
Abstract
Music students experiencing the potentially debilitating effects of playing-related injury (PRI) often first turn to their music teachers for help. This paper aims to document music instructors’ lived experience and perceptions surrounding PRI and better understand how teachers currently support students’ musculoskeletal health. Using a qualitative description approach, in-depth interviews with 10 oboe teachers (7 male, 3 female) documented their lived experience with or without injury and perceptions of PRI. Self-identified uninjured participants (n = 5) described PRI-adjacent and non-PRI problems which elicited empathy for injured musicians, and self-reflective practices that contributed to better health. Injured participants described varied relationships to their pain, including pain as a source of guilt, distress, learning, and growth, and described diverse coping mechanisms including physical therapy, medication, mindfulness, and self-experimentation. Participants’ observations and experiences of PRI influenced their teaching, and several described seeking greater efficiency in students’ instrument set-up and body use. Resources for injured musicians were perceived to be difficult to access due to financial constraints, unawareness, jargon-filled language, and misinformation. These results suggest a need for more outreach from performing arts health professionals connecting music teachers, often the first point of contact for injured students, with high-quality resources which support student wellbeing.
Keywords
Introduction
Background
Most musicians experience injuries related to their musical craft during their lifetimes (Kok et al., 2016; Rotter et al., 2020; Silva et al., 2015; Zaza, 1998). Meanwhile, a cultural penchant for playing through pain worsens these injuries, wreaking havoc in the mental, emotional, and social lives of musicians (Britsch, 2005; Guptill, 2011; Rickert et al., 2014a). Playing-related injuries (PRI) are typically defined as “any pain, weakness, numbness, tingling, or other symptoms which interfere with your ability to play your instrument at the level you are accustomed to” (Zaza & Farewell, 1997). PRI are highly prevalent among music students (Ballenberger et al., 2018, 2023; Cruder et al., 2020; Ranelli et al., 2011), and younger age has been found to be a predictive factor for PRI among university-aged amateur musicians (Kok et al., 2018). Instrument played also influences rates of PRI, with woodwind and bowed string players most likely to report an injury (Stanek et al., 2017). Oboists, for example, have a relatively high prevalence of PRI at 74.9%, largely due to static loading of the right thumb which can lead to issues on the right side of the body (Banzhoff et al., 2017; Macdonald et al., 2022; Thrasher & Chesky, 2001). Injured students most often first turn to their private music teachers for help and advice (Norton & Greasley, 2014; Stanek et al., 2017; Williamon & Thompson, 2006), making educators uniquely positioned to support students and direct them to the professional medical help they need. Unfortunately, private music instructors’ training rarely covers wellness topics, and teachers and students alike frequently espouse the belief that teachers are ill-equipped to deal with student PRI (Rickert et al., 2015; Wijsman & Ackermann, 2019). Teaching practices are often profoundly influenced by personal experience (Carrillo et al., 2015). Because there is no standardized training for private music instructors, educational approaches to injury prevention and healthy musicianship are therefore almost entirely dependent on teachers’ personal lived experience with or without PRI.
There is a growing body of literature addressing the need for qualitative research examining the lived experience and perspectives of performers dealing with injury (Bragge et al., 2006; Guptill, 2011; Rickert et al., 2014b; Schoeb & Zosso, 2012), and several works have explored music students’ experience and perspectives on dealing with injury and wellness initiatives in the context of their educational institutions and healthcare systems (Edwards, 2022; Park et al., 2007; Perkins et al., 2017; Rickert et al., 2015). A recent study asked K-12 (i.e. school students aged 4–18) music teachers about their perceptions of healthy musicianship (Salas-Ruiz et al., 2023), however no known studies have specifically focused on the lived experiences of private music instructors, despite their documented role as first point of contact for many injured students.
Research question
This paper is the first in a two-part series examining oboe teachers’ perspectives on PRI. The quantity of detailed qualitative data obtained in this study necessitated splitting the paper into two sections. The goal of the present paper (Part I) is to document music teachers’ lived experience and perceptions on the causes and remedies of PRI. Part II will document teachers’ perceived barriers and solutions to health promotion among students as well as current preventive and remedial teaching practices. For optimal comparability of results, we focus on a single group of musicians vulnerable to PRI: oboists, who experience relatively high rates of PRI (Stanek et al., 2017). This paper aims to document oboe teachers’ (1) lived experience with or without injury and (2) perceptions of playing-related injury.
