
Abstract
The function of the lower urinary tract is mainly storage and voiding of urine, which is coordinated by the nervous system. Various diseases of the nervous system may cause neuro-urological symptoms. Neuro-urological symptoms depend on the localization of the disease and the extension of the neurological lesion. About 80% of multiple sclerosis (MS) patients have neuro-urological symptoms within 10 years after diagnosis. In addition, 10% of MS patients may even present with voiding dysfunction at disease onset. In this review, different types of neuromodulation are discussed. The available studies suggest that sacral neuromodulation (SNM) and percutaneous tibial nerve stimulation (PTNS) may be helpful in the neuromodulation of MS-related overactive bladder symptoms. These techniques may not only decrease the severity of symptoms but also significantly improve the quality of life of affected patients. Exploring the role of implantable tibial nerve stimulation devices in patients with MS could open new doors in the management of urgency and urgency incontinence in this patient group.
Introduction
The function of the lower urinary tract is mainly storage and voiding of urine, which is coordinated by the nervous system. 1
Various diseases of the nervous system may cause neuro-urological symptoms. Neuro-urological symptoms depend on the localization of the disease and the extension of the neurological lesion. 2
Neuronal control of the urinary bladder
As the bladder fills during the urine storage phase, the detrusor muscle remains relatively quiescent and the urethral outlet is permanently kept in a contracted state. During the micturition phase, the detrusor muscle contracts and the urethral outlet relaxes. This involves a complex pattern of efferent (motor) and afferent (sensory) signalling in the autonomic and somatic nervous systems. The nerves involved form part of a reflex pathway, with an incorporated conscious control component. 3 The cerebral cortex, brain stem and spinal cord (S2–S4 segments) are the main structures involved in the regulation of lower urinary tract function. The micturition cycle is thought to be initiated in the brain stem, specifically in a region known as the pontine micturition centre. This area is in turn controlled by impulses from the cerebral cortex, which have an inhibitory effect on the detrusor muscle during bladder filling.
Both the autonomic (parasympathetic and sympathetic) and somatic nervous systems innervate the lower urinary tract. Autonomic innervation includes parasympathetic (pelvic) neurons derived from the S2–S4 segments of the spinal cord and sympathetic (hypogastric) neurons from the T10–L2 segments. The parasympathetic nervous system mediates contraction of the detrusor muscle (i.e. micturition) while the sympathetic nervous system contributes to urine storage via relaxation of the detrusor muscle and contraction of the bladder neck and to a lesser extend the urethra. 4 The postganglionic neurotransmitter in parasympathetic neurons is acetylcholine, while in postganglionic sympathetic neurons the transmitter is noradrenaline (norepinephrine). Somatic nerves originate from the S2–S4 segments of the spinal cord and are thought to be solely responsible for direct innervation of the striated muscle of the urethral sphincter and pelvic floor using acetylcholine as the neurotransmitter.
Bladder function disorders in patients with multiple sclerosis
Multiple sclerosis (MS) is an immune-mediated neurological disease of the central nervous system (CNS). The main target of the immune cells are the myelin-producing oligodendrocytes of the CNS which is characterized by demyelinated plaques on the brain, brainstem, cerebellum and/or spinal cord. 5 Demyelinated lesions eventually affect the myelinated nerve tracts that mediate lower urinary tract dysfunction.
About 80% of MS patients have neuro-urological symptoms within 10 years after diagnosis.
In addition, 10% of MS patients may even present with voiding dysfunction at disease onset. The most frequent urinary dysfunctions are detrusor overactivity (DO) due to suprapontine lesions (>60%), detrusor sphincter dysynergia (DSD) (25%) due to spinal cord lesions and hypocontractility which can be seen in 20% of the MS patients with urinary symptoms. 2 Neuro-urological symptoms of lower urinary tract dysfunction include urgency, increased daytime frequency, nocturia and urge urinary incontinence.
