
Abstract
Background:
Findings regarding the prevalence of vascular comorbidities in multiple sclerosis (MS) are conflicting.
Objective:
The objective of this review is to estimate the incidence and prevalence of vascular comorbidities and predisposing comorbidities in persons with MS and to assess the quality of the included studies.
Methods:
The PubMed, EMBASE, SCOPUS and Web of Knowledge databases, conference proceedings, and reference lists of retrieved articles were searched. One reviewer abstracted data using a standardized data collection form, while the second reviewer verified the abstraction. Included studies were assessed qualitatively. Quantitatively, we assessed studies using the I2 statistic, and conducted meta-analyses for population-based studies only.
Results:
The prevalence of hypertension and hyperlipidemia exceeded 10% in the MS population and increased with age. While the prevalence of ischemic heart disease, congestive heart failure, and stroke were less than 5% overall, the prevalence of these conditions exceeded expectations when compared to the general population. Cardiac valvular disease, however, affected the MS population less often than expected. Problems with study quality were common.
Conclusion:
Despite the relatively high prevalence of some vascular comorbidities in the MS population, important gaps exist in our understanding of their epidemiology. Most of our knowledge is based on studies conducted in a small number of regions.
Keywords
Introduction
In multiple sclerosis (MS), disease characteristics such as age at symptom onset and type of symptoms at onset are relatively poor at explaining heterogeneity in clinical outcomes such as disability progression. 1 Several studies suggest that vascular comorbidities including hypertension, hyperlipidemia, and heart disease may adversely influence disability progression. 2 Hyperlipidemia is associated with the accumulation of new hyperintense lesions on magnetic resonance imaging (MRI). 3 Further, hypertension and other comorbidities are associated with lower health-related quality of life. 4
Findings regarding the prevalence of vascular comorbidities in MS are conflicting. For example, some studies have reported that individuals with MS have an increased risk of ischemic heart disease 5 while others have suggested that individuals with MS are less likely to be hospitalized for ischemic heart disease. 6 Findings regarding stroke also conflict.7–11 Therefore, we aimed to systematically review the literature regarding the incidence and prevalence of comorbid vascular disorders in MS, and to evaluate the quality of all included studies.
Methods
This systematic review was part of a study regarding the worldwide incidence and prevalence of comorbidity in MS. Herein we describe the findings for vascular comorbidities including hypertension, hyperlipidemia, cardiac disease, cerebrovascular disease, and peripheral vascular disease.
The approach to developing the search strategies for each comorbidity is delineated in detail elsewhere. 12 Briefly, we searched the published literature using PubMed and EMBASE, and conference proceedings using SCOPUS and Web of Knowledge for all years available through November 1, 2013 (Supplemental Appendix I). The reference lists of articles identified by electronic searches were manually reviewed.
The abstracts were independently reviewed by two individuals with respect to relevance, with abstracts selected by either reviewer going on to full-text review. To be included a study had to be (i) conducted in an MS population, (ii) clearly identify the comorbidity of interest, (iii) report the incidence or prevalence of the comorbidity, (iv) include original data, and (v) be published in English. Disagreements between reviewers were resolved by consensus.
For each article selected, one reviewer abstracted information using a standardized data collection form. The second reviewer verified the data abstraction. As detailed elsewhere, the data collection form captured general study characteristics, as well as incidence and prevalence estimates. 12 Each study was critically appraised using a standardized assessment tool used in a systematic review of the incidence and prevalence of MS, and awarded quality scores based on yes or no responses to nine questions. 12
Statistical analysis
The I2 test was used to quantitatively assess heterogeneity of population-based studies in which the expressed aim was to assess the incidence or prevalence of comorbidity. Random-effects meta-analyses were conducted using a Microsoft Excel spreadsheet developed for this purpose. 13 We employed a continuity correction of 0.5 for studies in which zero events were recorded. 14
Results
Diabetes
Search
The search identified 590 unique citations after duplicates were removed (Supplemental Figure 1). After abstract screening and hand searching, 65 articles met the criteria for full-text review, of which we excluded 26, leaving 39.5,7–11,15–47
Study characteristics
The studies were conducted from 1930 to 2009, but the time period was not reported in several studies. Most studies were conducted in Europe (19, 48.7%) or North America (15, 38.5%), with only four (10.2%) conducted in Asia and two (5.1%) conducted in Australia. Data sources used included clinical databases or medical records review (16, 41.0%), administrative data (12, 30.8%), self-report (10, 25.6%), and interviews (seven, 17.9%); some studies used multiple data sources. Among studies using clinical databases, medical records or interviews,18,19,21,25–27,29,31,36–38,41,42,46,48 the diagnostic criteria for MS were reported in nine (56.2%) studies;25,26,31,33,36–38,40,42,46 the Poser criteria were most often used (six, 66.7%), sometimes in combination with the McDonald criteria. Most studies using administrative data specified the diagnostic codes for MS used; however, only four specified that the administrative case definitions for MS had been validated against a reference standard.5,23,30,34 Diabetes was ascertained largely using the same approaches as those used to identify the MS population. Specific diagnostic criteria for diabetes were rarely reported,36,37 and the validity of administrative case definitions for diabetes was assessed or described in only three studies.23,30,34 Study quality was variable (Supplemental Table 1, associated manuscript 12 ) with quality scores ranging from one of nine to eight of eight overall, and four of nine to eight of eight among population-based studies.
Incidence
Two studies reported the incidence of diabetes to range from 0.001% to 1.01% (Supplemental Table 1).5,47
Prevalence
Thirty-nine studies reported prevalence of diabetes, variably for type I diabetes, type II diabetes, or both (Supplemental Table 2).5,7–11,15–47 Possibly because of the different definitions of diabetes used, and variation in whether the MS cohorts were incident or prevalent, findings varied widely for diabetes (type unspecified) from 0% to 27.1%. Findings for type I diabetes are discussed with those for autoimmune disease. 49
For type II diabetes the prevalence varied from 6.75% to 8.57%.8,27 Only one of these studies was population based, reporting the highest estimate. 8 The prevalence of diabetes appeared to be higher in older populations and in men versus women. The prevalence of diabetes was likely underestimated in the studies relying exclusively on hospital data,5,7,20,28 as only hospitalized individuals’ data were captured. In the study from New York State only individuals hospitalized for reasons other than MS were included, potentially biasing the estimated prevalence of diabetes. 7
Seven studies reported diabetes prevalence at or before the diagnosis of MS to range from 0.85% to 5.65%.5,17,23,28,30,50,51 The prevalence of diabetes reported at MS diagnosis was very similar in the two Scandinavian studies that used similar designs and administrative data sources.5,28 These estimates were also quite similar to one based on self-reported diagnoses of diabetes from the North American Research Committee on Multiple Sclerosis (NARCOMS) Registry (1.2%). 50
Comparisons
Findings from those studies comparing the prevalence of diabetes in the MS population to another population were completely inconsistent, variously suggesting the prevalence of diabetes to be higher, lower or the same in the MS population.7,8,10,11,17,21,23,25,28,30–34,36,38,42,44 –46,51 Several of these studies reported comparisons based on the literature, rather than concurrently evaluating a control population (Supplemental Table 3).
