
Abstract
Background:
Longitudinal studies of health-related quality of life (HRQoL) in multiple sclerosis (MS) are limited. Most have examined average changes within the population, rather than dynamic changes within individuals.
Objective:
To assess the between- and within-individual association between depression, anxiety, fatigue, cognition, physical functioning, and physical comorbidities and HRQoL.
Methods:
Adults with MS underwent physical and cognitive assessments and reported symptoms of fatigue (Daily Fatigue Impact Scale), depression and anxiety (Hospital Anxiety and Depression Scale (HADS)), and HRQoL (RAND-36) annually (n = 4 visits). We evaluated associations of elevated symptoms of anxiety (HADS-A) and depression (HADS-D), fatigue, physical function (timed-walk and nine-hole peg test), cognitive function and comorbidity count with physical (PCS-36) and mental (MCS-36) HRQoL using multivariable linear models—estimating between-person and within-person effects.
Results:
Of 255 participants with MS enrolled, 81.6% were women. After adjustment, within-person increases in depression and fatigue were associated with decreases in physical HRQoL. Increases in depression, anxiety, and comorbidity count were associated with decreases in mental HRQoL.
Conclusions:
Within-person increases in symptoms of depression, anxiety and fatigue, and comorbidity count are associated with HRQoL decreases among adults with MS, highlighting the potential magnitude of individual benefit of intervention for these symptoms.
Introduction
Health-related quality of life (HRQoL) is a multidimensional concept encompassing physical, social, and emotional aspects of well-being and functioning, 1 which represents an important patient-centered outcome. 2 HRQoL is lower in individuals with multiple sclerosis (MS) than individuals from the general population and those with other chronic diseases. Physical impairments, relapse activity, physical comorbidities, and elevated symptoms of depression and anxiety have all been reported to be associated with worse HRQoL in individuals with MS.3-6 Relatively few studies have concurrently considered all of these factors, and most have been cross-sectional. Indeed, a recent systematic review of 106 studies emphasized that nearly 75% were cross-sectional. 5
More longitudinal studies of HRQoL in MS are needed to fully understand the relationships among the factors that influence it. Most longitudinal observational studies examining HRQoL in MS have used population-averaged approaches such as regression using generalized estimating equations that have reported on average changes in the population, thereby mixing the effects of between-person and within-person changes over time. HRQoL is dynamic and understanding determinants of within-person changes are particularly important when considering potential benefits of interventions for an individual. Within-person analyses also carry the advantage of controlling for unmeasured fixed characteristics of an individual, which may confound between-person comparisons.
We assessed the association between symptoms of depression, anxiety, fatigue, cognition, physical functioning, physical comorbidities, and HRQoL, as measured by the RAND-36, in an MS cohort over 3 years. We hypothesized that within-person fluctuations in symptoms of depression, anxiety, fatigue, cognition, and physical comorbidities would be associated with changes in HRQoL.
Methods
Study population
We examined a cohort of participants with MS enrolled in a prospective study conducted between November 2014 and July 2016 to study psychiatric comorbidity in immune-mediated inflammatory disease cohorts residing in Manitoba, Canada. 7 Participants with MS aged ⩾ 18 years were recruited from the provincial MS Clinic registry (see online Appendix). 7 All participants provided informed consent. The University of Manitoba Health Research Ethics Board approved the study.
Participants completed questionnaires, and underwent physical and cognitive assessments annually for 3 years following enrollment. 7
Health-related quality of life
We used the RAND-36, a general measure of HRQoL, which is valid and reliable in the general population (see online Appendix). 8 The RAND-36 generates aggregate scores summarizing physical HRQoL (Physical Component Score, PCS-36) and mental HRQoL (Mental Component Score, MCS-36), with factor analyses supporting a two-factor model of HRQoL. 8 Aggregate scores range from 0 to 100, with a mean of 50 and standard deviation of 10; higher scores represent better HRQoL. We chose a general measure of HRQoL to allow comparisons within our larger multi-disease cohort study. 9 The Short Form-36 (SF-36) was the most commonly used general measure in a recent systematic review of HRQoL in MS, 5 and in clinical trials of MS disease-modifying therapies (DMT). 10 While the SF-36 uses principal component analysis with orthogonal factor rotations to generate its aggregate scores, the RAND-36 uses item response theory-based scaling and oblique factor rotations to obtain aggregate scores from these same questions. 8 We employed the RAND-36 scoring as it assesses mental health better than scoring used for the SF-36 in persons with MS. 11
Symptoms and comorbidity
We evaluated symptoms of depression and anxiety using the Hospital Anxiety and Depression Scale (HADS), which includes seven items each for depression (HADS-D) and anxiety (HADS-A). Total scores on each scale range from 0 to 21. We dichotomized the HADS scores using the cut-point ⩾ 11 to indicate clinically meaningful elevations in symptoms; 12 sensitivity analyses included these scores as continuous variables (1-point change). We evaluated fatigue using the eight-item Fatigue Impact Scale for Daily Use (D-FIS), 13 which has good psychometric properties in MS. 14 Scores range from 0 to 32 and higher scores indicate more fatigue.
