
Abstract
Background:
Multiple sclerosis (MS) is influenced by pregnancy, sex and hormonal factors.
Objectives:
A comprehensive understanding of the role of pregnancy, sex and hormonal factors can provide insights into disease mechanisms, and new therapeutic developments and can provide improved patient care and treatment.
Methods:
Based on an international conference of experts and a comprehensive PubMed search for publications on these areas in MS, we provide a review of what is known about the impact of these factors on disease demographics, etiology, pathophysiology and clinical course and outcomes.
Results and conclusions:
Recommendations are provided for counseling and management of people with MS before conception, during pregnancy and after delivery. The use of disease-modifying and symptomatic therapies in pregnancy is problematic and such treatments are normally discontinued. Available knowledge about the impact of treatment on the mother, fetus and newborn is discussed. Recommendations for future research to fill knowledge gaps and clarify inconsistencies in available data are made.
Introduction
Sex- and pregnancy-related associations with multiple sclerosis (MS) include a higher and increasing prevalence in females than males and a lower relapse rate during pregnancy. Hormones associated with sex and pregnancy affect experimental models of MS and have therapeutic potential in humans.
Based on proceedings of a European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS)-sponsored international workshop held in March 2013 (see Acknowledgements for attendees list) and a comprehensive literature survey (PubMed search of papers in English, using terms: multiple sclerosis, MS, pregnancy, hormonal factors, treatment and related terms), we present an overview of sex, pregnancy and hormonal factors in MS. We provide etiological and pathophysiological insights from experimental models and clinical studies, and discuss management implications, including pregnancy risk counseling and pharmacological treatment during the reproductive years.
Hormonal effects in experimental models of MS
Animal models of MS demonstrate hormonal effects with potential relevance for pregnancy and development of MS therapies. 1 Estrogens (17β-estradiol-E2- and estriol-E3), progesterone and testosterone may provide anti-inflammatory and neuroprotective effects on induction and effector phases of experimental allergic encephalomyelitis (EAE).2,3 Anti-inflammatory effects appear mainly mediated by estrogen nuclear receptors alpha (ERα) and beta (ERβ) 4 expressed by regulatory CD4+CD25+ T cells (Treg), 5 regulatory B (Breg) cells 6 and dendritic cells 7 and may be abrogated in the absence of B cells 8 and the co-inhibitory receptor, Programmed Death-1 (PD-1) on CD4+ Foxp3+ Treg cells. 9 E2 protective effects on EAE seem to be mediated by binding to the membrane G-protein-coupled receptor 30 (GPR30). 10 Testosterone may work through androgen receptors 11 or after its conversion to estrogen through ERs, or GPR30. Androgens may induce remyelination in cuprizone-induced central nervous system (CNS) demyelination by acting on neural androgen receptors. 12
Some neuroprotective effects of estrogens in EAE are mediated by ERα expressed on astrocytes: 13 ERβ ligands can prevent demyelination and stimulate remyelination 14 and ERβ treatment can affect microglia with protective effects in CNS inflammation. 15 Progesterone appears to affect axonal protection 16 and remyelination, 17 and testosterone can restore synaptic transmission deficits in the hippocampus. 18
Sex-specific prevalence of MS: Temporal prevalence changes
MS is more prevalent in females than males. The female/male ratio has increased in many, but not all, locations19–23 and may reflect epigenetic factors and gene-environment interactions 24 (including sex differences in expression of and environmental effects on candidate genes on the X or Y chromosome); 3 lifestyle changes (contraception, diet, obesity, smoking, sunlight exposure, vitamin D deficiency); 25 higher age at first childbirth, 26 and fewer life-time pregnancies.27–29 Better understanding of factors that underlie the differential sex prevalence should illuminate MS susceptibility factors overall.
