
Abstract
Background/Objectives:
Delays to diagnosis of multiple sclerosis (MS) are largely unknown in sub-Saharan Africa. This study utilizes a quantitative approach to determine factors independently associated with delays to diagnosis among a cohort of Zambian people with MS.
Methods:
This cross-sectional study enrolled people with a confirmed diagnosis of MS at a public outpatient neurology clinic in Lusaka, Zambia. Standardized surveys were administered. Diagnostic delay was categorized into patient delay, health-system delay, and all delay. A multivariable linear regression model was used to determine factors independently associated with time to diagnosis.
Results:
A total of 22 participants had a confirmed diagnosis of MS. Median all delay from symptom onset to MS diagnosis was 11.4 months (interquartile range (IQR) = 4–35.5), with health-system delay accounting for the majority. Asian race correlated with a decrease in all delay, while evaluation outside of Zambia was associated with a decrease in patient delay and birthplace outside of Zambia correlated with decreased health-system delay.
Conclusion:
Black African people born in Zambia and evaluated in Zambia experienced prolonged diagnostic delays when compared to non-black Zambians born and/or evaluated outside Zambia, likely due to a combination of health system and patient factors, which necessitate further study to shorten time to diagnosis.
Introduction
Multiple sclerosis (MS) is one of the most common chronic neurological disorders in the world with the highest prevalence reported in North America, northern Europe, and southern Australia, but largely unknown in sub-Saharan Africa (SSA).1,2 Because SSA has the lowest number of neurologists per capita in the world and limited availability of brain imaging,3,4 a major ascertainment bias due to underdiagnosis is likely. A recent ecological study found that MS prevalence was lower in countries with lower healthcare expenditure per capita, reduced access to diagnostic technology, and lower number of neurologists per capita, 5 suggesting prior reports of low MS prevalence in SSA may be based on absence of data rather than true absence of disease. Recent epidemiological studies from Sudan, Kenya, and South Africa all suggest the prevalence, or ascertainment, of MS is rising among Black African people.6–8
Regional prevalence is associated with diagnostic delay of MS, which occurs due to a multitude of patient and health-system factors and can have important implications for prognosis, especially as delays in treatment initiation increase disability and even mortality.9–12 The degree of diagnostic delay varies worldwide and, with increased awareness and modifications to diagnostic criteria, has improved in many regions over time.13,14
Zambia is a country in southern Africa with a population of 20 million people and only 12 neurologists, less than 10 magnetic resonance imaging (MRI) units and often cost-prohibitive access to diagnostic testing. Since the formation of the country’s first neurology training program and expansion of specialized neurological care at the University Teaching Hospital (UTH) in the capital of Lusaka in 2018, approximately 30 patients have been diagnosed with MS. A qualitative assessment of 13 patients diagnosed with MS in Zambia found that most had long delays to diagnosis, visited multiple physicians, received misdiagnoses, underwent unnecessary tests, and had the socioeconomic means to pursue second opinions.15,16 Based upon these findings, we hypothesized that higher education level and socioeconomic status would be associated with decreased delay. While this qualitative data explores the patient perspective of causes of delay, the specific factors that increase delay to diagnosis of MS in this population remain unknown.
This study aimed to utilize a quantitative approach to determine factors independently associated with patient delay, health-system delay, and all delay to diagnosis among a cohort of people with MS (PwMS) in Zambia.
Methods
This cross-sectional cohort study was conducted in PwMS who presented for clinical care at an outpatient neurology clinic at UTH, the national referral hospital in Lusaka, Zambia, from October 2019 to February 2022. Patients could present to the neurology clinic upon self-referral or referral from another provider. Adult patients aged 18 years or older with a confirmed diagnosis of MS based on 2017 McDonald’s criteria 13 or clinically isolated syndrome (CIS) after evaluation by a neurologist at UTH were included in the study. Due to limitations in performing oligoclonal band testing at local laboratories, this criterion to fulfill dissemination in time was not utilized to aid with diagnosis; however, all patients underwent MRI. Patients with a suspected but unconfirmed diagnosis of MS due to incomplete evaluations were excluded (Figure 1). All participants in the study provided written consent.
