
Abstract
Background
Stroke is one of the leading causes of disability and mortality worldwide, and the 30-day readmission rate is a crucial indicator for assessing the quality of healthcare and patient outcomes. Previous studies have reported a readmission rate of approximately 10%-20%.
Objectives
This study investigated the impact of the COVID-19 pandemic on the readmission rate at 30 days among hospitalized stroke patients.
Methods
This retrospective cohort study was conducted in a 1500-bed medical center in central Taiwan between January 1, 2020, and December 31, 2023. Data, including 5095 hospitalized stroke patients, 505 readmissions within 30 days, and multiple variables that influence hospital readmission at 30 days, including demographics, clinical characteristics, physiological data, and medication use before discharge, were obtained from hospital electronic health records (EHR).
Results
The results revealed a significant decline in 30-day readmission rates between the early (2020∼2021) and latter (2022∼2023) phases of the pandemic, decreasing from 10.71% to 8.97% (P = .039). This reduction may be attributed to improvements in medical strategies, increased adoption of telemedicine, and improved post-discharge care. Generalized linear regression analysis indicated that male patients were at higher risk of readmission than female patients (OR = 1.28, P = .01), while other variables, such as age, BMI, and blood pressure, did not reach statistical significance. Furthermore, common cardiovascular and metabolic medications (antithrombotic agents, lipid-lowering drugs, antihypertensive drugs, and antidiabetic medications) did not significantly affect the risk of readmission (P > .05).
Conclusions
This finding suggests that improvements in medical management during the early pandemic phase may have contributed to a reduced risk of readmission. Furthermore, male patients had a higher risk of readmission, highlighting the need for improved care strategies for this group.
Introduction
Stroke is one of the leading causes of mortality and disability worldwide, with both ischemic stroke and hemorrhagic stroke that require intensive treatment and long-term rehabilitation. The 30-day hospital readmission rate is a crucial indicator for evaluating healthcare quality, patient prognosis, and disease severity. 1 Previous studies have reported that the 30-day readmission rate among stroke patients ranges from approximately 10% to 20%, influenced by factors such as stroke severity, comorbidities, social support systems, and access to healthcare. 2
Since the outbreak of COVID-19 at the end of 2019, the pandemic has had a profound impact on global healthcare systems. Medical resources were redistributed, hospital policies were adjusted, and patient care seeker behaviors changed, leading to changes in the clinical management of acute stroke and post-discharge care. Previous studies have shown that during the pandemic, emergency department visits and hospitalization rates for stroke patients decreased, but changes in the 30-day readmission rate varied depending on regional differences and healthcare strategies. 3
During the early phase of the COVID-19 pandemic, lockdown measures and patient fears of nosocomial infections led to a significant decrease in emergency department visits for acute stroke. 4 This reduction may have resulted in delayed treatment for patients with mild strokes, potentially increasing the risk of subsequent readmission. According to data from the Guidelines Stroke Registry in the United States, stroke hospitalization rates decreased by 30% during the pandemic, highlighting a substantial change in healthcare-seeking behaviors.
Redistribution of medical resources has led to modifications in stroke treatment protocols. For example, intravenous thrombolysis (IV rtPA) and mechanical thrombectomy rates have decreased, potentially affecting post-discharge neurological recovery and readmission rates. 5 Additionally, the increased incidence of COVID-19-related complications, such as hypercoagulability and arterial embolism, may have placed stroke patients at increased risk of recurrent stroke or other vascular events. 6
During the pandemic, many hospitals adopted early discharge policies to minimize the risk of infection in the hospital. However, this approach may lead to insufficient post-discharge rehabilitation, thereby affecting readmission rates.7,8 Telemedicine has been widely implemented during the pandemic, providing remote follow-up and rehabilitation guidance. Although telemedicine offers certain advantages, it cannot fully replace in-person evaluations, potentially affecting patient recovery and the management of post-stroke complications. 9
Several retrospective studies have investigated the impact of the COVID-19 pandemic on hospital readmission rates at 30 days, revealing varying trends. These discrepancies can be attributed to differences in regional healthcare policies, allocation of medical resources, and patient characteristics.10,11
The increase in the unplanned readmission rate during the pandemic was potentially due to inadequate post-discharge care, worsening patient health conditions, and COVID-19 infections. 12 Furthermore, stroke patients with comorbid cardiovascular disease (CVD) had significantly higher readmission rates during the pandemic, which may be related to the impact of COVID-19 on vascular endothelial function. 13
In contrast, other studies have indicated a decrease in readmission rates at 30 days during the pandemic. For example, a reduction in readmission rates in certain regions suggests that patients may have avoided unnecessary medical visits during this period, leading to a low report of mild cases requiring hospitalization.14,15
Age and comorbidities, elderly patients (>65 years of age), and those with comorbidities such as diabetes, cardiovascular disease, and renal dysfunction were at increased risk of readmission. Patients with COVID-19 infection may have a higher risk of readmission, primarily due to complications such as acute cerebrovascular events, pulmonary infections, or systemic inflammatory responses. 16 Post-discharge care models, patients receiving home care or those participating in structured rehabilitation programs were less likely to be readmitted, whereas those lacking regular medical follow-ups had a higher risk of readmission.