Preparing for pregnancy
When pregnancy is contemplated, reproductive decision-making questions include: impact of MS on fertility; risk of MS in offspring; risk to the child of a parent’s MS medications before and during pregnancy; effect of pregnancy on the course of MS; effect of MS on the ability to provide child care; and associated socioeconomic burden to the family. 30
MS and fertility
Female and male parenting over five years prior to MS onset has been associated with a reduced risk of MS,27,31 suggesting that pre-clinical MS may reduce biological fertility or affect reproductive decision making. While MS does not appear to impair fertility in women with MS, 32 the two may occur together. Assisted reproductive techniques using gonadotropin-releasing hormone (GnRH; either agonists or antagonists) and gonadotropins probably increase clinical and magnetic resonance imaging (MRI) lesion activity in MS,33–35 with an increased annualized relapse rate in the three months following in vitro fertilization (IVF). 34 Potential mechanisms include: GnRH-mediated increase in immune cell proliferation with increased cytokine, chemokine and endothelial growth factor production; GnRH-agonist-mediated rapid phasic changes in estrogen levels, with an increase followed by a decrease, similar to changes seen during pregnancy and postpartum, respectively; and discontinuation of MS disease-modifying treatments during fertility treatment.
Risk for MS in children
The risk for MS is about 2% for a child with one MS parent, 36 and MS has been observed in 6%–12% children when both parents had MS (conjugal MS).37,38 Counseling should emphasize that MS in a child is likely many years away, its course can be benign, and continuous progress in MS research includes development of more effective treatments.
Small differences in MS risk according to month of birth have been reported (higher in spring, lower in autumn 39 ) although the finding may be confounded by year and place of birth. 40 Lower vitamin D levels have been associated with a higher risk for MS, 41 and MS risk is lower among women born to mothers with high vitamin D intake during pregnancy. 42 Although safety of vitamin D supplementation in pregnancy is not established, supplementing vitamin D-deficient mothers might seem sensible, 42 but the dose given should achieve and not exceed a normal serum concentration (25-hydroxy vitamin D range 50–125 nmol/l). 43
Impact of pregnancy on MS disease course
Changes in circulating pregnancy hormones (estrogen, progesterone, prolactin and others) have effects on immune responses that underlie MS pathology. 44 The number of acute MS relapses is approximately halved during pregnancy, especially in the third trimester, and approximately doubled during the three months postpartum. 45 Pregnancy probably has no impact on long-term course or the likelihood of secondary progressive MS.46,47 Pregnancy and childbirth have even been associated with less long-term disability, 48 although interpretation of studies may be confounded by reverse causality when having MS affects reproductive decision making. Overall, the impact of pregnancy on MS course is not usually a concern when considering family planning.
Disease monitoring during pregnancy
While deleterious effects of MRI during pregnancy are not reported, its safety is not established sufficiently to support unrestricted use during pregnancy, with concern about the potential risk of heating effects from radiofrequency pulses, including teratogenicity, and effects of acoustic noise on the fetus. 49 It has been recommended to postpone elective MRI until after the first trimester, but MRI may be used at any time when potential clinical benefits clearly outweigh uncertain risks. Unlike radiography—including computed tomography (CT)—MRI avoids radiation exposure. 50 Intravenous gadolinium-contrast agents should be used with extreme caution during pregnancy. 50 Lumbar puncture or electrophysiological tests are not associated with specific risks to mother or fetus but should be used minimally as they may cause discomfort in a pregnant woman.