Participants reported physician-diagnosed comorbidities using a validated questionnaire, 15 including high cholesterol, hypertension, heart trouble, disease of arteries in the legs, lung trouble, diabetes mellitus, cancer of the breast, cancer of the colon or rectum, cancer of the lung, skin cancer, other cancers, migraine, thyroid disease, lupus, osteoarthritis, osteoporosis, fibromyalgia, kidney disease, peptic ulcer disease, liver problems, irritable bowel syndrome, and epilepsy. As individuals with MS who have more comorbidities report lower HRQOL, we categorized these as 0, 1, 2, and ⩾ 3. 16
Physical and cognitive function
We assessed lower limb function using the timed 25-foot walk test, and upper limb function using the nine-hole peg test.17,18 Both are valid, reliable measures. 19 We generated z-scores for lower and upper limb function using the baseline values of these measures for the cohort, then averaged them, similar to the approach for the Multiple Sclerosis Functional Composite (MSFC). We assessed cognition using the oral version of the Symbol Digit Modalities Test (SDMT), 20 and used alternate SDMT forms at the second and fourth visits to limit practice effects. We used raw scores for the SDMT as we included age, gender, and education in our regression models. We used the Expanded Disability Status Scale (EDSS) solely to describe the sample as a prior longitudinal study showed that changes in the MSFC were associated with changes in HRQoL, but changes in the EDSS were not. 21
Covariates
Fixed covariates included self-reported gender, ethnicity, education, and age at symptom onset. As detailed elsewhere, 7 ethnicity was reported using the categories used by Statistics Canada in national surveys. Because very few participants did not self-identify as White, ethnicity was collapsed as White and Other in our analyses. Highest level of education attained was summarized as less than high school, high school, and some post-secondary education.
Time-varying covariates included age, income, marital status, smoking status, body mass index (BMI), physical comorbidity count, physical function, cognitive function, disease activity and use of DMT. Participants reported date of birth from which we derived age, based on visit date. Annual household income was categorized as < US$50,000, ⩾ US$50,000, or “I do not wish to answer.” Marital status was classified as single (single/never married, divorced, widowed, separated) or partnered (married, common-law). We classified participants as current, past, and never smokers; smokers had smoked ⩾ 100 cigarettes in their lifetime. We determined BMI (kg/m2) from measured height and weight, and categorized it as normal (18 to 25), overweight (> 25 to < 30) or obese (⩾ 30). We defined disease activity as present/absent in the last year based on the presence of relapses identified on chart review. DMT use was classified as yes/no.
Analysis
We included participants who had completed ⩾ 1 visit; missing data were not imputed as only 5% were missing. We summarized participant characteristics using mean [SD], median (interquartile range (IQR)), and frequency (percent). Since a 3-point change is considered clinically meaningful for the PCS-36 and MCS-36, 22 we also report the proportion with ⩾ 3-point increase or decrease in score between visits for each. Generally, changes of 3–4 points represent small effects, 4–10 points moderate effects, and > 10 points large effects. 23
The co-primary outcomes of interest were PCS-36 and MCS-36 (HRQOL); each was evaluated separately. To determine the effect of the independent variables of interest on HRQOL, we used generalized linear models with an identity link, and generalized estimating equations with an exchangeable working correlation to account for dependence of observations within individuals. The outputs of these models are population averages of within-person and between-person effects. We were particularly interested in within-person effects, so parameterized the model to disaggregate these effects by using person-specific mean centering to generate separate variables (see online Appendix). 24 The primary independent variables of interest were the within-person and between-person variables for the HADS-D and HADS-A. Secondary variables of interest were the within-person and between-person variables for physical function, cognitive function, and physical comorbidity count; Daily Fatigue Impact Scale (DFIS) was a predictor for the PCS-36 models but not the MCS-36 models because the MCS-36 captures fatigue/vitality. We tested for two-way interactions between the within-person and between-person changes in depression and anxiety symptoms. Unadjusted models included only the primary variables of interest. Adjusted models included primary and secondary variables of interest and covariates including age (continuous), gender (woman as reference), education (< high school as reference), income (< US$50,000 as reference), race (White as reference), marital status (single as reference), BMI (normal as reference), physical function (z-score, continuous), smoking status (never as reference), age at MS onset (continuous), and DMT use (none as reference). Model fit was assessed using the quasi-likelihood information criterion (QIC). We report regression coefficients and 95% confidence intervals (95% CI) for the variables of interest.
Statistical analyses were conducted using SAS V9.4 (SAS Institute Inc., Cary, NC).
Results
Participants
We enrolled 255 participants with MS, of whom 8 died before study completion, 10 were lost to follow-up, and 2 withdrew. 25 As compared to participants in the MS cohort who completed all visits, those who did not were less likely to have a post-secondary education, reported more pain and fatigue at baseline, and were less likely to be using a DMT (see Table e1). Most participants were women and self-identified as White (see Table 1). Two-thirds had completed high school or some post-secondary education. The median EDSS score was 4 (3–6), and half of participants were using DMT.
Participant characteristics at enrollment.