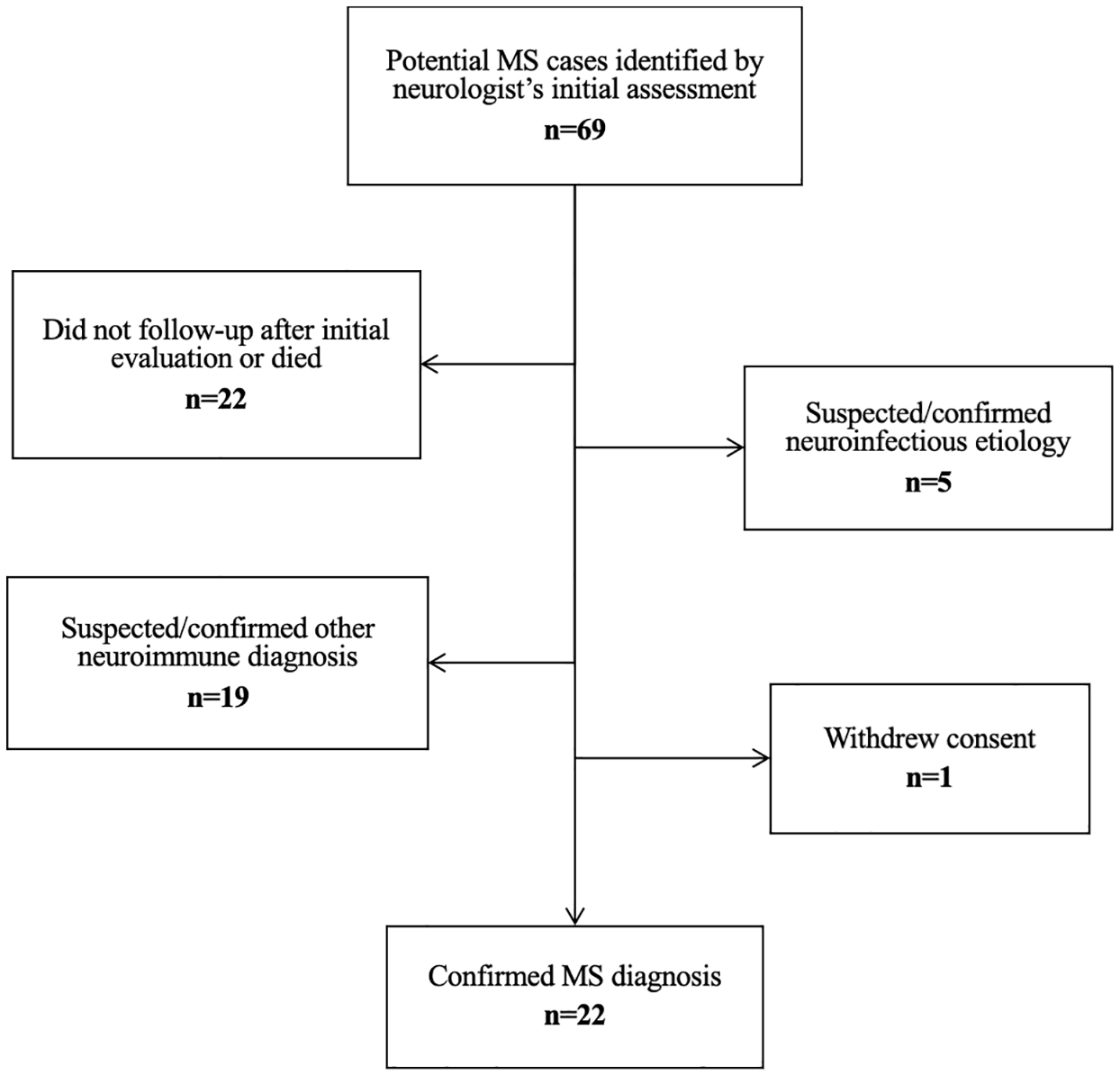
Flowchart of patient case identification and selection based on inclusion criteria.
Data were collected through standardized survey questionnaires developed by an MS specialist and administered by trained nurses and neurologists. Figure 2 summarizes the questionnaires including demographic variables (age, sex, self-reported race, marital status, birth province, highest education), clinical characteristics (date and symptoms of first attack), and diagnostic journey (date of first presentation to healthcare, number and type of prior doctors and facilities, and location of MS diagnosis). All data were de-identified and stored in a secure institutional REDCap database at Johns Hopkins University.17,18
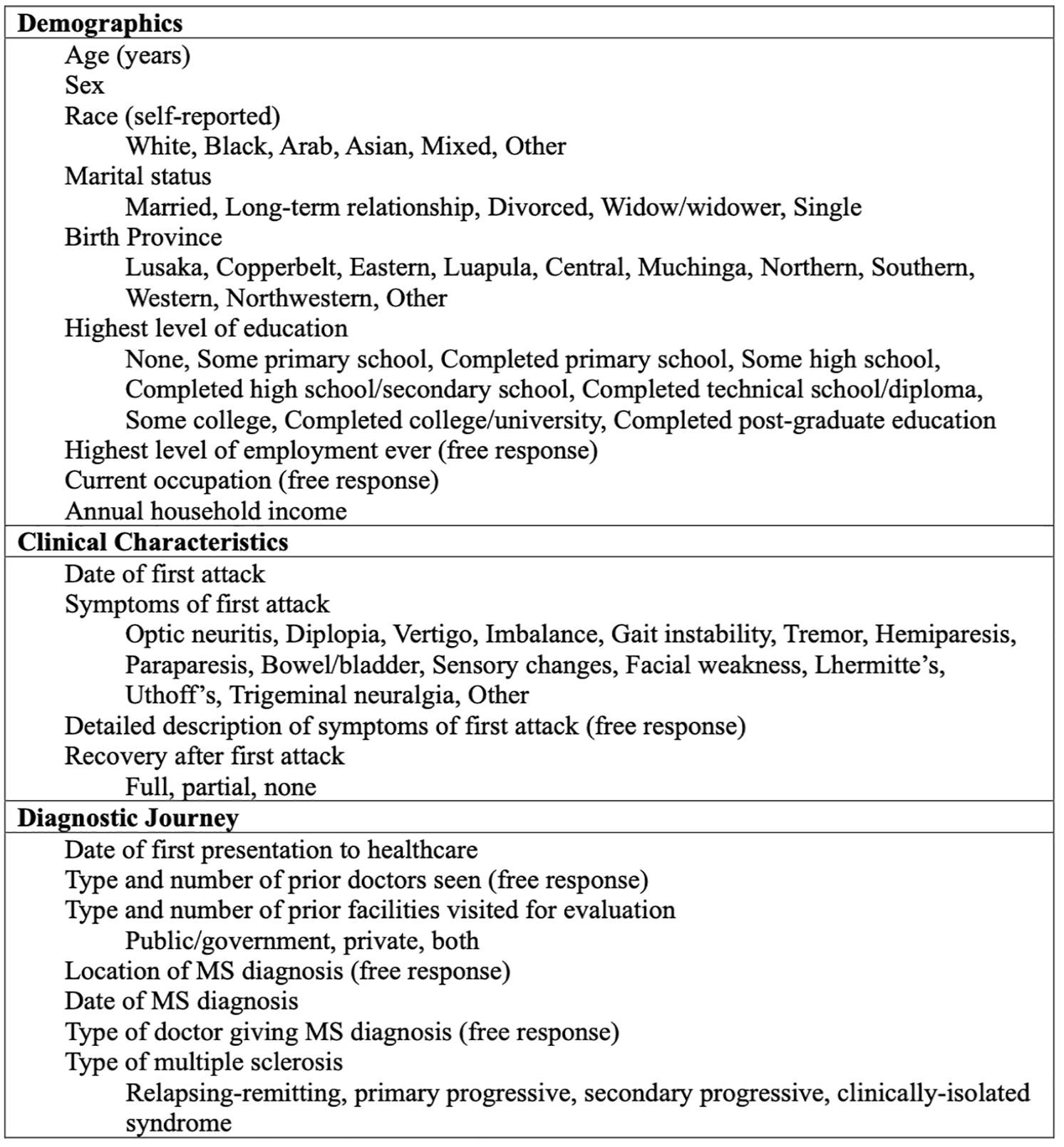
Summary of variables collected by standardized questionnaires (for additional details, please see Supplemental section including full questionnaires).
