
Abstract
Background and purpose
Nationwide data on childhood stroke prevalence and incidence in Mainland China are unavailable now. We aim to investigate the prevalence and incidence of childhood arterial ischaemic stroke and haemorrhagic stroke in China nationwide.
Methods
In 2013, we implemented a nationally representative, door-to-door epidemiological survey on stroke in China through a complex, multistage, probability sampling design. A post-hoc subgroup analysis was conducted to examine both the crude point prevalence and annual incidence of childhood stroke. Due to the small case number, the Poisson distribution was used to estimate the 95% confidence intervals (CIs) for the crude rates.
Results
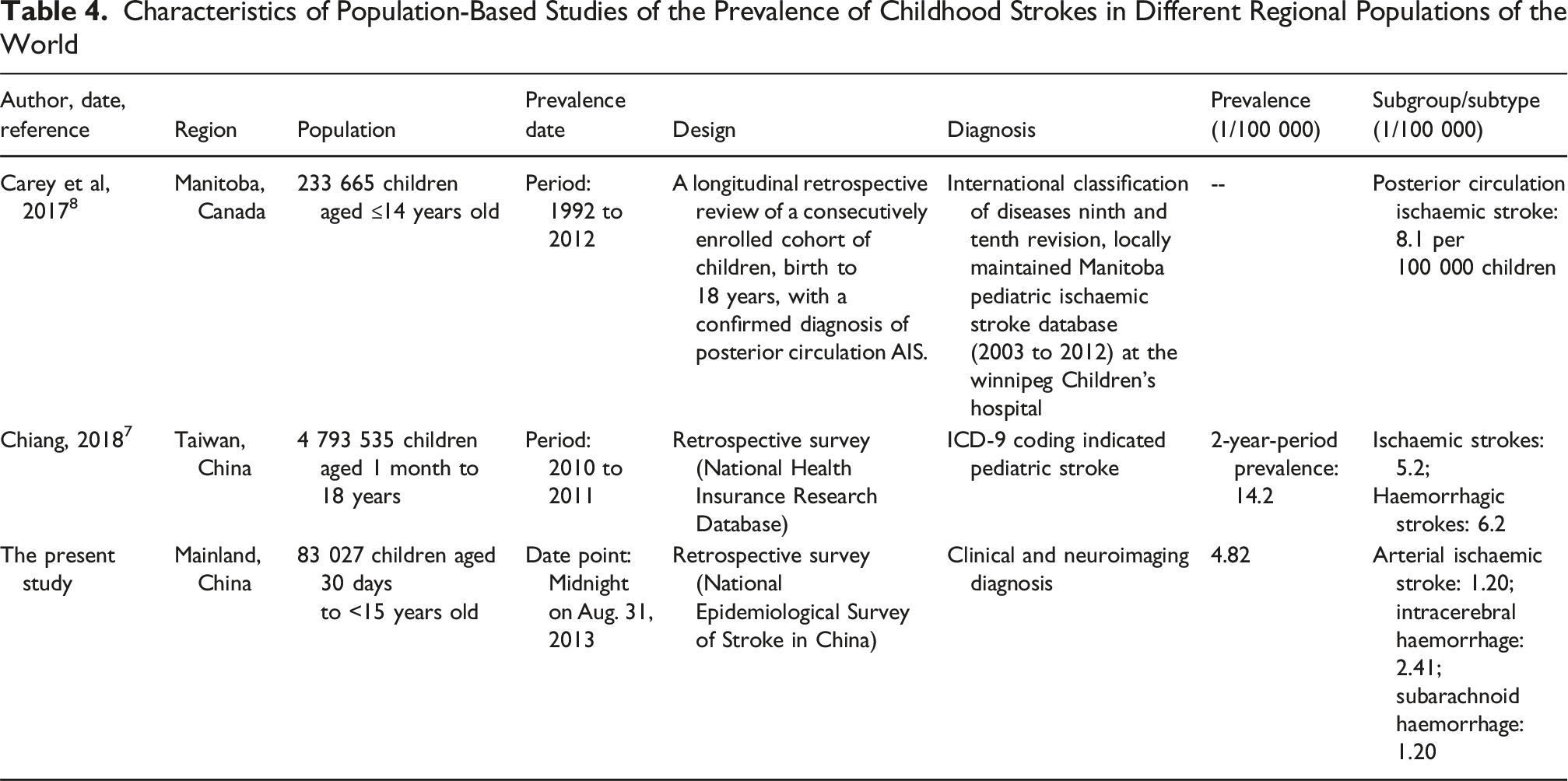
In this survey, only 4 strokes were identified. The crude point prevalence of childhood stroke was 4.82 (95% CI: 1.31-12.34) per 100 000 children in China; 4.51 (95% CI: 0.55-16.29) per 100 000 boys, and 5.17 (95% CI: 0.63-18.69) per 100 000 girls. Haemorrhagic stroke prevalence was 3.61 (95% CI: 0.75-10.56) vs 1.20 (95% CI: 0.03-6.71) per 100 000 children for arterial ischaemic stroke. The crude annual incidence of childhood stroke was 2.34 (95% CI: 0.28-8.45) per 100 000 children in China; 5.01 (95% CI: 0.60-18.10) per 100 000 girls. The crude annual incidences of both arterial ischaemic stroke and intracerebral haemorrhage were the same at 1.17 (95% CI: 0.03-6.52) per 100 000 children.