Although many goals exist in managing neurogenic detrusor overactivity (NDO), the main goals of treatment include improving the quality of life (QOL) for patients suffering from NDO and preserving the kidneys by preventing high-pressure transmission from the bladder to the upper urinary tract. 6
Epidemiological studies have shown that 50%–90% of all patients with MS complain of lower urinary tract symptoms (LUTS) at some time in their life.7,8 These include increased daytime frequency, nocturia, urgency, urinary incontinence and voiding difficulties. The incidence of urinary symptoms increases with prolonged disease duration and involvement of the motor system. 9
Treatment of bladder function disorders in MS
Different managements, including the use of pharmacotherapy, mainly anticholinergics, and even surgery have been proposed to treat bladder function disorders in patients with MS, but they usually do not restore functional synergy. In addition, some symptomatic treatments have been studied in MS, including, bladder training, 10 physiotherapy,11,12 desmopressin spray,13,14 bladder stimulators, 15 and percutaneous tibial nerve stimulation (PTNS)16–18 (Figure 1).
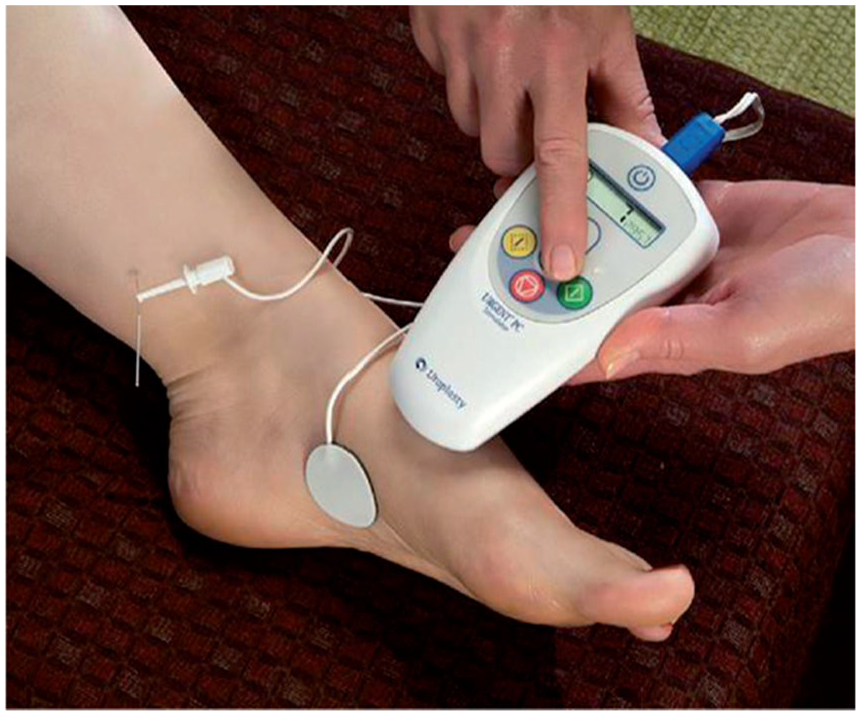
Percutaneous tibial nerve stimulation (PTNS). The patient sits comfortably with the treatment leg elevated. A fine needle electrode is inserted into the lower, inner aspect of the leg, slightly proximal to the medial malleolus. Electrical stimulation is given through the needle electrode near the tibial nerve. A surface electrode or grounding pad, is placed over the medial aspect of the calcaneus on the same leg. (Figure from Gobbi et al. 18 reproduced with permission of SAGE Publications Ltd.)
If patients are refractory to pharmacologic treatment of NDO or cannot tolerate the side effects, repeated intramuscular injections of botulinum toxin into the detrusor may be considered. 6
Furthermore, neuromodulation has been tried in patients with MS and LUTS. Several sites have been studied for neuromodulation including the sacral, pudendal, tibial and genital nerves, but the most widely reported area for the treatment of overactive bladder (OAB) has been the third sacral nerve root (S3). 19
Neuromodulation in MS
In the past, neuromodulatory treatment of OAB has involved intravesical, anal, vaginal, penile and perineal electrical stimulation; these techniques proved to be inconvenient and ineffective. 20
In addition, sacral anterior root neurostimulators, such as the Brindley stimulator have been described for patients with paraplegia, however as this stimulator mandates a dorsal rhizotomy, it is not usable in patients with MS. 21
The use of sacral neuromodulation (SNM) and PTNS has been suggested to be therapeutically beneficial for MS patients suffering from OAB.
