
Abstract
The media is a significant source of information about mental health and can considerably influence public attitudes. Elite sportspeople are role models for young people and prominent figures in Australian culture. However, little is known about journalists’ attitudes, experiences, and training needs for reporting on mental ill-health and suicide in high-profile athletes and coaches. An invitation email for a cross-sectional online survey was sent directly to journalists. The survey included demographic characteristics, and measures assessing their knowledge and attitudes towards mental health and suicide, and views, experiences and training needs for reporting on mental ill-health and suicide in sportspeople. Inductive qualitative content analysis of the written responses was conducted, and mean scores and percentages were calculated for the quantitative measures. A total of 81 Australian journalists (43 identified as women; 38 identified as men) aged 22–76 years (M = 22.0, SD = 13.8) participated in the study. Participants had diverse opinions on the media's responsibility when reporting mental health and suicide in elite sportspeople, with some believing they had an important role in reducing stigma. Notably, almost half of the participants had never received training on how to report on mental ill-health and suicide. Given that there are no current guidelines for reporting on these issues for sportspeople, further training resources are likely to be beneficial. However, training format, content and delivery may need to be shaped around journalists’ preferences and information needs, including delivery by experts such as those with lived experience, researchers, and practitioners.
Introduction
More than one in five Australians will experience mental ill-health in any 12-month period, and in a single year, 16.7% of Australians aged 16–85 years reported experiencing thoughts of suicide, and 38.0% had ever been close to someone who had attempted suicide or had taken their own life (Australian Bureau of Statistics, 2022). However, Australian studies indicate that less than half of those experiencing diagnosed mental ill-health or suicidal thoughts will seek help (Australian Bureau of Statistics, 2022; Bismark et al., 2022). Delays in help-seeking frequently lead to poorer outcomes for both mental health and functioning (Thornicroft, 2012). Whilst many factors impact help-seeking, including structural factors such as availability and accessibility of appropriate services, perceived stigmatising attitudes towards mental ill-health and suicide remain a significant barrier to help-seeking in the general community (Mok et al., 2020). Stigma can lead to those with mental ill-health experiencing feelings of hopelessness and lowered self-esteem (Moses, 2010). People already in treatment for mental ill-health also report reluctance to disclose suicidal thoughts to health practitioners (McGillivray et al., 2022), and those bereaved by suicide experience significant perceptions of shame and reduced help-seeking for themselves (Pitman et al., 2016). Thus, reducing stigma is critical to improving mental well-being across the population. To achieve this, significant cultural shifts may be needed in the public's understanding of mental ill-health and suicide (Pescosolido et al., 2021), to which journalism can contribute.
Elite sportspeople, including athletes and coaches, are significant public figures globally and in the Australian community (Yancey et al., 2011). A study of young women in 2008–2010 from secondary schools in Victoria, Australia, noted that the majority cited elite sportswomen as their role models (Young et al., 2015). Media coverage of the 2023 Women's Football World Cup generated significant public discourse about the Australian national team, the Matildas, acting as ‘powerful and inspiring’ community leaders and role models for young Australians (e.g. McCubbing, 2023; Rachwani, 2023). Elite sportspeople also impact both attitudes and behaviour more broadly in the community, with influence on social justice and climate change-related behaviours (Edgar, 2021), pracitising good hygiene during COVID-19 (Leng and Phua, 2022), and increasing participation in sports and physical activity (Kelly et al., 2024). Elite sport is a major industry in Australia (Shilbury and Rowe, 2017), and achievement in sport, particularly relative to population size, is a large part of the national identity (Morgan and Taylor, 2017). This strong focus also translates to community impacts. For example, the success of Australian elite athletes overseas, such as during the Olympics, generates economically measurable increases in societal well-being (Frontier Economics, 2009).
Elite athletes have been found to experience broadly similar levels of mental ill-health to the general community (Gorczynski et al., 2017; Gouttebarge et al., 2019). Like other ‘high profile people’ such as celebrities, the status of elite sportspeople generates high public interest and newsworthiness (Ross et al., 2024), leading to high levels of scrutiny when discussing their mental health. Athletes may face increased barriers to help-seeking compared to the general population due to this public scrutiny, as well as sporting culture and competitiveness, with concerns that their disclosure could result in negative reactions or consequences such as a loss of selection (Gulliver et al., 2012; Purcell et al., 2019). Thus, in this context, when elite sportspeople talk about their own experiences of mental ill-health publicly, it may be particularly powerful for reducing stigma in the community (Walton et al., 2019). Studies from the USA, where sports role models are prominent, highlight the importance of positive media framing of disclosure of mental ill-health in sportspeople, in reducing stigma, promoting awareness, and ultimately increasing help-seeking behaviour in communities (Parrott et al., 2019). Research from Australia also indicates that hearing about athletes managing mental ill-health is likely to contribute to self-acceptance and normalisation of mental ill-health, potentially encouraging help-seeking behaviour (Walton et al., 2019). Since the COVID-19 pandemic raised awareness of mental ill-health, greater numbers of athletes have spoken out on this issue (Mack et al., 2023). Cultural change around how mental health is viewed is also beginning to occur within sports organisations, with elite sports expected to establish a culture where mental health is seen as just as important as physical health for optimal performance (Mack et al., 2023; Purcell et al., 2019).
Journalism remains a significant source of information about both mental ill-health and suicide, and can considerably influence public attitudes (Corrigan et al., 2013) and behaviour (Pirkis et al., 2019). There are now clear standards on coverage of suicide by the Australian Press Council (Australian Press Council, 2025), the Dart Centre (2020), and guidelines on reporting about mental health and suicide by the mental health organisation ‘Mindframe’ (Everymind, 2020). The Media Entertainment & Arts Alliance (2025) code of ethics also links with elements related to suicide and mental health, such as the standard of ‘Respect private grief and personal privacy. Journalists have the right to resist compulsion to intrude’, even though it does not mention them explicitly. The Mindframe guidelines introduced in 2002 have had a measurable impact, particularly on the reporting of suicide in Australian media (Pirkis et al., 2022). Although these guidelines do not specifically mention elite sportspeople, they do outline briefly how to report on ‘celebrity’ mental illness and suicide. The impact of these guidelines is noticeable when examining Australian online news articles about suicide in elite sportspeople. To inform the background to our study, author KG appraised a selected sample of n = 22 elite athletes and coaches (across ∼100 articles; noting this search was not intended to be comprehensive), who had taken their own lives since these guidelines were introduced. In general, news articles during this time appeared to be framed sensitively towards the person and their family, focusing primarily on the athlete's positive qualities, their achievements, and the effect of their death on those close to them. Typically, more recent articles avoided reporting methods and included links to crisis support services as per guidelines. However, contrary to current advice (Everymind, 2020; Wake et al., 2020), many articles included reasons as to why it was thought the athlete took their own life, often quoting family or friends. Suggestions included challenges with an injury or retirement, unfair conditions, isolation, personal ‘battles’ or ‘demons’, or conversely, expressing complete shock that there were no indicators or obvious ‘reasons.’ Similarly, journalists rarely used stigmatising language themselves. However, on several occasions, they would include direct quotes by family members or friends that perpetuated stigma, such as saying the person ‘committed suicide’ or implying that it was better that the suicide could be explained in the context of a ‘real’ medical reason such as Chronic Traumatic Encephalopathy (CTE), rather than in the context of a mental health issue such as depression. Following this, recent research (Ross et al., 2024) has found that journalists have identified a tension between adhering to guidelines and telling the bereaved person's story ‘in their own words’ even when it contravenes those guidelines and may contribute to stigma or harm. Balancing these reporting challenges remains complex; Ross et al. (2024) suggests further resources should be developed to assist specifically around the telling stories of the lived experience of suicide or mental ill-health. In addition, reporting resources for elite athletes and coaches may require specific advice regarding issues unique to sport, such as CTE.
