
Abstract
Background
Mild acute ischemic stroke (AIS), characterized by a National Institutes of Health Stroke Scale (NIHSS) score of 5 or less, can lead to significant long-term disabilities. Reperfusion therapies like intravenous thrombolysis (IVT) and endovascular thrombectomy (EVT) are commonly used in AIS, but their efficacy and safety in mild stroke cases remain unclear.
Objectives
This meta-analysis aims to clarify the prevalence of mild AIS and evaluate the outcomes of reperfusion therapy, specifically IVT and EVT, in terms of functional recovery, mortality, stroke recurrence, and adverse events such as symptomatic intracerebral hemorrhage (sICH), intracerebral hemorrhage (ICH), and early neurological deterioration (END).
Design
A meta-analysis was conducted following PRISMA guidelines to combine and assess the results of independent studies examining the use of reperfusion therapies in patients with mild AIS.
Data Sources and Methods
A systematic search of PubMed, Embase, and Cochrane databases was performed. Studies assessing mild AIS prevalence and the outcomes of reperfusion therapy were included. Random effects modelling was applied to evaluate associations between reperfusion therapy and clinical outcomes at 90 days.
Results
Fifty-six studies, including 474 778 patients, were analyzed. The pooled prevalence of mild stroke was 54% among all AIS cases, 29% in IVT-treated patients, and 9% in EVT-treated patients. Reperfusion therapy was associated with significantly increased odds of sICH (OR 2.92), ICH (OR 2.20), and END (OR 2.37). However, no significant association was found with excellent functional outcomes (OR 0.93), good functional outcomes (OR 0.91), mortality (OR 1.14), or stroke recurrence (OR 0.93) at 90 days. Variations were observed between different reperfusion subgroups.
Conclusion
Mild AIS is prevalent, and reperfusion therapy in these cases is linked to higher rates of adverse events without a clear benefit in functional outcomes or mortality. These findings support the need for selective reperfusion therapy in mild stroke patients. The proposed SAFE framework—Selective use of IVT, Assessment of individual factors, Focus on EVT for large vessel occlusion (LVO), and Establishment of region-specific guidelines—may help guide clinical decisions. Further research should refine patient selection criteria and explore adjunctive therapies.
Plain language summary
Mild strokes, which affect millions of people worldwide, are often less severe but can still cause long-term disabilities. This study examined treatments commonly used for stroke patients, such as intravenous thrombolysis (IVT) and endovascular thrombectomy (EVT). These treatments aim to restore blood flow to the brain after a stroke, but their effectiveness in mild stroke cases is not well understood. The study analyzed data from 56 studies involving nearly 475,000 stroke patients and found that mild strokes accounted for over half of all stroke cases. However, only a small percentage of patients with mild strokes received IVT (29%) or EVT (9%). The results showed that these treatments increased the risk of serious complications, such as brain bleeding and early neurological decline. Despite these risks, the treatments did not significantly improve patients’ chances of full recovery, reduce the risk of death, or prevent future strokes. Based on these findings, the authors propose a decision-making framework called “SAFE” for treating mild strokes. This framework emphasizes selective use of IVT based on patient-specific risks, assessment of EVT only for certain severe cases, focus on individual patient profiles, and ensuring adherence to regional guidelines. The study underscores the urgent need for more research to identify safer and more effective treatments for mild strokes.
Keywords
Introduction
Mild acute ischemic stroke (AIS), typically defined as a National Institutes of Health Stroke Scale (NIHSS) score of 5 or less, 1 is increasingly recognized for its potential to cause significant long-term impacts,2–6 such as impaired executive function, reduced mobility, and diminished quality of life. Despite these consequences, the prevalence of mild stroke within the broader AIS patient population remains underexplored. Individual studies have provided some data,7–9 but a comprehensive pooled analysis is needed to better understand the burden of mild stroke and its implications for public health.
The prevalence of mild stroke among patients undergoing intravenous thrombolysis (IVT) and endovascular thrombectomy (EVT) is particularly important for informing treatment strategies and improving the uptake of reperfusion therapies. 10 Although previous meta-analyses have examined the effectiveness of IVT11–15 and EVT,16–25 they often suffer from inconsistencies, such as varying definitions of mild stroke and a lack of standardized outcome measures. Furthermore, there is a notable gap in pooled data regarding the outcomes of bridging therapy (BT) in mild-stroke patients.26–29
Understanding the effects of reperfusion therapies in mild stroke is crucial for ensuring appropriate treatment administration. This study aims to fill these gaps by determining the prevalence of mild stroke among AIS patients and evaluating the outcomes of those treated with reperfusion therapies. By addressing these issues, the study seeks to provide a clearer picture of the implications of mild stroke and inform clinical decision-making regarding the use of reperfusion therapies.
Objectives
This study aims to determine the prevalence of mild stroke in AIS patients among those undergoing IVT and EVT treatment through a meta-analysis. Additionally, it aims to explore the association of clinical outcomes among mild AIS patients. The research will address the following questions: 2a. Prevalence 2.1. What is the overall prevalence of mild stroke among AIS patients? 2.2. What is the overall prevalence of mild stroke among IVT-treated AIS patients? 2.3. What is the overall prevalence of mild stroke among EVT-treated AIS patients? 2b. Clinical Outcomes (90-Day Functional Outcome) 2.4. Is reperfusion in mild AIS patients associated with good 90-day functional outcomes? 2c. Mortality and Adverse Outcomes (sICH, END, and Stroke Recurrence) 2.5. Is reperfusion in mild AIS patients associated with 90-day mortality? 2.6. Is reperfusion in mild AIS patients associated with symptomatic intracerebral hemorrhage (sICH)? 2.7. Is reperfusion in mild AIS patients associated with intracerebral hemorrhage (ICH)? 2.8. Is reperfusion in mild AIS patients associated with early neurological deterioration (END)? 2.9. Is reperfusion in mild AIS patients associated with stroke reoccurrence?