Conclusions
The point prevalence and annual incidence estimates of childhood stroke were 4.82 and 2.34 per 100 000 children in China, respectively. Chinese children may have more prevalent cases of haemorrhagic than arterial ischaemic strokes.
Introduction
Childhood stroke is a neurologic disease characterized by higher mortality and disability rates in children, which can cause sensorimotor disorders, language impairment, intellectual disabilities, behavioral problems, and epilepsy. The concerns about the epidemiology of childhood stroke began in the 1970s. Early retrospective surveys found that the incidence of childhood stroke was 3.1 per 100 000 children per year (January 1, 1963, to December 31, 1963) in Iceland and 2.5 per 100 000 children per year (1965-1974) in the United States, respectively.1,2 However, the incidence rate of childhood stroke in Dijon, France, was as high as 13.0 per 100 000 children per year (January 1, 1985 to December 31, 1993) in a prospective study. 3 With the improvement of imaging diagnosis, acute and critical care, and treatment levels, both the incidence and prevalence of stroke in children have increased. Globally, the incident strokes and prevalent strokes among children increased by 18.51% and 31.97%, respectively, from 1990-2019. 4 Correspondingly, age-standardized incidence and prevalence rates increased from 18.02 per 100 000 children in 1990 to 19.11 per 100 000 in 2019, from 68.88 to 100 000 children in 1990 to 81.35 per 100 000 in 2019, respectively. 4 Moreover, the age-standardized incidence rates in the low, low-middle, and middle sociodemographic index (SDI) regions were 24.10 (95% Uncertainty Interval: 16.59-33.77), 19.97 (13.68-28.30), and 18.14 (12.43-25.82) per 100 000 children in 2019, respectively. 4
In the Hong Kong Special Administrative Region, China, the estimated incidence of pediatric stroke between 1998 and 2001 was 2.1 cases per 100 000 children per year.5,6 In Taiwan, China, the incidence of pediatric stroke in 2011 was 6.4 cases per 100 000 children per year; 2.3 per 100 000 children per year for ischaemic strokes, and 3.2 per 100 000 children per year for haemorrhagic strokes, whereas the 2-year-period prevalence of pediatric stroke is 14.2 cases per 100 000 children; 5.2 per 100 000 children per year for ischaemic strokes and 6.2 per100 000 children per year for haemorrhagic strokes.5,7 However, nationwide data on childhood stroke prevalence and incidence in Mainland China are unavailable now. In addition, there are still no reports on the point prevalence in a lifetime of childhood stroke, except for the period prevalence of childhood stroke, so far.7,8 China is a developing country with the fastest economic development, whose population accounts for one-fifth of the world’s population. The lack of data on childhood stroke in Mainland China has severely