Hyperlipidemia
Search
After duplicates were removed, the search identified 44 unique citations (Supplemental Figure 2). After abstract screening and hand searching, 18 articles met the criteria for full-text review, of which we excluded five, leaving 13 (Supplemental Table 4).7–10,16,26,29,34,35,39,40,44,51
Study characteristics
The studies were conducted from 1984 to 2010. Most were conducted in North America (eight, 61.5%), while three (23.1%) were conducted in Asia (all in Taiwan), one (7.7%) study was conducted in Europe and one (7.7%) was conducted in Australia. Diagnoses of MS and hyperlipidemia were established by several methods including administrative data either with or without formal validation of the case definition for MS (six, 46.1%), self-report (four, 30.8%), and review of medical records or clinical database (three, 23.0%). Only one of the studies that used administrative data reported efforts to validate the approach used to identify hyperlipidemia. 34 One of the studies from Taiwan aimed to improve the specificity of hyperlipidemia as identified using administrative data by requiring one hospital or two ambulatory claims for hyperlipidemia over two years, but the accuracy of this approach was not reported. 8 Study quality was highly variable, with quality scores ranging from two of nine to eight of eight overall and from four of eight to eight of eight among population-based studies (Supplemental Table 2, accompanying manuscript 12 ).
Incidence
None of the studies reported the incidence of hyperlipidemia.
Prevalence
The prevalence of hyperlipidemia ranged from 3.0% to 47.8%. In the study from New York State only individuals hospitalized for reasons other than MS were included, potentially biasing the estimated prevalence of hyperlipidemia. 7 The prevalence of hyperlipidemia was particularly high among a population of male veterans at 48.5% (Supplemental Table 4). 10
We identified only three population-based studies that aimed to estimate the prevalence of hyperlipidemia;8,34 39 all used administrative data. The first used a validated case definition and reported a prevalence of 13.8% (12.4%–15.2%) in 2005, 34 but noted a rising prevalence of hyperlipidemia over time. Heterogeneity was high, as measured by the I2 statistic (94.9). The summary prevalence estimate for these studies was 10.9% (95% confidence interval (CI): 5.6%–16.1%) (Figure 1).
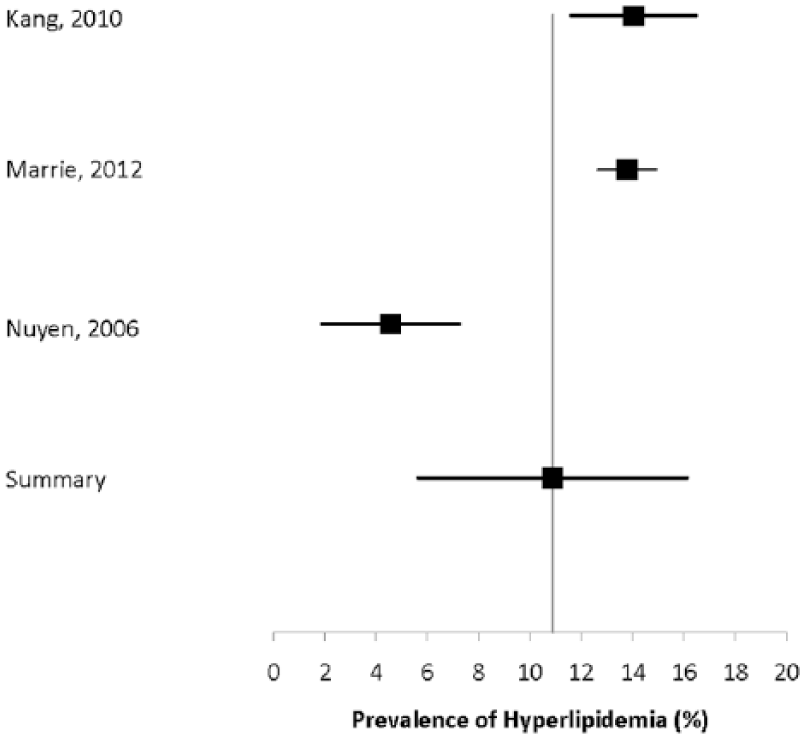
Forest plot of the prevalence of hyperlipidemia in multiple sclerosis in population-based studies.
Comparisons
Of the seven studies that compared the prevalence of hyperlipidemia in the MS population with a concurrent control population or published data for the general population, five reported a higher prevalence of hyperlipidemia in the MS population (Supplemental Table 5).8–10,44,51 Three of these studies used the same administrative data source in Taiwan.8,44,51 The other two studies reported a lower prevalence,7,34 but one reported that although hyperlipidemia was less prevalent in the MS population over a 20-year period, this disparity had dissipated by 2005 (Supplemental Table 5). 34
Hypertension
Search
The search identified 218 unique citations (Supplemental Figure 3). After abstract screening and hand searching, 26 articles met the criteria for full-text review, of which we excluded six. Twenty studies were the subject of this review.
Study characteristics
The studies were conducted from 1997 to 2009.4,5,7–11,16,26,28,32–35,40,44,51–54 Most were conducted in North America (10, 50%), while three (15%) were conducted in Europe and the other two (10%) were conducted in Asia (Taiwan). Diagnoses of MS were established by several methods including administrative data either with or without formal validation of the case definition for MS (nine, 45%), self-report (three by questionnaire or interview, 15%), and review of medical records or clinical database (three, 15%). Hypertension was ascertained by administrative data codes (nine, 45%), self-report (five, 25%), and review of medical records or a clinical database (one, 5%). Only one of the studies that used administrative data reported efforts to validate the approach used to identify hypertension. 34 One of the studies from Taiwan aimed to improve the specificity of hypertension as identified using administrative data by requiring one hospital or two ambulatory claims for hypertension over two years, similar to a validated Canadian definition, 55 but the accuracy of this approach was not reported. 8 Study quality was highly variable, with quality scores ranging from two of seven to eight of eight overall, and from four of nine to eight of eight among population-based studies (Supplemental Table 2, associated manuscript 12 ).