Each research question targets significant clinical and public health concerns, such as optimizing treatment strategies, minimizing adverse outcomes, and improving the quality of life in mild stroke patients. By addressing these questions, the study aims to provide a comprehensive understanding of the current treatment landscape and guide future clinical practices and policies.
Materials and methods
Literature search: study Identification and selection
Studies from January 1, 2005, to May 31, 2024, were sourced from online databases, including PubMed, Embase, and Cochrane. A comprehensive search strategy was used, with relevant terms including “Mild Stroke”, “Minor Stroke”, “NIHSS”, and “Ischemic Stroke”, along with terms such as “Reperfusion”, “Thrombolysis”, “Endovascular Procedures”, “Clinical Outcome”, “Prognosis” and “Prevalence.” The supplementary information provides a detailed overview of the search strategy ( The Preferred reporting System for systematic reviews and meta-analyses (PRISMA) flowchart showing the studies included in the meta-analysis. Abbreviations: N = number of studies, n = total number of patients, NIHSS = National Institute of Health Stroke Scale, AIS = Acute Ischemic Stroke, mRS = modified Rankin Scale, sICH = symptomatic Intracerebral Hemorrhage, ICH = Intracerebral Hemorrhage, END = Early Neurological Deterioration.
Inclusion and exclusion criteria
Studies included in this meta-analysis were selected based on the following inclusion criteria: (a) Participants were diagnosed with AIS confirmed through appropriate imaging methods to ensure accurate diagnosis. (b) Mild stroke was defined as having a NIHSS score of 5 or less, a standard definition that aligns with current clinical guidelines and ensures consistent categorization across studies. (c) The study provided data on the prevalence of mild stroke and/or outcomes following IVT and/or EVT treatment. This focus allows for a comprehensive understanding of treatment impacts. (d) There was a comparison group included in reperfusion outcome studies to facilitate the assessment of treatment efficacy and safety. (e) Patients treated were candidates for reperfusion therapy, ensuring that the data reflects real-world clinical decision-making. (f) The treatment timeframe for reperfusion was restricted to IVT within 4.5 hours and EVT within 24 hours of stroke onset, reflecting current clinical practice guidelines, which are based on evidence for optimal treatment windows. (g) Studies conducted between January 2005 and May 2024 were considered for mild stroke prevalence and IVT treatment, while those between January 2013 and May 2024 were considered for EVT treatment. These periods were chosen to capture the most relevant and recent data, reflecting advancements in treatment protocols (reperfusion therapy practices) over time. (h) Only studies with a prospective design were included to ensure high-quality, forward-looking data collection methodologies. (i) Studies were required to be of good quality, defined as having a minimum of 20 patients in each study group to ensure statistical power and reliability of the findings.
Exclusion criteria included: (a) Studies that did not focus on AIS or reperfusion therapies, as these would not provide relevant data for the research questions. (b) Studies involving pediatric populations (age ≤18 years) as they present different clinical profiles and treatment considerations. (c) Systematic reviews, meta-analyses, case reports, and editorials were excluded to focus on primary research data.
Data extraction
Clinical characteristics of studies selected for the meta-analysis of mild stroke prevalence and outcomes.

Abbreviations: AIS = Acute Ischemic Stroke, RT = Reperfusion Therapy, n = number of patients, % = percentage, SD = Standard Deviation, NIHSS = National Institute of Health Stroke Scale, sICH = symptomatic Intracerebral Hemorrhage, ICH = Intracranial Hemorrhage, END = Early Neurological Deterioration, NA = Not Applicable (Study does not report on this data), NR = Not Recorded, IVT = Intravenous Thrombolysis, EVT = Endovascular Thrombectomy, CT = Computed Tomography, MRI = Magnetic Resonance Imaging, ECASS II = European Cooperative Acute Stroke Study II, ECASS III = European Cooperative Acute Stroke Study III, IST-3 = Third International Stroke Trial, NINDIS = National Institute of Neurological Disorders and Stroke, PROACT II = Prolyse in Acute Cerebral Thromboembolism Trial two, SITS-MOST = Safe Implementation of Thrombolysis in Stroke Monitoring Study, BT = Bridging Therapy.
Note: *Study Type: Retrospective analysis of prospectively collected data is considered ‘Prospective’.
aRepeat Study: Data for different hypotheses available in study.
bNon-disabling only: Studies focusing on only non-disabling mild strokes treated with intravenous thrombolysis.
cLVO only: Studies focusing on only large vessel occlusion (LVO) mild stroke patients treated with intravenous thrombolysis.
Methodology quality assessment of included studies
The methodology quality assessment was performed using the modified Jaded analysis (MJA). Risk funding bias was noted based on conflicts of interest and author funding disclosures. Refer to the supplementary information for this data (Supplemental Tables 4 and 5).