Despite the existence of available guidelines, language used in media reporting remains stigmatising at times. Newsroom culture (Ross et al., 2022) and production factors such as sensationalist headlines, driven by fast news cycles and advertising revenue streams (Nelson et al., 2024) are thought to influence how stories are framed (Ross et al., 2024). As noted above, stigmatising language continues to be observed when reporters discuss mental health and suicide in elite sportspeople (Zakrajsek et al., 2023). Their critical role in public information provision may reinforce stigmatising attitudes, elicit feelings of shame, and discourage help-seeking in the community (Sampson et al., 2024). Thus, whilst media guidelines have assisted in improving the quality of news portrayals of mental ill-health and suicide, additional training, preparation and support for journalists is likely to be beneficial (Ross et al., 2024), with potential for tailored information on stories focusing on sportspeople. Further, little is known about the level of mental health literacy and stigma in journalists, with few studies conducted in Australia and only one in journalism students (Burns et al., 2022).
Aim
The current study aimed to investigate Australian journalists’ attitudes towards and knowledge of mental health and suicide, and their experiences reporting on mental ill-health and suicide in sportspeople. We had no formal hypotheses as the study was primarily exploratory.
Methods
Study design
The study design was a cross-sectional online survey using qualitative and quantitative questions conducted on the Qualtrics platform.
Participants and recruitment
Participants were recruited via an invitation sent directly via email in November 2023. We initially recruited via a paid market research panel; however, these data were not included due to data integrity concerns detected, such as AI or bot-generated, brief nonsensical responses, and several participants noted in free-text responses that they were ‘not journalists’ despite agreeing to the listed inclusion criteria on the information and consent webpage. Our other planned recruitment method was snowball sampling and distribution via media organisations, whereby contacts within organisations would be asked to distribute the email to journalists who may be interested in participating; however, this was also unsuccessful as none were able to distribute the invitation (e.g. to avoid sending too many surveys to their mailing lists). With an amendment to our ethics approval, our final recruitment method involved direct email invitations to potential participants, via an email list generated in a recent previous study in 2022 by author PE, from publicly available media guides (e.g. Information Australia-Margaret Gee Media Group, 2021) and available online resources, such as bylines on news websites. A total of 5991 emails were sent; approximately one-quarter of these bounced (e.g. server rejection, inactive email address) or were not received (e.g. lengthy out-of-office or ‘no longer at this address’ automatic replies), leaving a total of 4408 emails delivered. Each email address was sent an invitation twice.
Inclusion criteria were that participants were currently working as a journalist, living in Australia, aged 18 years or older, and able to read and write in English. Potential participants were required to read a description of the study and provide informed consent by checking a box on the survey page marked ‘yes’ to indicate they had read and understood the information provided, were eligible, and agreed to participate.
Debriefing
After completing the survey, participants were provided with further information on the study aims, plus websites and phone numbers for further information and mental health support. They were also invited to indicate their interest in receiving an email invitation to participate in the next phase of the study, which was to co-design a brief module on how mental ill-health in sportspeople should be discussed in the media. Those interested provided their contact email address in a separate survey that was not linked to their responses.
Survey measures
Demographic information
We collected participants’ gender (man, woman, different term, prefer not to say), age (in years), language spoken at home (English only, English and another language, or another language only) State/Territory, region/area of residence, level of education, employment status (full-time, part-time, casual), primarily employed as journalist type [news, feature, investigative, opinion/column/analysis, data, other (open-ended)], journalist subject [political, crime, business, arts and culture, celebrity, education, sport, lifestyle, fashion, science, travel, environment, other (open-ended)] and journalist field/medium [print, television, radio, online, news agency, social media, other (open-ended)]. We also asked whether they identified as living with mental ill-health, or as a carer/kinship group member of someone with mental ill-health.
Attitudes, knowledge, and stigma
Help-seeking attitudes. Help-seeking attitudes were measured using the 10-item short form of the Attitudes Towards Seeking Professional Psychological Help scale [ATSPPH-SF (Fischer and Farina, 1995)]. Participants were asked to rate their view on statements about psychological treatment using a 4-point scale (Disagree = 0, Agree = 3). Higher scores indicate more positive attitudes towards seeking professional help (range = 0–30). We used a version (Calear et al., 2014) with updated wording, i.e. ‘mental breakdown’ was altered to ‘personal or emotional problems’. The scale has previously shown sound psychometric properties (Calear et al., 2014; Elhai et al., 2008; Fischer and Farina, 1995), and Cronbach's alpha (α) in the current study was 0.86.
Stigma. The 5-item Social Distance Scale [SDS; (Link et al., 1999)] was used to measure stigmatising attitudes towards those experiencing mental ill-health, defined for this scale as ‘mental illness’. Items ask the willingness of participants to act in different scenarios (definitely willing = 1 to definitely not willing = 4), e.g. ‘Spend an evening socialising with a person with mental illness.’ Higher mean scores (1–4) indicate higher stigma and attitudinal social distance. A previous study using this scale demonstrated good internal consistency (α = 0.94) (Busby Grant et al., 2024), which was similar (α = 0.92) in the current study.
