
Abstract
Embedding musicians’ occupational health training in music education curricula is widely recommended due to the well-documented high prevalence of performance-related health problems (PRHPs) among musicians across their lifespan. A scoping review was conducted to examine the range of evidence from implementations of musicians’ health education programs, regarding the maintenance of hearing, musculoskeletal, psychological, and vocal health, as well as injury prevention strategies to minimize the risk of PRHP. Eligible sources of evidence included published and unpublished studies reporting occupational health education programs (which may have incorporated information on physical or psychological health, exercise, or somatic movement training) implemented with pre-tertiary and tertiary music students and teachers. Studies reporting stand-alone psychological health education were excluded. Key characteristics from included studies were extracted and charted. Data charts outline commonalities across the reported results, including physical, psychological, educational, and behavioral change outcome measures. Out of 46 records included for data extraction, 35 reported programs with tertiary-aged music students, seven reported programs with pre-tertiary-aged music students, two reported programs with music teachers, and two reported systematic reviews. Reported benefits from this research with both pre-tertiary and tertiary music students suggest that musicians’ health education and injury prevention strategies reduce self-reported playing-related pain and music performance anxiety. However, future implementation studies need to address identified challenges such as effective behavior change and the enablers and barriers to the long-term adoption of strategies for optimal music performance and health outcomes. This review highlights the need for further research into designing and embedding musicians’ health education into all music training settings, including more implementations with pre-tertiary music students, as well as training to support the professional development needs of instrumental and vocal teachers.
Keywords
The high prevalence of performance-related health problems (PRHPs) among musicians at professional, student, and amateur levels of diverse genres and cultures is well documented (Kok et al., 2016, 2018; Roos et al., 2022). School-aged children studying music already commonly suffer PRHP, with reported prevalence rates between 67% and 88% in adolescent musicians before starting tertiary studies (Brandfonbrener, 2009; Gembris et al., 2020; Nawrocka et al., 2014; Ranelli et al., 2011). PRHPs include musculoskeletal, neurological, hearing, vocal, and mental health issues that interfere with performance (Wijsman & Ackermann, 2019), and most are modifiable and preventable through appropriate health education and professional support (Chan & Ackermann, 2014). Preventive education is therefore imperative, with ongoing advocacy for university-level musicians’ health education interventions (Chesky et al., 2006; Rosset et al., 2022; Spahn et al., 2017); yet literature suggests that current musicians’ training provides inadequate health information (Perkins et al., 2017). While some research into the content, implementation, and efficacy of musicians’ health education exists, it is still not typically embedded in music training curricula (Wijsman & Ackermann, 2019). Using a health promotion approach to incorporating health and well-being information as foundational to musicians’ training enables music institutions to meet their responsibility for providing safe, supportive learning environments and ensure students develop health literacy skills for a sustainable career in music (Araújo et al., 2017; Guptill et al., 2022; Perkins et al., 2017).
Health, as defined by the World Health Organization (WHO, 2021), is a state of complete physical, social, and mental well-being, and not merely the absence of disease or infirmity. In broad terms, health promotion is the process of enabling people to increase control over and to improve their health (WHO, 2021). Health education is any combination of learning experiences designed to help individuals and communities improve their health by increasing knowledge, influencing motivation, and improving health literacy (WHO, 2021). Researchers have argued for a more holistic approach to music education to include health promotion strategies guided by the social determinants that affect health and well-being (Ascenso et al., 2017; Philippe et al., 2019). Societies that focus on well-being, as determined by the social, economic, and environmental conditions that support individual and collective health, intentionally create resilient, thriving communities prepared to transcend challenges (WHO, 2021). The rationale for this review is to examine preventive education for delivering musicians’ health information and minimizing occupational risk factors for PRHP, to provide evidence for a health promotion approach in which occupational health training is embedded in music education curricula. This review will present findings from studies on health education programs implemented with pre-tertiary-aged and tertiary-aged music students (or music teachers in these educational settings) to improve performance-related physical or psychological health.
Previous research into musicians’ health education has been criticized for its heterogeneity. Efficacy of published intervention studies has been unclear due to study designs with inconsistent definitions of musicians’ PRHPs (Ajidahun et al., 2019; Ong & Takenaka, 2022; Rotter et al., 2020; Stanhope et al., 2022), different measurement tools, or a lack of theoretical frameworks (Matei et al., 2018; Matei & Ginsborg, 2021; Norton, 2020; Stanhope et al., 2019). In addition, multifactorial considerations for symptoms, including intensity, frequency, location, interference with performance, and perceived causal relationship to symptoms, adds to the confusion with reporting musicians’ PRHPs (Rotter et al., 2020; Stanhope et al., 2019).
Recent literature reviews of tertiary and professional musicians’ health interventions either focused on exercise-based programs (Ajidahun et al., 2019) or health promotion programs (Ong & Takenaka, 2022; Stanhope et al., 2022). These reviews excluded interventions with pre-tertiary-aged musicians or other unpublished interventions that did not fit strict criteria. Research on music performance psychology training is similarly heterogeneous, as highlighted by recent systematic reviews evaluating psychological skills training and management strategies for music performance anxiety (Ford & Arvinen-Barrow, 2019; Zhukov, 2019). These and other literature on psychological health education for music students and teachers are beyond the scope of this review, which specifically assessed literature on physical health education programs for pre-tertiary-aged and tertiary-aged musicians to examine the range of content, outcome measures, and findings.
Recent research into musicians’ health education has recognized that understanding students’ needs and health behaviors as well as applying a behavioral science theoretical framework may be required for effective health promotion in music education settings (Norton, 2020; Rosset et al., 2022). Norton (2020) reviewed performing arts medicine research through the lens of the Behavior Change Wheel or the Capability-Opportunity-Motivation Behavior (COM-B) model (Michie et al., 2011) and highlighted one UK musicians’ health education study that used this model (Matei et al., 2018). Previously published programs have used other behavior change theories, including the I-Change Model (Baadjou et al., 2018), Transtheoretical Model and Precaution Adoption Model (Laursen & Chesky, 2014), Health Belief Model, and Protection Motivation Theory (Seever et al., 2018). These behavioral change frameworks were applied to guide and assess the effectiveness of programs to improve health, educational, performance, or long-lasting behavioral change outcomes.