Incidence
The only study reporting the incidence of hypertension found that 3.73% of an incident MS cohort developed the condition over a maximum follow-up of 30 years (Supplemental Table 6). 5
Prevalence
The reported prevalence of hypertension varied substantially from 0% to 47.8%,4,5,7–11,16,26,28,32–35,40,44,51–54 but the study populations were heterogeneous, including both incident and prevalent MS cohorts, and cohorts restricted to men. Some studies evaluated the prevalence of hypertension at or before the diagnosis of MS while others evaluated it after MS diagnosis (Supplemental Table 7). The prevalence of hypertension was likely biased in the studies relying exclusively on hospital data, as only hospitalized individuals were captured. In the two truly population-based studies with the aim of evaluating the prevalence of hypertension, the findings varied from 16% to 20.8%.8,34 Both studies used administrative data, with reasonably similar case definitions for hypertension. Heterogeneity was high, as measured by the I2 statistic (89.9). The summary prevalence estimate for these studies was 18.6% (95% CI: 13.9%–23.2%) (Figure 2).
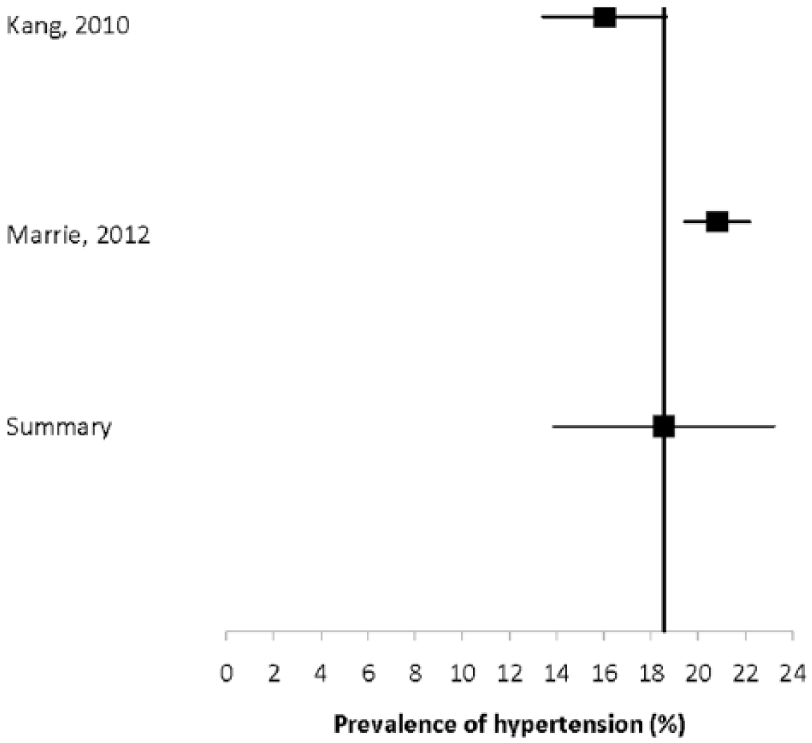
Forest plot of the prevalence of hypertension in multiple sclerosis in population-based studies.
In four studies, the prevalence of hypertension at diagnosis ranged from 0% to 8%,5,28,35,51 with the highest reported prevalence being in the North American cohort. 35
Comparisons
Two Scandinavian studies reported the incidence of hypertension in incident MS populations and in the general population but did not make statistical comparisons.5,28 Eleven studies compared the prevalence of hypertension in the MS population with a comparator population.7–11,32–34,44,51 Six of these reported that hypertension was less common in the MS population,8,10,33,44,51 while the others reported that it was more common (Supplemental Table 8).8,10,33,44,52
Cardiac arrhythmia
Search
The search identified 41 citations (Supplemental Figure 4). After abstract screening and hand searching, five articles met the criteria for full-text review, of which we excluded one. Four studies were the subject of this review.5,8,11,28
Study characteristics
The studies were conducted from 1977 to 2009. Half of the studies were conducted in Europe,5,28 while the other two were conducted in North America and Asia.8,11 All of these studies used administrative data and identified the MS population and comorbidities of interest using International Classification of Diseases (ICD) codes. While one study cited high predictive values for diagnoses based on hospital administrative data, 28 validity of the administrative codes used was generally not reported. Study quality was variable (Supplemental Table 2, associated manuscript 12 ) with quality scores ranging from four of eight to six of eight overall and from four of eight to six of eight among the three population-based studies.5,8,28 Limitations of the studies included failure to report validity of the administrative case definitions used to identify the MS population or cardiac arrhythmia, and failure to age-standardize findings. For example, age-standardized findings were reported in only one study. 28
Incidence
Both European studies reported the incidence of atrial fibrillation or flutter in incident MS cohorts.5,28 The incidence was 1.2% in Denmark and 0.55% in Sweden (Supplemental Table 9).5,28 Since these studies relied on inpatient hospitalizations, the incidence of atrial fibrillation may have been underestimated slightly. Based on an I2 statistic of 96.6%, heterogeneity was high. The summary estimate of the incidence of atrial fibrillation was 0.89% (95% CI: 0.68%–1.11%) (Figure 3).