Statistical analysis
Analysis was performed using STAT v 13.0 (StatCorp, College Station, USA). Baseline characteristics such as medians and interquartile ranges were converted to means and standard deviations to standardize data presentation and enhance comparability across studies. 78
Prevalence estimation
To assess the prevalence of mild acute ischemic stroke (AIS) among various patient groups, we utilized the ‘Metaprop' command in STATA. This command allows for the calculation of pooled prevalence using a random effects model, which accounts for variation across studies. The ‘cimethod(exact)' and ‘ftt' options were employed to obtain precise 95% confidence intervals (CIs).
Outcome associations
The ‘Metan' command in STATA was used to perform a DerSimonian and Laird (DL) random-effects meta-analysis. DL model was chosen due to its robustness in handling heterogeneity, poignant to meta-analyses involving clinical data from diverse sources. The analysis evaluated the association between reperfusion therapy in mild AIS patients and several outcomes, including functional outcomes (defined as excellent and good, for modified Rankin Scale scores 0-1 and 0-2 at 90 days, respectively), 90-day mortality, sICH, ICH, END or stroke recurrence. Only studies reporting baseline data and appropriate functional outcomes related to reperfusion and non-reperfusion were analyzed.
Statistical significance and heterogeneity
Statistical significance was determined with a P-value threshold of <0.05 or a z-score >1.96 or < -1.96. Forest plots were generated to visually present the odds ratios (ORs) for the association studies, with the I2 statistic and P-value used to quantify heterogeneity among studies. An I2 value greater than 50% indicates substantial heterogeneity, guiding the decision to use random-effects models.
Bias and sensitivity analyses
Potential publication bias was evaluated using Egger’s test, funnel plots, and Fagan’s nomogram. Sensitivity analyses were performed with the ‘metainf' package to assess the stability of the pooled OR when individual studies were excluded. Subgroup analyses were conducted to explore variations in outcomes across different types of reperfusion therapies and to examine the impact of excluding studies focused on non-disabling mild AIS and large vessel occlusion (LVO) patients.
Variance estimation
Tau-squared (τ2) was used to estimate between-study variance, providing insight into the extent of variability not accounted for by sampling error alone. Cochran’s Q test P-values further confirmed heterogeneity levels.
Results
Description of included studies
Rate of comorbidities in cohorts of acute ischemic stroke patients included in the meta-analysis of mild stroke prevalence and outcomes.

Abbreviations: n = number of patients, % = percentage, AF = Atrial Fibrillation, HT = Hyperlipidemia, HTN = Hypertension, CAD = Coronary Artery Disease, PS/TIA = past stroke/ transient ischemic attack, DM = Diabetes Mellitus, NR = Not Recorded.
aRepeat Study: Data for different hypotheses available in study.
bNon-disabling only: Studies focusing on only non-disabling mild strokes treated with intravenous thrombolysis.
cLVO only: Studies focusing on only large vessel occlusion (LVO) mild stroke patients treated with intravenous thrombolysis.
Clinical outcomes of mild acute ischemic stroke patients included in the meta-analysis of mild stroke outcomes following reperfusion therapy.

aRepeat Study: Data for different hypotheses available in the study.
bNon-disabling only: Studies focusing on only non-disabling mild strokes treated with intravenous thrombolysis.
cLVO only: Studies focusing on only large vessel occlusion (LVO) mild stroke patients treated with intravenous thrombolysis.
Abbreviation: RT = Reperfusion Therapy, mRS = modified Rankin Scale, sICH = symptomatic Intracerebral Hemorrhage, ICH = Intracerebral Hemorrhage, n = number of patients, % = percentage, NR = not recorded, IVT = Intravenous Thrombolysis, EVT = Endovascular Thrombectomy.
Summary effects and heterogeneity Obtained from the meta-analysis of mild stroke prevalence and outcomes following reperfusion therapy.