Student-centered teaching approaches may also serve to guide the design of effective musicians’ health education to ensure translation of and retention of health knowledge. For example, incorporating active learning methods, or authentic learning experiences designed to enhance student engagement, are beneficial in music education settings (Scott, 2011). Research shows that students better recall information through active learning methods compared with passive learning methods (Vanhorn et al., 2019). In this review, reports of programs were reviewed for their content and delivery, and whether the program included active learning opportunities which may have improved participants’ knowledge retention. Findings from this review may help music educators and researchers design, implement, and evaluate future health education programs in music curricula.
Aims
This review sought to evaluate the range of evidence from research on physical health education programs implemented with pre-tertiary-aged or tertiary-aged music students globally and across all genres of music. The research questions were as follows: (1) What types of strategies have been implemented and evaluated? (2) How were the implementations delivered? (3) What are the enablers for, or barriers to, implementing health education into the curriculum in music education contexts?
Method
Scoping reviews aim to map the key concepts that underpin a research area (Arksey & O’Malley, 2005). Now commonly used to synthesize a range of diverse sources of evidence, a scoping review is especially useful to summarize findings from research with heterogeneous methods (Tricco et al., 2018). A scoping literature review was conducted following the guidelines set out in the JBI Manual for Evidence Synthesis (Peters et al., 2020). In addition, the methodological framework proposed by Arksey and O’Malley (2005) and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist (Tricco et al., 2018) were used to guide the review process. The aim of this review was developed by the elements of population, concept, and context (PCC) (Peters et al., 2020). The population was pre-tertiary-aged (approximately 18 years or under) and tertiary-aged (approximately 18 years and over) music students and teachers; the concept was health education programs incorporated into a music curriculum; and the context was pre-tertiary or tertiary music educational settings.
Identification of the relevant studies
A three-step approach was used to search available published and unpublished literature of research involving physical health education programs implemented with both pre-tertiary-aged and tertiary-aged music students across all music genres. An initial search of relevant databases was undertaken (PubMed, Scopus, Cinahl, Embase, PsycInfo, Web of Science, ERIC, Cochrane) with the following keyword terms: “health promotion” OR “health education” OR “injury prevention” OR “intervention” OR “health program” OR “health resource*” AND “music*” OR “pianist*” OR “instrument*.” Duplicate records were removed and relevant records were selected based on analysis of text words in the title, abstract, and index terms for common keywords. Second, a search using all identified keywords and index terms was undertaken across all databases. And, third, reference lists of all identified records were hand-searched for additional records, as well as searching citations in Scopus and Google Scholar for any other records not already identified. The literature search was conducted, analyzed, and verified between July 2018 and August 2021.
Study selection
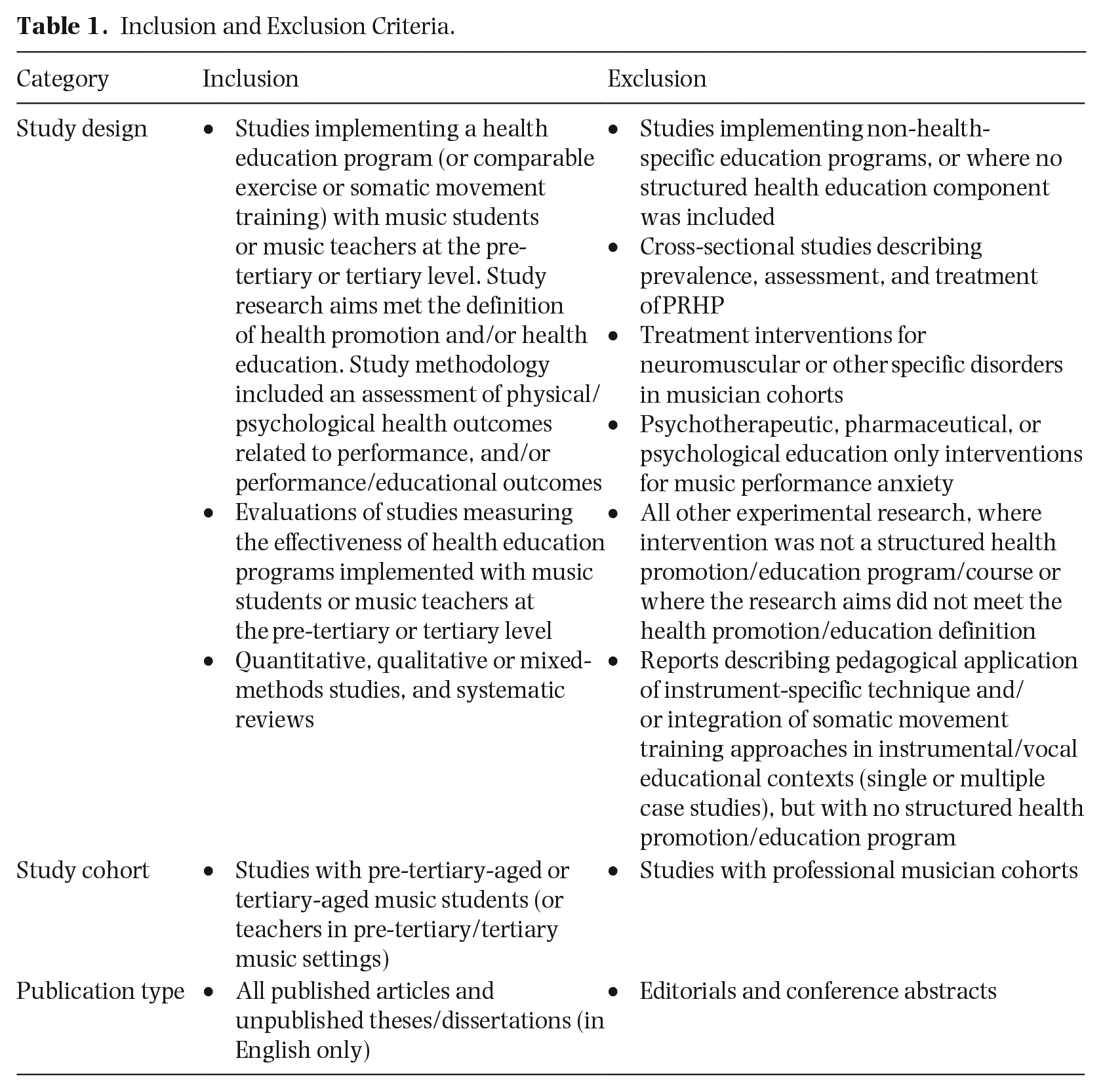
To guide study selection, inclusion and exclusion criteria were established. The inclusion criteria were determined by the elements of PCC listed above. Records were included if each category of the inclusion criteria were met. Outcome measures of interest were categorized into the following areas: physical or psychological health outcomes, educational outcomes, music performance quality outcomes, and health behavior change outcomes. The health education programs were delivered in a pre-tertiary or tertiary music institution as part of, or stand-alone from, the standard curriculum. The types of sources of evidence reviewed included primary research studies, systematic reviews, and dissertations which appropriately reported in-depth evaluations of programs relevant to the research questions. Conference abstracts were excluded. Only sources published in English were considered for inclusion. Included research studies reported physical health education programs (which may have incorporated components of both physical and psychological health). Studies reporting stand-alone psychological health education were excluded. See Table 1 for all inclusion and exclusion criteria.