We used the 9-item Depression Stigma Scale [DSS (Griffiths et al., 2006)] to measure stigmatising attitudes towards depression. Participants were presented with statements about depression, e.g. ‘People with depression could snap out of it if they wanted’, and asked to indicate their level of agreement on a 5-point scale (strongly disagree = 0, strongly agree = 4). Summed scores range from 0–36, with higher scores indicating greater personal stigma about depression. The DSS has demonstrated good internal consistency and validity (Griffiths et al., 2006), with the current study α = 0.86.
To assess stigmatising attitudes towards suicide, we used the 8-item Stigma of Suicide Scale (SOSS) (Batterham et al., 2013b). Participants were asked to rate their agreement with brief descriptors of a person who dies by suicide, such as ‘cowardly’ or ‘an embarrassment’, on a scale of strongly disagree = 1 to strongly agree = 5. Scores are summed (range = 8–40) with higher scores indicating higher stigma towards suicide. Cronbach's alpha was 0.92 in the current study.
Mental health literacy. We used the short forms of the Depression Literacy Questionnaire (D-Lit; 11 items (Griffiths et al., 2004)) and the Literacy of Suicide Scale [LOSS; 12 items (Calear et al., 2022)]. The scales assessed the participants’ knowledge about depression and suicide, respectively, by asking participants to rate what they believed to be the correct response to various statements with options of ‘true’, ‘false’ or ‘don’t know.’ Participants were scored 1 point for each correct answer, with higher scores indicating higher literacy for depression (D-Lit; range 0–11) or suicide (LOSS; range 0–12). Example statements include ‘Reckless and foolhardy behaviour is a common sign of depression’ (false; D-Lit) and ‘People who want to attempt suicide can change their mind quickly’ (true; LOSS). Citing internal consistency is not always appropriate for knowledge scales, as it is typically desirable that responses to items vary (Taber, 2018).
Beliefs and experience. Quantitative questions included whether participants thought that athletes were more likely, less likely, or equally likely to 1) experience mental ill-health or 2) suicide, compared to the general population (range 1–5, where 1 = much less likely, 3 = equally likely, 5 = much more likely). We also asked if they had ever had to write an article about an athlete experiencing mental ill-health or who had suicided, and if they had ever received any training on how to report on mental health and suicide, and if yes, what it comprised.
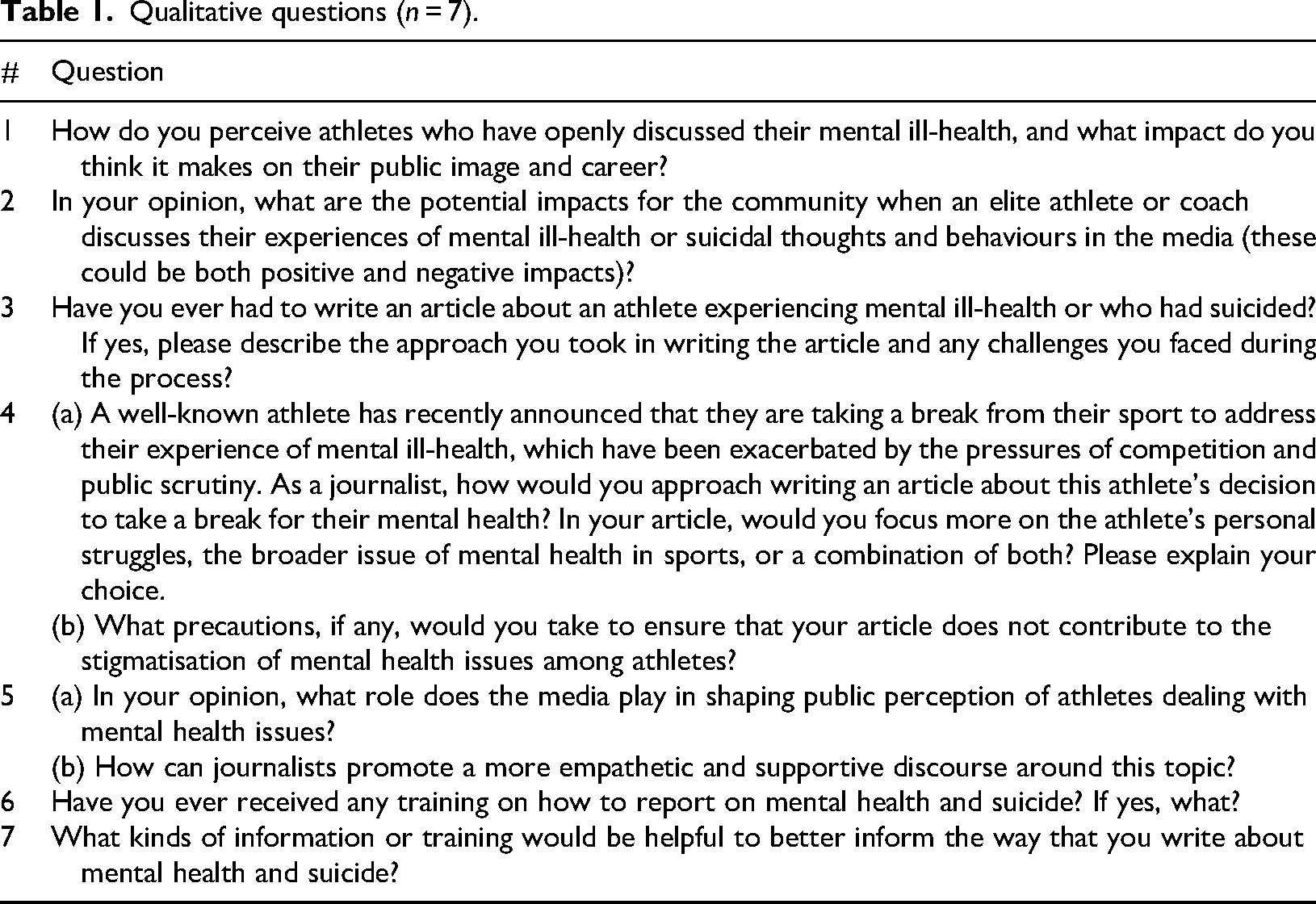
Athletes, mental health, and journalism impacts. Table 1 displays the seven open-ended questions we asked to gather qualitative data for the current study. These questions broadly addressed journalists’ views of athletes who have discussed their mental ill-health or suicidal thoughts and behaviours, the impacts on both athletes and the community, and their views on how journalism should approach these issues. Questions also explored whether they had received training and what would be helpful for them in informing how they approach these pieces in the future.
Qualitative questions (n = 7).