Treatment before conception and during pregnancy
Pharmacological treatments for MS should be avoided where possible during pregnancy. This normally means discontinuing existing disease-modifying and symptomatic treatments when planning conception and during pregnancy, unless the balance of benefit and risk favors continuing a treatment.51,52
Management of relapses
A short course of high-dose corticosteroids to hasten recovery from relapses appears relatively safe during pregnancy, but generally should be limited to disabling relapses, and there is a possible increased risk of fetal cleft palate associated with corticosteroid treatment in the first trimester. 53
Disease-modifying treatments
Reported experience of ß-interferon during pregnancy amounts to almost 1000 cases, most treated only during early weeks of the first trimester as treatment was discontinued when pregnancy was detected.54–58 While two small studies of MS patients who became pregnant while being treated with ß-interferon-1a 59 and ß-interferon-1b 54 reported a higher than expected frequency of spontaneous abortions, no increase in spontaneous abortions was observed in subsequent reports of larger cohorts who were being treated with ß-interferon-1a. There was a low incidence of fetal abnormalities with no consistent pattern for any syndrome, though data are insufficient to exclude an association with rare fetal abnormalities.55,56 ß-interferon treatment has been associated with premature delivery and reduced birth weight.55,60 ß-interferon should not be started during pregnancy, and in women already receiving treatment it is standard practice to discontinue it to avoid pharmacological effects 61 prior to a planned conception. Some physicians may elect to continue treatment until pregnancy is confirmed if they feel it essential to avoid any delay between treatment discontinuation and becoming pregnant.
Pregnancy outcomes have been reported in about 400 glatiramer acetate-treated patients and no increase in fetal abnormality noted.54,57,62,63 Although some physicians use glatiramer acetate during pregnancy when they feel its potential benefits outweighs risks, caution is advised as the reported numbers treated are not sufficient to exclude an uncommon fetal abnormality.
There is less or little information on pregnancy experience and fetal outcome with other disease-modifying treatments including natalizumab,64,65 fingolimod, 66 dimethylfumarate 67 and alemtuzumab. Natalizumab shows increased abortions in animal studies, 68 while none so far has been detected in MS. Conception should be avoided until fingolimod is eliminated from the body, about two months after treatment discontinuation. 69 Teriflunomide has teratogenic effects in animals and must not be given during pregnancy; 70 it has a long plasma half-life, and cholestyramine is routinely used to eliminate it whenever treatment is discontinued, for instance prior to conception and pregnancy.51,70 Mitoxantrone may cause amenorrhea (especially age >35 years 71 ) and should be avoided during pregnancy because of potential for teratogenicity. 52
In patients with previous highly active relapsing–remitting MS, cessation of disease-modifying treatment prior to conception may be associated with an increased relapse risk. 72 While it may be thought desirable to continue disease-modifying treatment in such patients, the potential for adverse effects on the fetus cannot be excluded, especially with newer, more potent treatments. In patients with highly active MS given natalizumab in the third trimester because of relapses, mild to moderate hematological abnormalities including thrombocytopenia and hemolytic anemia were seen in eight of nine newborns (K Hellwig, personal communication 2013).
There is little information regarding effects of MS disease-modifying treatments on human male fertility or pregnancy outcomes in fathers receiving treatment. 60 One study compared the outcome of pregnancies where fathers were treated (mainly with glatiramer acetate or ß-interferon) with outcomes from maternal MS cohorts with and without disease-modifying treatment and did not identify safety concerns for the offspring of the treated fathers. 73 Although some men discontinue glatiramer acetate or ß-interferon prior to conception, there is limited rationale for this approach. Teriflunomide is detected in semen and should be discontinued with cholestyramine washout in potential fathers. 70
Symptomatic treatments
There is little information on most MS symptomatic therapies from which to provide evidence-based advice for use during pregnancy, apart from anticonvulsants. 74 Frequently used MS symptomatic agents (e.g. baclofen, 75 oxybutynin, 76 amantadine 77 and clonazepam 78 ) carry United States Food and Drug Administration (FDA) class B, C or D risks. 79 A standard approach is to discontinue symptomatic therapies prior to conception, with an understanding of the potential functional impact; if continued, minimal effective doses should be used for the shortest time possible.
Delivery and post-pregnancy
Delivery and neonatal outcomes
Although not all reports concur, 80 there are probably no significant differences in gestational age, birth weight, length of birth hospitalization, and frequency of assisted vaginal delivery or cesarean section between women with MS and the general population.81–83 A trend for more frequent labor induction in women with greater disability warrants further investigation. 82 Neither epidural anesthesia84,85 nor cesarean section 85 has been associated with adverse effects on delivery or postpartum MS course.