This study aims to examine the influence of the COVID-19 pandemic on hospital readmission rates at 30 days among stroke patients within a large tertiary medical facility in Taiwan. The rationale for this investigation comes from the understanding that the pandemic prompted significant changes in healthcare delivery, including modifications to hospital workflows, increased use of telemedicine, and changes in patient healthcare-seeking behaviors. Such systemic changes may have directly or indirectly affected post-discharge outcomes, including readmission rates. By identifying these effects and the associated risk factors, this study offers critical insights for optimizing stroke care and the development of healthcare strategies in light of present and future public health crises.
Materials and Methods
This retrospective cohort study was conducted in a 1500-bed medical center in central Taiwan between January 1, 2020, and December 31, 2023. Data were obtained from the hospital’s electronic health records (EHR), including 5095 hospitalized stroke patients (early-pandemic 2755 and late-pandemic 2340 patients) and 505 readmissions within 30 days (295 and 210 patients were readmitted during the early and late pandemic periods, respectively) (Figure 1). The data set included demographic information, hospitalization details, medication records, and physiological parameters. The primary objective was to investigate trends in 30-day hospital readmission rates among stroke patients during the COVID-19 pandemic and to identify associated risk factors. Flow Chart of the Study for Hospitalized Stroke Patients, Early-Pandemic Patients and Late-Pandemic Patients, Including Those who Were Not Readmitted or Readmitted
Patient Inclusion and Exclusion Criteria
The inclusion criterion for the patient was a first-time hospitalization diagnosis of stroke, aged 20-90 years. Diagnoses were based on the ICD-9 codes 430--436, including hemorrhagic and ischemic stroke. Exclusion criteria included patients who were diagnosed with transient ischaemic attack (TIA) or asymptomatic cerebrovascular disease (ICD-9 codes: 432.x, 433.x0, 435.x), patients aged <20 years (considered a vulnerable population) or those aged >90 years (excluded due to developmental concerns and the impact of multiple comorbidities). Patients who died at discharge or discharged in critical condition.
Sample Size Determination
As this was a retrospective cohort study, all eligible stroke patients hospitalized between January 1, 2020, and December 31, 2023, at the study institution were included, based on the predefined inclusion and exclusion criteria. Therefore, no a priori sample size or statistical power calculation was performed. The final sample size (n = 5095) reflects the complete population that met the criteria within the specified study period, ensuring maximum use of data for analysis.
Data Collection
This study examined multiple variables that influence hospital readmission at 30 days, including demographics, clinical characteristics, physiological data, and medication use before discharge. For the private patient issue, we could not share our data with the public. Due to the limitations inherent in the retrospective nature of the dataset, the exact onset time of stroke symptoms and details of acute treatments, such as intravenous thrombolysis (IV rtPA) or mechanical thrombectomy, were not consistently documented in electronic health records and, as a result, were omitted from this analysis. 1 Demographic and clinical characteristics: Variables included age, sex, readmission status at 30 days, and body mass index (BMI). 2 Physiological data, including systolic blood pressure (SBP), diastolic blood pressure (DBP), pulse rate, respiratory rate, and peripheral oxygen saturation (SpO2), were recorded within 24 h before discharge. 3 Use of medication before discharge: Medication prescriptions at discharge were classified according to the World Health Organization (WHO) Anatomical Therapeutic Chemical (ATC) classification system. In this study, the ATC classification was used solely to categorize discharge medications into pharmacological classes for descriptive purposes. Medication adherence, dosage, and combination therapy were not assessed, as these data were not consistently available in the retrospective data set. The final prescriptions before discharge were analyzed to assess the potential impact of medications on readmission risk. The medications used included antithrombotic agents, lipid lowering drugs, antihypertensive agents, antidiabetic medications, diuretics, beta-blockers, calcium channel blockers, and renin‒angiotensin system inhibitors.