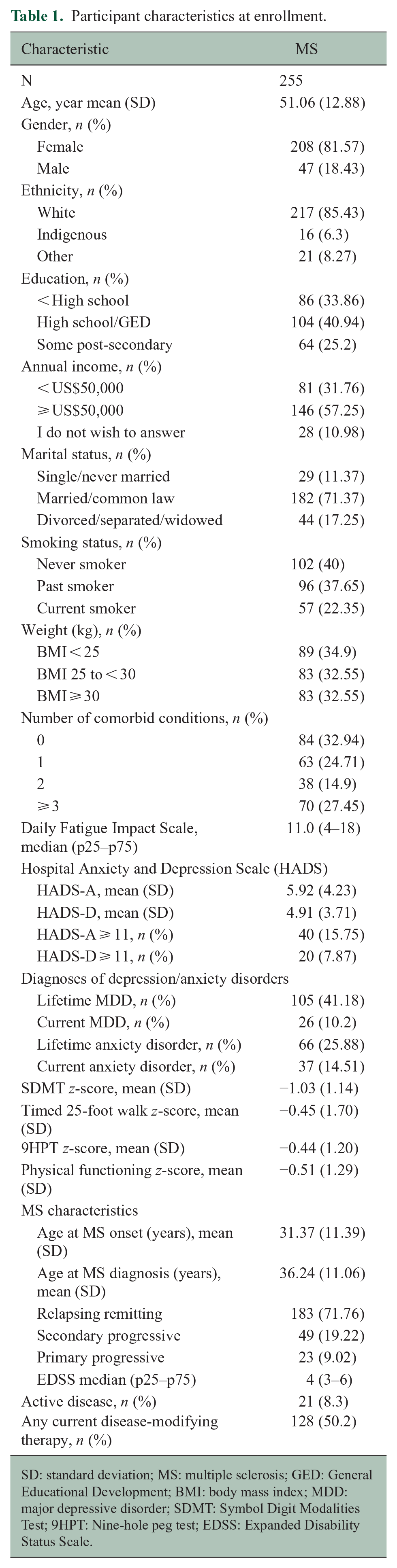
SD: standard deviation; MS: multiple sclerosis; GED: General Educational Development; BMI: body mass index; MDD: major depressive disorder; SDMT: Symbol Digit Modalities Test; 9HPT: Nine-hole peg test; EDSS: Expanded Disability Status Scale.
Health-related quality of life
Average (SD) PCS-36 scores varied little across visits, ranging from 33.8 (9.5) to 34.2 (9.4; see Table 2). However, when we examined the percentage of participants with ⩾ 3-point change in their PCS-36 score from one visit to another, 22–23% reported improvement, and 19–28% reported worsening, depending on the visit. Combined over all visits, 86.3% of participants had a meaningful change over the study period (see Figure 1).
Participant characteristics by study visit.
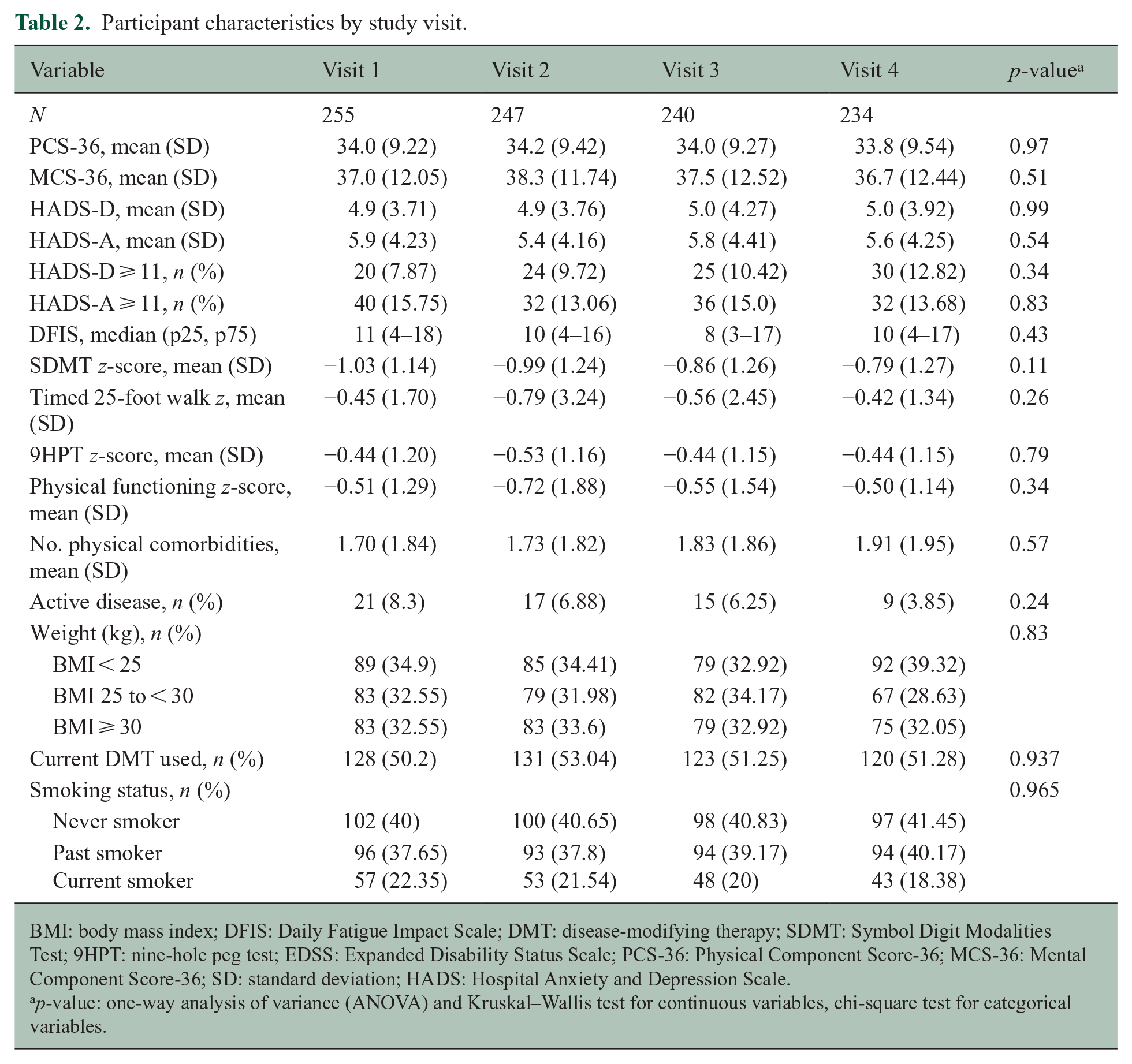
BMI: body mass index; DFIS: Daily Fatigue Impact Scale; DMT: disease-modifying therapy; SDMT: Symbol Digit Modalities Test; 9HPT: nine-hole peg test; EDSS: Expanded Disability Status Scale; PCS-36: Physical Component Score-36; MCS-36: Mental Component Score-36; SD: standard deviation; HADS: Hospital Anxiety and Depression Scale.