Postpartum relapses
Disease-modifying therapies may be restarted soon after birth to potentially mitigate postpartum relapses. Poorly controlled clinical studies have suggested that monthly intravenous methylprednisolone 86 or immunoglobulin87,88 may reduce postpartum relapses, but controlled studies are needed to confirm these effects.
Breastfeeding
Studies of the postpartum MS course42,89,90 suggest no effect or a possible decrease in relapse rate associated with breastfeeding. Exclusive breastfeeding may be protective, although there have been only limited studies.57,90 Because MS disease-modifying treatments may enter breast milk, they are normally withheld during breastfeeding. The decision whether to resume a disease-modifying treatment immediately after birth needs to be weighed against the potential benefits of breastfeeding. When patients receive high-dose methylprednisolone, brief suspension of breastfeeding for 24–48 hours has been recommended. 52
Clinical trials of sex hormone therapies
A baseline cross-over trial of oral estriol in 10 women with relapsing–remitting MS showed an 80% decrease in gadolinium-enhancing lesions, a favorable Th1 to Th2 immune shift in peripheral blood mononuclear cells (PBMCs), and improved cognition. 91 A baseline crossover trial of transdermal testosterone in 10 men with relapsing–remitting MS showed no change in gadolinium-enhancing lesion frequency, but reduced brain atrophy and increased production of neurotropic factors by PBMCs.3,92 These studies imply beneficial immunomodulatory and neuroprotective effects of estrogen in women and testosterone in men, respectively.
The effect of oral contraceptives (OCs) on MRI lesion activity was investigated in 149 women treated with subcutaneous ß-interferon 1a and randomized to receive ß-interferon 1a only, or ß-interferon 1a plus ethinylestradiol 20 mcg and desogestrel 150 mcg (low-dose estrogen group), or ethinylestradiol 40 mcg and desogestrel 125 mcg (high-dose estrogen group). 93 There were significantly fewer new lesions over two years in the high-dose estrogen group. Estrogen-containing OCs probably do not worsen MS disease course 94 and high-dose estrogen OCs may enhance the effect of ß-interferon in preventing new lesions in relapsing–remitting MS.
The Post Partum Progestin and Estriol in Multiple Sclerosis (POPARTMUS) trial investigated 12 weeks’ treatment with 10 mg nomegestrol acetate versus placebo 95 and found no difference in postpartum relapse rate between study arms (C Confavreux, personal communication 2013).
Menopause
Any effects of menopausal hormone changes per se may be confounded by age-related changes in MS disease activity and comorbidities. Observations of patients who developed MS aged >50 years suggested a similar rate of disease progression in both sexes, while men progressed more rapidly when disease started between 18 and 49 years. 96 This highlights potentially complex contributions of age and sex together with genetic and environmental factors in such studies.
Recommendations for managing reproduction-related issues in MS
Counseling the mother and father is important before, during and following pregnancy. Helping a family to assess parenting abilities (physical, financial, emotional), and to understand short- and long-term consequences of pregnancy on MS in the mother and risks of MS in offspring, can guide realistic expectations of pregnancy outcomes (Table 1). Management issues for the prospective MS parents include fertility and conception; impact of pregnancy on MS course; implications for disease-modifying and symptomatic therapies; obstetric management and delivery; and breastfeeding (Table 2). Physicians should be aware of regulatory guidance regarding pharmacological treatments during pregnancy and the principle that medications will normally be avoided unless their benefits are considered to outweigh risks.
Elements to be considered in counseling the patient/family at different stages of the reproductive “cycle” in MS.