Inclusion and Exclusion Criteria.
Data extraction
Once all eligible records were identified, data were extracted and charted graphically. Key characteristics extracted from the included studies were author/year, study aims, study design, sample size, program type and contents, program delivery, outcome measures, and key findings. Examples of outcome measures of interest included (1) physical or psychological health measure (e.g., reduction of PRHP or music performance anxiety), (2) educational measure (including assessment of health knowledge or behaviors), and (3) performance measure (including self-rated or expert judged rating of performance quality).
Data analysis
Authors 1 and 2 independently reviewed all included studies and both critically checked data. Key characteristics of all included records were collated for comparative analysis. A meta-analysis of study effectiveness was not possible due to the heterogeneity of this research. Instead, a quantitative content analysis approach was used to count and categorize the frequency of key findings based on outcome measures of interest defined a priori (White & Marsh, 2006). Quality appraisal of the included studies was not undertaken as this is not an integral component of scoping reviews (Peters et al., 2020).
Results
A total of 782 records were identified from the initial search. After duplicates were removed, there were 730 remaining records to be screened. A total of 115 records were identified for full-text review, with a final inclusion of 46 records for data extraction. Figure 1 outlines the search process, results and reasons for excluded records, followed by a descriptive summary of included studies detailing the study characteristics, intervention content, delivery approach, outcome measures, and key findings.
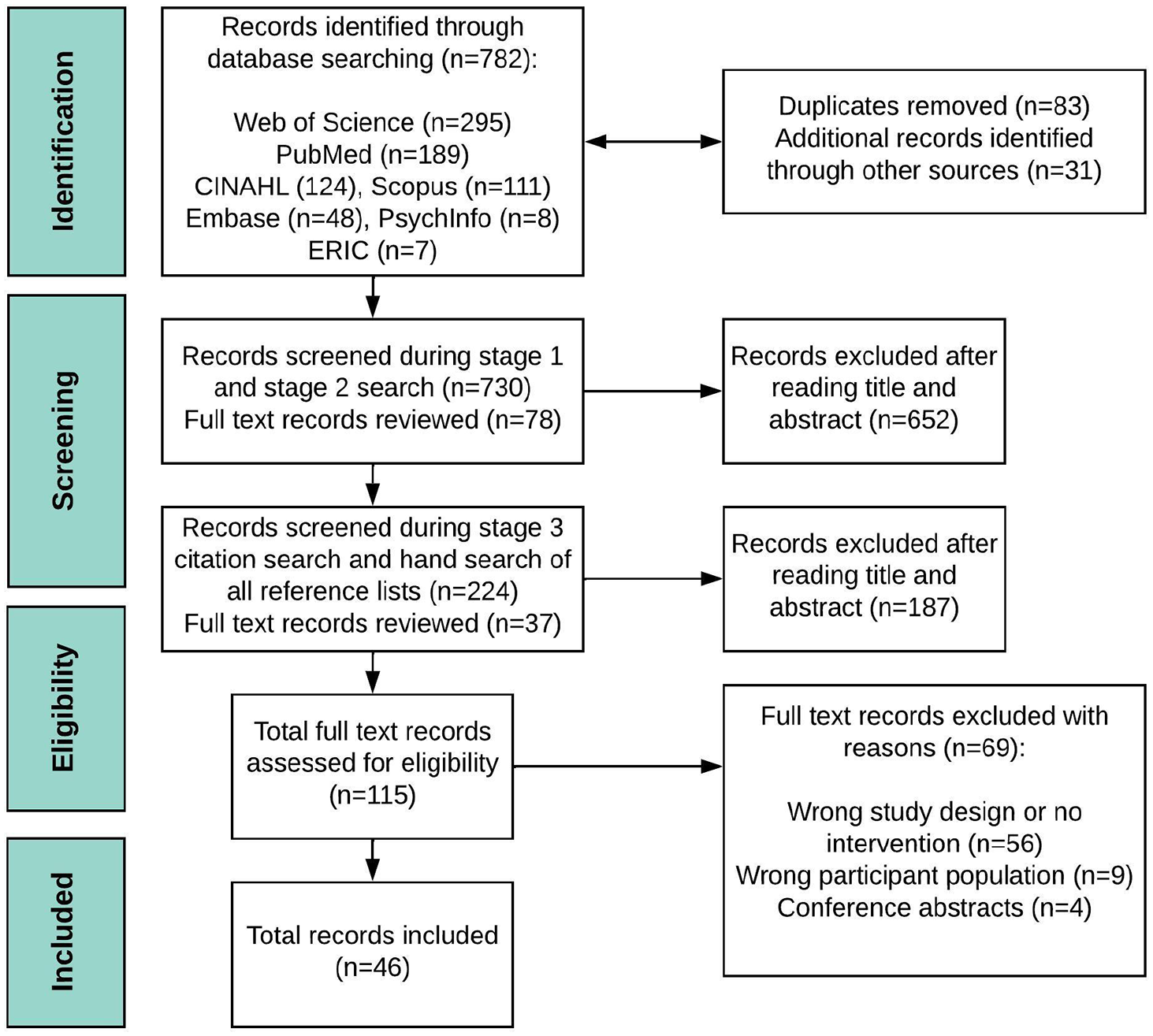
PRISMA Flowchart of the Search Process.