p-value: one-way analysis of variance (ANOVA) and Kruskal–Wallis test for continuous variables, chi-square test for categorical variables.
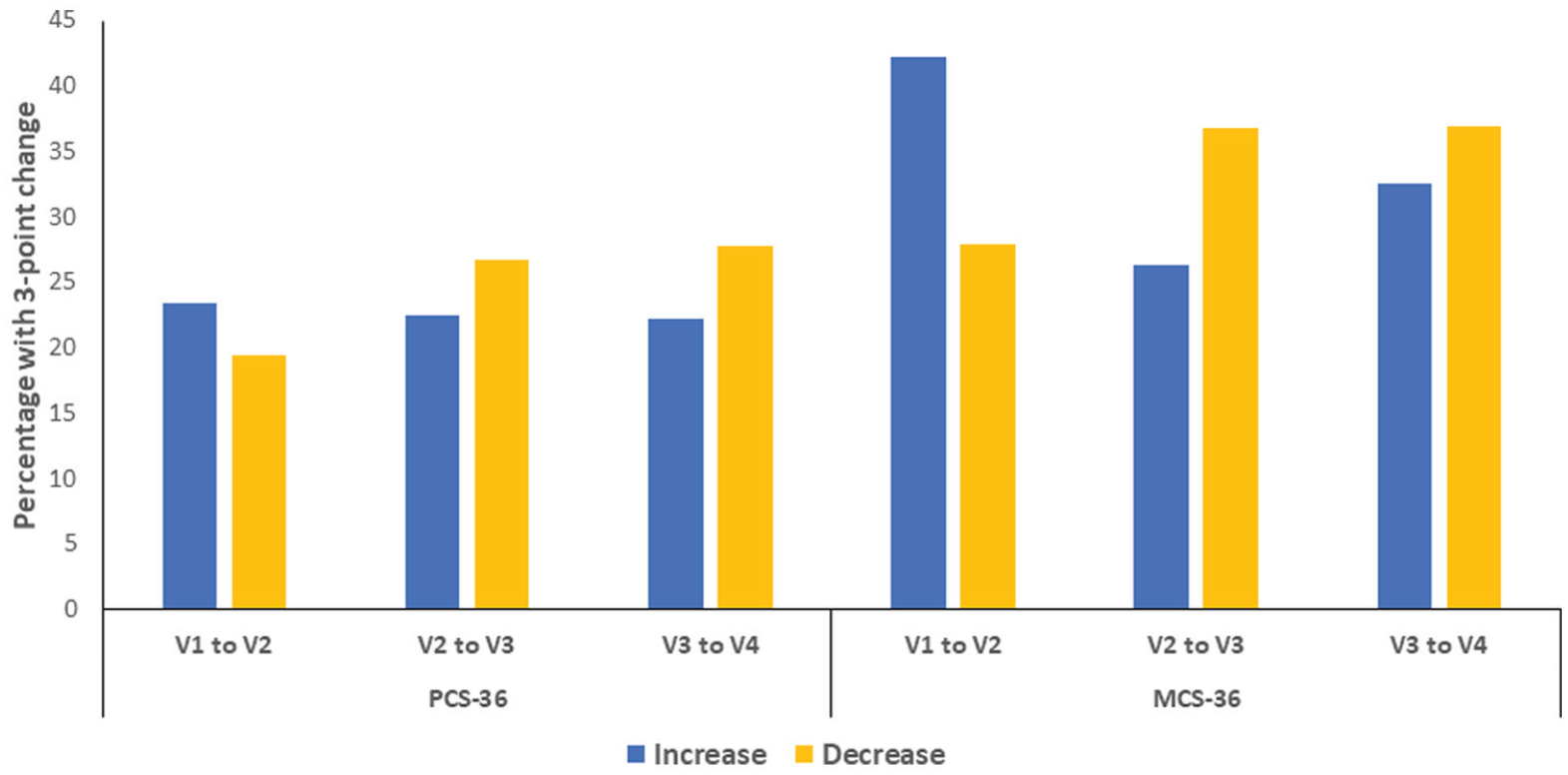
Percentage of participants with 3-point changesa in the Physical Component Score-36 (PCS-36) or Mental Component Score-36 (MCS-36) from one visit to another in participants from the multiple sclerosis (MS) and depression/anxiety (DEP/ANX) cohorts.