Methods
IRB approval
This project was approved by the University of Toronto Research Ethics Board (Protocol #42197).
Participants
Participants were selected based on their experience and reputation teaching and coaching young and early-career oboe players (see sections 3.2.1 and 3.2.2 for inclusion/exclusion criteria). A purposeful snowball sampling technique was used to identify and recruit participants. To ensure a range of lived experience and perspectives, participants both with and without prior experience of injury (self-identified) were included in the study. It was determined that a sample size of 10 participants would provide a sufficient diversity of characteristics (see Table 1) to produce a rich and detailed dataset. This sample size is in line with previous work on musicians using qualitative description methodology (n = 6, Salas-Ruiz et al., 2023), and other qualitative work on musicians’ health (n = 12, Guptill, 2011; n = 10, Rickert et al., 2013).
Participant characteristics.
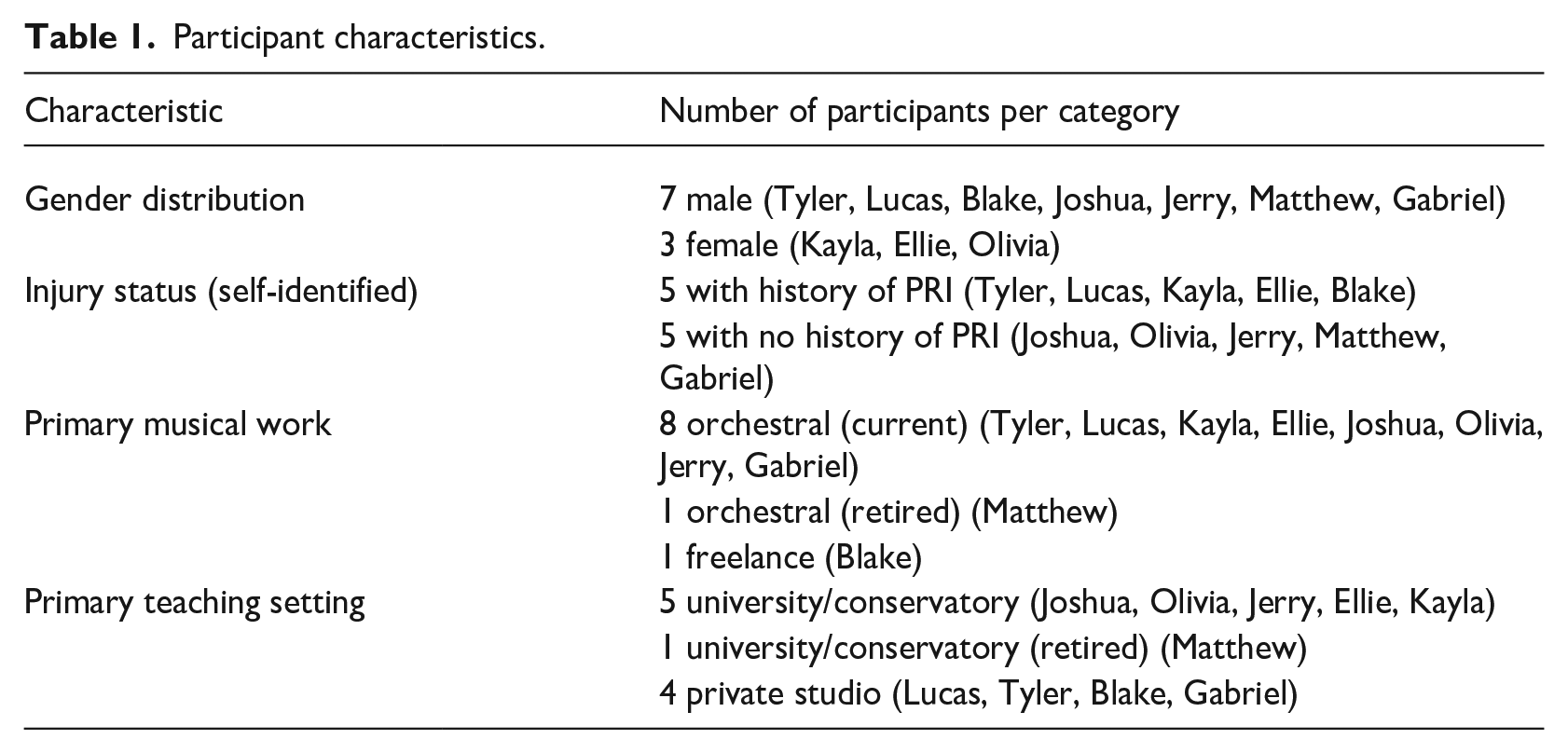
Ten participants (7 male, 3 female, 5 with personal history of injury) participated in the interviews. All were professional oboists and educators whose primary income source was performing and/or teaching on the oboe and/or English horn. Participants lived and worked in English-speaking countries in North America and Oceania. Eight of 10 participants were currently employed as members of professional orchestras, one was recently retired from a professional orchestra, and one freelanced with major orchestras. In terms of teaching, four taught primarily out of their private studios, five taught primarily as faculty at a university and/or conservatory, and one was recently retired from a faculty position at a university. See Table 1 for a summary of participant characteristics.
Inclusion criteria
Participants were included if they had: (1) a professional career as an oboist/English horn player and teacher (e.g. performs with a professional orchestra, teaches oboe at a university, or equivalent experience) and (2) extensive experience (e.g. a decade or more of professional experience) teaching/coaching young/early career oboe players.
Exclusion criteria
Participants were excluded if they were: (1) primarily performers with minimal teaching/coaching experience and (2) specialists in instruments other than the oboe.
Recruitment
Participants were recruited by the PI via email. Participants provided written, informed consent and were able to withdraw their information at any point prior to publication.
Interview questions and process