Clear inclusion and exclusion criteria were implemented to mitigate selection bias. Comprehensiveness and standardization of the majority of critical variables were guaranteed by retrieving the data set from a centralized electronic health record (EHR) system. No imputation methods were used, and cases with missing demographic, physiological, or medication data (<1% of all cases) were excluded from the analysis. Since this was a retrospective study using internal hospital records, there was no loss of follow-up and all readmissions at 30 days were monitored within the same system.
Statistical Analysis
All statistical analyzes were performed via STATA 18. Univariate and multivariate analyzes were performed to identify independent factors that influence hospital readmission at 30 days. For the univariate analysis, continuous variables were analyzed using t tests (for normally distributed data). Categorical variables were evaluated using the chi-square test. Multivariate analysis and generalized linear regression analysis were performed to identify independent predictors of 30-day readmission, with readmission as the dependent variable and age, sex, BMI, blood pressure, physiological data, and medication used as independent variables.
Independent predictors of 30-day readmission were identified using a generalized linear regression model (logit link function). Independent variables were demographic characteristics (age, sex), physiological measures (BMI, blood pressure, respiratory rate, pulse rate, SpO2), and medication use (antithrombotic, antihypertensive, lipid lowering and antidiabetic agents). The dependent variable was readmission status (yes/no). For the univariate analysis, categorical variables were analyzed using chi-square tests, while continuous variables were analyzed using t-tests. In the multivariate model, variables that were clinically relevant or had a P-value less than 0.1 in the univariate analysis were incorporated. Furthermore, multicollinearity between independent variables was assessed using the variance inflation factor (VIF). All variables included in the final multivariate model demonstrated VIF values below 2, which is well below commonly accepted thresholds (VIF >5 or 10) for significant multicollinearity. This result indicates that the included variables were not substantially intercorrelated and that the stability of the regression estimates was not compromised.
Institutional Review Board (IRB) Approval
This study was approved by the Institutional Review Board (IRB) of Changhua Christian Hospital (approval number: 241110). As a retrospective study, all patient data were deidentified and individual informed consent was waived by the IRB to ensure patient privacy and compliance with ethical standards. The authors have no potential conflicts of interest with respect to the investigation, authorship, and publication of this article. The methodological framework of this study ensures the reliability and validity of the results. These findings provide crucial clinical evidence on the risk of stroke patient readmission during the COVID-19 pandemic, contributing to improvements in healthcare strategies and postdischarge management.
Results
Baseline Characteristics and Generalized Linear Regression Results for 30-Day Readmission

Abbreviations: Std. err., standard error; SD, standard deviation; CI, confidence interval.
Factors influencing hospital readmission at 30 days (Readmission30) among stroke patients, including demographic variables (age, sex), physiological indicators (BMI, blood pressure, pulse rate, and oxygen saturation), use of clinical medications (antithrombotic agents, lipid-lowering drugs, antihypertensive agents, and antidiabetic medications) and early (2020∼2021) and late (2022∼2023) phases of the COVID-19 pandemic, were analyzed.
A generalized linear regression analysis was performed to identify independent predictors of readmission at 30 days, evaluating the associations between these variables and the risk of readmission (Table 1). 17 The results are presented as a chi-square of 0.0268, indicating that the generalized linear regression model is statistically significant at the α = 0.05. This suggests that at least one of the independent variables has a statistically significant association with the dependent variable.