Descriptive findings of study characteristics
Of the 46 studies included, 36 were published journal articles and 10 were unpublished dissertations. Most of the included studies were conducted in the United States (20). Other countries represented were Australia (5), Canada (3), Switzerland (3), the United Kingdom (3), South Africa (2), Spain (2), the Netherlands (2), Brazil (1), Germany (1), Iceland (1), Malaysia (1), Poland (1), and Taiwan (1). The majority of studies were experimental in design: comparative pre-post design studies (17), randomized controlled trials (6), uncontrolled trials (10), qualitative or mixed-method studies (7), program evaluations (3), and one cross-sectional study. Two systematic reviews were also included, one examining the effect of public health interventions on musicians’ musculoskeletal symptoms (Stanhope et al., 2022) and one examining the effect of Alexander Technique on music performance (Klein et al., 2014). From these two systematic reviews, two studies were included that were missed in our search but met our inclusion criteria. See Table S1 and Table S2 in the supplemental material for more detail on the 44 included primary research studies’ key characteristics: author, publication date, country, study design, population, intervention and control parameters, and outcome measures.
Population characteristics
Of all included studies, the sample size of study participants ranged between 3 and 247. Most studies targeted tertiary-aged music students (35), of which one study included both pre-tertiary-aged and tertiary-aged music students. Seven studies included pre-tertiary-aged music students. Two studies targeted music teachers.
Programs implemented and evaluated
Of the 44 primary research studies, 21 were exercise programs and 23 were health education programs. Types of exercise programs included strength training (8), Alexander Technique (8), Pilates (2), or yoga (3). Health education programs varied in design and content. Of these, 12 programs provided theoretical health education only, while eight programs included components of exercise training or other somatic training concepts (including Body Mapping, Alexander Technique, Feldenkrais, Mensendieck, Cesar, Laban Movement Analysis), and three programs focused on hearing health only. The 44 primary research studies by program type and cohort are summarized in Table 2.
Count of Included Primary Research Studies, a by Program Type and Cohort.
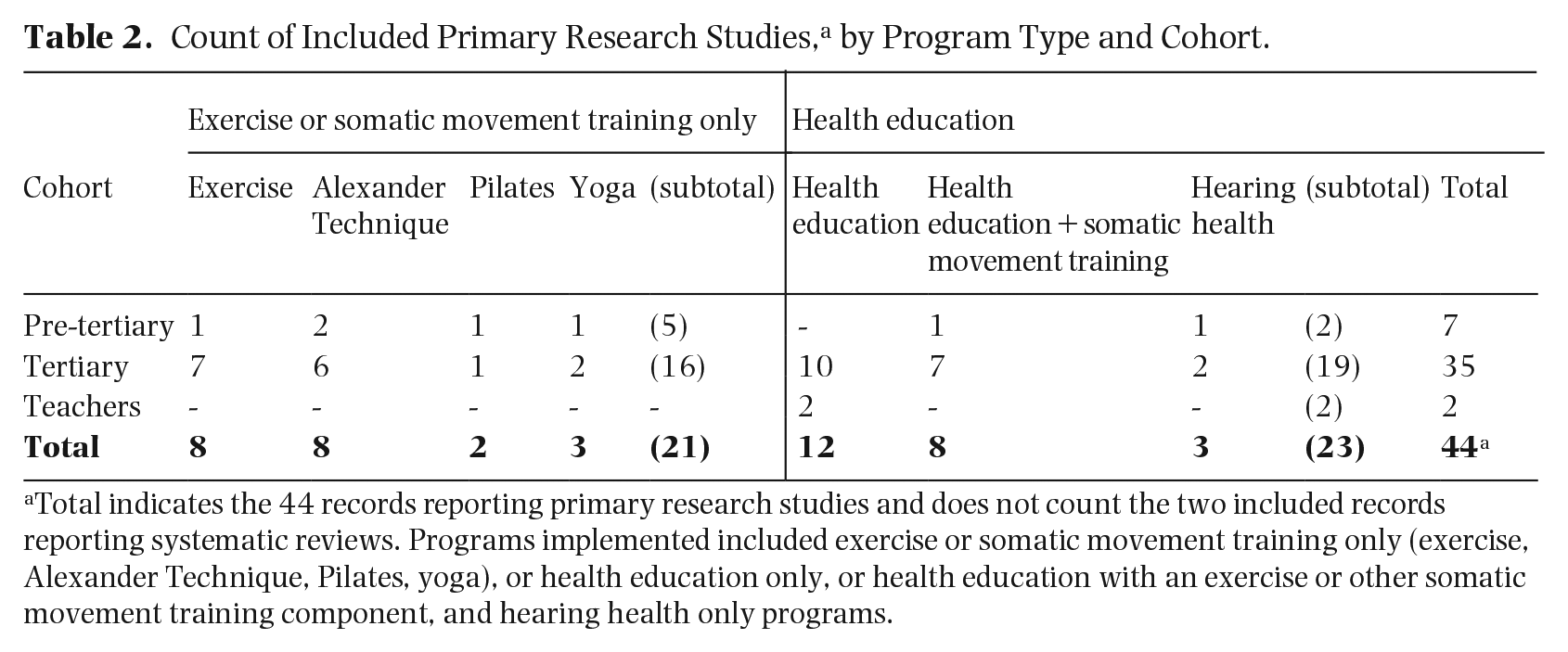
Total indicates the 44 records reporting primary research studies and does not count the two included records reporting systematic reviews. Programs implemented included exercise or somatic movement training only (exercise, Alexander Technique, Pilates, yoga), or health education only, or health education with an exercise or other somatic movement training component, and hearing health only programs.