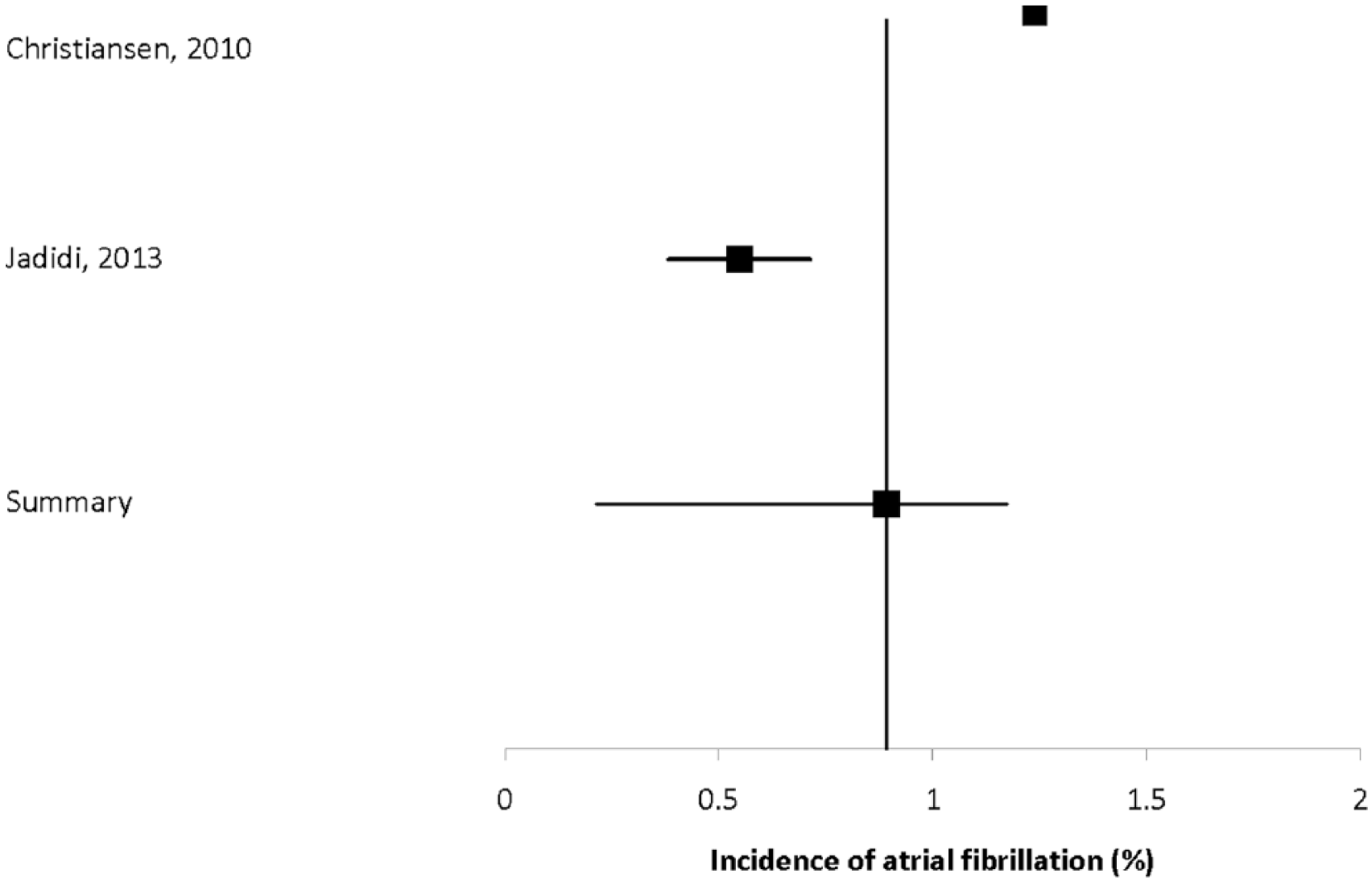
Forest plot of the incidence of atrial fibrillation in multiple sclerosis in population-based studies.
Prevalence
Two studies reported the prevalence of cardiac arrhythmia, with estimates ranging from 2.6% to 4.5% (Supplemental Table 10).8,11 Only one of these studies was population based.
Comparisons
All studies compared the burden of cardiac arrhythmias in the MS population with the general population, but findings conflicted. The two European studies found the incidence of atrial fibrillation was about one-third lower in the incident MS population than in the matched population.5,28 Similarly the prevalence of atrial fibrillation was lower in the hospitalized elderly population with MS than in the non-MS hospitalized population. 11 However, in the Taiwanese population, which largely consists of ethnic Chinese, cardiac arrhythmia occurred more than twice as often in the MS population as in the matched population (Supplemental Table 11). 8
Cardiac valvular disease
Search
The search identified two unique citations (Supplemental Figure 5). After abstract screening and hand searching, four articles met the criteria for full-text review, of which we excluded two. Two studies were the subject of this review.5,28
Study characteristics
The studies were conducted from 1977 to 2009. Both studies were conducted in Europe and used incident MS cohorts, as identified using diagnoses in inpatient hospital registers (administrative data). The Danish study cited the positive predictive value of a diagnosis of MS in the hospital register although the citation referred to an abstract, 5 but the Swedish study did not report the validity of MS as identified using administrative data. Neither study reported the validity of diagnoses of valvular disease based on administrative data. Quality scores ranged from five of eight to six of eight (both population based).
Incidence
Incidence of cardiac valvular disease was reported by one study to be 0.7% over a 30-year follow-up period (Supplemental Table 12). 5
Prevalence
Both studies reported the prevalence of cardiac valvular disease at the time of first diagnosis of MS to range from 0% to 2.3% (Supplemental Table 13).5,28 The sex distributions of the two populations were similar (64.1% and 68.05% female). Because of differences in the way the age distributions were reported they were difficult to compare, but the Danish study reported that 3.8% of the population was over age 70 years, 5 while 13.6% of the Swedish study population was over age 60 years. 28 The relatively high proportion of older individuals in both studies suggests that some of the MS cases identified were not truly incident. Since valvular disease was identified in only hospitalized individuals the true prevalence may be underestimated. Neither of these studies investigated valvular disease as the primary aim.
Comparisons
Neither study reported a statistical comparison of the prevalence of valvular disease between the MS population and controls, but valvular disease consistently occurred less often in the MS population (Supplemental Table 14).
Ischemic heart disease
Search
The search identified 170 unique citations (Supplemental Figure 6). After abstract screening and hand searching, 19 articles met the criteria for full-text review, of which we excluded five. Fourteen studies were the subject of this review.5,7–11,23,26,28,29,32,39,44,56
Study characteristics
The studies were conducted from 1970 to 2009. Most studies were conducted in North America (six, 42.8%) or Europe (five, 35.7%), with only two (14.3%) conducted in Asia and one (7.1%) conducted in Australia. Diagnoses of MS were established by several methods including administrative data either with or without formal validation of the case definition for MS (nine, 64.3%), self-report (two by questionnaire or interview, 14.3%), and diagnoses in an electronic health record (one, 7.1%) or clinical database (one, 7.1%). Ischemic heart disease was ascertained by administrative data codes (nine, 64.3%), self-report (three, 21.4%), and review of medical records, electronic charts or a clinical database (three, 21.4%). With one exception, studies that used administrative data did not report the validity of the case definitions used for ischemic heart disease. 56 Quality scores ranged from three of seven to eight of eight overall and from four of eight to eight of eight among population-based studies (Supplemental Table 2, associated manuscript 12 ).
Incidence
Three studies, two from Europe and one from North America, reported the incidence of ischemic heart disease.5,28,56 The two European studies reported that the incidence of myocardial infarction in incident MS cohorts ranged from to 2.36% to 2.75% (Supplemental Table 15).5,28 The North American study reported the incidence of ischemic heart disease, not restricted solely to myocardial infarction, but also in an incident MS cohort. 56
Prevalence
Ten studies reported the prevalence of ischemic heart disease, while one reported the prevalence of cardiovascular disease, without distinguishing ischemic heart disease specifically (Supplemental Table 16).7–11,23,26,29,32,39,44,56 The crude prevalence of ischemic heart disease ranged from 0.78% to 22.2%. The crude prevalence of myocardial infarction was 1.43% in a contemporary American cohort. 7 In a temporally more remote Swedish cohort the prevalence of myocardial infarction was as high as 12.7% in older males. 32 The prevalence of ischemic heart disease was lower in incident MS cohorts than prevalent MS cohorts.