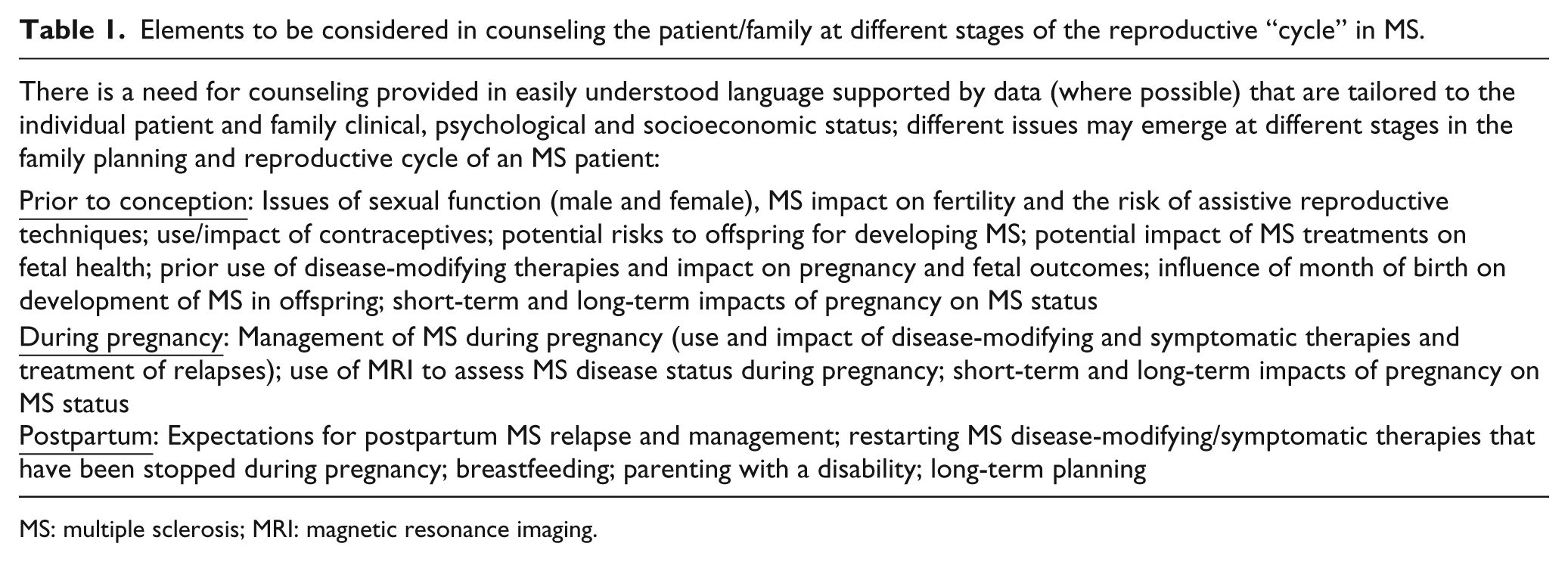
MS: multiple sclerosis; MRI: magnetic resonance imaging.
Recommendations related to management of MS around pregnancy.

MS: multiple sclerosis; MRI: magnetic resonance imaging; CT: computed tomography; IV: intravenous; FDA: United States Food and Drug Administration.
Future directions (Table 3)
The reasons underlying apparent changes of MS prevalence in women remain speculative. Future case-control studies to elucidate their cause(s) could yield major clinical insights and lead to new health care strategies for the prevention and treatment of MS.
Future directions.
