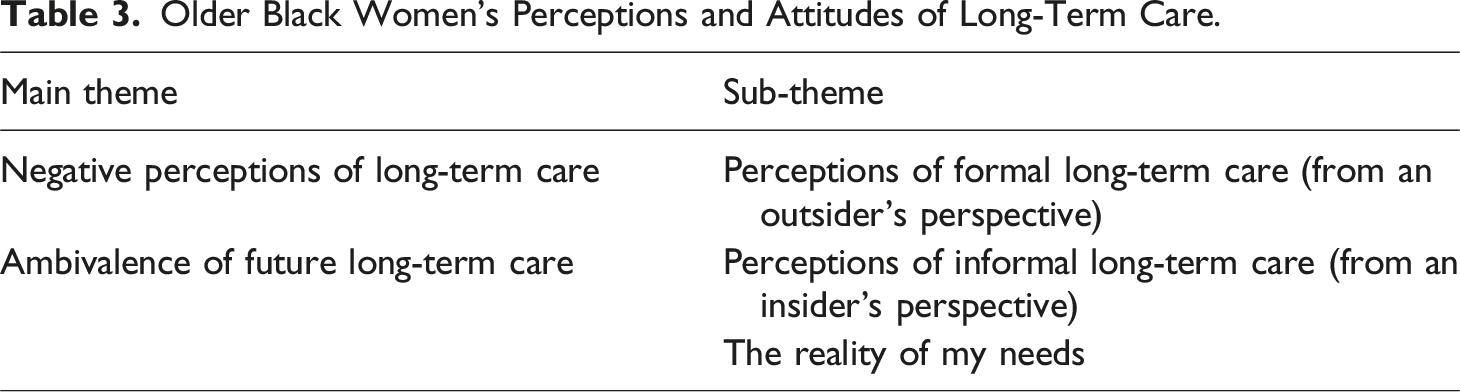
Negative perceptions of LTC
Negative perceptions refer to the participants’ negative views and/or negative preconceived notions of both formal and informal LTC. The research participants are still living independently, and some take care of either their grandchildren or adoptive extended family members. The negativity is linked to how participants perceive or experience both forms of care, either from an insider’s or outsider’s perspective.
Perceptions of formal long-term care
This theme refers to these women’s perceptions of LTC embedded in the experiences of formal LTC in their community from an outsider’s perspective, i.e., observations they have made about the formal LTC of others. These findings reflect the participants’ personal experiences of either visiting people in formal institutions in their community or having several encounters with a family member receiving care at a state-owned facility. Selina shared her perception as an outsider; ‘the people [community members] are trying in our communities to take care of [older people], you know, going around, giving them food, washing [bathing] them, you know, you’ll find that some are not cared for or mistreated, you know, they complain that, you know Hospice [terminal care facility], eh, it’s…it’s terrible.’ This perception resonated with the contribution of many other older women around the table. Sibongile added; ‘You hear the stories, you know, or you see it. We go there [formal care facilities] sometimes and see they don’t take care of the older people. They [employees at formal care facilities] eat [use] the pension [funds], they stay in the same clothes every day…it is not good.’ Palesa contributed; ‘…and that [old age] homes in Soweto are terrible. We have to go to a neighbour who is, eh, at Mphulo [SP], eh, Elderly Home. So, uh, when we came to…to that place [Home in Soweto] it was not nice, we saw things. People say, when we take the older people there, they have nice clothes, [but] these people [caretakers in homes] take them. They [caretakers/nurses] are very careless. When you give them [older people] food in bulk, they [caretakers] divide it amongst themselves and don’t share with the older people. And it all comes to the point that the people who care for the aged it’s not in their heart.’ Most of the older women around the table told stories that emphasised negative impressions of institutional care and a perceived lack of carer compassion.
Furthermore, their experiences of formal LTC are entrenched in feelings of powerlessness and lack of autonomy. This can be seen in Gorata’s statements; ‘Where we…we care for each other, really. That kind of a home one can consider and say, okay, I wouldn’t really mind going there…’ she continued: ‘…not to be thrown in hamba [disrespectful way of dismissing someone]. No, not the hamba that I am going.’ This resonated with Bontle’s narrative; ‘So we have to be stuck in our houses and, when our children are tired of us, they can send us to a home.’ Relebogile added; ‘…They just dump them [older people] in there.’ Sibongile retorted; ‘And when you recover and you want now – … to go back home, you can…you cannot go back home because your children have opted for you to live there. Sometimes, eh, as, eh, it was mentioned, uh, it’s this fear now what is going to happen to my house? What is going to happen to my furniture? You know…’ These perceived feelings of powerlessness were evident in the discourse of the majority of the women and undoubtedly contributes to the negative perceptions of formal LTC.