Implementation content
Programs implemented included exercise or somatic movement training or health education or components of all. The type of exercise tested included strength versus endurance training (Ackermann et al., 2002); a cross-training exercise program 1 (Roos et al., 2021; Roos & Roy, 2018); flexibility or stretching (Coker et al., 2004; Cooper et al., 2012); strength exercises versus massage (Cygańska et al., 2020); strength, flexibility exercises, and yogic breathing (Lee et al., 2012); and Pilates versus trunk endurance (Kava et al., 2010). The type of somatic movement training included Alexander Technique lessons (Davies, 2020a, 2020b; Lorenz, 2002; Mozeiko, 2011; Santiago, 2004; Valentine et al., 1995; Wolf et al., 2017; Ying et al., 2015), Pilates classes (Poncela-Skupien et al., 2020; Sutton, 2020), and yoga classes (Adams, 2012; Khalsa et al., 2013; Stern, 2012). The diverse range of health education content included in programs implemented is summarized in Table 3.
Summary of Musicians’ Health Education Content.
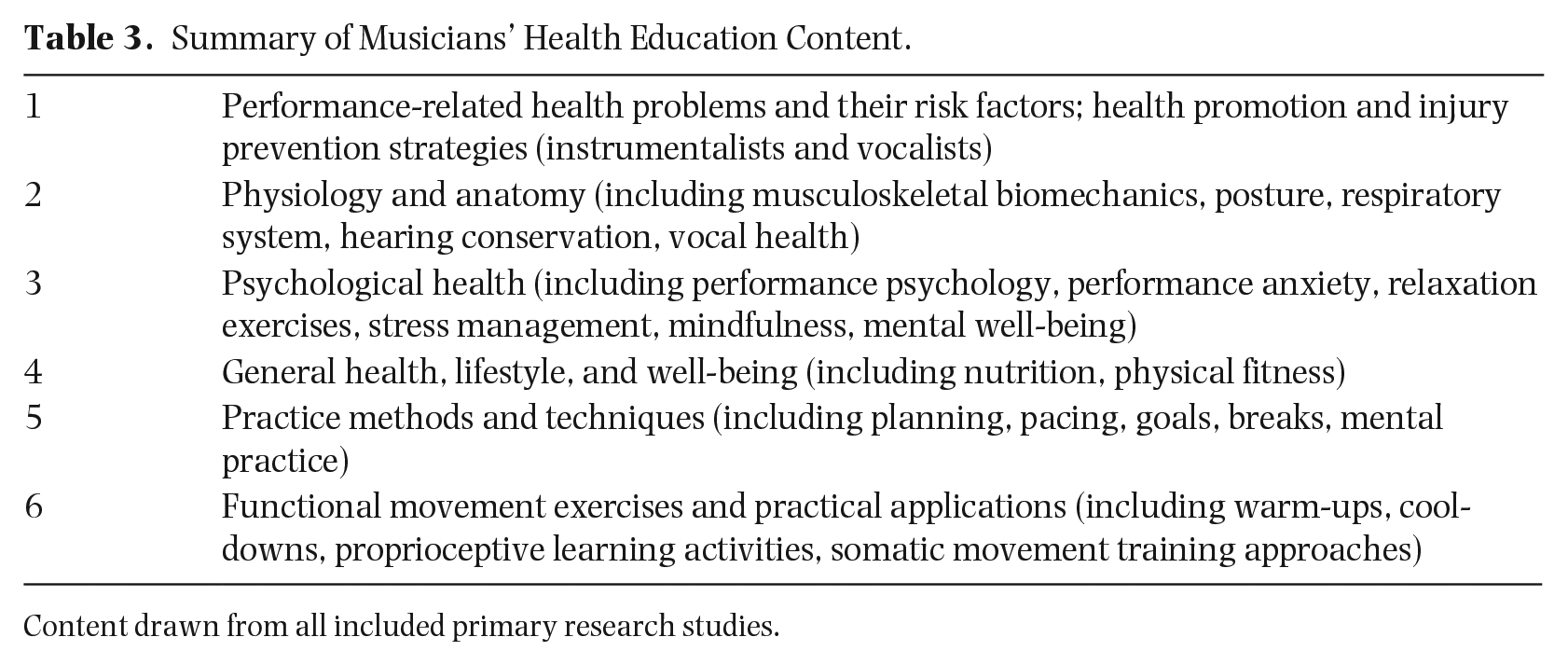
Content drawn from all included primary research studies.
While most programs consisted of content considered to be passive learning, there were nine programs that also included active learning strategies in the course content. Examples of these engagement activities include student reflection, journals, practical applications, experiential movement activities, 2 class discussions, and peer evaluation. See Table S3 in the supplemental material for further detail on program content, who delivered the program and key findings.
Implementation delivery mode
The majority of included primary research studies involved programs that were delivered face-to-face. Only three studies delivered programs online (Ingle, 2013; Su et al., 2012; Wilkenfeld, 2018). All programs were designed and delivered by experienced professionals from a range of backgrounds, including music education, medicine, physical therapy, occupational therapy, psychology, communications science or audiology, and sports science.
Of the 35 tertiary programs implemented, four exercise programs were led by trained health professionals and three exercise programs were delivered by a multidisciplinary team. All nine tertiary programs implementing Alexander Technique, Pilates, and yoga were led by trained instructors, of whom four were also music educators. Most tertiary programs implementing health education programs were delivered by a multidisciplinary team, while seven health education programs were led by music educators with expertise in performing arts medicine, somatic movement training, or included guest lectures from other health professional backgrounds.
Of the seven pre-tertiary programs, only two courses were led by a trained health professional (Auchter & Le Prell, 2014; Poncela-Skupien et al., 2020), while the remaining programs were led by music educators (Cooper et al., 2012; Khalsa et al., 2013; Rardin, 2007; Santiago, 2004). Most pre-tertiary programs implementing Alexander Technique and yoga were led by musicians who were also certified teachers in the somatic modalities, except for one program delivered by a noncertified Alexander Technique teacher (Lorenz, 2002).
Findings
A content analysis of the key findings shows reported benefits grouped by physical health and psychological health outcomes, educational outcomes, music performance outcomes (e.g., application of the health education to music performance), and health behavior change outcomes (see Table 4).
Summary Count of Intervention Key Findings.