Demographic and clinical data are reported using descriptive statistics, including mean and standard deviation for normally distributed continuous variables, median and interquartile ranges for non-parametric continuous variables, and proportions for categorical variables.
Both mean and median delays are reported. Mean delay was calculated to allow direct comparison with other published studies of diagnostic delays in MS. However, because the diagnostic delay data did not follow a normal distribution and to mitigate the influence of significant outliers in the data set, median delay was preferentially utilized in analyses of delay sub-types. Delay was categorized into patient delay, health-system delay, and all delay. Patient delay was defined as the time between the date of symptom onset and the date of first presentation to healthcare. Health-system delay was defined as the time between date of first presentation to healthcare and date of diagnosis of MS. All delay, the sum of patient and health-system delay, was defined as the time between the date of symptom onset and the date of diagnosis of MS.
Association of factors with diagnostic delays was first analyzed with Wilcoxon Rank Sum or Kruskal–Wallis tests for non-parametric predictor variables, and Spearman’s correlation coefficients were used for parametric predictor variables.
Due to non-parametric distributions and outlier values, delay times were log transformed before input into regression models. Delays of zero months were replaced with values of 1 day (1/365 = 0.002739726) to avoid missing values. Variable selection for the regression models was based upon the literature of diagnostic delay studies in other MS populations and the assumed relationships of factors influencing the diagnostic pathway in Zambia (Figure 3).19–23 Univariable linear regression models were used to identify variables for inclusion in a multivariable model. A priori, we planned to use a p-value threshold of <0.2 for inclusion of variables into all multivariable models. However, given the large number of variables that met this threshold for all delay and health-system delay models, in the context of a small sample size, we elected to use p < 0.05 for those models. We retained p < 0.2 as the threshold for the patient delay model. The inverse log of the beta coefficients of the linear regression models was calculated and is reported as they correspond to the percent change in delay for each variable. A two-sided p-value of less than 0.05 in the multivariable regression models was considered statistically significant. Fit statistics and variance inflation factors are reported in Supplementary Materials. Data analysis was conducted using Stata 17 SE (College Station, TX, USA).
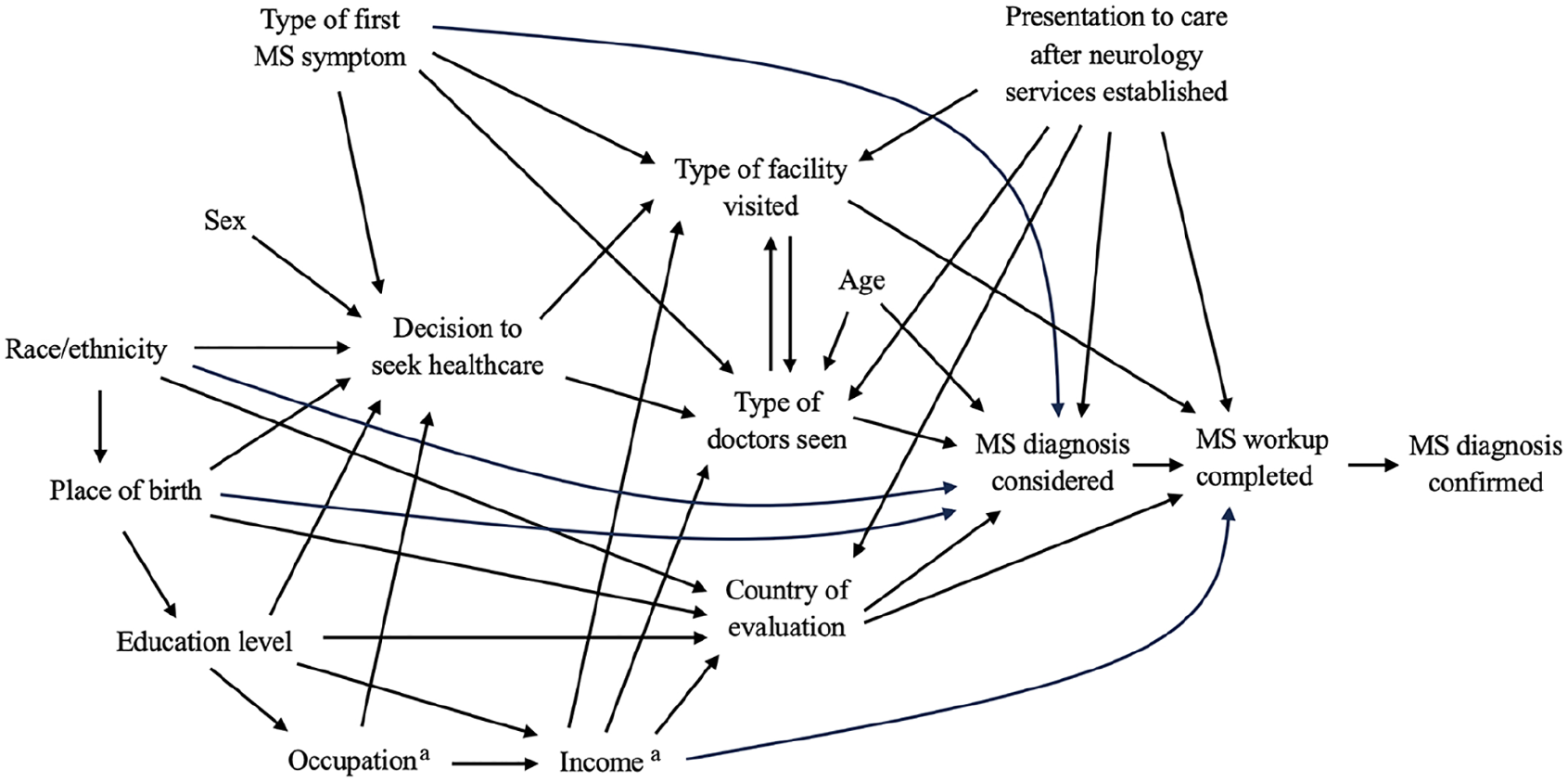
Directed acyclic graph of the relationships between selected variables influencing the MS diagnostic pathway in Zambia.