Among three population-based studies that aimed to estimate prevalence of ischemic heart disease,8,39,56 heterogeneity was high (I2 = 97.6%). The summary estimate of prevalence was 2.50% (95% CI: 0–5.77%) (Figure 4).
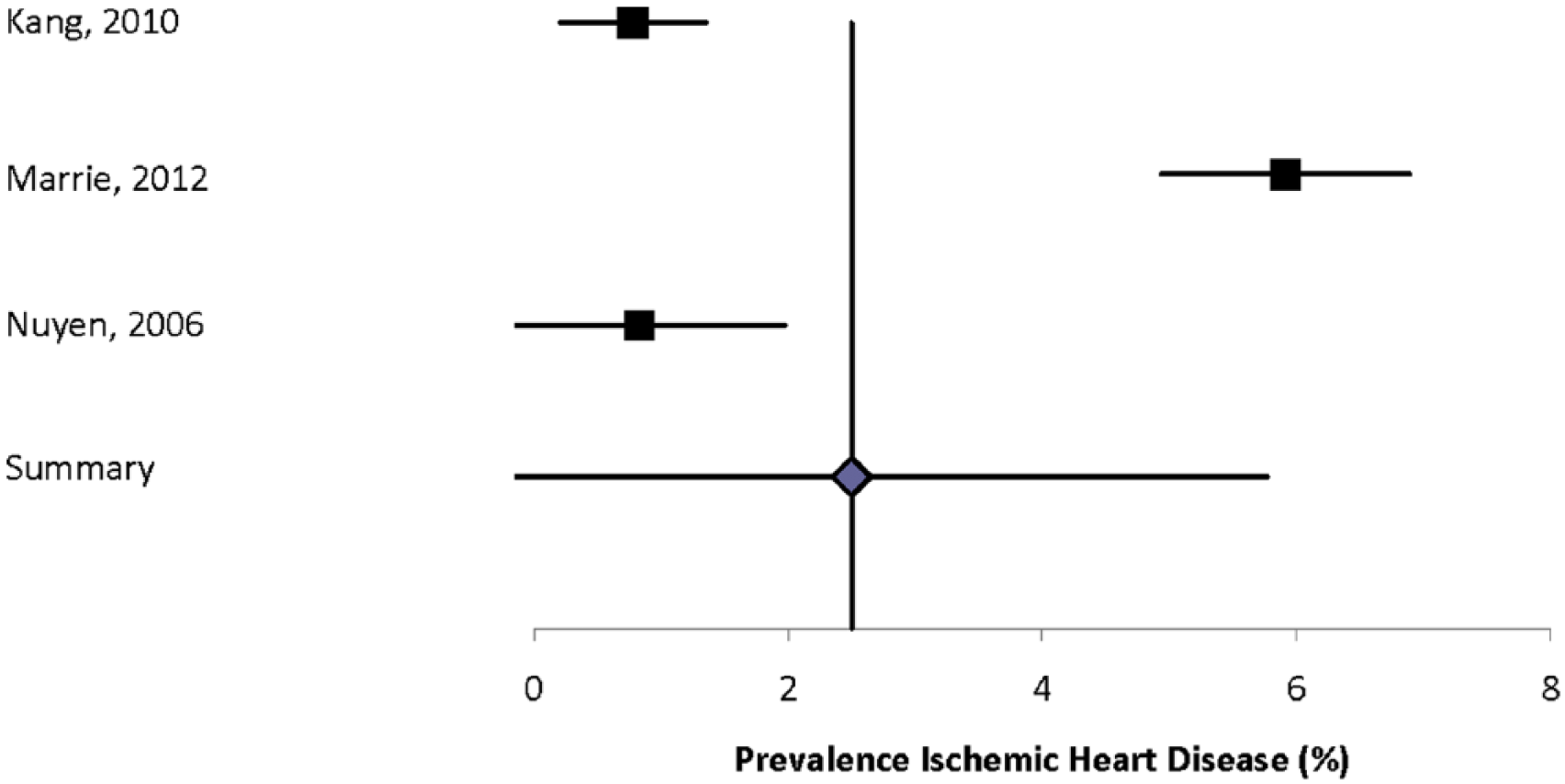
Forest plot of the prevalence of ischemic heart disease in multiple sclerosis in population-based studies.
Comparisons
All of the studies that reported the incidence of ischemic heart disease also compared findings to matched populations (Supplemental Table 17);5,28,56 all found elevated incidence rate ratios in their incident MS populations.
Congestive heart failure (CHF)
Search
After duplicates were removed the search identified 421 abstracts (Supplemental Figure 7). After abstract screening and hand searching of reference lists, 10 articles met the criteria for full-text review, of which we excluded six, leaving four.5,8,11,28
Study characteristics
The time periods covered by the studies ranged from 1977 to 2009. Half of the studies were conducted in Europe, both in Scandinavian countries,5,28 while the others were conducted in North America 11 and Asia. 8 All of the studies used administrative data.
Quality scores ranged from four of eight to seven of eight (all population-based studies) (Supplemental Table 18). Limitations of the studies included failure to report validity of the administrative case definitions used to identify the MS population or CHF, focus on hospital data rather than hospital and outpatient data, and failure to age-standardize findings. Christiansen et al. reported that the positive predictive value of MS in their source database was 94%. 5 The other studies did not report on the validity of their case definitions for MS, and none validated their administrative case definitions for CHF against a reference standard.
Incidence
Two European studies reported the incidence of CHF in incident MS cohorts, with findings ranging from 0.89% to 2.86% (Supplemental Table 19).5,28 Heterogeneity of the findings was high (I2 = 99.2%). The summary estimate of incidence was 1.87% (95% CI: 0%–3.80%).