While Matei et al. (2018) did not report significant health behavioral changes as assessed by quantitative measures, her doctoral thesis did report on qualitative findings indicating participants reported a variety of behavioral changes including engaging in physical activity and well-being strategies, incorporating warm-up strategies, and using hearing protection devices (Matei, 2019). These qualitative findings were also reported in a more recent paper (Matei & Ginsborg, 2021) which was published outside of this present study’s search period.
Implementation enablers and barriers
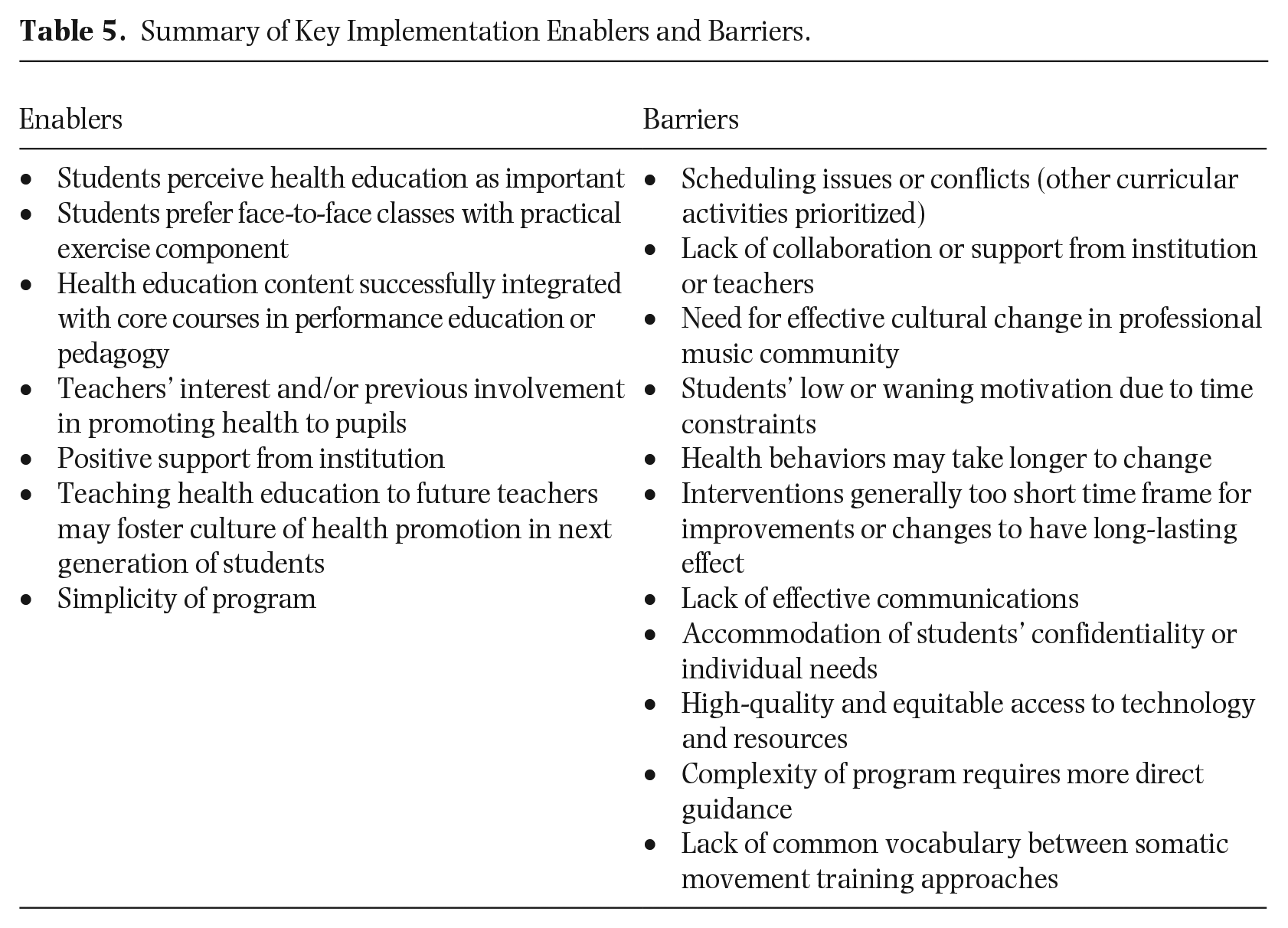
Where enablers or barriers were reported, these challenges and opportunities for future research are summarized in Table 5. These limitations may have occurred for a variety of reasons, as discussed in the next section.
Summary of Key Implementation Enablers and Barriers.
Discussion
Of the few programs implemented with pre-tertiary music students, reported evidence of physical benefits from incorporating exercise, yoga, Pilates, and health education theory were reduced levels of self-reported pain, discomfort, and music performance anxiety. From the many programs implemented with tertiary music students, there is evidence to suggest that health education—encompassing physical, psychological, hearing, and vocal health—significantly reduces performance-related pain and music performance anxiety. In addition, when incorporated into music learning settings, health education optimizes physical and musical efficacy for performance. Programs reporting measures of behavior change showed increased awareness of physical capability for performance and increased use of preventive strategies such as hearing protection devices.
Previous musicians’ health education research has typically relied on self-reported outcome measures. While many studies used standardized questionnaires, only 24% to 33% of studies included standardized questionnaires as an outcome measure (Stanhope et al., 2019). Other studies used modified or researcher-developed self-assessment questionnaires. While these tools may have been valid, study limitations remain, with potential measurement bias impacting validity of study results (Webb et al., 2005: 166). Relatively few studies included clinical measurements for assessing strength gains, muscular endurance, or flexibility. Future research study designs need to include clinical measurements (reliable, validated tools) as appropriate for the outcome measures of interest (Baadjou et al., 2016; Stanhope et al., 2019).
Health education programs contained a wide range of concepts broadly covering physical health (e.g., anatomy, physiology, common PRHP, and risk factors), psychological health (e.g., performance anxiety, mental health), performance-related hearing loss, preventive health (e.g., lifestyle management, diet/nutrition, sleep, behavior change techniques), and music practice and performance preparation (e.g., practicing and rehearsing strategies, postural awareness). Matei and Phillips (2023), who recently surveyed professionals about the content of health education for inclusion in music education, confirmed these broad categories (and other subtopics) as relevant.