This study was approved by the ERES Converge Institutional Review Board, the Zambia National Health Research Authority, and the Johns Hopkins University Institutional Review Board.
Results
A total of 22 participants with a diagnosis of MS or CIS were included in this study. All patients underwent MRI of the brain. Most were female (n = 14, 64%), Black African (n = 20, 91%), and had at least a college or university level of education (n = 13, 59%) (Table 1). The mean age of symptom onset was 30.1 years (standard deviation (SD) = 9.5 years), while the mean age of diagnosis was 33.7 years (SD = 10.7 years), leading to a mean diagnostic delay of 3.7 years (SD = 8.6 years). Most participants had a diagnosis of relapsing-remitting MS (n = 19, 86.4%), with the remainder diagnosed with secondary progressive MS (n = 2, 9.1%) and CIS (n = 1, 4.5%).
Demographic and clinical characteristics of cohort (n = 22).
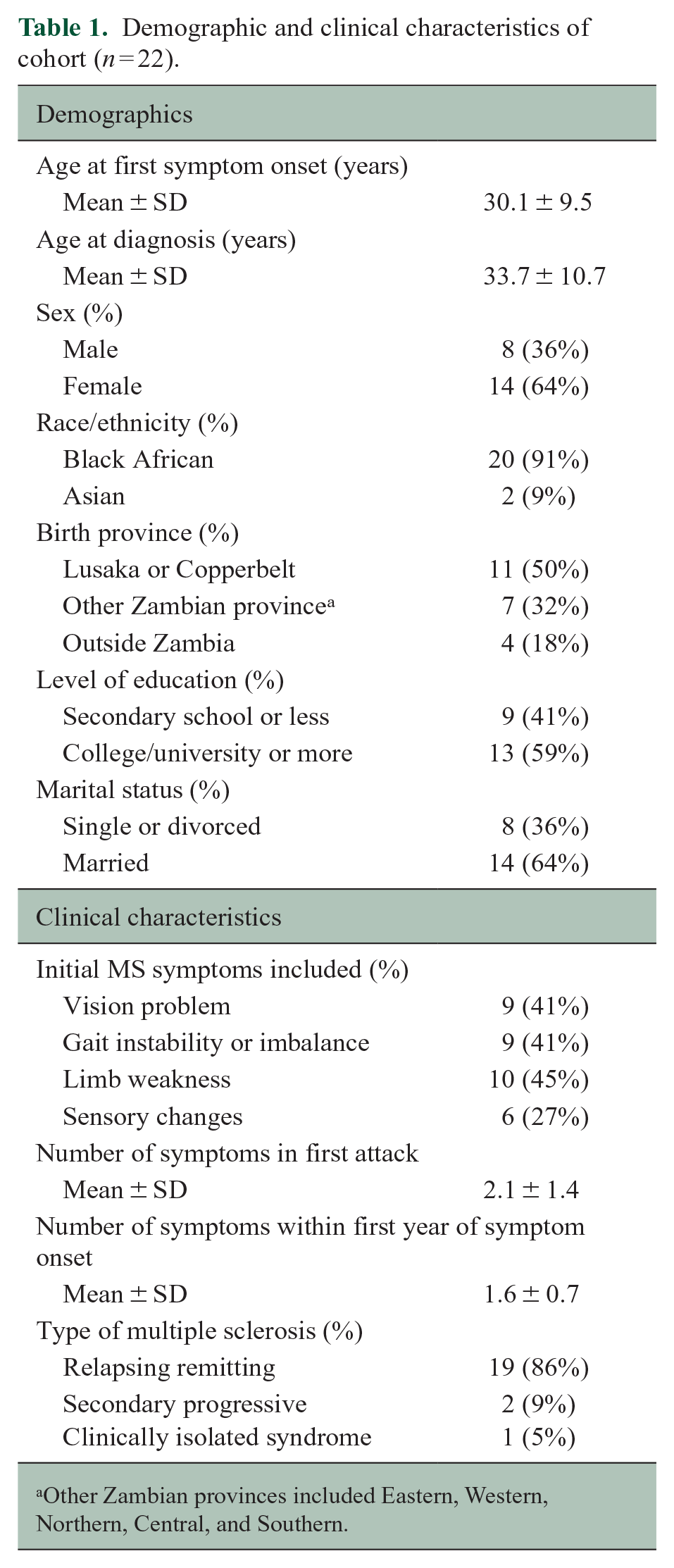
Other Zambian provinces included Eastern, Western, Northern, Central, and Southern.