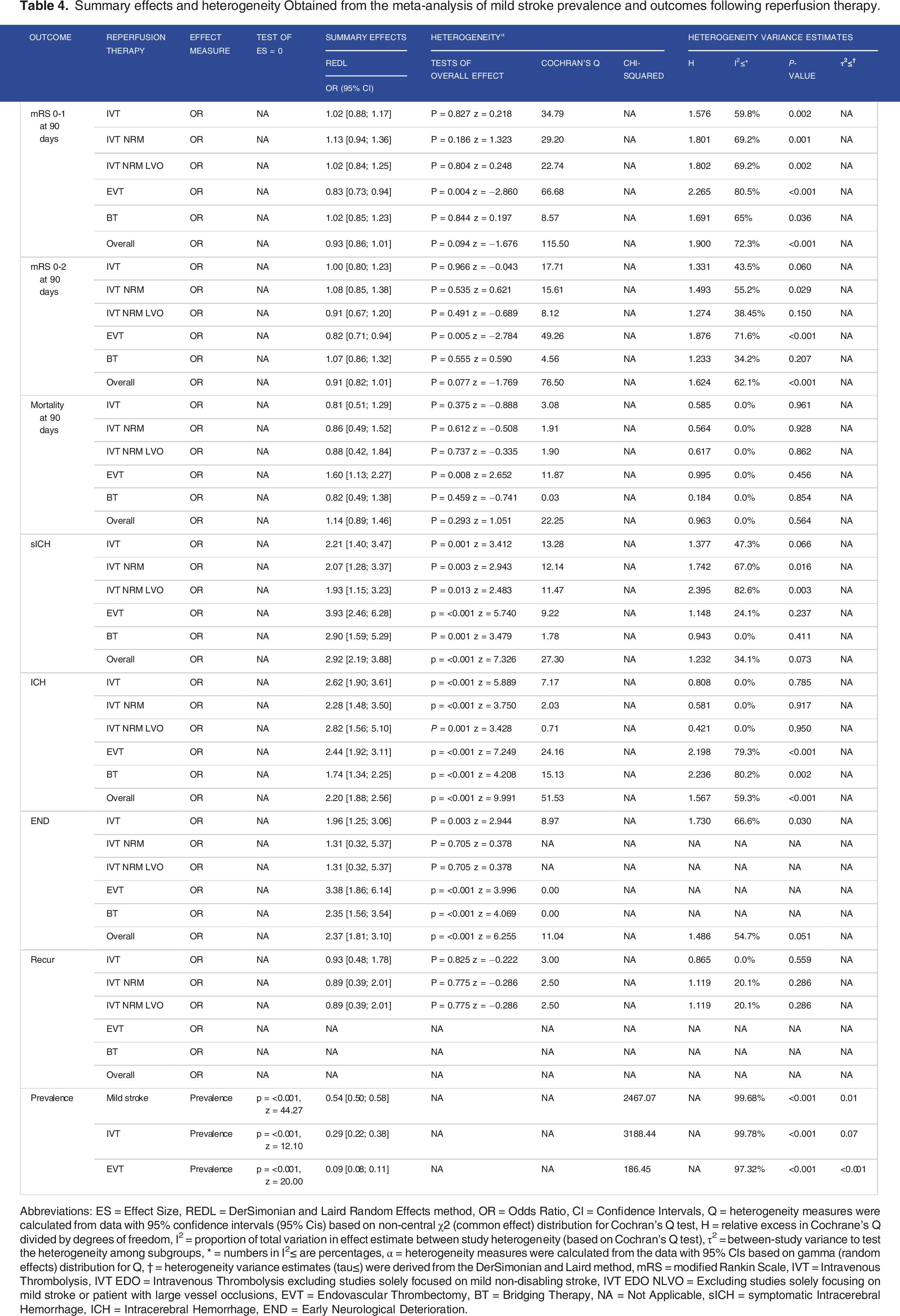
Abbreviations: ES = Effect Size, REDL = DerSimonian and Laird Random Effects method, OR = Odds Ratio, CI = Confidence Intervals, Q = heterogeneity measures were calculated from data with 95% confidence intervals (95% Cis) based on non-central χ2 (common effect) distribution for Cochran’s Q test, H = relative excess in Cochrane’s Q divided by degrees of freedom, I2 = proportion of total variation in effect estimate between study heterogeneity (based on Cochran’s Q test), τ2 = between-study variance to test the heterogeneity among subgroups, * = numbers in I2≤ are percentages, ⍺ = heterogeneity measures were calculated from the data with 95% CIs based on gamma (random effects) distribution for Q, † = heterogeneity variance estimates (tau≤) were derived from the DerSimonian and Laird method, mRS = modified Rankin Scale, IVT = Intravenous Thrombolysis, IVT EDO = Intravenous Thrombolysis excluding studies solely focused on mild non-disabling stroke, IVT EDO NLVO = Excluding studies solely focusing on mild stroke or patient with large vessel occlusions, EVT = Endovascular Thrombectomy, BT = Bridging Therapy, NA = Not Applicable, sICH = symptomatic Intracerebral Hemorrhage, ICH = Intracerebral Hemorrhage, END = Early Neurological Deterioration.

Forest plot on the prevalence of mild stroke among acute ischemic stroke patients. Abbreviations: AIS = Acute Ischemic Stroke, N = number of patients with mild AIS, C = total AIS patient cohort, P = Prevalence, ES = Effect Size, CI = Confidence Interval, I2 = heterogeneity value, p = p-value.

Forest Plot on the Association between Reperfusion and mRS 0-1 at 90 days among Mild Acute Ischemic Stroke Patients. *Bridging Therapy specific data provided. Abbreviations: exp(b) = exponential value of b/ odds ratio, CI = confidence interval, % = percentage, IVT = Intravenous Thrombolysis, EVT = Endovascular Thrombectomy, BT = Bridging Therapy, I2 = heterogeneity, p = P-value.

Forest plot on the association between reperfusion and mortality at 90 days among mild acute ischemic stroke patients. Abbreviations: exp(b) = exponential value of b/ odds ratio, CI = confidence interval, % = percentage, IVT = Intravenous Thrombolysis, EVT = Endovascular Thrombectomy, BT = Bridging Therapy, I2 = heterogeneity, p = p-value.

Forest plot on the association between reperfusion and symptomatic intracerebral hemorrhage (sICH) among mild acute ischemic stroke patients. *Bridging Therapy specific data provided. Abbreviations: exp(b) = exponential value of b/ odds ratio, CI = confidence interval, % = percentage, IVT = Intravenous Thrombolysis, EVT = Endovascular Thrombectomy, BT= Bridging Therapy, I2 = heterogeneity, p= p-value.
The meta-analysis incorporated a diverse range of studies, predominantly prospective, conducted across multiple countries, including the United States, China, and various European nations, which enhances the global applicability of the findings. The sample sizes varied widely, from as few as 377 to as many as 179 835 AIS patients, reflecting the diversity in research settings and capabilities.
Notably, demographic data showed that the proportion of male participants ranged from 39% to 73%, with the mean age of participants typically in the 60s, highlighting an older population commonly affected by stroke. The predominance of older patients, often in their 60s, indicates a population at higher risk for stroke-related complications. This demographic trend underscores the importance of tailored treatment approaches for older adults. High prevalence rates of hypertension (up to 76%) and diabetes (up to 40%) were observed across studies, which are known risk factors for stroke and may influence treatment outcomes and risks, such as increased susceptibility to hemorrhagic events following reperfusion therapies. Variation in treatment protocols and outcomes was observed across different countries, possibly reflecting regional differences in healthcare practices and population health characteristics.