Prevalence
Two studies, one population-based, reported the prevalence of CHF, with findings ranging from 1.8% to 5.39% (Supplemental Table 20).8,11 The prevalence of CHF was higher in the American study in which all members of the MS population were hospitalized, and aged 65 years and older. 11
Comparisons
All of the studies compared the incidence or prevalence of CHF in the MS population to a comparison population (Supplemental Table 21). The Danish study found a nearly two-fold increased incidence of CHF in the incident MS population versus an age- and sex-matched cohort from the general population in the first year after MS diagnosis, 5 but not over a 30-year follow-up period. The Swedish study also found a nearly two-fold increased risk of CHF in the MS population as compared to an age- and sex-matched cohort from the general population. 28 The Taiwanese study comparing the prevalence of CHF in a prevalent MS population as compared to matched controls similarly found a two-fold increased risk of CHF in the MS population. 8 However, the North American study, which was restricted to hospitalized patients with prevalent MS over age 65 years, drew the opposite conclusion, possibly because of differences in study population and design. 11
Cerebrovascular disease
Search
The search identified 515 abstracts for relevance review (Supplemental Figure 8). After abstract screening and hand searching of reference lists, 11 articles met the criteria for full-text review, of which we excluded one. Ten studies were the subject of this review.5,7–11,22,28,39,57
Study characteristics
The studies were conducted from 1977 to 2010. Four (40%) of the studies were conducted in Europe, while the others were conducted in North America (four, 40%) and Asia (one, 10%) and Australia (one, 10%). Eight of these studies used administrative data and identified the MS population and outcomes of interest using ICD codes. One study cited a high predictive value for MS diagnoses based on hospital administrative data; 5 validity of the administrative codes used was generally not reported. Three studies were population based. Limitations of the studies included failure to report validity of the administrative case definitions used to identify the MS population or stroke, and failure to age-standardize findings. The remaining studies used self-report to identify comorbid cerebrovascular disease. Quality scores ranged from two of nine to six of eight overall, and from four of eight to six of eight among population-based studies.
Incidence
Two Scandinavian (Denmark, Sweden) studies using administrative data reported the incidence of stroke, both in hospitalized, incident MS populations (Supplemental Table 22).5,28 The duration of follow-up and case definitions for stroke differed slightly between studies, but the findings were similar. The incidence of any stroke was 2.85% in Denmark, 5 and 2.53% in Sweden. 28 The reported incidence of ischemic stroke in Denmark was 1.22%. Heterogeneity of these studies was moderate (I2 = 47.4). The summary estimate for the incidence of any stroke was 2.73% (95% CI: 2.51%–2.95%) (Figure 5).
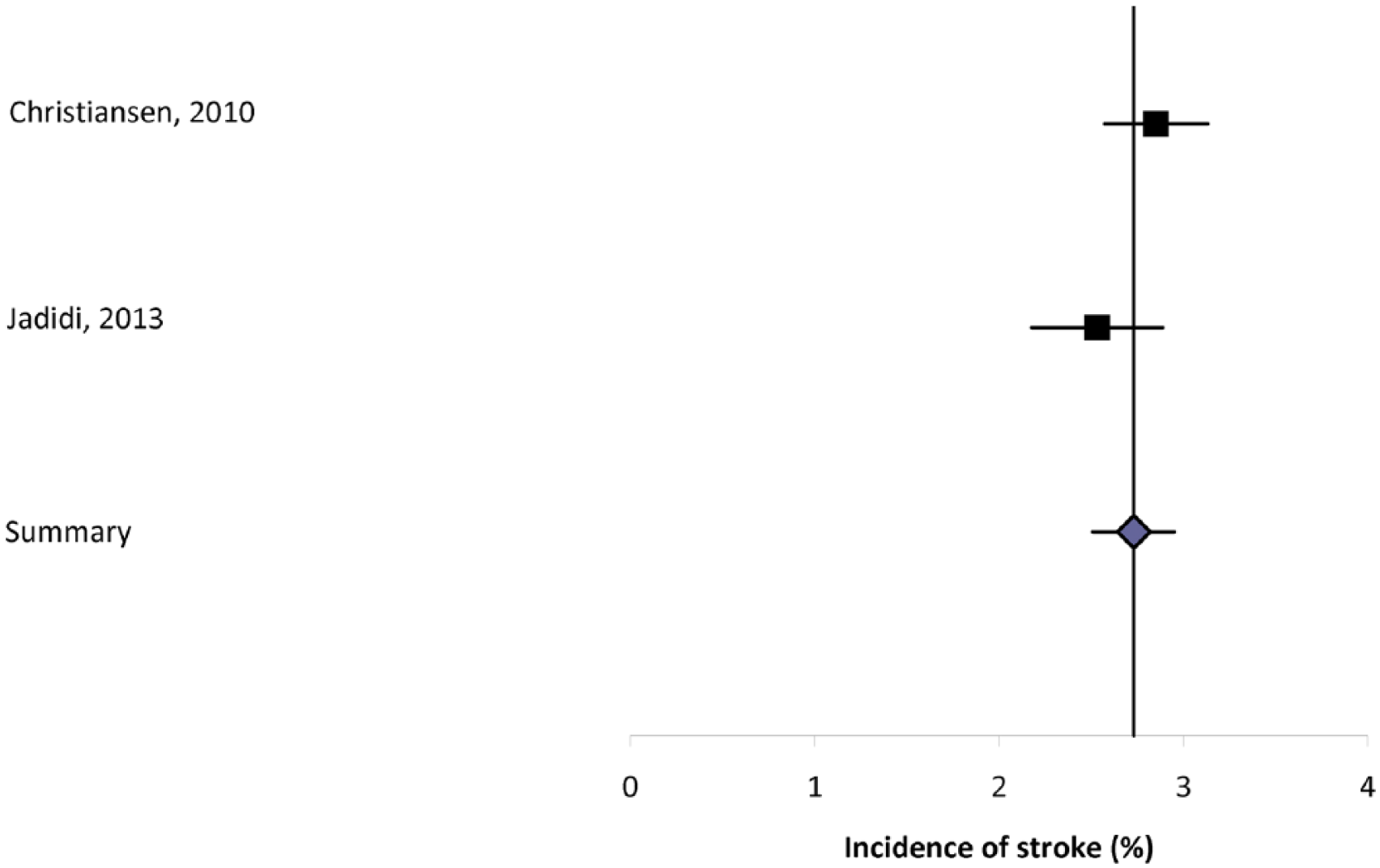
Forest plot of the incidence of stroke in multiple sclerosis in population-based studies.
Prevalence
Eight studies reported the prevalence of cerebrovascular disease, with one of the studies being restricted to men with MS (Supplemental Table 22).7–11,22,39,57 The definition of stroke varied, in some cases simply being any type of stroke, and in others divided into ischemic and hemorrhagic stroke. The prevalence of any stroke varied from 0.4% to 7.0%, while the prevalence of ischemic stroke varied from 1.2% to 1.4%. Only one study presented sex-specific data for both sexes, and observed a higher prevalence of stroke in women. 57 The two population-based studies aimed to estimate prevalence of stroke, with findings ranging from 0.4% to 6.2%.8,39 The prevalence of stroke was higher in the Taiwanese study, which consisted largely of ethnic Chinese, than in the Dutch study with a predominantly Caucasian population. Heterogeneity of the estimates was substantial (I2 = 97.4). The summary estimate was 3.28% (95% CI: 0%–8.98%) (Supplemental Figure 9).