Perceptions of informal long-term care
Informal LTC as an insider refers to informal forms of care familiar to the participants. Most of the informal care they reflected on was within the context of the extended family and its structural changes. The women’s reflections on these changes were mainly concerned with the attitudes and lack of knowledge among the younger generation and the community. Lerato shared her perception about the structural changes within the extended family; ‘If I’m old, my sister can take me or my mother can…or my…my aunt can take me. So, the extended family is now also shrinking and so, if the…the extended family shrinks and you have this family, it’s me and my children, and, you know, that kind of family, definitely show the structures of the family are changing as well. It means, even other things in the…in the…in the communities must change. We are not forcing…isn’t it? You are not pushing…it’s not being pushed but highlighting people that, you know what? The elderly people you…you…you can no longer depend on the…the…the extended family. Somewhere…somewhere…some people don’t have anybody.’
Zanele also shared her perception of the structural changes within the extended family and its perceived effect on the attitude of the younger generation; ‘… eh, … spoke about are the children of…after ninety-four [1994 – the start of democracy] still the same? They are completely different – …because, eh, before ninety-four, we still had – …we still had that, eh, extended family as [INDISTINCT] in our lives but right now, after that, we have a new, eh – It’s almost everybody…everyone for himself – So our children are looking at themselves – …and they are [INDISTINCT]. They don’t care about what their…their parent…as…and they forget that they are where they are because of us. We sacrifice so much for our children, you know, to make them have a better life but the minute they are up there, they forget where they come from. We used to not to forget. I remember… So that care that used to be there before is no longer there.’ Palesa’s perception resonated with the perception of structural changes within the extended family and the attitude of the younger generation; ‘…to be moved, you know. Today I’m with my daughter. Uh…uh, maybe the following two months I’m with so-and-so…Though they love you, though they care for you, but you still need your little bedroom. Ja [yes], it’s…and…and they ask that question [INDISTINCT]. When is she going to die? [INDISTINCT]. Yes, I mean, they are…they are…they…they know that granny so-and-so died and now you are eighty it means you are also going to die. [CROSSTALK] …going to die. Those are some of the things but, eh, those are beside the point but, for you to be moved from this one to that one, you…you see yourself as a burden as well.’
This highlights that the attitude of the younger generation is embedded in a lack of care and knowledge of care. This perception links to Dulana pondering on the idea of her children providing informal LTC; ‘How do they take care of me even when their friends are there? Are they going to lock me up in the room, and I start beating [them] with a stick?’ She continued to explain that this perception was based on the experiences of an acquaintance; ‘You see. I had a friend. She’s a lady teacher. Her mum became demented and, because they really did not understand it, her mum, whenever they were flushing the toilet, she thought somebody’s…is saying ssshhh [keep quiet] to her and, at some stage, when they came back…because she used to be alone at home, they were not aware that, really, she’s…she’s not up-to-date in her mind anymore. Coming back from…coming back from home, they found the toilet broken to pieces because she was beating these ‘people’ who were always saying ssshhh [keep quiet] to her in her house. So, if they had been educated about these conditions, then they would have thought we…we can’t leave her all by herself because she is not safe at all.’ Whereby Gorata responded by referring to the lack of care and knowledge of such care among the younger generation and the community as a whole; ‘Your thinking is no longer as sharp as it was. And there are diseases that attacks the brain. The aged, most of them, suffer…suffer from Alzheimer’s, they suffer from dementia, and then, when they have dementia, they will be roaming the streets, you know, and, in our African land…in our African culture, a woman can’t just go about naked and that.’ Whereby others contributed; ‘They will label you. They say it’s a witch. Meanwhile, it’s not because she is a witch. It’s because her mentality has changed.’ Keeya contributed, saying, ‘Those are the things that happen and then children will be throwing stones at you because now you are labelled a witch.’
These contributions encapsulate the perceived threats to the structural stability of the extended family as observed or experienced by the majority of these women. The group concluded that education is needed to address these threats, as Relebogile stated; ‘We need to think of how are we going to take the information forward to young people to educate them about how to take care of their parents or family or those, you know…or a member of a family.’
Ambivalence of future long-term care
Ambivalent perceptions refer to the perceived future-orientated uncertainty experienced by the participants. This theme emerged from the narratives of the perceived reality of the participants’ needs and the problems accompanying both formal and informal LTC. This state of ambivalence is characterised by these women acknowledging that they would need some form of care in the future, but due to socio-economic realities and traditional norms, they experience uncertainty as to which route to take in terms of care. Their future needs were contextualized against their communal beliefs and moral position, socioeconomic status, and their family capital.