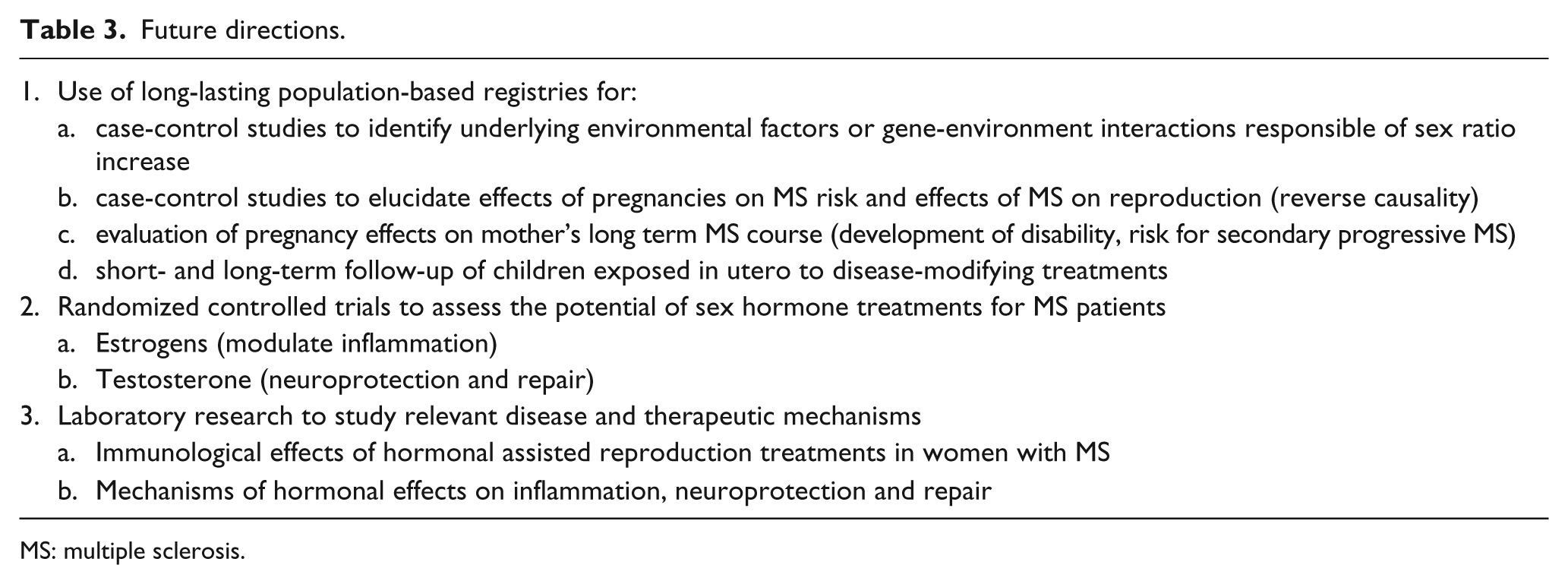
MS: multiple sclerosis.
Numerous studies have investigated effects of pregnancy on risk of MS or a first clinical or radiological demyelinating event,26–29,97 outcomes of pregnancy for the mother and child,82,83 and effects of drug exposure during pregnancy on the child,55,56,60,63 but results are not always consistent and sometimes conflicting. Different study findings may reflect small sample sizes; heterogeneous methodologies and populations; and confounding factors such as co-morbidities, co-treatments, family history and maternal age. Using population-based registries with linkages to independent national databases, future studies should address the impact of pregnancy and MS therapies during pregnancy on long-term outcomes for mother and child. A challenge for all MS registry initiatives is to combine datasets to generate large international cohorts, with shared demographic and clinical information.98,99
Hormonal treatment trials with definitive clinical endpoints are warranted. A placebo-controlled trial of estrogen as add-on therapy to glatiramer acetate in women with relapsing–remitting MS is in progress. 100 Further laboratory investigation to elucidate mechanisms of potential beneficial (estrogens and testosterone) and adverse (gonadotropins) hormonal effects is needed.