During the later phase of the pandemic (2022∼2023), the 30-day hospital readmission rate decreased significantly (OR = 0.80, P = .02), indicating a lower risk of readmission than in the earlier phase of the pandemic. Male patients were more likely to be readmitted than female patients (OR = 1.28, P = .01). Additionally, patients with a higher respiratory rate were more likely to be readmitted (OR = 1.04, P = .034). However, age (P = .92), BMI (P = .12), and blood pressure (P > .1) did not reach statistical significance. Furthermore, antithrombotic agents, lipid-lowering drugs, antihypertensive agents, and antidiabetic medications were not significantly associated with the risk of readmission risk (P > .05).
A Declining Trend in Readmission Rates, Decreasing From 11.23% in 2020 to 8.89% in 2022

Abbreviations: Std. err., standard error; CI, confidence interval.
A Two-Sample Test of Proportions was Conducted to Compare 30-Day Readmission Rates Early (2020∼2021) and Late (2022∼2023) the Pandemic
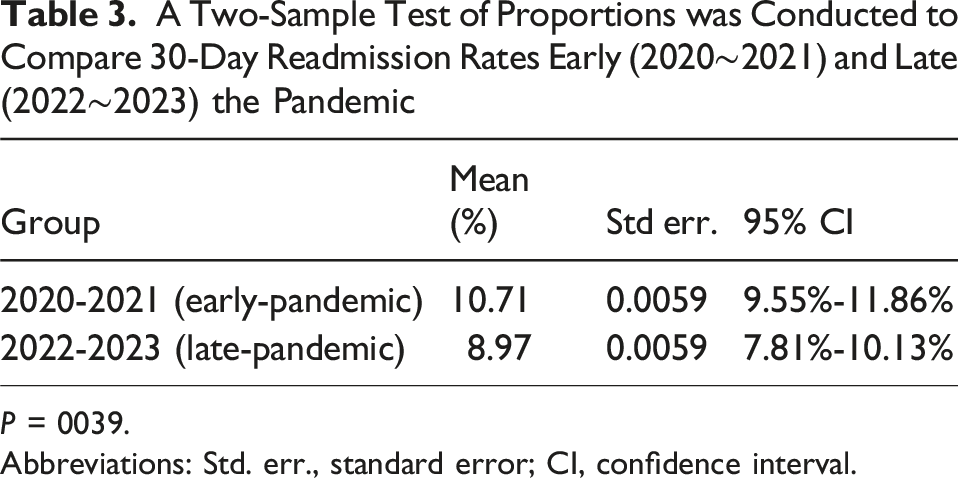
P = 0039.
Abbreviations: Std. err., standard error; CI, confidence interval.
In 2023, the readmission rate increased slightly to 9.05%, although it remained lower than the rates reported in 2020 and 2021. More research is needed to determine whether this change was influenced by the lingering effects of COVID-19, changes in patient characteristics, or modifications in healthcare policy. We performed a sensitivity analysis by excluding patients whose readmissions were likely related to planned procedures (for example, staged interventions). The results remained consistent with the primary analysis, with the late-pandemic period showing a significantly lower odds of 30-day readmission compared to the early-pandemic period (adjusted OR = 0.81, P = .024). We further evaluated whether the effect of the pandemic period on readmission risk differed by sex by adding an interaction term (sex × pandemic period) to the generalized linear regression model. The interaction term was not statistically significant (P = .41), indicating a similar reduction in the risk of readmission for both male and female patients.
We applied a Bonferroni correction considering the number of secondary comparisons in our analyzes (n = 4). After adjustment, the P-value of the difference in 30-day readmission rates between the early pandemic (2020-2021) and late pandemic (2022-2023) periods increased to p_adj = 0.156, which did not meet the conventional significance threshold of 0.05. However, the downward trend across all study years (2020: 11.23%, 2021: 10.11%, 2022: 8.89%, 2023: 9.05%) remained consistent and may indicate a clinically relevant improvement in post-discharge care during the late pandemic.