The overall median all delay from symptom onset to MS diagnosis was 11.4 months (interquartile range (IQR) = 4–35.5). The median patient delay from symptom onset to first presentation to care was less than 1 month (IQR = 0–3). The median health-system delay from first presentation to MS diagnosis was 8.8 months (IQR = 2.6–25.4). Of note, all participants reported seeking evaluation at a healthcare facility for their initial symptoms.
A significant unadjusted association was found between birth province and health-system delay (p = 0.03), with a shorter health-system delay for those who were born outside Zambia (Table 2). The presence of sensory changes during the initial attack was associated with a decrease in all delay (p = 0.01) and health-system delay (p = 0.006). When evaluating the diagnostic journey, visit to a specialist surgeon significantly increased both all delay (p = 0.01) and health-system delay (p = 0.003). Symptom onset before 2019, prior to the establishment of specialty neurology care in Zambia, significantly increased both all delay (p = 0.01) and health-system delay (p = 0.003). Among continuous factors, the age at time of diagnosis was positively and significantly correlated with all delay (p < 0.001) and health-system delay (p < 0.001) (Table 3).
Association of categorical characteristics and diagnostic delay.
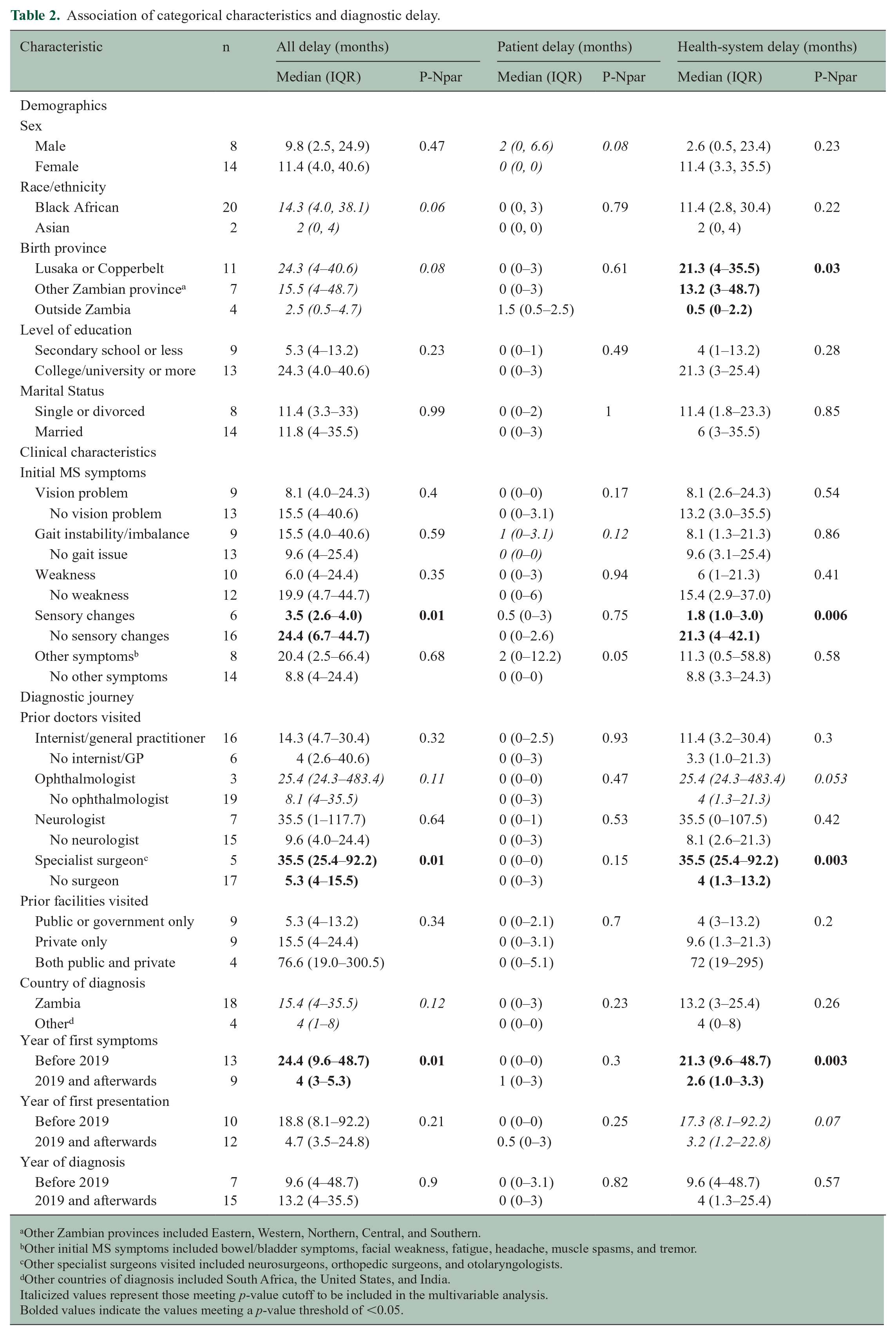
Other Zambian provinces included Eastern, Western, Northern, Central, and Southern.
Other initial MS symptoms included bowel/bladder symptoms, facial weakness, fatigue, headache, muscle spasms, and tremor.
Other specialist surgeons visited included neurosurgeons, orthopedic surgeons, and otolaryngologists.
Other countries of diagnosis included South Africa, the United States, and India.
Italicized values represent those meeting p-value cutoff to be included in the multivariable analysis.
Bolded values indicate the values meeting a p-value threshold of <0.05.
Association of continuous characteristics and diagnostic delay.