Research studies have been designed and delivered by professionals from varying fields of expertise including music educators, occupational or physical therapists, psychologists, and other expert professionals (including in hearing conservation). Programs designed and conducted by multidisciplinary teams are beneficial, especially when health professionals have knowledge and understanding of musicians’ required skills. Including an occupational or other physical therapist in delivery teams has been recommended, for their expertise to assess students (in an occupational setting) or to lead/supervise exercise classes (Barton & Feinberg, 2008; Cygańska et al., 2020).
As seen with the pre-tertiary programs, many programs have been led by musician-researchers alone, albeit with knowledge of musicians’ health issues and expertise in a variety of somatic modalities. Matei and colleagues (2018) argued for high-quality evidence-based musicians’ health education programs that employ rigorous approaches and include the best available research evidence. Hornby and Greaves (2022) define effective evidence-based teaching practices as integrating current research evidence of meaningful change, relevant teacher wisdom and skills, and consistency with the school and community cultures. This is important for future implementations of musicians’ health education in curricula, not only to consider course content but also to consider how the content is delivered to achieve desired learning outcomes. It would be preferable if future interventions are designed and delivered collaboratively by multidisciplinary teams to ensure that evidence-based program content and evidence-based teaching occur in supportive learning environments incorporating health education, screening, and specialized musicians’ health services (Araújo et al., 2017; Perkins et al., 2017).
Musicians’ health research has not consistently used a pedagogical lens or included adequately defined teaching and learning outcomes. This review found limited programs that incorporated active learning strategies in lesson instruction. The elements of active learning—to reflect, evaluate, analyze, synthesize, and communicate information presented (Fink, 2003)—would be beneficial in learning preventive health strategies and applying health information.
More recent pedagogical research has investigated alternative strategies to deliver higher education music curricula. López-Íñiguez and Bennett (2021) suggested developing a holistic music curriculum that incorporated strategies to support music students’ critical thinking skills, fostering growth mindset and a learner identity. These authors further argued the value of student-centered teaching in higher music education settings where students are actively involved in processing knowledge, thereby developing a learner mindset transferable to their career (López-Íñiguez & Bennett, 2021; López-Íñiguez et al., 2022). These important pedagogical aspects in relation to musicians’ health education may serve to foster preventive health strategies, students’ agency, and their health-promoting behaviors.
A common theme among health education programs that measured health behavior change outcomes was that study results did not find significant evidence for predicted change (Auchter & Le Prell, 2014; Baadjou et al., 2021; Ingle, 2013; Matei et al., 2018). This is reportedly due to multiple factors impacting students’ opportunity and motivation to adopt health-promoting behaviors. This observation is consistent with other research investigating health behavior change, due to a well-documented discrepancy between a person’s intention and actual behavior known as the intention-behavior gap (Sheeran & Webb, 2016). Other theoretical models address this gap by examining factors determining a person’s motivation or intentions (e.g., attitudes, social influences, self-efficacy) and by promoting action through specific behavioral strategies, such as self-monitoring, action planning, and goal setting (Ayre et al., 2019; Schwarzer, 2008). While music educators and performing arts health researchers have acknowledged that programs have not been as effective in changing musicians’ health behaviors as predicted, the reasons for this are unclear (Baadjou et al., 2018, 2021; Matei et al., 2018; Norton, 2020; Seever et al., 2018; Spahn et al., 2017). This and the following issues to be addressed are foci of current ongoing research of international collaborative teams (Baadjou et al., 2019). It is recommended that health behavior change assessment mechanisms be incorporated into future intervention or course designs (Matei et al., 2018; Matei & Phillips, 2023; Norton, 2020).
Health promotion initiatives in education settings may inform effective methods for musicians’ health education. Danish school-based health promotion initiatives were found to be beneficial when health-promoting activities were embedded into the curriculum, rather than being offered as an “add-on” activity, although for this approach to be effective, teachers needed adequate training (Bentsen et al., 2020). Other reported effective implementation characteristics of health-promoting initiatives include a positive school culture, creating school/community partnerships, as well as the need to assess change at the level of the whole-school (curriculum, environment, partnerships, and policy) over time to see positive impacts (Calder et al., 2019). Consistent with the accounts of musicians’ health researchers are the important roles within communities and institutions in applying a settings-based approach to promote and develop students’ health literacy and health responsibility, enabling them to maintain their physical, mental, and social well-being throughout their career (Araújo et al., 2017; Matei & Phillips, 2023; Perkins et al., 2017).
Pedagogical approaches, in addition to employing health promotion and health literacy theory, may serve to guide musicians’ health education to enhance engagement, motivation, and application of health information to optimize performance. Health literacy research and musicians’ health research show that health information delivery alone does not always result in better health outcomes or changes in health behaviors (Guptill et al., 2022). Health literacy comprises knowledge, motivation and competencies to access, understand, appraise, and apply health information in order to make judgments and take decisions in everyday life concerning healthcare, disease prevention and health promotion to maintain or improve quality of life during the life course. (Sørensen et al., 2015)
The lens of health literacy may be useful in providing a well-tested, multidimensional framework to guide effective program design, implementation, and evaluation. Musicians’ health literacy, as a construct distinct from general health literacy, has recently been established (Guptill et al., 2022). It is important to understand how musicians’ health literacy influences student and teacher health-promoting behaviors, as well as curriculum design and delivery, and organizational policy in music education settings. A future article will explore how the four dimensions of health literacy—to access, understand, appraise, and apply health information (Sørensen et al., 2012)—could be used to design and scaffold future musicians’ health education programs. Furthermore, future program evaluations should examine how students are being assessed not only for knowledge but also for comprehension, critical evaluation, knowledge application, and skills acquisition. This will provide better understanding to inform effective implementation of musicians’ health education that can positively influence music students’ occupational health literacy, for better health outcomes over their lives.