We also examined effect sizes for key outcomes, including 90-day good functional outcome, 90-day mortality, sICH, ICH, END, and stroke recurrence, as detailed in Table 4. The studies demonstrated minimal potential for publication bias, a conclusion further supported by Egger’s test, as illustrated in Supplemental Figure 15. Funnel Plots (Supplemental Figure 16), Sensitivity analyses (Supplemental Figure 17), Summary receiver operating curves (SROC) (Supplemental Figure 18), Deeks Funnel Plots (Supplemental Figure 19), and Fagen’s Nomograms (Supplemental Figure 20) were also generated. Supplemental Table 6 provides quantitative data on bias measures among the different study subgroups.
Prevalence of mild stroke
As depicted in Figure 2, the overall prevalence of mild stroke among all AIS patients included in the current meta-analysis was 54% (95% CI: 0.50; 0.58; p = <0.001; z = 44.27). The prevalence of mild stroke among those treated with IVT was 29% (95% CI: 0.22; 0.38; p = <0.001; z = 12.10), while among those treated with EVT, it was 9% (95% CI: 0.08; 0.11; P < 0.001; z = 20.00). Study data demonstrates a high degree of heterogeneity among these studies, with an I2 of 99.68%, 99.78%, and 99.68%, respectively, among the 3 prevalence analyses. The data depicts possible variations in prevalence based on location and time, indicating a potential increase in IVT use over time in mild AIS patients. However, there remains insufficient data to determine whether a trend exists. Refer to Supplemental Figures 1 and 2 for forest plots on IVT and EVT prevalence.
Association of reperfusion therapy with 90-day functional outcomes in mild AIS
For association with excellent functional outcome (mRS 0-1) at 90 days, the meta-analysis included a total of 33 studies,19,26–29,31,40,47,49,51,53,54,56–61,63,65,66,68–72,74–77,79 comprising 13 978 patients, as depicted in Figure 3. Overall, reperfusion therapy did not exhibit statistical significance and resulted in an OR 0.93 (95% CI: 0.86; 1.01; P = 0.094; z = −1.676). However, subgroup analysis indicated EVT treatment demonstrated statistical significance, although it had limited association with excellent outcomes with OR 0.83 (95% CI: 0.73; 0.94; P = 0.004; z = −2.860). While IVT and BT failed to reach statistical significance and exhibited minimal association with excellent outcomes, with an OR 1.02 (95% CI: 0.88; 1.17; P = 0.827; z = 0.218) for IVT treatment and OR 1.02 (95% CI: 0.85; 1.23; P = 0.844; z = 0.197) for BT. There remained no statistical significance for IVT treatment after excluding studies focusing on non-disabling mild strokes or LVO AIS patients; refer to Supplemental Figure 3 for a forest plot depicting this data. Overall, the study’s heterogeneity was high, with an I2 of 73.3%.
For association with good functional outcome (mRS 0-2) at 90 days, the meta-analysis included a total of 30 studies,19,26–29,40,49,51,53,54,57,58,61,63,67,68,70–77,79–82 comprising 12 315 patients. While reperfusion therapy failed to demonstrate significance overall, EVT reached statistical significance. However, it showed a limited effect with OR 0.82 (95% CI: 0.71; 0.94; P = 0.005; z = −2.784). IVT and BT failed to reach statistical significance, which remained true after excluding studies focusing on non-disabling mild strokes or LVO AIS patients. Overall, the study’s heterogeneity was high, with I2 at 62.1%. Refer to Supplemental Figures 4 and 5 for forest plots depicting study data.
Association of reperfusion therapy with 90-day mortality in mild AIS
The meta-analysis included 25 studies,19,28,29,47,49,51,53,57,60,61,63,68,71–77,79–83 comprising 10 196 patients aiming to study the association of reperfusion therapy and mortality at 90 days in mild AIS. Overall, reperfusion failed to reach statistical significance and displayed OR 1.14 (95% CI: 0.89; 1.46; P = 0.293; z = 1.051), as depicted in Figure 4. However, subgroup analysis revealed EVT treatment had a statistically significant association. Whereby EVT had an OR of 1.60 (95% CI: 1.13, 2.27; P = 0.008; z = 2.652) for 90-day mortality. However, there was no significance following IVT and BT, which remained true following with the exclusion of studies focusing on non-disabling mild strokes or LVO AIS patients. Refer to Supplemental Figure 6 for a forest plot depicting this data. Overall, the study’s heterogeneity was low, with I2 at 0.0%.
Association of reperfusion therapy with sICH in mild AIS
The meta-analysis included 19 studies,19,26,27,29,51,60–64,68,70,73,76,77,79,80 comprising 13 586 patients to study the association between reperfusion therapy and sICH in mild AIS. Overall, reperfusion therapy and all subgroups reached statistical significance, with an overall OR of 2.92 (95% CI: 2.19; 3.88; p = <0.001; z = 7.326), refer to Figure 5. Among these subgroups, EVT demonstrated the strongest association with sICH, with an OR of 3.93 (95% CI: 2.46, 6.28). Meanwhile, IVT treatment demonstrated an OR of 2.21 (95% CI: 1.40; 3.47). When excluding studies solely focused on non-disabling mild stroke, the OR for sICH following IVT decreases to 2.07 (95% CI: 1.28; 3.37; P = 0.003; z = 2.943), indicating a possible lower risk of ICH among those with disabling symptoms, refer to Supplemental Figure 7. When further excluding studies focusing on mild stroke patients with LVO, the OR decreases to 1.93 (95% CI: 1.15; 3.23; P = 0.013; z = 2.483), which may be indicative of a higher odd of sICH in LVO AIS patients, refer to Supplemental Figure 8. Overall, the study’s heterogeneity was low, with I2 at 34.1%.
