
Abstract
People with MS may be at heightened risk of intimate partner violence (IPV) compared to the general population; however, little is known about the prevalence of IPV among people with MS or its effects on MS-specific clinical outcomes. Additionally, while MS clinicians often discuss family planning with patients, many clinicians may have received little training in detecting and responding to IPV. Moreover, no studies have investigated how to implement IPV case-finding and resource provision in the MS clinical setting. Overall, there are several scholarly, educational, and implementation-related gaps in IPV-associated care for people with MS. This article aims to summarize the available literature on IPV in people with MS, identify future research questions, and aid MS clinicians in safely addressing IPV while awaiting vital MS-specific knowledge.
Intimate partner violence (IPV) refers to actions by a current or former partner that can cause harm. 1 Also known as domestic violence, IPV can include physical violence, sexual violence, stalking, economic abuse, and psychological aggression. Often under-recognized and insufficiently addressed by clinicians, IPV occurs across diverse populations and jurisdictions and can lead to serious injury, and even death. People with multiple sclerosis (MS) may constitute a specific group at increased risk of IPV.
In the general population, risk factors for victimization by IPV include female sex, younger age, living with disability, comorbid psychiatric conditions, and alcohol use. 1 Many of these same factors are characteristic of the MS population, with MS being more common in women, commonly presenting with comorbid psychiatric conditions, and potentially resulting in neurologic disability. 2 Recent studies estimate that 38%–63% of women with MS have experienced abuse, most commonly perpetrated by intimate partners,3,4 and possible risk factors include physical disability, fatigue, and cognitive impairment.3–5 However, these studies are limited by small sample sizes, narrow geographic regions, and the absence of healthy control comparison groups. Also, no studies have examined the prevalence of IPV among men with MS or people who care for those with MS. Overall, existing conceptual and epidemiological evidence, while preliminary, suggests a link between IPV and MS.
To date, no studies have evaluated the relationship between IPV and clinical or patient-reported outcomes in MS, emphasizing the pressing need for investigation. In the general population, IPV is associated with injuries, homicide, reduced quality of life, chronic pain, sleep disorders, disability, gynecological illness, sexually transmitted infection, depression, post-traumatic stress disorder, and numerous other adverse physical and mental health outcomes. 1 IPV also exposes children to violence, amplifying their risk of mood, anxiety, and substance use disorders. 1 Developmental exposure to IPV can also raise the risk of later engagement in violent relationships, potentially leading to an intergenerational cycle of violence. 1
Of relevance to people with MS and their families, adverse childhood experiences may increase the risk of children later developing MS. 6 People with MS who report prior traumatic experiences may have an earlier onset of illness and higher relapse rates, but these findings require replication and prospective study. 6 A recent large prospective cohort study reported an association between childhood emotional and sexual traumatic experiences and the future development of MS. Also, it demonstrated an increased likelihood of MS when women experienced multiple types of childhood abuse. 7 This research suggests an exposure-response relationship between adverse childhood experiences and the future risk of MS. One could hypothesize that violence is one potential non-genetic mechanism for the intergenerational transmission of MS; however, investigation of this potential link remains needed. The current literature highlights the possible impact of IPV on morbidity and mortality in people with MS and the necessity for disease-specific analysis.
MS clinicians play an essential role in addressing IPV. As emphasized by Krysko and colleagues, many patients diagnosed with MS aim to have children, and family planning is a common focus of neurological clinical encounters. 8 The perinatal period can also be high-risk for IPV with potential negative maternal and neonatal consequences. 1 At the same time, many neurologists may be unaware of how to identify and safely address IPV, contributing to a reluctance to incorporate this topic into complex family planning discussions. For example, in a database of 830 patient visits at an academic MS center, no MS clinicians had flagged any encounters for patient abuse or neglect. 3 In contrast, at the same clinical site, approximately 40% of patients with MS reported prior abuse, of which 16% described it as occurring in the past 12 months. 3 There is therefore a need for IPV-focused neurological training and regular collaboration with colleagues in social work, nursing, psychiatry, obstetrics, and family medicine. All healthcare team members can support the trans-disciplinary goal of addressing IPV. It is also salient to re-emphasize that little is known about the impact of IPV on MS clinical outcomes, highlighting the need for prospective studies on IPV and its effects on MS disease progression and quality of life. These findings would be relevant to include in family planning discussions.
While awaiting additional research, MS clinicians can identify victims/survivors of IPV during clinical encounters. Although randomized-controlled trials do not support universal screening for IPV, most guidelines emphasize the role of case-finding. 1 This approach involves being alert to signs and symptoms connected to IPV (e.g. chronic pain or somatic concerns, unexplained injuries, missed appointments) and safely asking about exposure and perpetration of violence during clinical assessments.