Average (SD) MCS-36 scores also varied relatively little, although more than the PCS-36 scores (see Table 2). When we examined 3-point changes in MCS-36 scores, > 90% of the cohort had a meaningful change over the course of the study (see Figure 1). Severity of fatigue (DFIS), depression and anxiety symptoms (HADS) also varied little on average (see Table 2, Figure e1).
At enrollment, the PCS-36 and MCS-36 correlated moderately (r = 0.57; 95% CI: 0.48–0.65). Findings were similar over time (online Appendix).
Regression analyses
In regression models including only variables for symptoms of depression (HADS-D) and anxiety (HADS-A), participants with HADS-D and HADS-A scores ⩾ 11 had lower PCS-36 scores on average than participants who had scores < 11 at any given visit (see Table 3). Participants who experienced increases in HADS-D or HADS-A scores over time reported large decreases in their PCS-36 scores. In the fully-adjusted model, on average, participants with meaningfully worse DFIS and physical function scores had lower PCS-36 scores; these effects were large. Participants who experienced increases in HADS-D or DFIS scores over time reported decreases in their PCS-36 scores. We did not observe interactions between within-person and between-person effects for the HADS-D or HADS-A.
Regression coefficient estimates (95% confidence intervals (CIs) for variables associated with health-related quality of life over time.
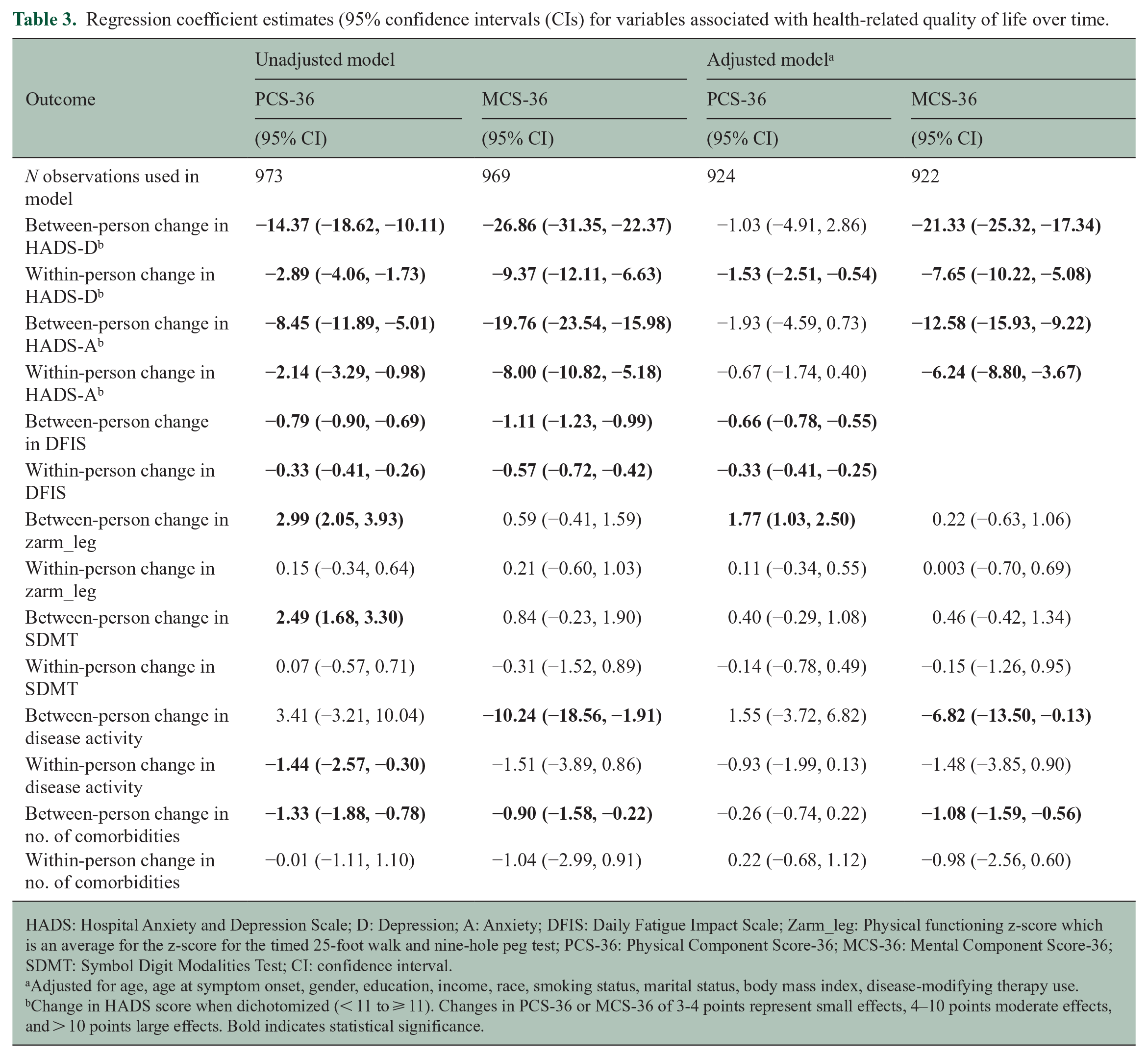
HADS: Hospital Anxiety and Depression Scale; D: Depression; A: Anxiety; DFIS: Daily Fatigue Impact Scale; Zarm_leg: Physical functioning z-score which is an average for the z-score for the timed 25-foot walk and nine-hole peg test; PCS-36: Physical Component Score-36; MCS-36: Mental Component Score-36; SDMT: Symbol Digit Modalities Test; CI: confidence interval.