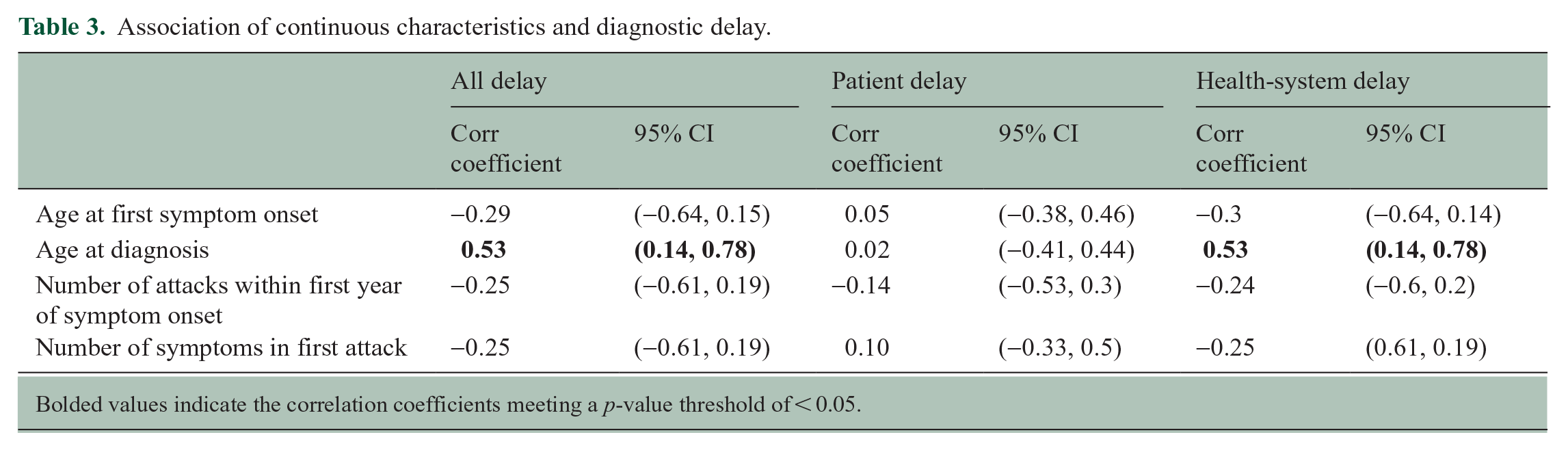
Bolded values indicate the correlation coefficients meeting a p-value threshold of < 0.05.
The results of the final multivariable regression model elicited several factors that were independently associated with a decrease in delay, as outlined in Table 4. Patient race, if Asian, correlated with a decrease in all delay (p = 0.01), when compared to Black African participants. Evaluation outside of Zambia was significantly associated with a decrease in patient delay (p = 0.02), and birthplace outside Zambia correlated with a decrease in health-system delay (p = 0.01). In this model, the number of symptoms during the first attack and Asian race also trended toward a significant association with health-system delay.
Multivariable linear regression analysis of log of diagnostic delay.
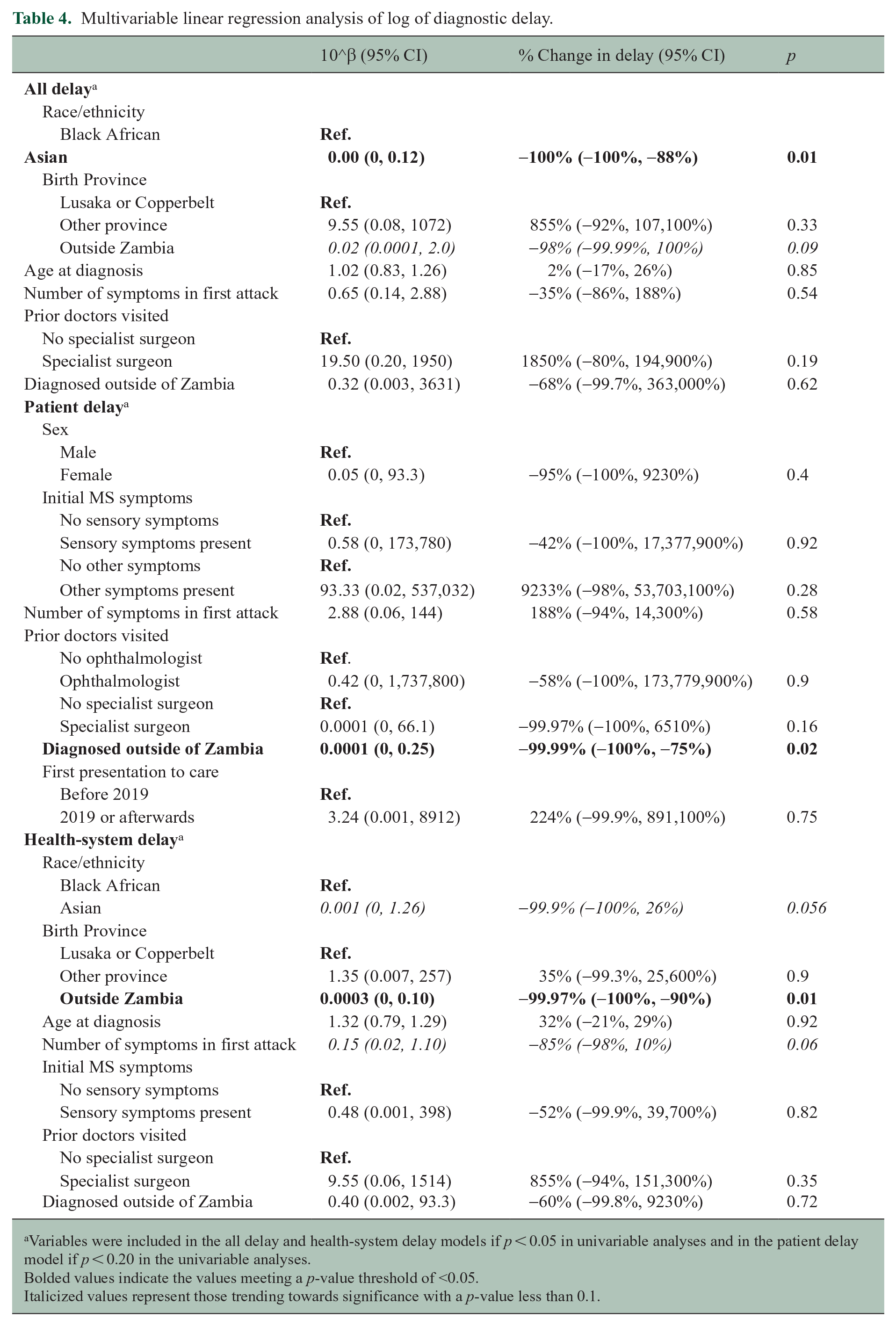
Variables were included in the all delay and health-system delay models if p < 0.05 in univariable analyses and in the patient delay model if p < 0.20 in the univariable analyses.