Data analysis
Mean scores were calculated using SPSS 29.0 for Windows (IBM Corp) for help-seeking attitudes, stigma, literacy, and beliefs measures and participant age, and percentages were calculated for demographic information and the experience questions. Eight exploratory regression analyses were conducted with the demographic variables of age, years employed as a journalist; type of journalist employed [news vs other (feature, opinion/column/analysis, investigative, other)]; gender (man vs woman) and location (metropolitan vs regional/rural/remote) to investigate any potential impact on the each of the eight different knowledge, attitudes, and belief scales.
For the qualitative data, we used a thematic analysis (Braun and Clarke, 2006) combining deductive and inductive codes. Author AG summarised participant responses under each question into codes (e.g. answers to question 6 on what training they had received was coded as (1) general training, (2) Mindframe, (3) guidelines, and (4) policy discussions, assigning meaning based on the author's interpretation of the quotes (Braun and Clarke, 2021). These codes were then combined responses across questions to form basic themes, e.g. the data under question 6, was recoded into Theme 3. Professionalism and accuracy. In the final step, the thematic structure was further developed across the questions in collaboration with author MB. Data were organised using NVivo 12 (QSR International).
Results
Eighty-one journalists (N = 4408; response rate = 1.8%) completed the survey and were included in the analysis. The quantitative and qualitative data are presented concurrently below. Quotes are identified by participant number and journalism field.
Table 2 presents the participant demographic characteristics. Almost half were in NSW, a quarter in Victoria, and the rest were from all other states and territories except the Northern Territory. More than half of the participants were news journalists, a large proportion working primarily in print journalism. Participants specialised in a wide variety of fields, with the most common being political, business, and lifestyle, and those who covered multiple fields (‘all-rounders’) or general news. Almost half had lived experience themselves or cared for someone with lived experience.
Demographic characteristics of participants (N = 81).
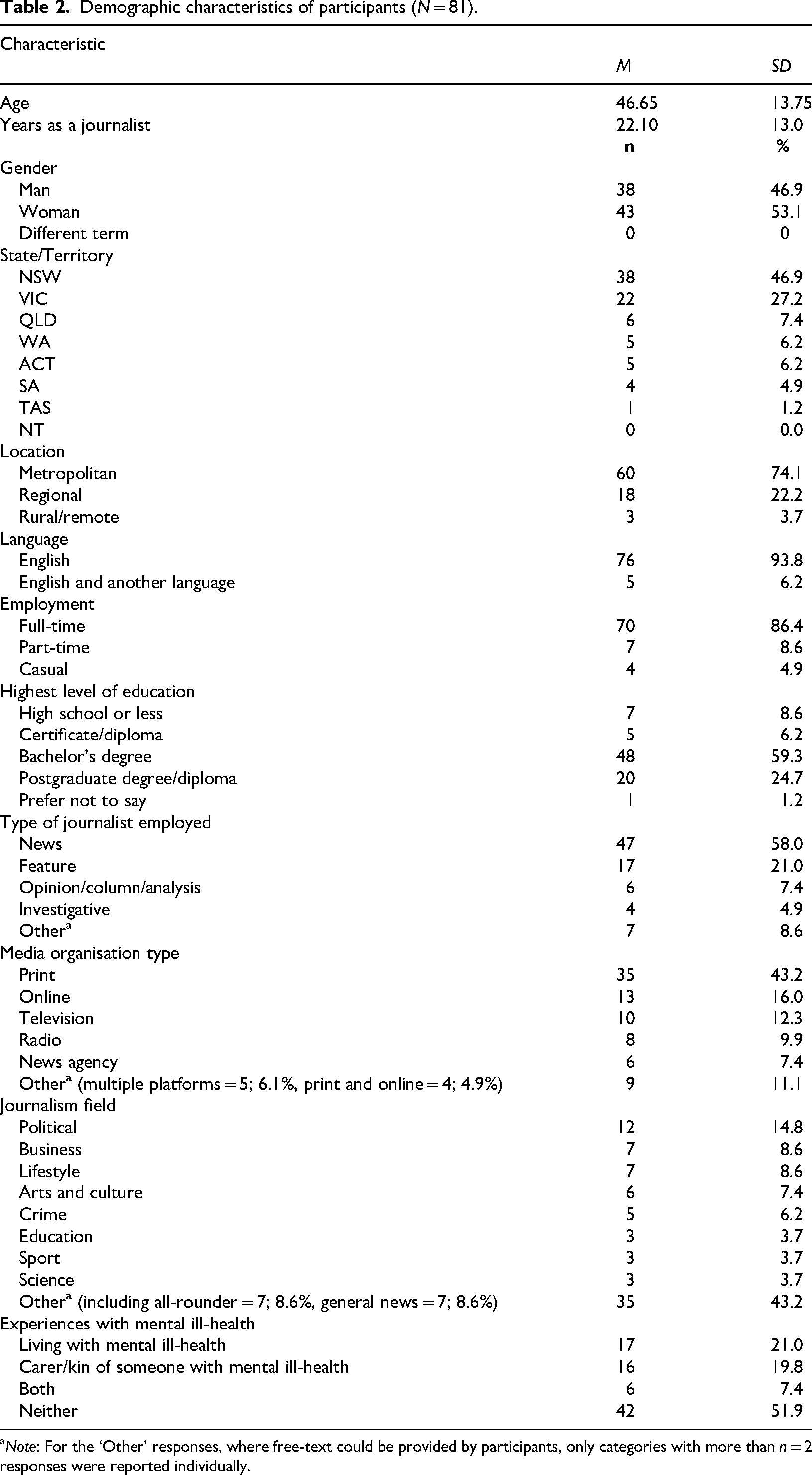
Note: For the ‘Other’ responses, where free-text could be provided by participants, only categories with more than n = 2 responses were reported individually.
Table 3 presents the results for mental health knowledge, attitudes, beliefs about athletes, and experiences of mental health training or writing about athletes. The only model out of the eight linear regressions conducted for the different knowledge, attitudes, and belief scales (see Table 3) that was significant overall was for depression literacy [R2 = .24, F(5, 75) = 4.76, P < .001], where being a woman (t = 2.91, P = .005) or a journalist employed outside of news reporting (e.g. feature, opinion/column/analysis, investigative, other; t = 2.78, P = .007) predicted higher depression literacy scores.
Knowledge, attitudes, beliefs, and experiences of participants (N = 81).