Semi-structured individual interviews were conducted with 10 participants by the first author via Zoom. The interviews consisted of a series of open-ended questions about (1) their lived experience with or without playing-related injury, (2) their perception of musicians’ injuries and the culture surrounding musicians’ health, and (3) their teaching or mentoring philosophy as it relates to musicians’ health. Interview lengths ranged from 30 to 75 min. Please see the Supplemental Material for the full interview guide. Interviewees were encouraged to elaborate on their answers and narrate stories of their personal experience that have contributed to their perceptions and practices. The Zoom recordings of the interviews were transcribed verbatim using the transcription software Whisper and the resulting transcripts were reviewed and edited for accuracy by the first author. A rich and detailed description of participants’ experiences was compiled from these transcripts. Data were anonymized, with pseudonyms used for all participants and any institutions referenced in the interview dialog.
In the interviews, PRI was defined using Zaza and Farewell’s (1997) definition (“any pain, weakness, numbness, tingling, or other symptoms that interfere with your ability to play your instrument at the level you are accustomed to”). The term “playing-related injury” (PRI) was used as opposed to “playing-related musculoskeletal disorder” (PRMD) as it was anticipated that the language would be more accessible to a general musician audience.
Analysis
Data were analyzed using a qualitative description approach (Neergaard et al., 2009; Sandelowski, 2000, 2010). This low-inference approach has been used extensively to answer questions of why/how and to complement the abundance of quantitative research that asks how much/when. While no research is ever free of bias and interpretation, qualitative description methodology stays true to the data as much as possible, directly communicating the participants’ experiences to the reader while minimizing interpretation by the researcher. This data-near approach has been used in previous work analyzing music teacher’s perceptions of healthy musicianship (Salas-Ruiz et al., 2023).
A combination of deductive and inductive coding was used to analyze the data. The first author compiled data in a spreadsheet organized into larger categories arising from the questionnaire and research questions (e.g. “Lived experience with injury”). These categories are indicated in section headings in the Results and Discussion sections. Sub-themes, indicated within the text of the Results and Discussion sections in boldface, arose inductively from the initial sorting of data as patterns emerged (e.g. relationships with pain).