affected the representativeness and applicability of global stroke statistics. The limited regional data currently available from Hong Kong and Taiwan are insufficient to inform national policy-making for pediatric stroke prevention and control strategies. Given the critical importance of evidence-based decision-making, there is an urgent need to conduct comprehensive research on childhood stroke incidence and management in Mainland China. In this study, we investigated the prevalence and incidence rates of arterial ischaemic stroke and haemorrhagic stroke in children in China using data from a nationally representative cross-sectional sampling survey on all-age strokes.9,10
Methods
Study Design
We had conducted a nationally representative cross-sectional sampling survey on all-age strokes and transient ischaemic attacks (TIA) in mainland China from September 1 to December 31, 2013, which was described in detail in previous studies.9-12 We had used a complex, multistage probability sampling design to define the sampling frame and the participants; namely, 2010 Chinese population census data and probability proportionate to population size (PPS) sampling were used to select 64 urban and 93 rural areas from 31 provinces of China (see Figure 1).9-12 The sampling frame for this survey was the National Disease Surveillance Points (DSP) System, which may represent the 2010 China national census data concerning geographical distribution, social status, and economic status. The sample size for this survey was calculated at approximately 600 000 subjects based on a 1% stroke prevalence, with a two-sided 95% CI, a design effect (deff) value of 5, and a relative error of 15%, according to the complex sampling formula. Distribution of Survey Sites in 31 Provinces of China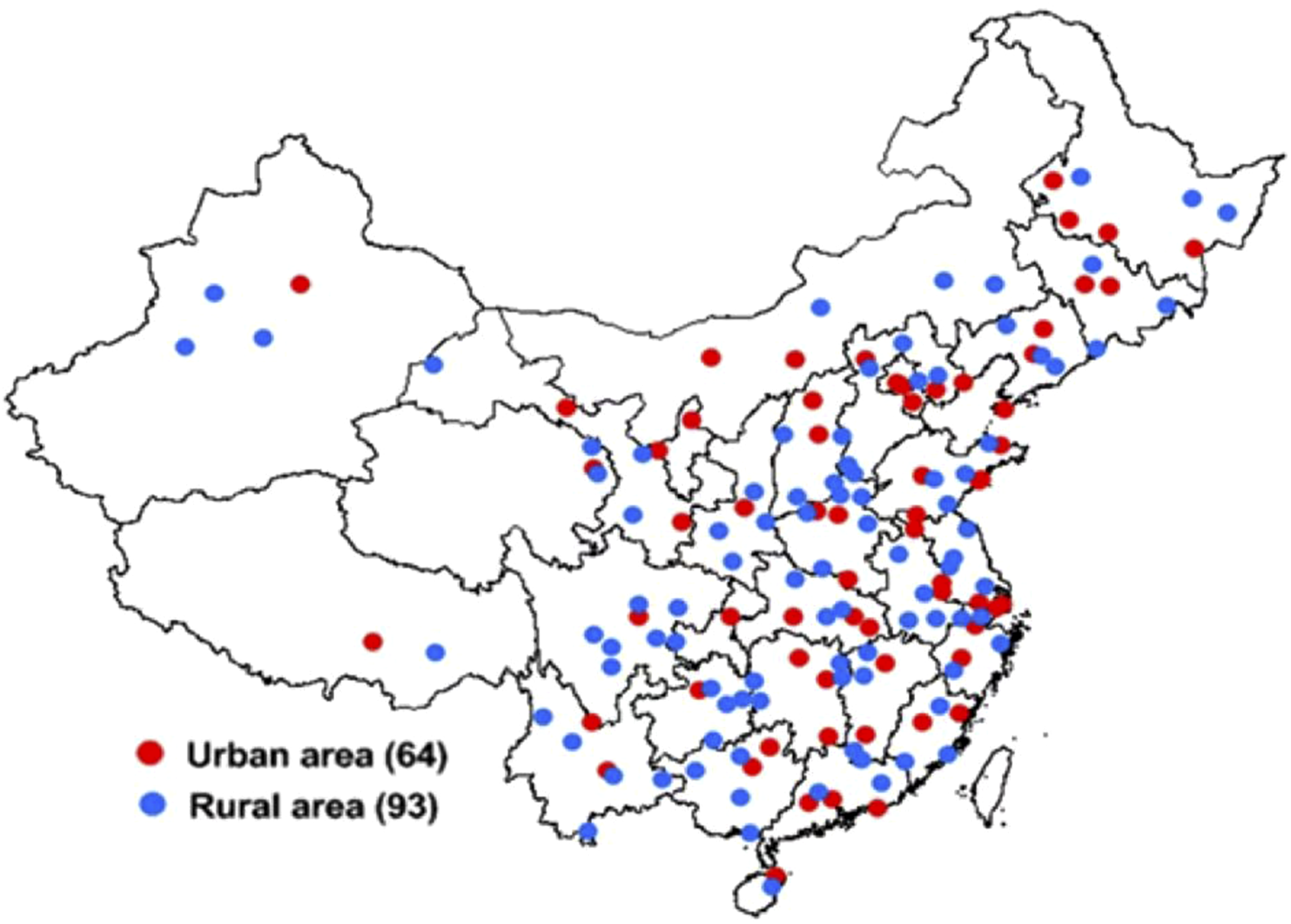
Case Ascertainment
In this survey, CDC investigators conducted household visits to collect signed informed consent forms from each family in the sample population. During these visits, they also completed a preliminary screening form. This form included key information such as basic family details, any deaths within the household since January 1, 2012, and indicators of positive stroke symptoms. Participants who had positive stroke symptoms were invited to see a neurologist in a town/village clinic. Diagnoses of definite and probable stroke and TIAs were determined after the neurologist completed a physical examination and reviewed previous medical documents, including an identity card or household register, the medical history of the individual with stroke or TIA, and computed tomography (CT) /magnetic resonance imaging (MRI) scans. The validated verbal autopsy technique involving household members of people who died within the 12 months preceding the survey was used to identify stroke as a possible cause of death.