Given the risk of an overheard inquiry, clinicians should remain mindful of the clinical setting, ensuring privacy, support, and confidentiality for this discussion. It is also vital for clinicians to consider the legal implications of questioning (e.g. mandatory reporting to child protection services) and to advise patients of these risks before the discussion. For many MS clinicians, this discussion may involve asking families of people with MS to step out of the examining room. The Violence, Evidence, Guidance, and Action (VEGA) Project suggests a phased inquiry approach beginning with an open-ended question about home relationships. 9 For example, as suggested in VEGA Project educational resources, a neurologist could ask, “How are things at home?” 9 Afterward, clinicians should ask a specific question about IPV, such as “Has your partner ever threatened or harmed you?.” It is essential to adapt this follow-up question to the individual. People with MS may experience heightened vulnerability due to physical disability and reliance on their partners for financial or healthcare-related support. As a result, patients may fear disclosing IPV. MS clinicians should remain sensitive to these concerns, express validation and support, and acknowledge to patients that everyone has the right to live without violence. 1 After appropriate recognition of IPV, careful assessment and documentation are necessary.
From the authors’ knowledge, there are no interventional studies devoted to addressing IPV in the MS population. In accordance with the VEGA Project Intimate Partner Violence Care Pathway, it is important for MS clinicians to respond safely and determine the risk of immediate danger following the detection of IPV. 9 Cognizant that many neurologists do not have access to interdisciplinary services, we include a checklist of resources that could be compiled in each region and referred to by busy clinicians (see in Table 1). Clinicians should exercise caution with providing patients with handouts since perpetrators of violence may find these documents. For telephone-based services, patients may appreciate using the office telephone to connect in a safe environment. While following jurisdictional-specific legal requirements, if a patient is in immediate danger or in need of urgent intervention, MS clinicians can share options for immediately involving police, contacting an urgent IPV hotline, involving child protection services, or referring a patient to an emergency department or urgent care facility. 9 In addition, resources and referrals should be provided to facilitate responding to IPV, which may involve treating related symptoms or conditions (e.g. post-traumatic stress disorder, major depressive disorder, injuries), incorporating advocacy interventions (e.g. shelters, safety planning, legal services), and psychological interventions (e.g. cognitive trauma therapy). 1 Notably, it is unclear whether couples’ interventions are beneficial, and given the potential for safety risks, these interventions are not recommended. 1 With patient consent and based on their scope of practice, MS clinicians may consider referral to other services, such as social work or psychiatry, depending on the local availability of specialized resources. Throughout this process, clinicians should assess readiness for change and engage patients as collaborative partners in decision-making. If a patient declines a referral, a clinician can still provide a follow-up appointment and information about IPV and relevant services.