Comparisons
Seven studies compared the incidence (two) or prevalence (five) of stroke in the MS and a comparator population (Supplemental Table 23). In both studies the incidence of any stroke and ischemic stroke was greater in the MS population than in matched populations.5,28 The prevalence of any stroke and ischemic stroke was higher in the MS population than in the comparator populations in four studies,7 –10 but lower in the fifth study. 11 The prevalence of hemorrhagic stroke did not differ between the hospitalized MS population and matched controls in the single study that evaluated this question. 7
Peripheral vascular disease
Search
The search identified 30 abstracts for relevance review (Supplemental Figure 10). After abstract screening and hand searching, three articles met the criteria for full-text review, all of which were included (Supplementary Table 24).8,35,40
Study characteristics
The studies were conducted from 2000 to 2007, two (66.6%) in North American and one (33.3%) in Asia. The methods used in the studies differed substantially, variously using administrative data without validation of the diagnostic codes or algorithm used, self-report using a validated questionnaire, and medical records review to establish the MS study populations and determine the prevalence of administrative data. Study quality was variable with quality scores ranging from four of eight to six of eight (same variability among population-based studies). Limitations of some of the studies included not being population based, failure to report validity of the approaches used to identify the MS population or peripheral vascular disease, and failure to age-standardize findings.
Incidence
None of the studies reported the incidence of peripheral vascular disease.
Prevalence
In all three of the studies the prevalence of peripheral vascular disease was low, ranging from 1.0% to 3.8% (Supplemental Table 24).8,35,40 The prevalence of peripheral vascular disease at MS diagnosis was even lower (0.41%) in the only study that evaluated this question. 50 Heterogeneity among the two population-based estimates was high (I2 = 88.2%). The summary estimate for these studies was 2.40% (95% CI: 0%–5.14%).
Comparisons
Two of the studies compared the prevalence of peripheral vascular disease in the MS and general populations (Supplemental Table 25).8,58 The population-based Taiwanese study observed that the prevalence of peripheral vascular disease was six-fold higher in the MS population than in matched controls. 8 The study using the NARCOMS volunteer population compared the findings to those obtained from the National Health and Nutrition Examination Survey (NHANES) population. 58 No clear conclusions could be drawn because of differences in the way the findings were reported with respect to age.
Discussion
Worldwide, the burden associated with cardiovascular disease and cerebrovascular disease is considerable, but incidence, prevalence, and associated mortality rates vary substantially by region.59–61 We identified relatively few population-based studies that evaluated the epidemiology of comorbid vascular disease in MS. Based on these studies the prevalence of ischemic heart disease and stroke was less than 5%; however, the prevalence of these conditions increased with age. Given the paucity of studies in regions other than North America and Europe (largely Scandinavia), variations in study design, and lack of standardization of the estimates to account for differences in the age and sex structure of the underlying populations, we could not evaluate geographic variation in the incidence or prevalence of these comorbidities in the MS population. This is an important issue that can be addressed only by conducting similarly designed studies concurrently in multiple regions. To further minimize heterogeneity due to methodologic issues, any such studies using administrative data should also address how well comorbidities are coded in different jurisdictions as under-reporting may occur, 62 potentially differentially.
Based on this systematic review, hypertension, hyperlipidemia, and diabetes are reasonably common in the MS population. The prevalence is higher in prevalent MS populations than in incident MS populations, increases with age, and is higher among men than women. Because of the age-associated increases in disease prevalence, we can expect that these conditions are more common in individuals with longer disease duration, and may be a particular concern as very few studies explicitly aimed to evaluate the incidence of these conditions, and age- and sex-specific estimates were limited. This particularly limits the ability to assess the impact of shorter survival in the MS population on assessment of the incidence and prevalence of conditions that are most prevalent at older ages, such as these ones. These conditions are sufficiently frequent, and associated with enough morbidity in the MS and general population,2,3 to warrant specific efforts at prevention.
Although the findings regarding the incidence and prevalence of cardiovascular and cerebrovascular disease were variable, most well-designed studies suggested an increased risk of ischemic heart disease, CHF, ischemic stroke, and peripheral vascular disease in the MS population as compared to the general population. This may reflect several factors. First, individuals with MS have a higher prevalence of smoking, overweight, and obesity than the general population. Second, they have relatively low levels of physical activity, even early in the disease course when disability is mild. These lower levels of physical activity are associated with subclinical atherosclerosis. 63 The studies we reviewed suggest that diabetes, hypertension, and hyperlipidemia are reasonably prevalent, with a particularly high burden in some populations, although not increased as compared to the general population.10,34 Finally, in other immune-mediated conditions such as rheumatoid arthritis and psoriasis,64,65 the risk of vascular disease is not fully explained by these traditional risk factors, suggesting that inflammatory processes related to the conditions themselves independently increase the risk of disease.
The prevalence of cardiac arrhythmias and valvular disease, which have been the subject of very limited work, were less than 5%. Unexpectedly, the prevalence of valvular disease was lower than expected when compared to age- and sex-matched populations. Risk factors for acquired valvular heart disease include increasing age, hypertension and hyperlipidemia, smoking, overweight or obesity, physical inactivity, rheumatic fever, as well as risk factors for endocarditis. 66 With the exception of risk factors for endocarditis, mainly intravenous drug use, which has been little studied in MS, these other risk factors appear to affect the MS population with equal or greater frequency to the general population. Therefore differences in the prevalence of valvular disease might reflect less adequate control of risk factors in the MS population, or differences in disease ascertainment. This requires further evaluation.