Results
Lived experience with or without injury
Participants described a wide range of experiences with or without injury. Five self-identified as not having been injured during their careers (Joshua, Olivia, Jerry, Matthew, Gabriel; all pseudonyms), while the other 5 (Tyler, Lucas, Kayla, Ellie, Blake; all pseudonyms) had dealt with injuries that were, at times, debilitating.
Uninjured participants
A few of the self-identified uninjured participants
Some of the uninjured participants
Some of the uninjured participants narrated stories of
Several participants brought up
Injured participants
Participants who identified as having had an injury described a
For some participants, the
Participants described a variety of
Participants’ observations of others
Participants discussed their observations of students and colleagues dealing with injury, as well as the conclusions they came to as a result of these observations.
Some participants’ observations of their students dealing with injury influenced their
A few participants made observations about
Some participants commented on an apparent
Some participants observed students or colleagues using
Perceptions on availability of resources
Participants shared their thoughts on the availability of resources for injured musicians. They expressed mixed opinions on whether these resources were adequate.
Several participants expressed their belief that there are many resources out there for injured musicians, but cited inadequacies or barriers preventing universal access to these resources (see Figure 1). For example, Joshua thinks that over the last few years, many more resources have become available to musicians, however not all this information is available in
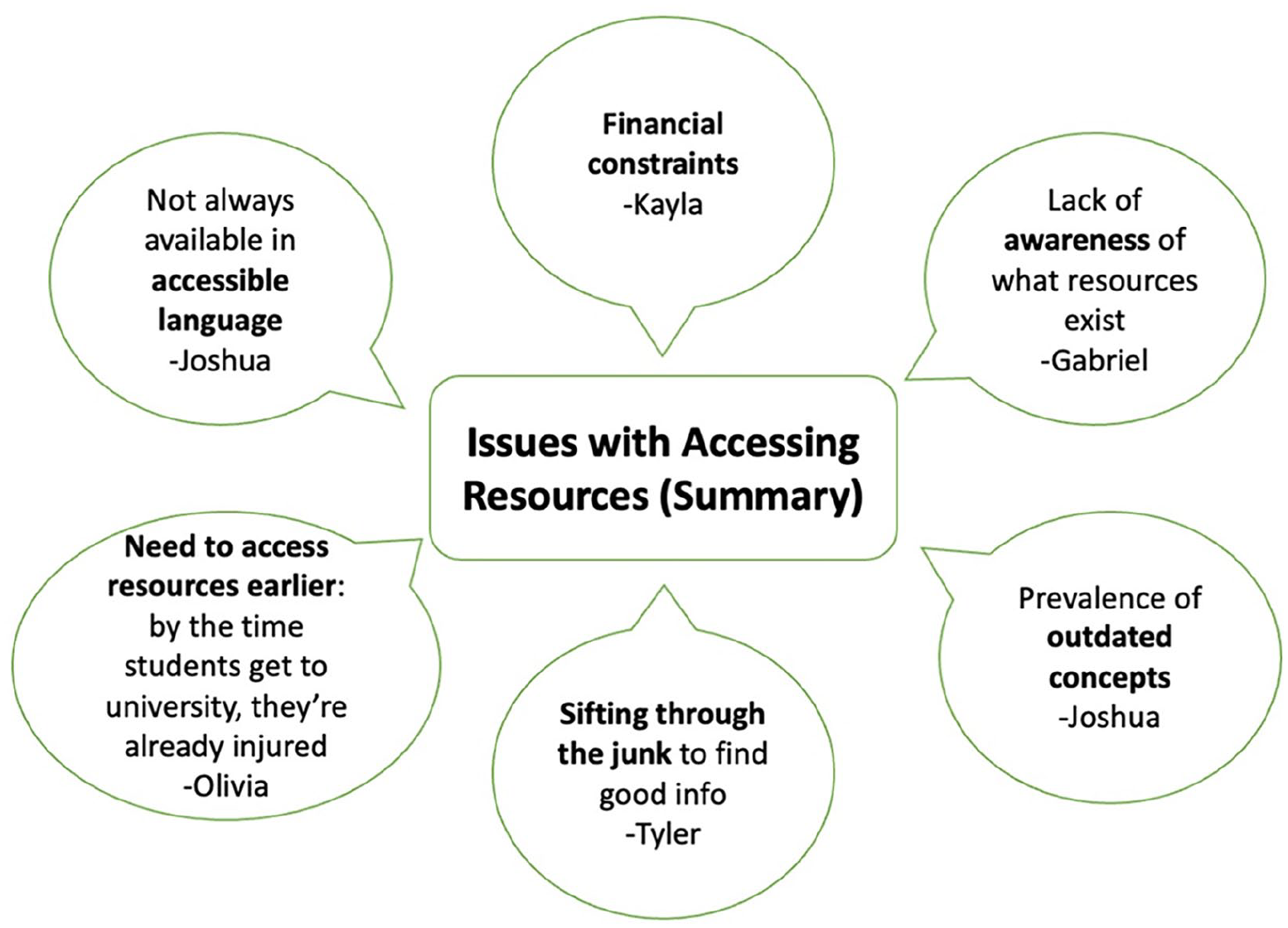
Participants’ perceived barriers to accessing resources.