Clinical resource checklist for intimate partner violence (IPV). a
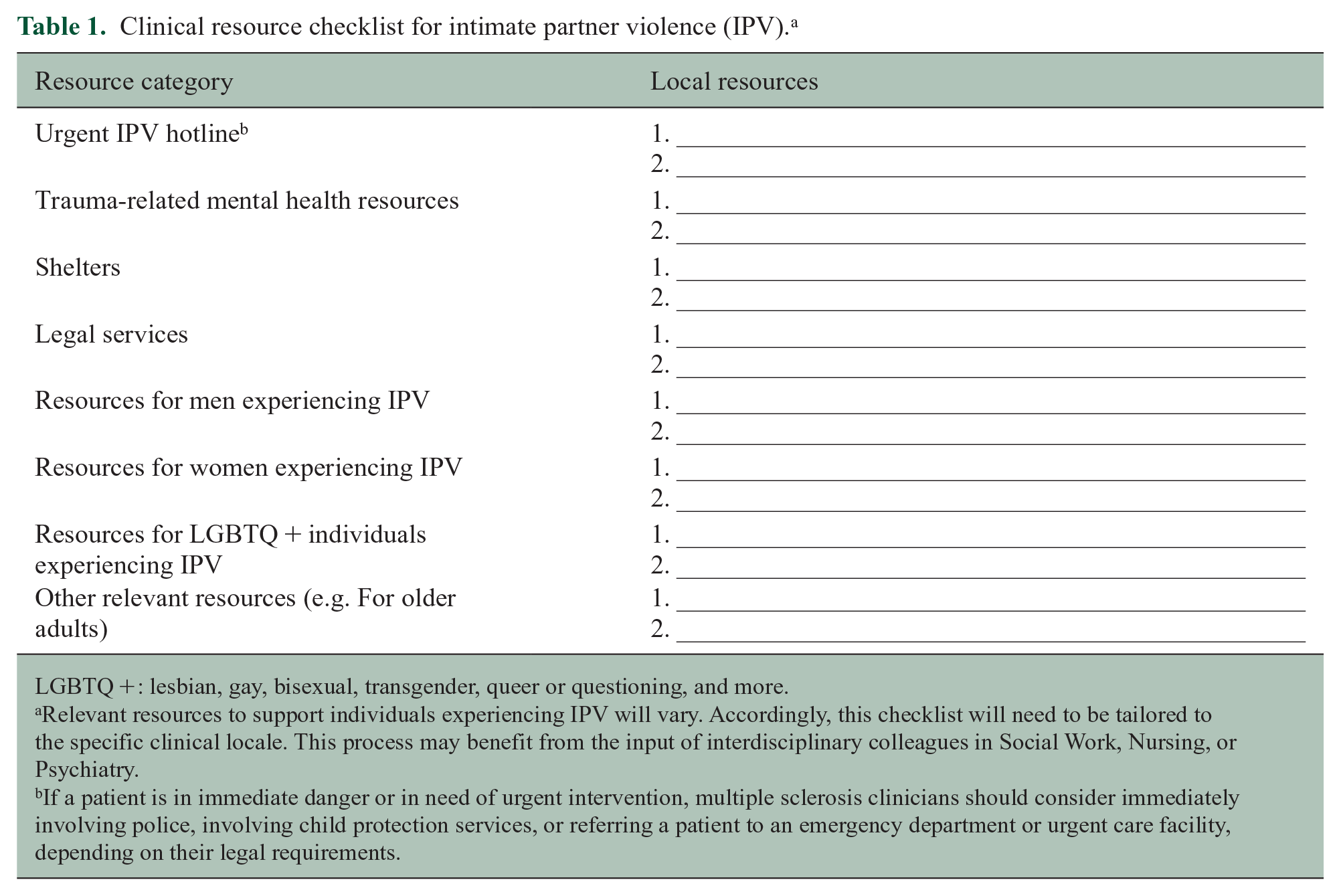
LGBTQ +: lesbian, gay, bisexual, transgender, queer or questioning, and more.
Relevant resources to support individuals experiencing IPV will vary. Accordingly, this checklist will need to be tailored to the specific clinical locale. This process may benefit from the input of interdisciplinary colleagues in Social Work, Nursing, or Psychiatry.
If a patient is in immediate danger or in need of urgent intervention, multiple sclerosis clinicians should consider immediately involving police, involving child protection services, or referring a patient to an emergency department or urgent care facility, depending on their legal requirements.
In addition to patient and organizational-related obstacles to identifying and responding to IPV, there will also be clinician-related challenges. Clinicians may not view IPV as one of their primary responsibilities. To address these perspectives, we recommend organizing group discussions among clinic staff (if working in an interdisciplinary team) or local clinical colleagues. Also, clinicians who have not received formal training in this area may perceive that they lack the necessary knowledge or skills. Potential solutions could include educational rounds dedicated to IPV or peer observation and coaching. Notably, many clinicians are already busy with MS disease management and face significant time constraints. Prior to clinical encounters, clinicians should prepare resources and practice these skills to enhance efficiency and competency in addressing IPV with patients. To address these gaps in the MS literature, implementation-oriented studies could determine how best to identify and address IPV in the complex MS clinic environment.
Across all domains, there is much more to learn about IPV among people with MS. Clinicians can seek education through clinically based online resources from the VEGA Project 9 and World Health Organization clinical and policy guidelines. 10 Clinicians can also explore services, policies, guidelines, and crisis lines in their local and national regions, and partnerships with nursing, social work, and psychiatrists can assist with developing resources to provide to those with MS affected by IPV. We hope this article will stimulate much-needed research in this field and support clinicians in safely addressing IPV among people with MS and their families.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr DEF has reviewed content from the VEGA Project educational resources. Dr KMK was supported by the Sylvia Lawry award from the National Multiple Sclerosis Society, and a Biogen MS fellowship grant during her fellowship. Dr KMK has received grants from MS Canada; a contract for a study site from Roche; speaking or consulting fees from Biogen, EMD Serono, Novartis, Roche; advisory board member for Biogen, EMD Serono, Novartis, Roche; scientific advisory committee member for Bristol Myers Squibb. Dr AF has received grants from MS Society of Canada, CIHR, and Bristol Myers Squibb; royalties from Johns Hopkins University Press and Cambridge University Press; and honoraria from Novartis.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.