Discussion
The lower risk of 30-day readmission in the late pandemic period can be attributed to several improvements in medical management strategies. Advancements in stroke treatment and refinement of mechanical thrombectomy and thrombolysis techniques likely contributed to a reduction in stroke recurrence and subsequent hospital readmissions. 18 Enhanced hospital management and improved hospital care, including early rehabilitation, blood pressure control, and metabolic regulation, may have helped reduce post-discharge complications and the need for readmission. The increase in telemedicine utilization and the expansion of telehealth services allowed patients to seek outpatient consultations or virtual follow-ups, potentially preventing unnecessary hospitalizations.19,20 Changes in patient behavior in the later stages of the pandemic led to a greater preference for home care or outpatient treatment. The increase in community care and home rehabilitation services may have contributed to a reduction in hospitalizations related to rehabilitation needs. 21
The additional sensitivity analysis, which excluded patients with planned readmissions, confirmed the robustness of the observed association, with the late pandemic period remaining significantly associated with a reduced risk of readmission at 30 days. Furthermore, our assessment of a potential sex × time period did not reveal a statistically significant modification of the effect, suggesting that the decline in readmission rates was consistent between sexes.
Although causality cannot be inferred from our retrospective observational design, the concurrent increase in post-discharge care resources during the late pandemic period supports the plausibility of a link between enhanced care and reduced readmissions. Specifically, telemedicine follow-up utilization increased by 13 percentage points, structured rehabilitation participation increased by 7 percentage points, and home care referrals increased by 4 percentage points compared to the early pandemic period. These system-level changes may have provided more accessible and timely support for patients, potentially mitigating preventable readmissions. However, since these postdischarge care data are aggregate and not linked to individual patient outcomes, their contribution should be interpreted with caution.
Male patients had a higher likelihood of readmission than female patients. This discrepancy may be associated with poorer lifestyle habits, a greater burden of comorbidities, and lower adherence to medications among men. Patients with higher respiratory rates were also more likely to be readmitted. A higher respiratory rate may indicate impaired cardiac or pulmonary function, resulting in a higher risk of readmission. Although respiratory rate was found to be a statistically significant predictor of 30-day readmission (OR = 1.04, P = .034), the magnitude of the effect was modest. The clinical relevance of such a small increase in odds per unit increase in respiratory rate should be interpreted with caution. This result may reflect underlying cardiorespiratory stress, but further research is needed to determine whether it has meaningful implications for clinical decision making or patient monitoring. Age, BMI, blood pressure, and pulse rate were not significantly associated with the risk of readmission at 30 days. This suggests that short-term readmission outcomes may be less influenced by these physiological parameters and may require longer-term follow-up (for example, readmission rates at 90 or 180 days) to identify trends. Similarly, commonly used cardiovascular and metabolic medications (eg, antithrombotic agents, lipid-lowering drugs, antihypertensive agents, and antidiabetic medications) did not have a statistically significant effect (P > .05) on readmission rates at 30 days. These results indicate that, within the context of this dataset, the 30-day readmission rate was not significantly influenced by the use of commonly prescribed cardiovascular and metabolic medications. However, these findings should be approached with caution in light of potential confounders and unmeasured variables, such as adherence to medications.
The implementation of telemedicine during the early pandemic may have contributed to lower readmission rates. Continued online outpatient services and community education programs are recommended to ensure that patients receive adequate care. Expanding remote monitoring for high-risk patients, including blood pressure monitoring and home rehabilitation programs, could further reduce readmission risks.
Strengthening case management would ensure timely medical access for high-risk patients. Identifying high-risk patients (eg, those with a history of multiple readmissions) and ensuring intensive follow-up and monitoring can help mitigate readmission risks. The development of a proactive post-discharge tracking system is recommended to ensure that patients receive timely medical care, thus preventing delayed treatment due to fear of infection or resource limitations. There are several potential factors contributing to the slight increase in the readmission rate in 2023. During the pandemic, the redistribution of healthcare resources may have impacted rehabilitation and follow-up care for patients with chronic diseases. In terms of patient characteristics, if hospitalized patients in 2023 were older or had a greater burden of comorbidities, their readmission risk may have been inherently higher. Modifications in healthcare policies, if discharge criteria became more stringent in 2023, leading to early discharge of high-risk patients, could have contributed to an increase in 30-day readmission rates. During the early phase of the COVID-19 pandemic in the United States, acute complications occurring during index hospitalization, such as acute coronary syndrome, congestive heart failure, acute kidney injury, the need for mechanical ventilation and renal replacement therapy, were associated with an increased risk of 30-day readmission among patients with COVID-19. 22 These findings emphasize the importance of ongoing monitoring of readmission trends and the need for targeted interventions to optimize post-discharge care, particularly for high-risk patients.