Adjusted for age, age at symptom onset, gender, education, income, race, smoking status, marital status, body mass index, disease-modifying therapy use.
Change in HADS score when dichotomized (< 11 to ⩾ 11). Changes in PCS-36 or MCS-36 of 3-4 points represent small effects, 4–10 points moderate effects, and > 10 points large effects. Bold indicates statistical significance.
Findings were slightly different for the MCS-36 (Table 3). In regression models including only variables for HADS-D and HADS-A, participants with HADS-D scores ⩾ 11 or HADS-A scores ⩾ 11 had lower MCS-36 scores than participants whose scores were < 11 (Table 3). Participants who experienced increases in HADS-D or HADS-A scores over time reported decreases in their MCS-36 scores. In the fully adjusted model, on average, participants with higher HADS-D and HADS-A scores and more comorbidities reported lower MCS-36 scores; these effects were large. Disease activity was associated with lower MCS-36 scores. Participants who experienced increases in HADS-D or HADS-A scores over time reported large decreases in their MCS-36 scores; the largest effect was for changes in HADS-D.
Findings were similar when the HADS was included as a continuous variable although smaller in magnitude given, they reflected a 1-point change rather than elevated versus non-elevated symptoms (see Table 4).
Regression coefficient estimates (95% confidence intervals (CIs) for variables associated with health-related quality of life over time when Hospital Anxiety and Depression Scale scores were continuous.
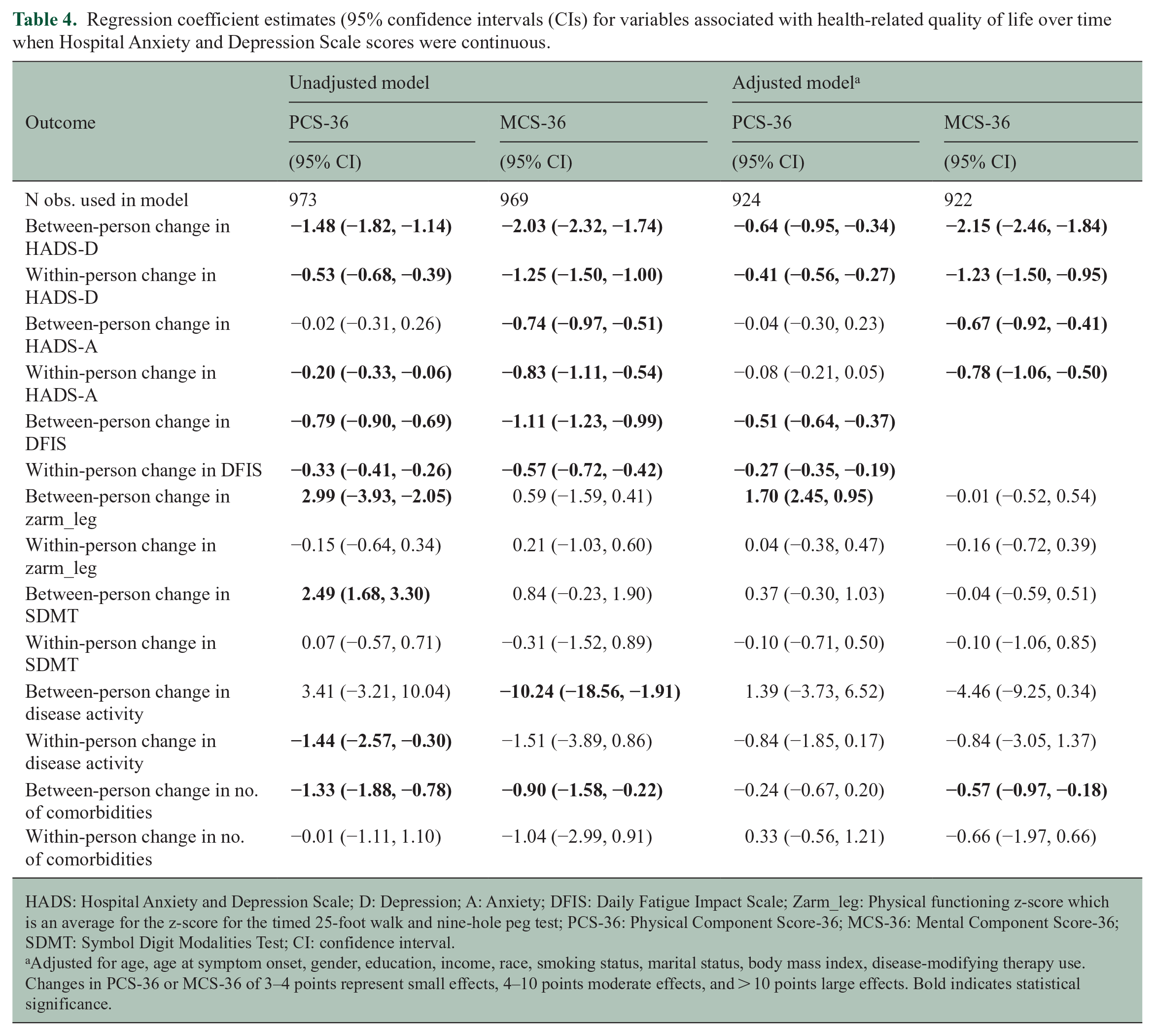
HADS: Hospital Anxiety and Depression Scale; D: Depression; A: Anxiety; DFIS: Daily Fatigue Impact Scale; Zarm_leg: Physical functioning z-score which is an average for the z-score for the timed 25-foot walk and nine-hole peg test; PCS-36: Physical Component Score-36; MCS-36: Mental Component Score-36; SDMT: Symbol Digit Modalities Test; CI: confidence interval.