Many participants referenced specific resources that they either have used themselves or that they recommend to students. These resources included
Discussion
Lived experience with or without injury
Several self-identified uninjured participants described non-PRI issues and self-reflective practices that underlined an
The many non-PRI issues described by the self-identified “uninjured” participants, including sensations that could be interpreted as pre-injury symptoms, demonstrate that injury exists on a spectrum from mild and manageable to severe and debilitating. Future research could gain valuable insights into injury prevention through in-depth analysis of the experiences of musicians with pre-injury symptoms that do not develop into full-blown PRI (i.e. interfering with their ability to play, as per Zaza & Farewell, 1997).
Injured participants described a variety of
Interviewees who had been injured described a range of
Participants’ observations of others
Participants discussed their observations about PRI, and described ways in which their observations had influenced their teaching. Some observations had to do with who in their experience was more likely to get injured—namely
Several participants commented on an apparent two-way connection between
Some participants commented on their observations of colleagues and students using
Perceptions: Availability of resources
Participants had mixed perceptions on the
Scope, limitations
As with all qualitative studies, results from this study are not necessarily generalizable to other oboists or musicians. The value of studies such as this lie in the nuance and detail of the participants’ perspectives, which can lead to valuable insight with a potential to improve how we approach musicians’ health with student musicians. It is possible that a selection bias influenced the results: those who were willing to participate in these interviews may be the teachers who already think a great deal about injury and health and may not be reflective of the perspectives of music teachers in general. We attempted to mitigate this potential for selection bias by including participants both with and without a history of PRI, to ensure a diverse range of lived experience and perspectives.
Conclusion: Applications and future directions
Music educators are typically the first line of defense for students dealing with PRI, yet little is known about how their lived experience and perspectives inform their approach to student wellness. This is the first known study to specifically document the lived experiences and perspectives of music educators as they pertain to PRI. In conclusion, here are some main takeaways from the present research:
Interviewees demonstrated a great deal of empathy for and a desire to help injured students regardless of their personal history with or without injury.
There is a need for further de-stigmatization of instrument supports and modifications.
Availability, accessibility, and knowledge of resources for musicians dealing with PRI is lacking, and more outreach efforts should attempt to reach music teachers to increase awareness.
To build on these results, the second article in this series will examine perceived barriers preventing musicians from seeking help, as well as teachers’ current approaches to wellness topics with their students. Future research into how performing arts medicine outreach efforts might more effectively reach music teachers is also warranted.
Supplemental Material
sj-docx-1-ijm-10.1177_02557614241279723 – Supplemental material for Oboe educators’ perspectives on playing-related injury, Part I: Lived experience and perceptions surrounding injury
Supplemental material, sj-docx-1-ijm-10.1177_02557614241279723 for Oboe educators’ perspectives on playing-related injury, Part I: Lived experience and perceptions surrounding injury by Heather M Macdonald and Christine Guptill in International Journal of Music Education
Footnotes
Author’s note
Prior presentation: Results from this study have previously been presented at the following conferences: the Performing Arts Medicine Association, the Music and Health Research Collaboratory, the International Society for Performance Science, and the University of Toronto Music Graduate Student Conference.
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.