Association of reperfusion therapy with ICH in mild AIS
The meta-analysis included 22 studies,19,26–29,40,49,54,57–63,75,79–82 comprising 11 770 patients aiming to study the association of reperfusion therapy and ICH in mild AIS. Overall reperfusion in all subgroups demonstrates statistical significance with an overall OR of 2.20 (CI 95%: 1.88; 2.56; p = <0.001; z = 9.991). Among the subgroups, IVT demonstrated the strongest association with ICH with an OR of 2.62 (95% CI: 1.90; 3.61; p = <0.001; z = 5.889). A slight increase in the odds of ICH was noted when studies that focused on non-disabling stroke and LVO AIS patients were excluded, refer to Table 4. EVT treatment demonstrated an OR of 2.44 (95% CI: 1.92, 3.11; p = <0.001; z = 7.249), while BT demonstrated an OR of 1.74 (95% CI: 1.34; 2.25; p = <0.001; z = 4.208). Overall, heterogeneity was high, with an I2 of 59.3%. Refer to Supplemental Figures 9 and 10 for forest plots depicting the odds of ICH following reperfusion.
Association of reperfusion therapy with END in mild AIS
The meta-analysis included six studies,29,48,60,61,63,76 comprising 3497 patients aiming to study the association of reperfusion therapy and END in mild AIS. Overall, reperfusion therapy was significantly associated with END in mild AIS, with an OR of 2.37 (CI 95%: 1.81; 3.10; P < 0.001; z = 6.255). In subgroup analysis, IVT treatment demonstrated statistical significance with an OR of 1.90 (95% CI: 1.25; 3.06; P = 0.003; z = 2.944). Excluding studies focused on IVT in only mild stroke patients and LVO AIS patients increases the odds of END following reperfusion. However, this analysis failed to reach statistical significance (Table 4). EVT and BT demonstrate statistical significance and present an OR of 3.38 (95% CI: 1.86, 6.14; p = <0.001; z = 3.996) and OR of 2.35 (95% CI: 1.56; 3.54; P < 0.001; z = 4.069), respectively. However, only a single study provided data on END in EVT and BT, limiting the certainty of these findings. Overall, heterogeneity was high, with an I2 of 54.7%. Refer to Supplemental Figures 11 and 12 for forest plots depicting the odds of END following reperfusion therapy.
Association of reperfusion therapy with stroke recurrence in mild AIS
The meta-analysis included five studies,37,40,54,58,61 comprising 2330 patients aiming to study the association of reperfusion therapy and stroke recurrence at 90 days in mild AIS. While IVT treatment demonstrated an OR of 0.93 (95% CI: 0.48; 1.78; P = 0.825; −0.222), this failed to reach statistical significance. This remained true following the exclusion of studies focusing on non-disabling mild strokes or LVO AIS patients, refer to Table 4. Refer to Supplemental Figures 13 and 14 for forest plots depicting the association between 90-day stroke recurrence and reperfusion.
Discussion
Findings from this meta-analysis provide significant insights into mild AIS prevalence and outcomes following reperfusion therapy. Results indicate that while mild stroke constitutes the majority of AIS cases, only a small minority of patients treated with IVT and EVT fall into this category. Reperfusion therapy is associated with a statistically significant increase in sICH and ICH. However, there is no significant association with functional outcomes, mortality, stroke recurrence at 90 days, or END. Notably, excluding studies focusing on IVT in non-disabling stroke and LVO patients resulted in decreased odds of sICH and increased odds of ICH, though these changes in OR were minimal. This highlights the substantial prevalence of mild stroke and the associated risks of reperfusion therapy in such patients. Therefore, treatment decisions must consider risks and benefits to optimize long-term outcomes. Our subgroup analysis demonstrated a statistically significant association of EVT with functional outcomes and mortality, albeit with a limited effect size. This indicates potential benefits but raises questions about the magnitude of these benefits in mild strokes. The findings suggest a nuanced benefit of EVT, advocating for more refined subgroup analyses to identify patients who might benefit most from this intervention.
Mild stroke is prevalent, accounting for 54% of all AIS patients, yet only a minority receive IVT (29%) or EVT (54%). This suggests a potential under-treatment or conservative management approach for mild-stroke patients. This discrepancy may highlight a gap in treatment strategies where mild stroke patients are potentially underserved by reperfusion therapies,7,37,44 warranting further investigation into why these patients are less frequently treated.
Our analysis shows a significant increase in the odds of sICH and ICH with reperfusion therapies, particularly with EVT showing the highest association with sICH. Alteplase’s mechanism, involving the conversion of plasminogen to plasmin, 84 aims to restore cerebral blood flow but may also lead to hemorrhagic events, 85 resulting in edema, disability, and mortality. 86 Such hemorrhagic events can lead to edema around the ischemic lesion, with resultant disability and mortality. Co-morbidities like hypertension, atrial fibrillation, and diabetes further elevate ICH risk. 87 Additionally, age and specific imaging characteristics, such as low ASPECTS score and early CT hypodensities, may increase hemorrhagic risk. Despite these risks, the benefits of reperfusion often outweigh the dangers in moderate to severe strokes,88,89 though they are less clear in mild AIS. Therefore, there is a need for careful patient selection and risk assessment, especially considering the comorbidities and imaging characteristics that may predispose patients to hemorrhagic events.