Data Collection
For all the participants, self-reported information on age, sex, ethnicity, and the medical history of the individuals with stroke/transient ischaemic attacks was also obtained and reviewed.9-12 Each stroke/ or transient ischaemic attack event experienced by a participant in the study was meticulously documented. The onset timing, diagnosis, and clinical assessment of each event were carefully tracked throughout the participant’s lifetime. For all definite and probable cases with strokes/transient ischaemic attacks, physical disabilities were assessed by a modified Rankin Scale. BP was measured twice, respectively in the right and left arms with 40%-50% BP cuff width of the arm circumference in the seated position using an Intellisense® electronic blood pressure monitor (Omron HEM-7200, Omron (China) Co, Ltd, Dalian City, Liaoning Province, China) after the patient had been seated for 5 min.
Quality Assurance
The survey process was meticulously managed through a comprehensive quality control framework. This included rigorous oversight of all preparatory activities, meticulous fieldwork, and thorough data processing procedures. To ensure the highest standards of data integrity, specialized quality assurance measures were implemented at every stage of the project.9-12 In this survey, we implemented cluster sampling and prevented the replacement of selected participants to control both sampling errors and response bias. Additionally, 2 survey points were excluded due to non-compliance with study design requirements (see Figure 2). In this survey, 596 536 and 595 711 individuals for the analyses of all-age prevalence and incidence of stroke /transient ischaemic attacks were ultimately included, respectively, with a response rate of approximately 81%.
12
Flowchart for Childhood Stroke Case Ascertainment. Note: DSP, Disease Surveillance Points; CDC, Centers for Disease Control and Prevention
Definitions of Stroke and TIA
In this epidemiological study, the minimum criterion for definite or probable stroke was evidence of a sudden or rapid onset of neurological symptoms lasting for >24 h or leading to death without evidence of a nonstroke cause.9-12 Any patients with nervous system abnormalities induced by trauma, metabolic disorders, tumours, or central nervous system infections were excluded. Whenever brain imaging was used within the first week of stroke onset and the imaging results were available for review by the study neurologist, the pathological type of stroke was classified into 4 major categories: subarachnoid haemorrhage (SAH; only lumbar puncture was allowed for the diagnosis of SAH); intracerebral haemorrhage (ICH); and arterial ischaemic stroke (AIS); and stroke of an undetermined pathological type in the case of stroke patients with no brain imaging performed within the first week of stroke onset or when the imaging results were not available for review by the study neurologist.
A TIA was originally defined as the sudden onset of a focal neurologic symptom or sign lasting less than 24 h, presumably brought on by a transient decrease in blood supply that rendered the brain ischaemic in the area producing the symptom.11,12
Specification of a Post-hoc Subgroup Analysis of Childhood Strokes
A post-hoc subgroup analysis of childhood strokes was performed in this study. The participants were children aged between 30 days and 14 years old whose parents or guardians had lived in the defined areas for at least 6 months during the year preceding the survey. Based on the exclusion criteria of stroke and the pathogenesis of cerebral venous sinus thrombosis (CVST) in children, the CVST subtype was not involved in this survey. For the post-hoc subgroup analyses of childhood stroke prevalence and incidence, a total of 83 027 and 85 461 children aged between 30 days and 14 years were ultimately recruited (see Figure 2).