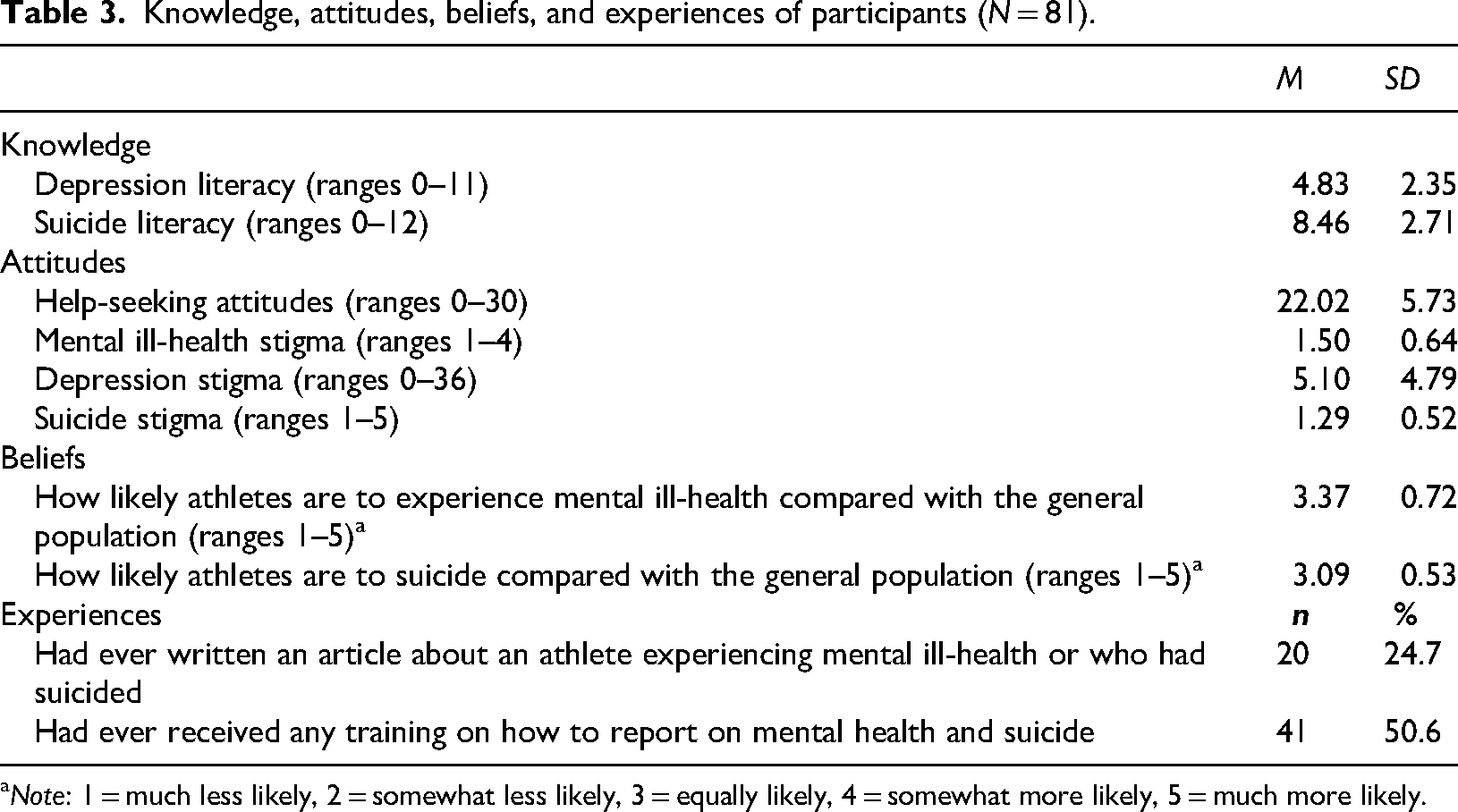
Note: 1 = much less likely, 2 = somewhat less likely, 3 = equally likely, 4 = somewhat more likely, 5 = much more likely.
In general, participants had moderate literacy scores, low stigmatising attitudes towards both depression and suicide, and low social distance scores. These scores were reflected in the qualitative comments, with many participants’ comments reflecting an awareness of the importance of the topic and understanding about the role the media plays in shaping public attitudes – ‘I think the media plays an enormous role in “normalising” mental ill health, and getting people to recognise that it is no different to physical ill-health’ (Participant 1, Court).
Views on how journalists can reduce stigma and promote empathy in reporting
Figure 1 presents three interrelated themes identified when discussing what precautions participants would take to avoid contributing to stigma and how they can create a more empathic discourse around mental health in the media. These themes, sensitivity and respect, professionalism and accuracy, and positive framing and avoiding stigmatisation are elaborated below.
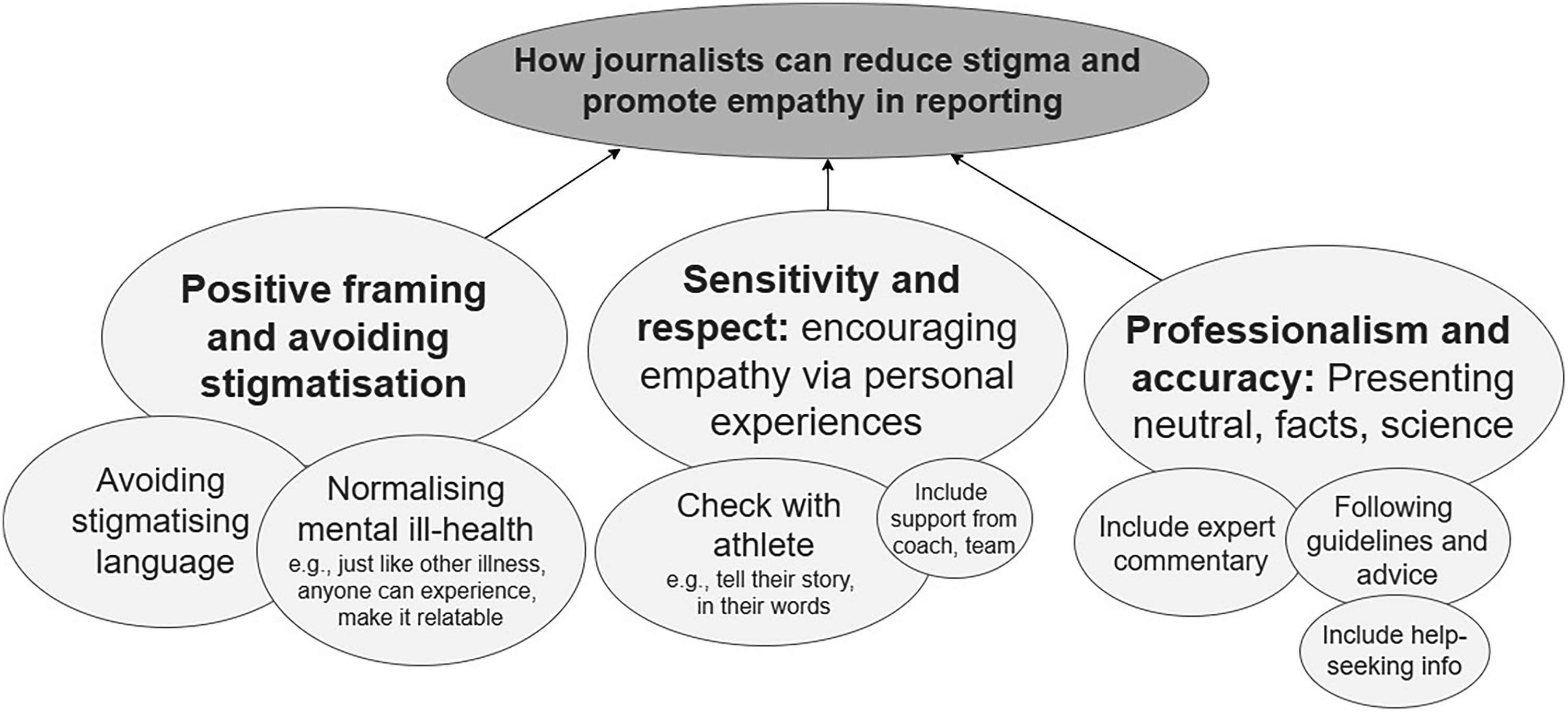
Thematic analysis of how journalists can reduce stigma and promote empathy around mental health when reporting on this topic.