The heterogeneity among prevalence studies may be linked to unique population characteristics in the datasets. Geographical differences in stroke risk factors, such as hypertension prevalence, might explain variations in stroke severity.90,91 Effective management of these risk factors can significantly reduce stroke severity. 92 Furthermore, discrepancies in reperfusion guidelines across regions impact treatment prevalence.7,9,93,94 For instance, American Heart Association (AHA) / American Stroke Association (ASA) guidelines strongly recommend IVT within three hours for mild strokes with disabling symptoms but are weaker for the 3-4.5 hour window. 95 Conversely, Australian guidelines advocate for IVT within 4.5 hours for all symptomatic patients. 96 Such differences highlight the influence of evidence-based guidelines on treatment decisions and outcomes.
All included studies defined mild stroke as NIHSS
In considering past meta-analyses on mild stroke outcomes following reperfusion, similar trends were observed. Zang et al found no significant differences in functional outcomes or mortality post-IVT but noted increased risks of END, sICH, and HT. 11 Lan et al 13 observed a higher ICH risk but associated thrombolysis with favorable outcomes when adjusting for heterogeneity. Zhao et al 16 indicated a higher sICH risk with EVT and no significant mortality difference. Significantly, Shang et al 18 found no increased risk of sICH following EVT and found that EVT was significantly associated with good outcomes and mortality. While our meta-analysis generally depicts trends similar to those of previous studies, our more stringent inclusion criteria and statistical methodology resulted in a comprehensive assessment of association. Further, this report also considered outcomes following bridging therapy. Future research should focus on standardizing outcome definitions, conducting subgroup analyses to address heterogeneity, and incorporating more randomized controlled trials (RCTs) to strengthen evidence.
Limitations
This study has several limitations that need to be acknowledged. (1) Inconsistent Outcome Definitions: There is significant variability in how symptomatic intracerebral hemorrhage (sICH), intracerebral hemorrhage (ICH), and early neurological deterioration (END) are defined across the included studies.50–52,79 This inconsistency introduces variability in the outcomes reported. Future research should aim to adopt standardized definitions for these outcomes to enhance the comparability and reliability of the results. (2) High Study Heterogeneity: The high heterogeneity observed in the included studies, with high I2 values across the different prevalence analyses, underscores substantial variability in the data. This variability likely stems from a range of factors, including differences in population characteristics, study designs, treatment protocols, and regional variations in stroke risk factors such as hypertension prevalence and lifestyle differences. These regional differences can significantly influence both the presentation and outcomes of mild strokes, suggesting that the prevalence and effect of reperfusion therapies may not be uniform across different settings.
91
This heterogeneity highlights the importance of developing region-specific guidelines and interventions that account for local population health dynamics and treatment practices. Such tailored approaches could enhance the relevance and applicability of treatment strategies for mild stroke patients, ensuring that interventions are both effective and aligned with the specific needs of diverse populations. (3) Limited RCTs Inclusion: The meta-analysis predominantly includes observational studies, which limits the ability to make causal inferences. The lack of recent RCTs, particularly those evaluating outcomes for patients treated with EVT and BT, constrains the quality of available data. Incorporating more RCTs in future analyses would strengthen the evidence base and effectively guide clinical practice. (4) Variability in Control Treatments: There is notable variability in the treatment regimens for control groups across studies, with some patients receiving only supportive care and others receiving different treatments, such as dual antiplatelet therapy.40,61 This variability may skew the results and complicate comparisons between treatment effects. Future studies should standardize control group treatments to improve accuracy and reliability. (5) Limited Data on Prevalence and Outcomes: There is insufficient data on the prevalence of mild stroke, particularly among those treated with IVT and EVT. Additionally, there is limited information on END in EVT and BT-treated patients, reducing the generalizability of the study outcomes. Additional data from large databases could provide a better understanding of epidemiological factors influencing prevalence. (6) Standardization of Mild Stroke Definitions: The consistent use of NIHSS≤5 as the definition for mild stroke may improve data availability and comparability, as many studies were excluded from this meta-analysis for using alternate definitions.
1
(7) Variations in Guidelines: There are discrepancies in reperfusion guidelines across different jurisdictions,95,96,103,104 affecting treatment decisions and outcomes. The differences in guidelines highlight the impact of evidence-based clinical recommendations on the uptake of reperfusion therapies, suggesting a need for global consensus or adaptable guidelines that consider local population health dynamics. (8) NIHSS as a Predictor: While NIHSS≤5 is a standard for mild stroke, its limitations in posterior circulation strokes97–100 and inferior predictive value for functional outcomes in the era of acute intervention are noted.
101
This suggests a need for additional or alternative measures, such as discharge NIHSS
101
or ASPECTS,102,105 to better predict outcomes and guide treatment in specific subgroups.
By addressing these concerns, future research can enhance the reliability and applicability of findings, supporting more accurate assessments and informed clinical decisions regarding reperfusion therapies in mild stroke patients. These improvements would contribute to more accurate assessments and informed clinical decisions regarding reperfusion therapies in mild-stroke patients.
Evidence-based SAFE recommendations for acute reperfusion therapy in mild stroke patients
Evidence-based SAFE recommendations for acute reperfusion therapy in mild stroke patients.