This study was conducted as a retrospective cohort analysis in a single tertiary medical center. As such, findings may be influenced by regional-specific healthcare policies, resource allocation, and institutional care models. The generalizability of the results to other populations or healthcare settings is limited. Although the study was adjusted for several demographic characteristics, vital signs, and medication variables, other potentially impotent clinical variables - such as stroke subtype (ischemic vs hemorrhagic) and neurological severity scores (eg, NIHSS) - were not available in our data set. This limitation is due to the retrospective nature of the study and the fact that the hospital’s electronic health record system did not record these variables consistently and systematically throughout the study period. The absence of data on Adherence to medication, dosage, and combination therapy of medications prevented a possible assessment of the impact of these pharmacotherapy characteristics on the risk of readmission. Another limitation is that no prestudy sample size or power analysis was conducted. This was because the study included all eligible patients within the defined time frame, rather than relying on a predetermined sample. Although this approach maximizes case inclusion and statistical representativeness for the study setting, it can limit the ability to detect small effect sizes in certain subgroups.
Furthermore, individual-level social determinants of health, such as access to rehabilitation services, home care availability, and socoeconomic status, were not captured in the data set. These unmeasured factors may have introduced residual confounding. We recommend that future research link hospital-based data sets with public health or national insurance databases to allow a more comprehensive adjustment for these social determinants.
Another limitation is the absence of individual-level COVID-19 infection status, as SARS-CoV-2 test results were not consistently documented during portions of the study period. This precluded a direct assessment of the impact of COVID-19 infection on readmission risk. Future work should integrate infectious disease surveillance data to address this gap.
Although the study stratified patients according to the pandemic timeline, the exclusion of patients deceased at discharge or discharged in critical condition may have introduced selection bias. Furthermore, cases with incomplete data were excluded to ensure analytical quality, although the proportion was negligible. Lastly, the single-center design reflects region-specific clinical practices and healthcare infrastructure, limiting the generalizability of the findings.
Conclusion
This study analyzed the key factors that influence hospital readmission at 30 days among stroke patients. The results indicated that in the late pandemic period (2022∼2023), the readmission rate at 30 days was significantly lower than in the early pandemic period (2020∼2021). This finding may be associated with improvements in medical management during the early pandemic phase may have contributed to a reduced risk of readmission. Furthermore, male patients had a higher risk of readmission, highlighting the need for enhanced care strategies for this group. More detailed analysis of long-term readmission trends should be performed, as this study focused on 30-day readmission rates. Future research should monitor readmission trends over 60-day and 90-day periods to determine whether the observed reduction in readmission rates is a short-term phenomenon or a genuine improvement in patient health outcomes.
Footnotes
Acknowledgements
The authors would like to thank all the participating physicians and administrative and academic staff for taking part in the study. Furthermore, the authors would like to acknowledge the contributions of the members of the research team, as well as of the staff of the Department of Neurology, Department of Nuclear Medicine, Changhua Christian Hospital, Changhua, Taiwan, and the Department of Applied Mathematics, National Chung Hsing University, Taichung.
Ethics Approval
This study was conducted according to the Institutional Review Board (IRB) of Changhua Christian Hospital (Approval Number: 241110).
Consent to Participate
As a retrospective study, all patient data were deidentified and individual informed consent was waived by the IRB to ensure patient privacy and compliance with ethical standards.
Authors’ Contributions
Hsu-Tung Chang: Contributed to the conception and design of the study, coordinated the acquisition of clinical data, and participated in the interpretation of the results. Drafted the initial version of the manuscript.
Chih-Ming Lin: Assisted in the design of the study, provided expertise in neurological aspects of stroke care, and contributed to the interpretation of clinical implications. Critically reviewed and revised the manuscript for important intellectual content.
Chun-Yi Lin: Participated in data acquisition and validation, contributed to data interpretation, and assisted in drafting the results and discussion sections.
Yin-Tzer Shih: Conception of the general concept of the study, supervised data analysis, and contributed to the statistical methodology. Oversaw the entire research process, provided critical review of the manuscript, and approved the final version for submission.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Science and Technology Council (NSTC), Taiwan (NSTC 113-2115-M-005-004).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The supporting data for this study are available from the corresponding author upon reasonable request.