SNM
SNM is an established therapy for refractory OAB, non-obstructive retention and frequency–urgency syndrome.22,23 Several studies have reported procedure-related outcomes, effect on QOL, sexual effect, and other off-label uses. 24
SNM involves stimulating the pelvic nerves, but its exact mechanism of action is unknown. SNM may potentiate the somatic afferent inhibition of sensory processing of the bladder in the spinal cord, or it may directly inhibit efferent input to the bladder. 25 While acute percutaneous stimulation of the pelvic nerves, particularly S3, has been shown to have some therapeutic benefit to MS patients with bladder overactivity, the technique is impractical. 26
Although SNM is relatively safe and is accompanied with small complication rates, the need for battery change, compatibility with magnetic resonance imaging (MRI) and the high costs of the device and procedure, can be mentioned as drawbacks of SNM.
Technology has brought about changes to SNM therapy and has rendered it as a minimally invasive procedure. The presence of tined lead, smaller implantable pulse generator and the different available patient programmers are the factors of new modifications in this procedure. 27
SNM in MS
The implantation of a device that stimulates the pelvic nerves is a preferred technique. 25
Minardi and Muzzonigro 28 found that SNM via an implantable intermittent pulse generator (IPG) improved the urinary symptoms in 25 MS patients who suffered from medication-refractory OAB and responded positively to test stimulations of the sacral nerve.
Similarly another study showed that 12 female MS patients with bladder overactivity, who underwent successful SNM IPG implantation, experienced a decreased number of catheterizations per day. 29
In a retrospective study of 17 MS patients utilizing SNM outside of trial setting, 75% of patients reported significant and long-lasting effect on the QOL, bladder symptoms and number of self-catheterizations. Results were favourable in patients who had either storage or voiding symptoms, but not in those with mixed symptoms. 30
While the use of implantable SNM for treatment of bladder overactivity in MS patients is promising, there have been some side effects including stimulation-related pain and hardware malfunction.28,29
Transcranial magnetic stimulation
Repetitive transcranial magnetic stimulation (rTMS) can modulate cortical excitability and also induce long-lasting neuroplastic changes when it is applied over the cortical areas corresponding to the pelvic region. 31 rTMS can be delivered as continuous trains of low frequency (LF, 1 Hz) or bursts of higher frequency (HF, 5 Hz). 32 There has been one report regarding a study in 10 patients with MS, that showed rTMS to result in an improvement of voiding phase lower urinary tract symptoms and a significant reduction of postvoidal residue. 33
PTNS
PTNS is a minimally invasive neuromodulation technique that has been shown as an effective treatment for patients with neurogenic and non-neurogenic LUTS unresponsive to medical treatment.34,35
The mechanism of action of PTNS is not completely understood yet. Long-latency somatosensory evoked potentials (LL-SEPs) are well known to reflect information processing in the brain after stimulation of peripheral somatosensory system.
PTNS involves stimulating the posterior tibial nerve, which contains L4-S3 fibres. Although the mechanism of action remains unproven, Caldwell 36 suggests that electrical stimulation of the tibial nerve may inhibit bladder activity by depolarizing somatic sacral and lumbar afferent fibres. These depolarized fibres, in turn, inhibit preganglionic bladder motor neurons in the spinal cord. 37
Finazzi-Agro et al. 38 treated 16 women with refractory OAB by PTNS while 8 women with the same diagnosis underwent sham stimulation. LL-SEPs were performed at baseline and at the end of treatment. The authors found a modification of brain activity after PTNS and speculated that its efficacy is mediated by sacral and suprasacral centres of stimulus elaboration involving cortical associative areas. A specific beneficial effect which is enhanced due to the demyelinating nature of the disease (MS as ‘less disconnecting pathology’ in comparison with spinal trauma or primary degenerative diseases) remains speculative.
PTNS in MS
The efficacy of 12 weeks of PTNS treatment to improve idiopathic OAB symptoms has been established through randomized, controlled trials, with long-term durability and sustained therapeutic effects during 12 and 24 months.34,39–41
In addition, there have been studies that looked at the efficacy of PTNS in the treatment of LUTS in patients with MS.