The reality of my needs
This theme refers to the participants’ perceptions of what might happen to them in the near future. It contains their perceptions of needing and/or receiving formal or informal LTC and the perceived reasons and conditions for considering one or the other. These reasons are based on the cultural beliefs of this community as embedded in the historical class and economic division of black communities in South Africa and the availability of the younger generation. These reasons are clouded by their state of ambivalence and uncertainty regarding their future. Karabo reflected on her perceived need for care; ‘The older you become, you…you become sensitive of tomorrow and that I’m growing older and older and perhaps somewhere I’m not going to be able to move around. What’s going to happen to me? You ask yourself, who will take care of me?’ The uncertainty she, and the rest of the group, felt about their future became evident in most of these women’s stories, as Fezeka relates; ‘People are living longer than they used to live. I don’t know the cause but I have noticed that, you know, people reach…you know, people…when you were retired, we are saying, joh, I’m sure, by seventy, I will be gone and ten years looked to be such a long, eh…eh, period but now you look at it. Ten years is just nothing. And people are growing older, they are reaching their hundreds –…over hundred. So, we don’t know…when we are already hundred, then you’ll don’t know how to walk, who is going to look after you?’
This uncertainty may be rooted in this community’s normative beliefs of formal LTC, as Bontle summarized; ‘Um, the…the concept of, em, old age homes, um, in our communities, goes back with history. Um, our culture doesn’t, eh…eh, expect us to remove the elderly to a strange or a different environment where there are no family members to take care of them…’ This reflection resonated with Karabo who emphasized the historical background and added her take on the current government; ‘So history has led to…to this and, even with the…the current government, old age homes do not exist…is…is a concept that doesn’t exist in…in their minds and in their…in, you know, programmes.’ Keeya shared her perception, which is grounded in the historical class and economic division of the black communities in South Africa; ‘Yes, there are some home-based, eh, caregivers who are trained now, these days, but, previously, we didn’t have such because um, we were communities that, you know, were looked down upon. Facilities that would keep us in good conditions were not for us. They were for the haves….’ And Buhle added; ‘Another thing is training or giving people, you know, the…the knowledge, the skills, is non-existent in our…in our country, except for the haves but the have-nots, those things…as though we don’t age. It’s only the haves who age. It’s only the haves who retire…’ Based on these reflections, Karabo came to the following conclusion about formal LTC; ‘So such things have made us not even think or consider old age homes. In fact, they’ve given us a negative concept and a…a lot of people just don’t feel like going to an old age home….’
These women’s uncertainties are further deepened by the previously discussed structural changes within the extended family, and the unavailability of younger generations to provide informal LTC, as can be seen in Lerato’s statement; ‘You know, it’s really very, very difficult for the aged. I…I don’t know where we are going to [INDISTINCT] because the other thing is that, funny enough, in life, there is longevity now – Because even your children, at that time, they will be in their whatever years and they will be caring for themselves and their own and you won’t be included in their circle of life. So, it is a very difficult [INDISTINCT].’ Similarly, Fezeka expressed; ‘Somewhere…I don’t know how, eventually I’m going to, and I may need to be in a home of some sort because the children are still working. You see. So, all of us need protection. All of us need to protect somebody.’ This not only highlights the unavailability of the younger generation but further brings to light this community’s beliefs.
Discussion
In the face of the perceived disintegration of the extended family and societal norms – entirely at odds with a worldview and moral position built around Ubuntu – these participants find themselves with a lack of options and opportunities when planning for their future, and those around them. In planning for their future care, the participants need to select between either formal or informal LTC. However, neither of these is seen as viable due to both the real and perceived flaws present in both paths. Although the socio-political context of South Africa has undergone many changes since 1994 (start of democracy), it is evident that many of the participants’ future care decisions are still influenced by the consequences of Apartheid. Consequently, formal LTC remains non-viable for these women, not only due to fears of systemic neglect, mistreatment, and abuse (Ananias & Strydom, 2014; Ferreira & Lindgren, 2008), but also because formal LTC is perceived as geographically, socially, and economically unobtainable (Lloyd-Sherlock, 2019). The majority of participants have taken on a strong caring role in the lives of their relatives and community members, and as such have directly witnessed, and are privy to reports of abuse and neglect of older individuals within formal LTC institutions. These experiences and perceptions are also rooted in South Africa’s historical class and economic division of black communities. Informal LTC is their only perceived alternative, but this also comes with a host of problems that are directly antithetical to their ideal form of informal LTC – whereby family members take care of their older relatives. Their preference for familial care can be assigned to their cultural values. According to Fang and Yang (2023), cultural values play a pivotal role in choosing a primary caregiver. Traditional cultural values place emphasis on family traditions and familial ties. Informal LTC is thus