Theme 1. Positive framing and avoiding stigmatisation
In general, participants believed that athletes experienced a relatively similar risk of mental ill-health (M = 3.37/5.00) and suicide (M = 3.09/5.00) compared to the general population. When asked specifically about how they perceived athletes who discussed their mental health in the media, many responses described how the journalists admired and believed they were ‘brave’ or ‘strong.’ Some noted the generational shifts in how mental health is discussed: ‘With each generation – and the improved education and support available to each generation – it feels like there's a more positive shift toward treating mental ill-health the same way we would treat physical ill-health or injury’ (Participant 1, Court). Most believed the impact on the athlete would be positive or neutral, some viewed it as negative, and others saw that it would depend on the group – ‘it will increase their standing in some people's eyes and diminish it in others’ (Participant 2, Business). Some responses also suggested that the athletes may be exposed to increased negative commentary online via social media – ‘The individual athletes may face an increase in online bullying’ (Participant 3, News).
Participants generally described that it was important to frame the reporting in what they felt was a ‘positive’ way that did not contribute to stigma in the community. Some examples include explaining the positive impact of athletes’ talking about prioritising their mental health and using this to ‘highlight the good example their choices set for others who may be experiencing similar’ (Participant 4, Political). Another remarked it may help when reporting on athletes’ mental health to ‘avoid framing their story around concepts of strength and weakness and use their stories about the issue to build a greater awareness’ (Participant 5, News).
In addition to the overall framing of their reporting, avoiding stigmatising language was specifically noted as important. Some identified simply being ‘careful’ with language, because ‘we use language that other people repeat, for better and worse’ (Participant 2, Business). Others noted ‘avoiding words that diminish or trivialise the problem’ (Participant 6, Arts and culture) or ensuring their language ‘accurately describes the person's condition. I would try not to use words that blame the person or show that they were weak for taking time for their mental health’ (Participant 7, Education). Several participants mentioned that they believed the current guidelines may be contributing to stigma, Suicides are basically covered up. This used to be the case with domestic violence. I wonder if one day we'll see the current approach as unhelpful. (Participant 8, All-rounder) I don't think dancing around it with ph[r]ases like “took their lives” or “ended their lives” or waiting until the third paragraph of a story to mention it is going to make any positive difference at all. In fact I think it stigmatises suicide even more by declaring it something we only speak about in hushed voices and euphemisms. Suicide is as devastating and real as someone's death from cancer or a car accident and I've spoken to people who think we need to stop treating it differently. But all the professional organisations tell us to do the exact opposite. (Participant 1, Court).
Participants also discussed ‘normalising’ mental ill-health by firstly helping to make elite sportspeople ‘relatable’ and demonstrating that their experience of mental ill-health is no different to those in other industries or the community – ‘Anything to explode the us and them syndrome. We are all vulnerable’ (Participant 9, Lifestyle). There was also the view that providing context around the aetiology of mental ill-health was important by ‘framing the story as a structural issue rather than an individual issue’ (Participant 10, Political). This theme was also about showing that mental ill-health was ‘a normal part of life, almost but not quite the same as if the athlete has a physical injury or is taking time out due to family issues. No one questions those decisions’ (Participant 11, News). Another participant remarked, ‘the more it's spoken about and normalised, the more people can see that mental health issues are okay and just something to be treated by a professional’ (Participant 12, Science).
When asked about the impacts on the community of sportspeople discussing their mental health publicly, many journalists believed it would be very likely to have positive impacts, through role modelling and reducing stigma of mental health and help-seeking – ‘I think it's a courageous thing to do, helpful for those experiencing mental illness, and contributes to a better understanding of mental health problems in the general public’ (Participant 13, Lifestyle). Some also noted that speaking out specifically helped by making sportspeople ‘relatable to other people or show that anybody can be affected by mental ill-health at times in their lives, even when they are performing at an elite level’ (Participant 7, Education), and was particularly important for some groups: ‘I think it's courageous and important as they have such influence, particularly on young men who we know don’t talk enough about their struggles’ (Participant 14, Education).
Some responses advised it was important to be cautious in the reporting, stating ‘it does depend on how it's discussed. Anything discussing the means of suicide is obviously dangerous or anything appearing to glorify suicide’ (Participant 14, Education). Potential positive impacts also relied on the role-modelling available within the story itself, for example, ‘if the athlete or coach are unable to improve their health and are critical of good treatments, this may discourage others from seeking treatment’ (Participant 15, Arts and culture).
Theme 2. Sensitivity and respect
Nearly one-quarter of participants reported having written an article about an athlete experiencing mental ill-health or who had suicided. For those who had, many noted how careful they were. Firstly, aiming to represent the person's story accurately – ‘I let them tell their story in their own words. It's their experience to share’ (Participant 16, Political). Secondly, when reporting on suicide, they were careful to provide supportive resources and explicitly follow guidelines, which links with the theme of professionalism and accuracy below: ‘We never referenced the word suicide or detailed the manner of death. We tried to focus on preventative measures that were ignored’ (Participant 17, Sport).