Addressing enablers and barriers for future implementations
Research studies reporting enablers and/or barriers to implementing musicians’ health education have commonly identified the problematic, systemic culture of resistance to change within musician communities as a barrier to implementing effective health education in curricula (Baadjou et al., 2021; Perkins et al., 2017; Roos et al., 2021). This is despite reports that students perceive health education as important (Ingle, 2013; Matei et al., 2018) and that administrators and teachers support holistic health promotion in music education settings (Norton, 2016; Roos et al., 2021; Wolff et al., 2021). In addition to culture, Thacker (2018) identified other systemic barriers to health promotion in the music studio setting, including teacher education, time, and financial constraints. For institutions, the challenge lies in implementing health education in music teaching curricula that are already full (Laursen & Chesky, 2014). For example, in an intensive music festival setting, Wolff and colleagues (2021) experienced scheduling difficulties in delivering a health program for music students due to an already full program of rehearsals and performances. Similarly, Matei and Phillips (2023) found conservatories are still more likely to prioritize technical and performance skill acquisition over the inclusion of broader educational topics. These findings suggest that, while music administrators and teachers acknowledge the need to support students’ health needs, prioritization of this essential educational component in music curricula and pre-professional performance settings is still lacking.
Baadjou and colleagues (2021) identified prevailing themes impacting implementation of health education related to student motivation, institutional support, and communication. They further argued that music students’ health should be a shared responsibility of students, conservatories, teachers, and health care professionals, thereby providing a supportive culture within the learning environment to influence student motivation leading to behavior change. Roos and colleagues (2021) described the lack of appropriate health education for musicians as a challenge and the high expectations placed on musicians to achieve mastery. Many researchers have described the “musicians’ bubble” where music students experience a closed community and a competitive environment with a culture focused on a high mastery of achievement, thereby perpetuating the “master-apprentice” culture (Matei & Phillips, 2023; Perkins et al., 2017; Waters, 2020). In addition to a problem with institutional cultures, there appears to be an incompatibility of curricula with employability needs (Bennett & Bridgstock, 2015; Creech et al., 2008; Perkins et al., 2017). Further investigation into curriculum change is recommended to ensure higher music education allows students to develop their learner identity, critical thinking, and employability skills to serve current industry needs (Araújo et al., 2020; European Association of Conservatoires, 2023; López-Íñiguez & Bennett, 2021; Matei & Ginsborg, 2021).
A perpetual issue of students’ negative attitudes and beliefs toward managing pain, and a lack of (or fear of) reporting pain and injury, has been reported by many authors in this field (Guptill et al., 2000; Matei & Ginsborg, 2021; Rardin, 2007; Roos et al., 2021). This trend needs to be demystified by further research. Roos and colleagues (2021) identified participants’ readiness for change to address musicians’ needs across all levels of music education. It has been suggested that musicians’ health programs should be made available as part of music education courses to teach future teachers, thereby supporting their important role in promoting musicians’ health to their students (Atkins, 2015; Laursen & Chesky, 2014; Norton et al., 2015; Thacker, 2018). There is also a need for studio teachers’ continuing professional development. Private music teachers and community musicians need to have suitable education and adequate resources to develop musicians’ health literacy, to better support and motivate students to adopt health-promoting behaviors for optimal music performance.
Current research developments occurring globally aim to raise awareness of good practices for physical and mental health of musicians (European Commission et al., 2023) and promote musicians’ health education in the tertiary music education setting, including tailor-made health and performance programs (e.g., Codarts, Rotterdam 3 ), the Healthy Conservatoires Network in the United Kingdom, 4 and new research addressing the education of music teachers regarding musicians’ health (Training Sound Performers project 5 ).
Limitations
This study only included sources published in English. However, while all sources in other languages were excluded, the inclusion criteria were sufficiently broad to have found sufficient relevant sources to address our research questions. While study quality assessment is not usually undertaken in a scoping review, risk of study bias has not been evaluated. As this review contains diverse studies, representing a range of methodologies (quantitative, qualitative, and mixed methods) to assess various interventions, it is difficult to compare these sources for effectiveness of the programs. As noted in this review and in previous systematic reviews of literature on musicians’ health education, it is difficult to compare the quality of these research studies due to issues of measurement inconsistency and variability. Instead, we have systematically compared and mapped the research findings, and discussed individual study limitations where relevant.
Conclusions and recommendations
Due to the scarcity of literature reporting health education implemented in pre-tertiary contexts, and the concerning high prevalence of PRHP in this cohort, future research is needed that evaluates the use of health education resources in pre-tertiary music education settings. Additional, future study areas include research on developing relevant content for professional development and health education training for private instrumental or vocal studio teachers. As highlighted in this article and elsewhere, a more consistent framework for testing musicians’ health education interventions is also needed for this field.
These results synthesize the existing body of literature in English on health education programs implemented in pre-tertiary and tertiary music educational contexts. A wide range of programs have been implemented containing health information relevant to music performance, and different exercise and somatic training designed to improve strength, endurance, flexibility, posture, and/or proprioception. Most programs were delivered by multidisciplinary teams employing mostly direct instruction (passive learning) and some critical reflection (active learning) strategies. Identified enablers and barriers to program implementations suggest that more work is needed to improve organizational cultures to enable music educators to adopt a healthy settings approach to ensure music education provides adequate health and wellness information. Recommendations from these findings can help to inform future musicians’ health education strategies and curriculum development for implementation and evaluation with instrumental and vocal musicians in varied training settings. Further research is needed by multidisciplinary teams to investigate the effectiveness of co-designed programs to support students’ agency and health responsibility in the context of preparing for professional music occupations. Moreover, it is vital that future musicians’ health education be embedded into all music training settings, involving a holistic health promotion approach that includes support from institutions and their leadership, teachers, parents, and the wider community.
Supplemental Material
sj-docx-1-rsm-10.1177_1321103X241235794 – Supplemental material for A scoping review of occupational health education programs for music students and teachers
Supplemental material, sj-docx-1-rsm-10.1177_1321103X241235794 for A scoping review of occupational health education programs for music students and teachers by Alison Evans, Bridget Rennie-Salonen, Suzanne Wijsman and Bronwen Ackermann in Research Studies in Music Education
Footnotes
Author contribution(s)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and/or informed consent
As this study was a scoping literature review, and involved no human study participants, ethics approval and/or informed consent was not required.
Supplemental material
Supplemental material for this article is available online.
Notes
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.