Bolded values indicate the values meeting a p-value threshold of <0.05.
Italicized values represent those trending towards significance with a p-value less than 0.1.
Discussion
Delay to diagnosis of MS varies widely worldwide. Contemporary cohort studies report a median diagnostic delay of 1.6 years in Italy, 23 and mean diagnostic delay of 0.9 years in Germany, 24 1.1 years in the United States, 25 and 0.6 years in Iran. 22 From other countries, however, even recent cohort studies suggest longer delays. A Columbian study found a mean delay of 3.07 years, 20 and cohort studies from Kenya and Nigeria have found that mean delays to diagnosis were approximately 4 years.7,26 These differences are likely due to a host of factors, including limitations in resources, lack of referral pathways and/or access to specialized neurological care, and limited regional awareness of MS, and highlight the need for further characterization of the factors that influence diagnostic delay in different countries. 27 Prominent neurophobia among African medical students likely contributes to few neurologists and limited regional awareness about neurological conditions. 28
In this study, the mean delay to diagnosis of MS in Zambia was 3.6 years, which is comparable to contemporary cohorts from other countries with reported low MS prevalence.7,20,26 Prominent findings were that race, birthplace, and country of evaluation most significantly impacted diagnostic delay, even after controlling for other factors.
When all delay was examined in a multivariable regression model, only race was significant. However, when this delay was further categorized into patient delay and health-system delay, evaluation outside of Zambia and birthplace outside of Zambia were significantly associated with patient and health-system delay, respectively. Race also trended toward significance in health-system delay. Of note, associations between race and time to diagnosis have not been previously reported in other cohorts.29,30 One explanation is that those of Asian race or born outside Zambia are more likely to seek care outside Zambia in regions with greater MS awareness and, therefore, have a shorter delay to diagnosis. Alternatively, local physicians may be more likely to consider an MS diagnosis and/or referral to neurology when the person is not Black African, resulting in a shorter diagnostic delay. As such, long-held beliefs that MS is rare in SSA may prevent clinicians from even considering an MS diagnosis in a Black African person and further perpetuate under-ascertainment of MS in the region.31,32 Both explanations support the underlying conclusion that Black African people born in Zambia and evaluated in Zambia experience prolonged diagnostic delays when compared to non-black Zambians born and/or evaluated outside Zambia.
Besides race and birthplace, another demographic variable that correlated with delay in unadjusted analyses was age at diagnosis, with older patients experiencing a prolonged health-system delay. This is consistent with findings from other cohort studies in Italy, Germany, and Iran22–24 and may be explained by provider attribution of MS symptoms to an alternate diagnosis that is more common among older patients, especially cerebrovascular disease. However, age at diagnosis did not reach significance in a multivariable model, suggesting that the univariable association is more likely due to the prolonged diagnostic journey of patients who grew older by the time of diagnosis or a survivorship bias.
The lack of significant association of education level with delay in any analysis was notable, especially in a predominantly highly educated cohort, and supports the viewpoint that education among black Zambian people does not necessarily shorten diagnostic delay. This contrasts with findings from studies in Iran and Italy, where lower education levels prolonged delay.22,23 However, education levels of this cohort were much higher than average education levels in the Zambian population. This may have led to an undercoverage bias due to the absence of data from those with lower educational attainment. Furthermore, low levels of MS awareness across the Zambian population may diminish the association between higher education and shorter diagnostic delay, as even those with higher education may not have awareness of MS.
In terms of notable clinical characteristics that were associated with delay in univariable analyses, the presence of sensory symptoms correlated with a shorter all delay and health-system delay, a finding which was not noted in other symptom categories, including vision, gait, or motor symptoms. There are mixed reports from different studies, with certain cohorts, especially in Portugal and Canada, reporting that isolated vision or motor symptoms were associated with prolonged delays, possibly due to these patients being initially referred to a medical or surgical specialist, while sensory symptoms resulted in a shorter referral delay directly to neurology.19,21 In this cohort, being seen by a surgeon was associated with a significantly longer health-system delay in univariable analyses.