Participants used many ways to describe the importance of treating the topic of mental health and suicide with ‘sensitivity’ and ‘respect’. Some simply noted that the use of ‘sensible sympathetic reporting’ and using ‘sensitive photos and headlines’ was important. Others described how they would achieve this: ‘If you provide an insight into the effect that living with a condition can have on a person's life, people will naturally sympathise if the story is told with empathy’ (Participant 5, News). One participant noted that this sensitivity should extend to prior to the reporting phase – ‘It should approach the topic in a sensitive and empathetic way, starting with considering whether it's in the public interest to report it in the first place’ (Participant 18, News). Another way of ensuring the article was written with sensitivity and respect was to check with the athlete themselves, providing a safe space for them to discuss their personal experience, such as to ‘ensure it is in their own words, so their own agency is maintained’ (Participant 19, News). Many described checking with the athlete directly, such as by ‘reading interviewees’ quotes back to them to ensure they're happy’ (Participant 20, Legal) and indirectly: If you think you're reporting in a way that would make them unhappy with how they've been portrayed (by using inappropriate language, for example), you're probably contributing to the problem rather than helping. (Participant 5, News).
Including words of support, such as from teammates, captains, or ‘supportive coaches/bosses helps guide public opinion – if they're accepting and understanding, its likely fans will be too’ was also thought to be useful (Participant 21, Science).
When asked hypothetically if they had to write an article, their ideas on how they would approach it, such as whether they would focus more on the athlete's personal struggles, the broader issue of mental health in sports, or a combination of both, the vast majority said they would include both angles. Participants noted that ‘context is important’ (Participant 22, Health and social affairs), with many starting with the personal story, followed by the wider context with an aim ‘to improve public understanding of the issue’ (Participant 23, News). You need to tell the personal story to show the audience the effect that poor mental health has at a personal level and then you need to focus on the broader issue to show that the athlete's story is part of a broader issue (Participant 5, News).
Theme 3. Professionalism and accuracy
The final theme focused on using professionalism and facts to reduce stigma and promote empathic discourse. This included the use of ‘fair and accurate reporting’, ‘sticking to the facts’, and using evidence to support assertions, such as the use of ‘statistics to show that athletes are no more likely to have mental illness than the rest of the population’ (Participant 24, Business). Another way they suggested to achieve this was by seeking expert opinion from those in the field, such as mental health professionals to both describe the broader context and how common mental health issues are, and also to indicate the importance of open discussion about mental health: ‘I would perhaps seek comment from an expert in the space about how important it is that this individual has spoken out and what good might come of sharing their story’ (Participant 25, News). Many identified that they would follow guidelines and advice to achieve this, citing that ‘News media already works to guidelines on mental health reporting’ (Participant 6, Arts and culture). Some also reported that they would include help-seeking information such as ‘helplines on stories relating to suicide and mental illness’ (Participant 20, Legal) and a few noting this was mandatory where they work already – ‘we always have a footnote pointing to Beyond blue and other services, with any stories published about mental health. It is built into the editorial system’ (Participant 26, Political).
Many participants felt it was the media's responsibility to report accurately, sensitively, ethically, and compassionately, and that there was a lot of recognition of the potential influence in contributing to public opinion – ‘The media have a mouthpiece to make a positive impact on the way people perceive mental ill-health’ (Participant 1, Court). However, a minority said it was not their job – ‘Our role is to provide the facts, not shape opinions’ (Participant 27, Political). Several comments described the role of the traditional media as changing now that social media and other less regulated media formats are growing. – ‘The media plays a key role, however it is rapidly diminishing as social media grows’ (Participant 28, Sport). Others said this responsibility extends to those who are involved in sports coverage as well, not just those who report on it: It's a huge role, and extends beyond just journalists, but also to commentators, producers and directors in sports coverage. Were a [sports commentator] to flippantly use stigmatising language during coverage of a Friday night game, it would have far more impact than a print article. (Participant 29, Political).
However, there was also a cynicism in some of the responses: ‘sensationalist and clickbait sells, otherwise it wouldn't exist. More people will click on an article about “why did athlete x QUIT?!” than one addressing systemic issues of mental health in high stress and high performance situations. Just the way it is. For now anyways’ (Participant 30, News).
However, there was also some hope presented: I think the way the media covers these stories has changed for the better. There is also now much more willingness by athletes and people generally, to speak openly about mental health issues they are struggling with. This is a positive thing and journalists, by and large, are willing to do stories of this nature. (Participant 31, Education)
Just over half of participants reported having received any training on how to report on mental health and suicide (see Table 2). When asked about what type of training they had received, participants reported that they had either received training in their work setting, accessing brief workplace guidelines, or completing formal training delivered by external groups: ‘The Dart centre's program was fantastic and has very much informed my approach’ (Participant 32, Lifestyle) and ‘Mindframe has provided training sessions at my work on general mental health coverage, as well as more specifically in relation to court reporting’ (Participant 1, Court). A few mentioned that they received training via formal or information discussions, were provided with training at university, or had accessed publicly available guides.
When asked what training would be helpful, many participants mentioned evidence-based style guides that included specific language and examples of ‘what to do’ vs ‘what not to do’. Including evidence-based data and factual information to build knowledge and understanding of mental health was also considered important, as well as keeping this information up-to-date. Providing ‘evidence’ to support the guidelines was valued; for example, some participants mentioned that they were not sure that the current guidance was based on research evidence –‘…does including the helplines actually make any difference? And is there any evidence that supports saying “police are treating the death as non-suspicious” as a euphemism for suicide?’ (Participant 16, Political). One asked for a specific ‘policy’ on how to manage the reporting of deaths, such as accidents, where it has not yet been confirmed as a suicide (Participant 33, News). Some also felt that the information should be delivered by experts including psychologists, those with lived experience, and researchers, with one participant who had not yet received training remarking – ‘I would be most likely to watch a documentary or training video with evidence-based research and recommendations featuring a psychologist and someone with lived experience’ (Participant 34, Crime). Lived experience was thought to be particularly valuable for providing evidence to support guidelines, such as hearing from people about how media coverage of mental health and suicide affected them. At the moment it feels more like a guess from people based on how they might feel in a situation, versus the reality of how someone in a situation feels (Participant 1, Court).
Discussion
In the current study, we found that the 81 journalists who participated had relatively positive attitudes towards mental health and help-seeking, moderate levels of mental health and suicide literacy, and low levels of stigma. Almost half of the participants had experience of mental ill-health either themselves and/or as a carer, and one-quarter had experience reporting on an athlete experiencing mental ill-health or who had suicided. There was recognition of the role of the media in promoting positive attitudes in the community. Several key themes depicted how to do this, including reporting using positive framing and avoiding stigmatising language, communicating with sensitivity and respect, and ensuring reporting was conducted with professionalism and accuracy by following guidelines and focusing on factual reporting. However, only half of the participants had received any training on reporting on mental ill-health and suicide. Journalists noted that their training needs included the provision of evidence to support guidelines, and emphasised the importance of training delivery by experts, including those with lived experience, researchers, and mental health practitioners.