Adjusted for age, age at symptom onset, gender, education, income, race, smoking status, marital status, body mass index, disease-modifying therapy use. Changes in PCS-36 or MCS-36 of 3–4 points represent small effects, 4–10 points moderate effects, and > 10 points large effects. Bold indicates statistical significance.
Discussion
In this 3-year longitudinal study, the physical and mental HRQOL of participants with MS were below population norms (i.e. < 50). After accounting for age, age at symptom onset, gender, race, education, income, marital status, smoking status, body mass index and DMT use, participants with higher symptoms of depression and fatigue, and worse physical function reported lower physical HRQoL on average. Similarly, meaningfully elevated symptoms of depression and anxiety, and disease activity were associated with large effects on mental HRQoL of ⩾ 6 points, and more comorbidities were associated with a small effect of 1 point; symptoms of depression had the largest effect (21 points). Within-person fluctuations in symptoms of depression and fatigue were associated with small changes in physical HRQoL of ⩽ 1 point, whereas within-person fluctuations in symptoms of depression and anxiety were associated with large fluctuations in mental HRQOL exceeding 6 points. By comparison, changes in the timed 25-foot walk and nine-hole peg test of ⩾ 20% are considered clinically meaningful, 19 being associated with changes in walking ability in daily activities, and employment status; 26 worsening in the timed 25-foot walk is associated with a decrease of −2.18 in the PCS-36, whereas ⩾ 20% worsening in the nine-hole peg test is associated with a decrease of −2.86, 3 months confirmed disability worsening on the EDSS is associated with a decrease of −2.75, and a 4-point reduction in the Symbol Digit Modalities Test is associated with a decrease of −1.15. 27 The large effects of depression and anxiety on HRQoL emphasize the clinical importance of effective evaluation and treatment of these comorbidities.
On average, our MS cohort exhibited little change in physical or mental HRQoL over time, but similar to other studies,21,28 most individuals within our cohort exhibited meaningful changes in HRQoL between annual study visits at some point during the study, reflecting the importance of considering intra-individual differences. For example, a 5-year study of the 3779 participants in the NARCOMS registry using the Short Form-12 reported an average change in physical QoL of 1 point, and in mental QoL of 0.03, whereas 40% of the cohort reported ⩾ 3-point changes in their HRQoL. 28 Recent longitudinal studies in MS have adjusted for baseline HRQoL when testing the association between baseline symptoms and HRQOL at follow-up. 5 This approach provides information about factors that affect HRQoL in the study population on average, but does inform on the effects of changes in a symptom or other factors on the individual. We cannot assume that if a person who is depressed at one point in time reports lower HRQOL than someone who is not depressed; she or he will necessarily report better HRQoL if the depression subsequently resolves. A recent study used group-based trajectory models to address heterogeneity in the evolution of HRQoL; 29 while this approach identified several distinct subgroups for physical and mental HRQoL, inference at the individual level remained lacking. In contrast, we separately assessed the population-level (average) effects from the within-person effects of changes in symptoms, such as depression and anxiety, which often fluctuate over time.
A 2020 systematic review examining risk factors and interventions for HRQoL in MS identified higher disability, longer disease duration, relapses (disease activity), fatigue, cognitive impairment, depression, and anxiety as key factors associated with lower HRQoL. 5 Direct comparisons with our study are challenging because the predictors considered differed. On multivariable analysis, we did not detect an effect of relapses but relapse activity was very low. Similarly, we did not observe an association with a change in cognitive function. We examined the effect of a one standard deviation change/difference in the SDMT, which reflected a 2.5-point change in raw score. Another study found that a 4-point change in SDMT was associated with a very small effect on PCS-36 (1.15 points), 27 so the magnitude of the effect here was likely to be very small and require larger sample sizes to detect. Shared causal pathways between depression, anxiety and physical comorbidity may have also limited the ability to detect an association. Among eight longitudinal studies in a prior systematic review, 5 one study followed 43 participants for 3 years and used a mixed-effects model, thus testing the within-person (subject-effects) effects of changes in the independent variables. 21 Those findings were consistent with our observations in that worsened depressive symptoms and worsened physical function were associated with lower PCS-36 scores; the effect of anxiety was not assessed. Unlike our study, this study found that improvements in cognitive performance, as assessed using a composite based on five tests, were associated with improved MCS-36 scores but adjusted only for age, sex, physical function, and fatigue.