In contrast, studies from Iran and Italy reported that motor and vision symptoms at onset were associated with shorter delays, presumably due to the functionally impairing nature of these symptoms resulting in increased care seeking by patients or shorter referral delay to neurology.22,23 In our cohort, due to most patients reporting multiple symptoms at onset of MS and sensory symptoms being a commonly co-occurring symptom, it is possible that the presence of sensory symptoms correlated with those who had more symptoms at onset. Indeed, in the multivariable analysis, it was not the presence of sensory symptoms but rather the number of symptoms during the first attack that trended toward significance in decreasing health-system delay. In addition, this supports the possible conclusion that patients presenting with multiple symptoms, especially sensory, were more likely to be referred to neurology sooner, whereas those presenting with isolated motor or vision symptoms, which may have better established referral pathways to specialists such as ophthalmologists or neurosurgeons/orthopedic surgeons, experienced longer delays. Longer delays in those referred to surgeons were also supported by qualitative work in Zambia and led to a targeted educational course for these specialists.16,33
Within the median all delay of 11.4 months, much of this delay (8.8 months) occurred after first presentation to healthcare and was categorized broadly as health-system delay. This finding points to the role of country-specific healthcare system factors in delaying MS diagnosis, which may include lack of provider knowledge of MS, delays in appropriate referrals to neurology, and limited access to resources to aid with an expedited diagnostic evaluation, including both human resources (e.g. neurologists) and physical resources (e.g. MRI machines). When the diagnostic journey was examined further, visitation to a private versus public healthcare facility did not play a role, suggesting that despite the private healthcare sector’s lower barrier to access diagnostic tests, under-recognition of MS symptoms, lack of neurologists in local private practice, and low rates of neurology referral by private healthcare providers cannot be overlooked. In terms of prior provider subtype, consultation with a specialist surgeon associated with increased health-system delay in the univariable analysis, possibly due to a lack of knowledge of MS among local surgical practitioners or a higher threshold for specialist referrals compared to general practitioners. However, this association was not seen in the multivariable model. Furthermore, there was a reduction in all and health-system diagnostic delay for patients with symptom onset after the establishment of a neurology program in Zambia in 2018, underscoring the importance of access to neurology specialty care in making a timely diagnosis of MS.
There were a few notable limitations to this exploratory study, particularly as a single-center cohort study in a resource-limited setting. As such, we recognize the risk of overfitting the multivariable regression models and not detecting true associations due to the small sample size. However, we believe this unique cohort represents an important and under-investigated population, and these data may be useful in hypothesis generation for future, larger cohort studies, especially regional collaborations with pooled MS cases across sub-Saharan Africa. Still, they should be interpreted with caution considering these limitations. To ensure rigorous and accurate data, participants who were unable to complete diagnostic evaluation due to socioeconomic or geographic factors were excluded, as denoted by 59% of this cohort being college-educated, which is not reflective of Zambia’s overall population. As such, these data are likely not representative of the overall population of people with MS in Zambia, but they call attention to the continued persistence of underdiagnosis in the most socioeconomically vulnerable segments of the population. In addition, of those who were able to seek neurologist evaluation and afford diagnostic testing, potential participants with clinical and radiographic presentations atypical of MS were excluded due to local systemic limitations in obtaining supporting data to definitively rule out alternative diagnoses. Lack of an electronic medical record meant we relied on participant-provided historical data, raising a possibility of recall bias, and these could not be secondarily verified. While household income and occupation were included on questionnaires, participant refusal to disclose financial information was high, so these data were excluded, and education level was instead used as a proxy for these variables. In addition, the delay imposed by waiting for diagnostic tests such as MRI was not measured due to lack of validated dates, and this may have falsely inflated the health-system delay. Because this study was only conducted in Zambia among participants with MS, the results are highly contextualized and not generalizable to other populations. Regardless of these limitations, the strengths of this study include its conduct in an understudied and underrepresented region and population that, despite local resource limitations, still had access to fully trained neurologists who conducted the clinical evaluations and confirmed diagnoses.
This study elucidated several factors associated with delays to diagnosis of MS in Zambia. While a nationwide educational lecture series targeted for local providers was recently launched to advance knowledge of MS in Zambia, a more comprehensive study to understand gaps in provider knowledge, appraisal of MS symptoms, and referral patterns is needed. Furthermore, patient-specific factors, including perceptions and health literacy of MS symptoms, care-seeking thresholds, and selection of specialist and facility type, need to be more fully understood, especially among black Zambian people of varied socioeconomic backgrounds; while these factors have been qualitatively studied to understand delays in presentation for meningitis in Zambia, this remains unknown for neurologic symptoms of MS. 34 In addition, given the costs associated with delayed diagnosis, the role of economic factors remains largely understudied in this population. Further studies are imperative to improve health equity for other similar populations in SSA, as shortening diagnostic delays should lead to earlier access to treatment and less accrual of disability.
Supplemental Material
sj-docx-1-msj-10.1177_13524585251344832 – Supplemental material for Factors associated with delay to diagnosis of multiple sclerosis in Zambia
Supplemental material, sj-docx-1-msj-10.1177_13524585251344832 for Factors associated with delay to diagnosis of multiple sclerosis in Zambia by Malya Sahu, Mashina Chomba, Dominique Mortel, Sarah Braun, Lorraine Chishimba, Frighton Mutete, Naluca Mwendaweli, Coolwe Namangala, Stanley Zimba and Deanna Saylor in Multiple Sclerosis Journal
Supplemental Material
sj-pdf-2-msj-10.1177_13524585251344832 – Supplemental material for Factors associated with delay to diagnosis of multiple sclerosis in Zambia
Supplemental material, sj-pdf-2-msj-10.1177_13524585251344832 for Factors associated with delay to diagnosis of multiple sclerosis in Zambia by Malya Sahu, Mashina Chomba, Dominique Mortel, Sarah Braun, Lorraine Chishimba, Frighton Mutete, Naluca Mwendaweli, Coolwe Namangala, Stanley Zimba and Deanna Saylor in Multiple Sclerosis Journal
Footnotes
Data availability statement
Anonymized data not published within this article will be made available by request from any qualified investigator that follows Zambian regulations regarding data sharing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding from a National Multiple Sclerosis Society Pilot Grant (PP-1807-32127), NIH Fogarty International Center (K01TW011771, D43TW009340), Multiple Sclerosis International Federation Du Pre Award, and American Academy of Neurology/American Brain Foundation Neurodisparities Clinical Research Training Scholarship.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.