We found that for journalists in this study, mental health literacy was moderate, and that stigma was low. There is limited data to compare these results as data matched on age and other characteristics is unavailable; however, the journalists who responded reported somewhat higher help-seeking attitudes (Busby Grant et al., 2024), lower stigma (Batterham et al., 2013b, 2013a; Busby Grant et al., 2024), and comparable literacy (Batterham et al., 2013b; Gulliver et al., 2018) to university-based staff and students and general community samples. In addition, compared with a study of Australian journalism students with moderate levels of stigma (Burns et al., 2022), the journalists in the current study appeared to have low stigmatising attitudes, well below the mid-point of the scale. However, it is important to note that given likely differences in sample characteristics and potential sampling bias due to self-selection, these differences must be cautiously interpreted.
One notable issue was that some of the journalists commented that the guidelines they had received mentioned avoiding using the word ‘suicide’, or using euphemisms for suicide to avoid talking about it directly. Of note, current guidelines, including Mindframe (Everymind, 2020), the Dart Centre (2020), the Australian Press Council (2025) do not recommend avoiding these terms completely, but they do note that the word suicide should be avoided in headlines, ‘as these can attract vulnerable people to the story’ (Everymind, 2020). It is possible that internal media guidelines for different outlets may recommend avoiding the term ‘suicide’ throughout the article. More recent guidelines from the World Health Organization (WHO) state that whilst previous research has identified that media reports may lead to increased suicide risk in the community (e.g. Pirkis et al., 2019), responsible reporting is also important to provide education to the community and reduce stigma (World Health Organization, 2019). Several journalists also commented that they felt unconvinced that the current guidelines were evidence-based, either based on scientific evidence or lived experience. This is notable, as many of the publicly available guidelines provide references for their recommendations’ sources. However, they do not typically include voices of lived experience. Thus, including this information may be important for improving journalists’ confidence in reporting guidelines.
Journalists provided a broad range of ideas on promoting empathy and avoiding stigma when reporting on this topic. Much of what was mentioned is included in media guidelines for reporting (e.g. Everymind, 2020). These included framing reporting positively, avoiding stigmatising language, and normalising mental ill-health by making athletes relatable (Walton et al., 2019). The views of the journalists may reflect an understanding of guidelines and align with previous research (Ross et al., 2019). For example, media reports using positive framing, such as the experience of recovery from mental ill-health, have been found to reduce stigmatising attitudes in community members, with negative framing doing the opposite (Corrigan et al., 2013). Journalists also believed that providing fair and accurate reporting, seeking and publishing expert opinion, was also a key method to reduce community stigma. The provision of accurate information, including factual information and addressing common misconceptions about mental ill-health, has also been found in the research to improve stigmatising attitudes (Dietrich et al., 2006). More specific to the context of elite sport, they also suggested they could aim to provide sensitive and respectful reporting, starting with whether it is in the public interest to report at all, aligning with the MEAA Journalist Code of Ethics of respecting grief and personal privacy (Media Entertainment & Arts Alliance, 2025). They also suggested including supportive comments from teammates and coaches and checking with athletes to ensure accurate representation.
Only half the participants reported receiving explicit training on how to report on mental health and suicide. Some ideas were offered in the qualitative data for improving training, including the potential for delivery of information by key experts, including people with lived experience, researchers, and practitioners. Providing direct and positive ‘contact’ with people with lived experience is an established, evidence-based method of providing education and reducing stigma (Maunder and White, 2019). Existing Australian programmes, such as the Mental Illness Education Australian Capital Territory (MIEACT) programme, use this method by supporting volunteer educators to share their stories of living with mental ill-health to increase knowledge of mental health, reduce stigma, and contribute to help-seeking behaviours (Mental Illness Education ACT, 2025). Future research could develop a new module or training program on this topic by exploring the best ways to engage journalists in learning about these issues, informed by research, lived experience and practitioner expertise.
Strengths and limitations
A key strength of the current study is the online survey method, where participants can share their ideas privately. It was considered important in previous research as it may reduce perceived risk of judgement (Ross et al., 2024) and encourage honest and open responses. However, there are several limitations to this research. We were only able to contact a selected list of journalists, and many of these emails bounced due to ‘out of office’ replies or were out of date at the time of the study. The response rate was low, although not uncommon in this population for broadly delivered online surveys (Örnebring and Mellado, 2016), and our topic may not have attracted widespread interest. Whilst proportionally few sports journalists responded, the survey was not targeted at this population specifically. In addition, many types of journalists may report on high-interest news stories, including those focused on suicide and mental health. Accordingly, the results are likely affected by sample bias, as those more interested in the topic of the study were likely more inclined to participate. This primarily affects quantitative results, meaning that we cannot generalise beyond the current study, nor make clear comparisons with other studies on findings such as the levels of stigma or mental health literacy. Further, the quantitative data should be treated with caution. For example, half of the participants reported completing training on how to report on mental health and suicide; however, it is possible this is an overestimate, as those who had completed such training may have been more interested to participate in the study. However, the study generated rich qualitative data, which is not reliant on representativeness and may be particularly valuable with a more focused sample of individuals who have an interest and experience in the topic.
Conclusion
This study of Australian journalists aimed to better understand journalists’ attitudes, experiences, and training needs for reporting on mental ill-health and suicide in high-profile athletes and coaches. A cross-sectional online survey was completed by 81 Australian journalists who had diverse opinions on the media's responsibility when reporting mental ill-health and suicide in elite sportspeople, with some believing they had an important role in reducing stigma. Given that almost half of the participants had never received training on how to report on mental ill-health and suicide, further training resources are likely to be beneficial. The format, content and delivery of this training should be developed in collaboration with the end users of these resources and best delivered by experts such as those with lived experience, researchers, and practitioners.
Footnotes
Ethical considerations
The Australian National University Human Research Ethics Committee (ANU HREC) approved the ethical aspects of this research (Protocol number 2023/374) on August 28, 2023.
Consent to participate
Participants provided consent via an online survey by ticking a box marked ‘yes’ when asked if they consented to participating in the research prior to commencing the survey.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by an unrestricted Next Generation Researcher Network Capacity Building Funding Award as part of the ALIVE National Centre for Mental Health Research Translation, funded by NHMRC Special Initiative in Mental Health GNT2002047.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.