PTNS was demonstrated to be effective in suppressing detrusor overactivity in MS patients when evaluating the acute effect of PTNS on urodynamic parameters.16,17,42
Moreover, a multicentre, prospective trial that included 21 patients (5 men and 16 women) with MS and LUTS unresponsive to anticholinergics treated with 12 sessions of PTNS, showed that there was a significant reduction of daytime frequency (from 9 to 6, p = 0.04), nocturia (from 3 to 1, p = 0.002) and mean post-micturition residual (from 98 ± 124 mL to 43 ± 45 mL, p = 0.02). 18 In addition, the mean voided volume increased from 182 ± 50 mL to 225 ± 50 mL (p = 0.003). In total, 89% of patients reported a treatment satisfaction of 70%. Significant improvement in QoL was seen in most domains of the King’s Health QoL questionnaire (p < 0.05) and no adverse events were reported. 18
Long-term sustained therapeutic effects of PTNS in MS patients were shown in a study with 21 patients (5 men and 16 women) with MS and PTNS treatment. One year PTNS treatment with a tapering protocol of 6, 9 and 12 months of therapy, respectively, was applied. A total of 21 patients were enrolled in the study. 43 The results showed a significant improvement in all voiding diary parameters in the 6th, 9th and 12th months when compared with baseline. Mean values between baseline and 12 month parameters suggested that daytime frequency decreased by 5.4 voids daily, urge incontinence decreased by 3.4 episodes daily, urgency episodes decreased by 7.4 episodes daily, nocturia decreased by 2.6 voids and voided volume improved by a mean of 72.1 mL. 43
PTNS over 12 weeks was shown to improve urodynamic measurements in 19 MS patients with OAB. 17 An increased mean urine volume, increased maximal cystometric capacity and suppressed detrusor contraction was demonstrated. In addition, PTNS has been shown to improve subjective LUTS in MS patients. 44
The less invasive, transcutaneous (via surface electrodes) tibial nerve stimuation, rather than percutaneous stimulation of the tibial nerve, may also be therapeutically effective in treating MS patients with OAB. Using a sample size of 70 patients, a study found that daily 20-min transcutaneous PTNS sessions over the course of 3 months resulted in reduced urinary urgency, frequency and incontinence. 20
To date, the transcutaneous technique has not been studied against the percutaneous technique in bladder dysfunction. However, based on faecal incontinence studies, the percutaneous technique is thought to be relatively more effective. 45 Also based on faecal incontinence non-randomized studies, SNM and PTNS are thought to be comparable in efficacy. 46 A study among 33 patients with MS and faecal incontinence, showed that PTNS has potential as an effective therapy for faecal incontinence in patients with MS. 47
PTNS is more cost-effective than SNM for bladder overactivity, but patients utilizing SNM are less likely to discontinue therapy. 48
Implantable PTNS for MS
More recently, some clinical trials have reported positive outcomes for battery-free implantable devices that can stimulate the tibial nerve transcutaneousely. A battery-free stimulation device for tibial nerve stimulation (BlueWind Medical, Herzliya, Israel) was studied in 15 patients. 49 Two males and 13 females were enrolled in this study. Mean age was 54 (range 19–72) years. Five of 15 patients were previously treated with percutaneous tibial nerve stimulation and 12 experienced urgency urinary incontinence. Safety and efficacy assessments were reported at 3 months after activation with a 3-day bladder diary, a 24-h pad test and two QOL questionnaires.
At 3 months of follow up, a significant change was seen in 24-h frequency from a mean, the number of severe urinary urgency episodes from, the number of severe incontinence episodes from episodes per day, urinary loss per day and improvement in QoL.
After implantation, three patients received prolonged antibiotic treatment and three received pain medication for 1 week. In one patient, the device was explanted due to pain and swelling suspicious for infection, although tissue cultures did not reveal a bacterial infection. 49
The most important development is a battery-free implantable tined lead, StimRouter™ distributed by Bioness, to stimulate the tibial nerve. In June 2019, the first patient with OAB and urgency incontinence due to MS was implanted with a StimRouter™ in Germany, resulting in a reduction of urgency incontinence as well as urgency episodes and frequency in this patient. More research is needed to establish the role of StimRouter™ in patients with MS.
Conclusion
It can be concluded that, the results of the available studies suggest that SNM and PTNS may be helpful in the neuromodulation of MS-related OAB. These techniques may not only decrease the severity of symptoms but also significantly improve the QOL.20,28,44
Because most of the data are limited to case studies, these techniques are currently not included in expert panel consensus recommendations in some countries. 50 SNM and PTNS are not recommended for MS patients with bladder hypoactivity. 28
It seems to be justified that neuromodulation (SNM and PTNS) are safe and effective treatments for LUTS in patients with MS. Exploring the role of implantable devices such as BlueWind or StimRouter™ in patients with MS could open new doors in the management of urgency and urgency incontinence in this patient group.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The author is a consultant for Astellas Pharma, Dr Pfleger pharma, Allergan, Bioness, Medtronic, Janssen Pharma.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.