Note. Grading: A: Strong recommendation based on consistent and good-quality evidence; B: Moderate recommendation based on fair evidence.
Level of Evidence: I: Evidence from randomized controlled trials; IIa: Evidence from well-conducted cohort studies or meta-analyses; IIb: Evidence based on the need for consistent data to identify and address gaps in care.
These SAFE recommendations are designed to help clinicians navigate the complex decision-making process involved in treating mild-stroke patients, ensuring that each patient receives the most appropriate care based on the latest evidence and best practices.
Conclusion
In conclusion, mild stroke constitutes a significant proportion of acute ischemic strokes (54%) but accounts for a smaller percentage of patients treated with IVT (29%) and EVT (9%). This meta-analysis reveals a strong association between reperfusion therapies and increased risks of symptomatic intracerebral hemorrhage (sICH) and intracerebral hemorrhage (ICH). However, no statistically significant association was found between reperfusion and functional outcomes, mortality, early neurological deterioration (END), or stroke recurrence in mild stroke cases. Although EVT shows significance for functional outcomes and mortality, it presents with a limited effect size. These findings emphasize the importance of assessing stroke severity before treatment, given the high prevalence of mild stroke. The risks of reperfusion therapies must be carefully weighed against potential benefits, particularly given the inconclusive treatment benefits in mild strokes. Despite these risks, reperfusion therapies can offer potential benefits in select mild-stroke patients, especially those with disabling symptoms or large vessel occlusion (LVO). The possibility of restoring cerebral blood flow and preventing further neurological deterioration should be considered, especially in individualized treatment decisions that account for patient-specific factors like comorbidities, stroke etiology, and imaging findings.
SAFE recommendations
To guide clinical decision-making, we propose the SAFE framework: • • • •
Future research and policy changes
Future research should focus on refining patient selection criteria to identify those most likely to benefit from reperfusion therapies, particularly EVT. This includes conducting more RCTs to strengthen the evidence base and effectively guide clinical practice. Additionally, research should aim to standardize definitions for clinical outcomes and incorporate subgroup analyses to explore sources of heterogeneity, enhancing the reliability and applicability of findings in mild stroke management. Policy changes should consider establishing region-specific guidelines that align with local population health dynamics, considering the variability in stroke risk factors and treatment practices. Developing global consensus or adaptable guidelines could help optimize treatment strategies across diverse healthcare settings. By addressing these concerns, future efforts can contribute to more accurate assessments and informed clinical decisions regarding reperfusion therapies in mild-stroke patients, ultimately improving patient outcomes and healthcare efficiency.
Supplemental Material
Supplemental Material - Prevalence and outcomes of mild stroke patients undergoing reperfusion therapy: A meta-analysis and SAFE recommendations for optimal management
Supplemental Material for Prevalence and outcomes of mild stroke patients undergoing reperfusion therapy: A meta-analysis and SAFE recommendations for optimal management by Pathmesh Rajeswaran, Bella B. Huasen, Peter Stanwell, Murray C. Killingsworth and Sonu M. M. Bhaskar in Journal of Central Nervous System Disease
Footnotes
Acknowledgments
We acknowledge the JSPS International Fellowship (Grant ID: P23712) and the Grant-in-Aid for Scientific Research (KAKENHI) (Grant ID: 23KF0126) for their financial support.
Author contributions
SMMB conceived the study, contributed to the planning, drafting, and revision of the manuscript, and supervised the members of the Global Health Neurology Lab, including PR; SMMB encouraged PR to investigate and supervised the findings of this work. All authors (PR, BBH, PS, MCK, SMMB) contributed to the overall discussions on the study, critical review of the data analyses, writing of the manuscript, and subsequent revisions. All authors approved the final draft of the manuscript.
Declaration of conflicting interests:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SMMB reports leadership or fiduciary roles in various organizations, including the National Cerebral and Cardiovascular Center (Osaka, Japan) as Visiting Director (2023-25); Rotary District 9675 (Sydney, Australia) as District Chair for Diversity, Equity, and Inclusion; the Global Health and Migration Hub Community, Global Health Hub Germany (Berlin, Germany) as Chair, Founding Member, and Manager; and editorial board memberships at PLOS One, BMC Neurology, Frontiers in Neurology, Frontiers in Stroke, Frontiers in Public Health, Journal of Aging Research, and BMC Medical Research Methodology. Additionally, SMMB serves as a Member of the College of Reviewers for the Canadian Institutes of Health Research (CIHR), Government of Canada; Director of Research for the World Headache Society (Bengaluru, India); a member of the Scientific Review Committee at Cardiff University Biobank (Cardiff, UK); and as an Expert Adviser/Reviewer for the Cariplo Foundation (Milan, Italy). These roles are unrelated to the submitted work. Other authors (PR, BBH, PS, MCK) report no conflicts of interest. The funding body had no influence on the study design, data collection, analysis, interpretation of findings, or manuscript preparation. The content is solely the responsibility of the authors and does not necessarily represent the official views of the affiliated or funding organizations.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: financial support for a separate project was received through the Grant-in-Aid for Scientific Research (KAKENHI) (PI: S.M.M.B.), funded by the Japan Society for the Promotion of Science (JSPS), Japanese Ministry of Education, Culture, Sports, Science and Technology (MEXT), Japan (Grant ID: 23KF0126). S.M.M.B was awarded the JSPS International Fellowship, supported by MEXT and the Australian Academy of Science, for the period 2023-2025 (Grant ID: P23712).
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.