Statistical Analysis
The sociodemographic characteristics of the study sample were categorized and presented as numbers and crude rates. In this retrospective epidemiological survey, the point prevalence of stroke was defined as the rate of children with stroke before midnight on August 31, 2013, among the survival children from the sampled families, whereas the annual incidence of stroke was defined as the rate of the first stroke between September 1, 2012, and August 31, 2013 among the survival children from the sampled families. The point prevalence and annual incidence of childhood stroke, arterial ischaemic stroke, and haemorrhagic stroke were calculated by subgroups of sex (male/female), place of residence (urban/rural), and geographic location (eastern/central/western China). The 95% confidence intervals (CIs) for all the crude rates of prevalence and incidence were also calculated. The estimation of the 95% CIs for the point prevalence and annual incidence was performed by using the Poisson distribution because the number of cases was small. All statistical calculations were performed using IBM® SPSS® statistics for Windows version 21.0 (IBM Corp, Armonk, NY, USA). P < 0.05 was considered statistically significant.
Results
Characteristics of the Children Aged 30 Days to 14 Years Old From the National Epidemiological Survey of Childhood Arterial Ischaemic and Haemorrhagic Strokes in China

Clinical Characteristics of 4 Cases of Childhood Strokes

Notes: 1. Arterial ischaemic stroke (AIS); intracerebral haemorrhage (ICH); subarachnoid haemorrhage (SAH).
2. Sudden neurological symptoms: + indicates yes, - indicates no.
3. Examinations: Computed tomography/computed tomography angiography (CT/CTA); magnetic resonance imaging/magnetic resonance angiography (MRI/MRA); Digital subtraction angiography (DSA); Lumbar puncture (LP); Transcranial Doppler ultrasound (TCD); Carotid/subclavian artery color ultrasound (CA/SCA CUS); modified Rank Scale (mRS); + indicates yes, - indicates no.
4. Blood pressure (BP).
Prevalence
Prevalence (1/100 000 Person*Lifetime) and Incidence (1/100 000 Person*Years) of Childhood Strokes by Major Subtypes and Different Populations in China

aEstimated by the 2010 Chinese population census data.
bEstimated by the 2020 Chinese population census data.
Incidence
In this survey, the crude annual incidence of childhood stroke was 2.34 (95% CI: 0.28-8.45) per 100 000 children in China; 5.01 (95% CI: 0.60-18.10) per 100 000 girls; 1.39 (95% CI: 0.04-7.75) per 100 000 children with Han ethnicity, and 7.36 (95% CI: 0.19-41.03) per 100 000 children with other ethnicity; 2.62 (95% CI: 0.07-14.60) per 100 000 urban children, and 2.11 (95% CI: 0.05-11.77) per 100 000 rural children; 5.82 (95% CI: 0.70-21.02) per 100 000 children in central China. By major subtypes, the crude annual incidences of both arterial ischaemic stroke and intracerebral haemorrhage were the same as 1.17 (95% CI: 0.03-6.52) per 100 000 children. (see Table 3) According to the above-estimated incidence, there were annually an estimated 5179 (95% CI: 620-18702) childhood strokes in 2010, and 5929 (95% CI: 709-21411) childhood strokes in 2020, respectively, in mainland China.
Discussion
The subgroup analysis of childhood stroke from the national epidemiological survey of stroke in China found, for the first time, that the prevalence of childhood stroke was lower than that previously reported, and the incidence of childhood stroke was close to the global average, compared with previous reports.1-3,6-8,13-29 Among prevalent childhood strokes in China, children may have a greater preponderance of childhood haemorrhagic stroke than arterial ischaemic stroke.