Given prior work reporting an increased risk of death from cardiovascular disease, 67 and adverse impacts on disability progression, an increased focus on these comorbidities in the MS population is required. Studies to establish the incidence and prevalence of these conditions in the MS population worldwide are needed. It is important to understand the clinical characteristics of vascular comorbidities in the MS population, the role of common risk factors. and the role of novel disease-modifying therapies in determining the risk of these conditions. Future research should also focus on understanding the influence of treatments used for these comorbidities on MS. 68
Footnotes
Acknowledgements
Thanks to Tania Gottschalk, BA, MEd, MSc (Librarian, University of Manitoba), who provided assistance regarding the development of the search strategies for this review. This study was conducted under the auspices of the International Advisory Committee on Clinical Trials of New Drugs in Multiple Sclerosis, whose members include Jeffrey Cohen, MD (Cleveland Clinic Foundation, Cleveland, United States), Laura J. Balcer, MD, MSCE (NYU Langone Medical Center, New York City, United States), Brenda Banwell, MD (The Children’s Hospital of Philadelphia, Philadelphia, United States), Michel Clanet, MD (Federation de Neurologie, Toulouse, France), Giancarlo Comi, MD (University Vita-Salute San Raffaele, Milan, Italy), Gary R. Cutter, PhD (University of Alabama at Birmingham, Birmingham, United States), Andrew D. Goodman, MD (University of Rochester Medical Center, Rochester, United States), Hans-Peter Hartung, MD (Heinrich-Heine-University, Duesseldorf, DE), Bernhard Hemmer, MD (Technical University of Munich, Munich, Germany), Catherine Lubetzki, MD, PhD (Fédération des maladies du système nerveux et INSERM 71, Paris, France), Fred D. Lublin, MD (Mount Sinai School of Medicine, New York, United States), Ruth Ann Marrie, MD, PhD (Health Sciences Centre, Winnipeg, Canada), Aaron Miller, MD (Mount Sinai School of Medicine, New York, United States), David H. Miller, MD (University College London, London, United Kingdom), Xavier Montalban, MD (Hospital Universitari Vall d’Hebron, Barcelona, Spain), Paul O’Connor, MD (St Michael’s Hospital, Toronto, Canada), Daniel Pelletier, MD (Yale University School of Medicine, New Haven, United States), Stephen C. Reingold, PhD (Scientific & Clinical Review Assoc, LLC, Salisbury, United States), Alex Rovira Cañellas, MD (Hospital Universitari Vall d’Hebron, Barcelona, Spain), Per Soelberg Sørensen, MD, DMSc (Copenhagen University Hospital, Copenhagen, Denmark), Maria Pia Sormani, PhD (University of Genoa, Genoa, Italy), Olaf Stuve, MD, PhD (University of Texas Health Sciences Center, Dallas, United States), Alan J. Thompson, MD (University College London, London, United Kingdom), Maria Trojano, MD (University of Bari, Bari, Italy), Bernard Uitdehaag, MD, PhD (VU University Medical Center, Amsterdam, Netherlands), Emmaunelle Waubant, MD, PhD (University of California- San Francisco, San Francisco, United States), and Jerry S. Wolinsky, MD (University of Texas HSC, Houston, United States)
Conflicts of interest
Ruth Ann Marrie receives research funding from: Canadian Institutes of Health Research, Public Health Agency of Canada, Manitoba Health Research Council, Health Sciences Centre Foundation, Multiple Sclerosis Society of Canada, Multiple Sclerosis Scientific Foundation, Rx & D Health Research Foundation, and has conducted clinical trials funded by Sanofi-Aventis.
Nadia Reider has nothing to declare.
Jeffrey Cohen reports personal compensation for consulting from EMD Serono, Genentech, Genzyme, Innate Immunotherapeutics, Novartis, and Vaccinex. He receives research support paid to his institution from Biogen Idec, Consortium of MS Centers, US Department of Defense, Genzyme, US National Institutes of Health, National MS Society, Novartis, Receptos, Synthon, Teva, and Vaccinex.
Olaf Stuve is an associate editor of JAMA Neurology, and he serves on the editorial boards of the Multiple Sclerosis Journal, Clinical and Experimental Immunology, and Therapeutic Advances in Neurological Disorders. He has participated in data and safety monitoring committees for Pfizer and Sanofi. Dr Stuve has received grant support from Teva Pharmaceuticals.
Maria Trojano has served on scientific advisory boards for Biogen Idec, Novartis, and Merck Serono; has received speaker honoraria from Biogen-Idec, Sanofi Aventis, Merck-Serono, Teva, and Novartis; and has received research grants from Biogen-Idec, Merck-Serono, and Novartis.
Gary Cutter has served on scientific advisory boards for and/or received funding for travel from Innate immunity, Klein-Buendel Incorporated, Genzyme, Medimmune, Novartis, Nuron Biotech, Spiniflex Pharmaceuticals, Somahlution, Teva Pharmaceuticals; receives royalties from publishing Evaluation of Health Promotion and Disease Prevention (The McGraw Hill Companies, 1984); has received honoraria from GlaxoSmithKline, Novartis, Advanced Health Media Inc, Biogen Idec, EMD Serono Inc, EDJ Associates Inc, the National Heart, Lung, and Blood Institute, National Institute of Neurological Diseases and Stroke, National Marrow Donor Program, Consortium of Multiple Sclerosis Centers; Mt. Sinai School of Medicine and Teva Pharmaceuticals; and has served on independent data and safety monitoring committees for Apotek, Ascendis, Biogen-Idec, Cleveland Clinic, Glaxo Smith Klein Pharmaceuticals, Gilead Pharmaceuticals, Modigenetech/Prolor, Merck/Ono Pharmaceuticals, Merck, Neuren, PCT Bio, Teva, Vivus, NHLBI (Protocol Review Committee), NINDS, NMSS, NICHD (OPRU oversight committee).
Stephen Reingold reports personal consulting fees from the National Multiple Sclerosis Society (NMSS) and the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS), during the conduct of this work; and over the past three years, personal consulting fees from Bayer HealthCare, Biogen Idec, Coronado Biosciences Inc, the Cleveland Clinic Foundation, Eli Lilly & Company, from EMD Serono and Merck Serono, Genentech, F. Hoffmann-LaRoche, Ironwood Pharmaceuticals Inc, ISIS Pharmaceuticals Inc, Medimmune Inc, Novartis Pharmaceuticals Corporation, Observatoire Français de la Sclérosis en Plaques, Opexa Therapeutics, Sanofi-Aventis, SK Biopharmaceuticals, Synthon Pharmaceuticals Inc, Teva Pharmaceutical Industries, and Fondation pour l’aide à la Recherche sur la Sclérosis en Plaques, for activities outside of the submitted work.
Per Soelberg Sorensen has received personal compensation for serving on scientific advisory boards, steering committees, independent data monitoring boards in clinical trials, or speaking at scientific meetings from Biogen Idec, Merck Serono, Novartis, Genmab, Teva, GSK, Genzyme, Bayer Schering, Sanofi-Aventis and MedDay Pharmaceuticals. His research unit has received research support from Biogen Idec, Merck Serono, Teva, Sanofi-Aventis, Novartis, RoFAR, Roche, and Genzyme.
Funding
This work was supported (in part) by the National Multiple Sclerosis Society and a Don Paty Career Development Award from the MS Society of Canada.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.