While prior studies have consistently found depression to be associated with HRQoL, fewer studies have assessed the role of anxiety, which is similarly more common in persons with MS. Some cross-sectional studies have found that elevated anxiety symptoms are associated with lower mental HRQoL,3,30 although in one longitudinal study, elevated symptoms of anxiety measured by the HADS, were not associated with lower HRQoL at baseline or at follow-up after adjusting for depression. 31 The absence of an association between symptoms of anxiety and physical HRQoL in our study and the earlier longitudinal study may reflect exclusion of somatic symptoms of anxiety from the HADS. Our findings indicate the importance of considering both anxiety and depression as relevant contributors to HRQoL for individuals with MS as their contributions differ.
We acknowledge several study limitations. Although the RAND-36 is a validated measure, it may be less responsive to change in the MS population than disease-specific measures. Nonetheless, use of the RAND-36 supports comparisons of HRQoL to other populations, and to the literature in MS using the SF-36 32 and MS-specific measures that incorporate the SF-36;33,34 it discriminates between people with MS with differing severities of disability, 35 with and without depression, and with differing numbers of comorbidities. 35 While we captured symptoms of depression and anxiety, we did not assess other psychological variables such as resilience and self-efficacy due to the participant burden of long study visits. However, within-person analyses effectively controlled for unmeasured, time-invariant characteristics. We measured only some social determinants of health. Our study population predominantly included White women, although we attempted to improve sample diversity by using multiple methods of recruitment including working with primary care practices; covering transportation costs; providing gift cards; and conducting visits before and after usual working hours. Our study has several strengths including the high retention, longitudinal design, comprehensive set of covariates considered, and analytic approach.
Among people with MS, HRQoL falls below general population norms. Within-person fluctuations in symptoms of depression, anxiety and fatigue, as well as number of physical comorbidities are associated with changes in physical and mental HRQoL. Our findings highlight the potential magnitude of individual benefit of interventions for these symptoms, and warrant further investigation.
Supplemental Material
sj-docx-1-msj-10.1177_13524585231190771 – Supplemental material for Within-person fluctuations over three years in depression, anxiety, fatigue, and health-related quality of life in multiple sclerosis
Supplemental material, sj-docx-1-msj-10.1177_13524585231190771 for Within-person fluctuations over three years in depression, anxiety, fatigue, and health-related quality of life in multiple sclerosis by Ruth Ann Marrie, Charles N Bernstein, Casandra Dolovich, James M Bolton, Lesley A Graff, Carol A Hitchon, Lisa M Lix, James J Marriott and John D Fisk in Multiple Sclerosis Journal
Footnotes
Data availability
The data sets presented in this article are not readily available because some participants did not agree to data sharing. Components of the data sets may be made accessible to qualified investigators with the appropriate ethical approvals and data use agreements upon request. Requests to access the data sets should be directed to RAM,
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ruth Ann Marrie receives research funding from CIHR, Research Manitoba, MS Canada, Multiple Sclerosis Scientific Foundation, Crohn’s and Colitis Canada, National Multiple Sclerosis Society, CMSC, the Arthritis Society and the US Department of Defense, and is a co-investigator on studies receiving funding from Biogen Idec and Roche Canada. She holds the Waugh Family Chair in Multiple Sclerosis. Dr Bernstein is supported by the Bingham Chair in Gastroenterology. Dr Bernstein has served on advisory Boards for AbbVie Canada, Amgen Canada, Bristol Myers Squibb Canada, JAMP Pharmaceuticals, Lilly Canada, Roche Canada, Janssen Canada, Sandoz Canada, Takeda Canada, and Pfizer Canada; Consultant for Mylan Pharmaceuticals and Takeda; Educational grants from Abbvie Canada, Bristol Myers Squibb Canada, Ferring Canada, Pfizer Canada, Takeda Canada, and Janssen Canada. Speaker’s panel for Abbvie Canada, Janssen Canada, Pfizer Canada, and Takeda Canada. Received research funding from Abbvie Canada, Amgen Canada, Sandoz Canada, Takeda Canada and Pfizer Canada. Ms Dolovich has no conflicts to declare. Dr Graff has consulted to Roche Canada. She receives research funding from CIHR, MS Canada and Crohn’s and Colitis Canada. Dr Bolton receives research funding from CIHR, Brain and Behavior Research Foundation, Crohn’s and Colitis Canada and the MS Canada. Dr Fisk receives research grant support from the Canadian Institutes of Health Research, the National Multiple Sclerosis Society, MS Canada, Crohn’s and Colitis Canada, Research Nova Scotia; consultation and distribution royalties from MAPI Research Trust. Dr Hitchon receives research funding from CIHR, unrelated grant funding from Pfizer; Advisory board for Astra-Zeneca Canada for unrelated product, unrelated research funds from Research Manitoba, Health Sciences Center foundation, International League of Associations for Rheumatology, unrelated educational funds from the Royal College of Physicians and Surgeons of Canada. Dr Lix receives funding from the Canadian Institutes of Health Research and the Natural Sciences and Engineering Research Council of Canada. Dr Patten receives research funding from CIHR, the MS Society of Canada, Roche, Biogen, and the Government of Alberta. He holds the Cuthbertson & Fisher Chair in Pediatric Mental Health at the University of Calgary. Dr Marriott has conducted trials for Biogen Idec, Sanofi and Roche, and receives research funding from MS Canada.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Canadian Institutes of Health Research (THC-135234), Crohn’s and Colitis Canada, and the Waugh Family Chair in Multiple Sclerosis (to RAM). The authors acknowledge use of Shared Health facilities.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.