Prevalence
Characteristics of Population-Based Studies of the Prevalence of Childhood Strokes in Different Regional Populations of the World
A prior study showed that the prevalence of IS and HS in children in developed countries significantly decreased from 1990 to 2013, while only a decrease in HS was found in developing countries, with no change in the prevalence of IS. According to the 2013 incidence data, the incidence of IS in developing countries was 4 to 5 times higher than that in developed countries, while the incidence of HS in developing countries was approximately twice that of that in developed countries. 30 Furthermore, the highest age-standardized prevalence rate was observed in low SDI regions, as indicated by the Global Burden of Disease study 2019. In contrast, the most significant increase in age-standardized prevalence rate occurred in high SDI regions. 4 China generally remains a developing country. This survey categorizes China into developed eastern regions, intermediate-developed central regions, and underdeveloped western regions based on their levels of economic development. The childhood stroke cases identified in this survey mainly came from intermediate-developed central regions and underdeveloped western regions. To some extent, this seems to validate the results of the global disease burden.
Incidence
Characteristics of Population-Based Studies of the Incidence of Childhood Strokes in Different Regional Populations of the World

Although most epidemiological surveys of childhood stroke show that boys were at a higher risk of stroke than girls,3,6-8,15,17-21,27 not all research results were consistent with the findings of boys at a higher risk.14,22,28 Although this subgroup analysis of children cannot confirm this. Indeed, it is the case of more strokes in males than females in adults aged ≥20 years in this survey. 10 Black children who constitute a minority in the United States are at a higher risk of stroke than white and Asian children.2,7,15,19 However, in China, compared with Han children, the prevalence and incidence rate of stroke in non-Han children are higher. Although there is no direct evidence, it is speculated that the higher prevalence and incidence of childhood stroke in the minority ethnic groups of the population may be related to their respective socioeconomic status.
A previous prospective study found that the incidence rate of childhood TIA was 0.37 per 100 000 persons per year for children aged 30 days to 18 years in Estonia. 27 Due to the influence of a small sample size, no transient ischaemic attacks were found in this subgroup analysis of the survey. In addition, without a TIA diagnosis certificate issued by the hospital, it is indeed difficult to provide a TIA diagnosis in the population.
Although CVST is classified as a subtype of childhood stroke, most epidemiological investigations of childhood stroke currently do not include this type of childhood stroke. Nonetheless, 2 previous studies found that the incidence rates of CVST were 0.25 and 0.67 per 100 000 children per year.18,27 Except for hereditary or acquired thrombosis, CVST is often associated with infection; however, infection-related stroke diagnosis was excluded from this survey.
Methodological differences and several potential factors may contribute to the differences in childhood stroke incidence across the abovementioned studies, and will be discussed below. First, the age range of children defined is not completely consistent across various studies (see Tables 4 and 5). Second, due to the rarity of pediatric stroke, most epidemiological studies are based on relatively few cases and cannot identify gender or other social demographic differences. Research on childhood stroke also presents unique challenges. A comprehensive insight requires a thorough investigation of multiple dimensions, including the clinical spectrum, etiological factors, pattern analysis, risk assessment, and outcome evaluation. Third, not all higher incidences of childhood stroke were from previous prospective surveys (see Table 5); however, retrospective epidemiological studies may be inaccurate due to recall bias. 33 Fourth, the approaches to case ascertainment in previous studies were indeed inconsistent. A study found that the incidence of childhood ischaemic stroke doubled when assessed through both ICD-9 coding searches and neuroimaging reports. This finding highlights the importance of combining administrative data with clinical imaging in identifying paediatric stroke cases. 26 Fifth, there seems to be no identical definition and diagnosis of pediatric stroke and its risk factors in previous epidemiological surveys. These studies report mainly on AIS and often do not include CVST, transient ischaemic attack, or stroke-like episodes. Some studies include trauma patients, even though these patients have different pathophysiology, treatments, and outcomes. 25 Taking childhood ischaemic stroke as an example, its risk factors are complex, including arteriopathies, cardiac disease, inherited thrombophilia, acquired thrombophilia, sickle cell disease, malignancy, congenital vascular syndromes, inborn errors of metabolism, and rheumatologic disease. Risk factors included sickle cell disease (38%), embolic heart disease (9%), and anemia (3%) in a study. 34 In 2004, Chung and Wong found no cases of SS homozygote sickle cell disease in a Chinese cohort.6 In short, the genetic and environmental factors of the population may also be potential reasons for the difference in the incidence rate of stroke among children in different populations beyond sample size and methodological differences. However, any patients with nervous system abnormalities induced by trauma, metabolic disorders, tumours, or central nervous system infections were excluded from this survey. Therefore, a set of diagnosis and classification criteria for childhood stroke, as well as all-age population-based case ascertainment based on multiple overlapping sources of information from hospitals, outpatient clinics, general practitioners, and death certificates, should be considered before launching a large-scale epidemiological survey of childhood stroke in the future.