more likely to be preferred by older adults with traditional values that stress connections between family and community members. The principle of care is integrated and embedded in Ubuntu as a moral theory and abiding by this principle is proof of personal and communal moral maturity (Chuwa, 2014). Shutte (2001) explains that with regards to Ubuntu as a moral theory, one’s deepest moral obligation is to become ‘fully’ human, which can only be achieved by reciprocating care, being compassionate and respectful, and delving deeper into community life to enhance group solidarity (Mpedi, 2008). Ubuntu promotes life-centred ethics to ensure a quality community life (Broodryk, 2008; Chuwa, 2014). It functions under the guiding principle of “I am a person through other persons” (Broodryk, 2008). Thus, focusing on the enhancement of group solidarity, and encourages traditional African morals such as reciprocity, care, compassion, respect, and ultimately ‘humanness’ (Chuwa, 2014; Van Niekerk, 2013). These principles subsequently encompass the characteristics of informal care provision for older individuals, as it is based on a support network rooted in the above-mentioned principles to ensure quality community life (Broodryk, 2008; Chisale, 2018). However, there has been an increased focus of said generation on individual success and provision for the nuclear family, as opposed to the extended family (Amoateng & Heaton, 2007; Mokomane, 2012; Seekings, 2009). According to Makiwane and Berry (2013) and Milligan (2016), the disintegration of the extended family is one of the major aspects of change when traditional households transform into modern households. The process of modernisation consequently results in the inability, and unwillingness of the younger generation to provide for the aged. One woman reflected that after 1994 the extended family began to disintegrate as a result of the growing attitude amongst the younger generation of ‘everyone for [themselves]’. According to Pinquart and Sörensen (2006), women are more likely to expect informal support from their adult children because they have been their children’s primary caregivers. For some, particularly women, being cared for by their adult children is an indication of the regard they have for them (Edwards et al., 2001) and within the traditional African value system, it is also deemed a sign of respect (Mpedi, 2008). As Mpedi (2008) confirms, the community reciprocating care to older persons acts as a sort of payment for the contribution these persons provided to the community in the first place. These women now find themselves in a position where the time and resources they have devoted to caring for those in their community no longer guarantee the care that they had once reciprocated. Ananias and Strydom (2014) depicted the social shift as being a result of the younger generation living further away from their parents in the current socio-economic climate, the high cost of living, and the imperative of employment.
Running parallel to a common perception of a changing society, as discussed above, is an understanding that providing care is inherently taxing, and people are less willing to fulfil this type of responsibility (Edwards et al., 2001). This is evident among the participants who hold the unusual position of not wanting to be a burden to their children. This position is considered unusual as it exists in opposition to social and traditional values of reciprocity and group solidarity within the traditional African worldview. This further marks the second change from a more traditional household to a modern one (Milligan, 2016). However, from an individualistic framework of care, research suggests that although some individuals may wish to be cared for by their children, they do not want to be a burden as their children have their own lives to lead (Cahill et al., 2009; Edwards et al., 2001; Ward-Griffin et al., 2006). The culmination of these factors marks the disintegration of the reciprocal care element of Ubuntu as a moral framework. This discussion encapsulates the current perceptions and attitudes of these women, and may be subject to change. In the wake of the seeming disintegration of the factors that are essential to Ubuntu as moral framework, familial care may also become a less popular option which may consequently lead to more individuals opting for formal LTC.
Limitations and recommendations
The study consisted of 27 female participants drawn from a specific urban location and therefore the findings cannot be generalised to the larger black South African population. The participation of males could have offered a more diverse range of perceptions and attitudes of LTC. Although English was the agreed upon language used in the Focus Groups, deeper intensities and nuances of contributions might have emerged if the primary languages of the participants were used. It is recommended that future LTC research could be brought in line with the WHO (2015) framework objectives outlined in the Decade of Health and Ageing 2020-2030.
Conclusion
Formal LTC poses an alien, uncaring environment that serves as not only a counter to the participants’ best interests but so too their entire ontological framework. Informal LTC, although based in a familiar environment, still poses threats of abuse rooted in a lack of knowledge, the unavailability of the younger generation to provide care, and the perceived disintegration of the extended family. Atop all these obstacles lies a turmoil in which the modern reality no longer resembles the once on-going system of reciprocity that these women had participated in – not only for the care of those around them but as an investment for the future of their own care.
These factors ultimately result in the women experiencing a state of ambivalence, embedded in a future-orientated uncertainty, and the disintegration of the principles of Ubuntu. Until these perceived problems are addressed, the future of their wellbeing and the basic right to healthy ageing is steeped in uncertainty.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
![]() .
.