Footnotes
Acknowledgements
We thank all meeting participants for their active participation and contributions to the workshop and the review of this manuscript. Meeting attendees: MP Amato (Florence, IT); R Bove (Brookline, MA, USA); H Butzkeueven (Melbourne, AU); T Chitnis (Brookline, MA, USA); O Ciccarelli (London, UK); M Clanet (Toulouse, FR); C Confavreux (Lyon, FR); R Dobson (London, UK); M d’Hooghe (Melsbroek, BE); Y Dadalti Fragoso (São Paolo, BR); E Havrdova (Prague, CZ); K Hellwig (Bochem, DE); M Hutchinson (Dublin, IE); L Kappos (Basel, CH); A Langer-Gould (Pasadena, CA, USA); C Lebrun-Frénay (Nice, FR); MI Leite (Oxford, UK); C Lubetzki (Paris, FR); D Mason (Christchurch, NZ); P McCombe (Herston, QLD, AU); A Miller (New York, NY, USA); D Miller (London, UK); X Montalban (Barcelona, ES); H Offner (Portland, OR, USA); T Olsson (Stockholm, SE); C Pozzilli (Rome, IT); S Reingold (Salisbury, CT, USA); D Sadovnick (Vancouver, BC, CA); M Sandberg-Wollheim (Lund, SE); F Sellebjerg (Copenhagen, DK); P. Soelberg-Sorensen (Copenhagen, DK); S Tenembaum (Buenos Aires, AR); M Tintoré (Barcelona, ES); H Tremlett (Vancouver, BC, CA); M Trojano (Bari, IT); R Voskuhl (Los Angeles, CA, USA); E Waubant (San Francisco, CA, USA); D Williams (London, UK).
Conflict of interest
DHM has received honoraria through payments to his employer, UCL Institute of Neurology, for Advisory Committee and/or Consultancy advice in multiple sclerosis studies from Biogen Idec, GlaxoSmithKline, Novartis, Merck, Chugai, Mitsubishi Pharma Europe and Bayer Schering Pharma, and has also received grants through payments to his employer for performing central MRI analysis of multiple sclerosis trials from GlaxoSmithKline, Biogen Idec, Novartis and Merck. The Queen Square MS Centre at UCL Institute of Neurology is supported by the UK MS Society and UCL-UCLH Biomedical Research Centre.
FF serves on scientific advisory boards for Bayer-Schering, Biogen Idec, Genzyme, Merck Serono, Perceptive Informatics, Pfizer, Novartis and Teva Pharmaceutical Industries Ltd and has received speaker honoraria and support from Biogen Idec, Bayer Schering, Merck Serono, Novartis, Sanofi-Aventis and Teva Pharmaceutical Industries Ltd.
XM has received speaking honoraria and travel expense reimbursement for participation in scientific meetings, has been a steering committee member of clinical trials or participated in advisory boards of clinical trials in the past years with Bayer, Biogen Idec, Merck, Genentech, Genzyme, Novartis, Sanofi-Aventis, Teva Pharmaceuticals and Almirall.
SCR has served as a consultant to the National Multiple Sclerosis Society (USA) and the European Committee for Treatment and Research in MS; and has received honoraria and travel reimbursement for service on Data Safety Monitoring Boards or Advisory Boards for Bayer HealthCare, Coronado Biosciences Inc, Eli Lilly & Company, EMD Merck Serono, Genentech, F. Hoffmann-LaRoche, Ironwood Pharmaceuticals Inc, ISIS Pharmaecuticals Inc, MedImmune Inc, Novartis Pharmaceuticals Corporation, Observatoire Français de la Sclérosis en Plaques, Opexa Therapeutics, Sanofi-Aventis, SK Biopharmaceuticals, Synthon Pharmaceuticals Inc, and Teva Pharmaceutical Industries; and served as an editorial board member of the Multiple Sclerosis Journal.
MT has served on scientific Advisory Boards for Biogen Idec, Novartis, Roche and Merck Serono; has received speaker honoraria from Biogen-Idec, Bayer-Schering, Sanofi Aventis, Merck-Serono, Teva and Novartis; has received research grants from Biogen-Idec, Merck-Serono, and Novartis.
Funding
The Focused Workshop on Pregnancy, Gender and Hormonal Factors in Multiple Sclerosis (held in London, UK, March 6–8, 2013) was supported in its entirety by the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).