Strengths and Limitations of This Survey
The primary strength of this study lies in the robust representativeness of the national stroke epidemiological survey for the Chinese population, ensuring that our findings are broadly generalizable. However, a notable limitation is that these analyses were conducted as a post hoc subgroup investigation based on the national stroke epidemiological survey data. First, the sample size of the subgroup makes it difficult to ensure the validity of the study, subgroup, and subtype analysis.
The widened 95% CIs for prevalence and incidence likely reflect the inherent uncertainty associated with rare events, which can occur in surveys with limited case counts. This pattern is consistent with most previous epidemiological studies. Therefore, the present results of subgroup analysis should be interpreted with caution. Second, there are more children’s guardians’ responses in the survey of childhood stroke. This may lead to underestimating the prevalence and incidence of childhood due to guardians’ response or mild or asymptomatic stroke being omitted. Third, the lack of CT/MRI brain imaging may not only underestimate the stroke prevalence and incidence rates in the population, but also affect the classification of stroke subtypes. Only 4 survival stroke cases were confirmed by CT/MRI imaging in this survey. We cannot exclude the possibility of potential cases in the population that have not been identified due to the lack of brain imaging. However, standardized methodology, diagnostic criteria, case ascertainment, and quality assurance can reduce this bias.
Conclusions
In summary, the point prevalence and annual incidence estimates of childhood stroke were 4.82 and 2.34 per 100 000 children in China, respectively. Chinese children may have more prevalent cases of haemorrhagic than arterial ischaemic strokes. The low incidence rate of rare events like childhood stroke may imply it is necessary to build a Collaboration network of both regional and global stroke registries for childhood stroke research in the future. Based on the Chinese children’s stroke registry, in the future, the registry may help us better identify genetic or acquired risk factors for childhood cerebral arteriopathy to bridge the gaps in childhood stroke research between regions.
Footnotes
Acknowledgements
We thank Drs. Shengping Wu, Hongmei Liu, and Ms Jie Fu from the Beijing Neurosurgical Institute, China; Drs. Liangyou Wu and Lingzhi Kong from the Ministry of Health, China; Drs. Xiaofeng Liang, Limin Wang, and Linhong Wang from the Chinese Center for Disease Control and Prevention (CDC). We also thank all 383 neurologists and 1626 CDC staff from 31 provinces who worked very hard to ensure the accuracy of the data, and all the study participants for their participation and contribution.
Ethical Considerations
This study was approved by the Ethics Committee of the Beijing Tiantan Hospital affiliated with the Capital Medical University (Ethic ID: KY2013-006-01).
Consent to Participate
Informed consent was obtained from all participants or their caregivers. This study was performed per the Declaration of Helsinki.
Author Contributions
Conceptualization: Bin Jiang, Wenzhi Wang
Data curation: Bin Jiang, Haixin Sun, Xiaojuan Ru, Dongling Sun, Siqi Ge, Wenzhi Wang
Formal analysis: Bin Jiang, Haixin Sun, Xiaojuan Ru, Dongling Sun, Siqi Ge, Wenzhi Wang
Funding acquisition: Bin Jiang, Wenzhi Wang
Investigation: Bin Jiang, Wenzhi Wang
Methodology: Bin Jiang, Wenzhi Wang
Project administration: Bin Jiang, Wenzhi Wang
Resources: Bin Jiang, Wenzhi Wang
Software: Bin Jiang
Supervision: Bin Jiang, Wenzhi Wang
Validation: Bin Jiang, Wenzhi Wang
Visualization: Bin Jiang, Wenzhi Wang
Writing-original draft: Bin Jiang
Writing-review & editing: Bin Jiang, Wenzhi Wang
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Ministry of Science and Technology and the Ministry of Health of the People’s Republic of China under grant No. 2011BAI08B01 of the National Key Technology R&D Program, and partially by the National Natural Science Foundation of China under grant No. 81571130090. The funders had no role in the study design, data collection, analysis, interpretation, or writing of the report. The project investigators were responsible for the decision to submit the report for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data relevant to the study are included in the article. No additional data are available.