
Abstract
Background
NEURO® is a 2-week program that combines low-frequency repetitive transcranial magnetic stimulation (rTMS) and intensive occupational therapy (OT) to treat patients with chronic hemiparesis following stroke. The degree to which each element contributes to the improvement of upper limb function remains unclear. It has been suggested that low-frequency rTMS applied to a healthy cerebrum activates neural activity in the contralateral hemispheric area surrounding the lesion. Intensive OT performed in parallel to rTMS promotes the functional remodeling of the cerebrum to help with rehabilitation.
Objectives
However, this has not been demonstrated using NEURO®. Therefore, we aimed to compare the effects of the NEURO® and OT-only protocols in patients with hemiparesis following stroke.
Methods
Thirty-seven patients with upper limb paralysis following stroke were recruited and hospitalized for treatments and randomly divided into two groups. Group A consisted of 16 patients who underwent NEURO® for the first 2 weeks, and Group B consisted of 21 patients who underwent OT-only for the first 2 weeks. After 2 weeks of hospitalization, the treatments of Groups A and B were reversed for the subsequent 2 weeks of treatment. Improvement in upper limb motor function in Groups A and B at 2 and 4 weeks after the start of treatment was evaluated using the Fugl-Meyer Motor Assessment (FMA) and the Wolf Motor Function Test (WMFT).
Results
Group A, who underwent NEURO® first during their initial 2-week hospitalization, showed significantly greater improvement than that in Group B, who underwent OT-only first (P = .041 for FMA and P < .01 for WMFT). At 4 weeks following the reversal of treatments, Group A who underwent NEURO® and then OT-only showed significantly greater improvement than that in Group B, who underwent OT-only followed by NEURO® (P = .011 for FMA and P = .001 for WMFT).
Conclusion
Our findings indicate that rTMS facilitates neuromodulation when combined with OT, which leads to more effective rehabilitation than with OT alone (Trial registration: JMACCT (http://www.jmacct.med.or.jp/); trial ID JMA-IIA00215).
Keywords
Introduction
Over 65% of stroke survivors are unable to perform activities of daily living (ADL) because of an affected upper limb. 1 Even mild motor impairments of the upper limb result in disability and negatively impact patients’ quality of life. 2 Intensive occupational therapy (OT), such as constraint-induced movement therapy (CIMT), has been reported to activate the lesional hemisphere in post-stroke hemiparetic patients. 3 Recent studies have confirmed the clinical effectiveness of CIMT, in which patients are required to undergo daily 6 h one-on-one (OTO) training with the unaffected upper limb restrained during 90% of waking hours over 2 weeks of hospitalization.4-6 However, its clinical feasibility is questionable: some patients consider the therapy strenuous and concerns have been raised regarding the intensive schedule of treatment and the ability to carry out home duties and work during their hospital stay. 7 Therefore, there is a need for intensive OT protocols that are more feasible than the original CIMT protocol.
Recently, a non-invasive method of low-frequency repetitive transcranial magnetic stimulation (rTMS) has been used to promote functional recovery of stroke patients by suppressing the contralesional intact motor cortex, which reduces interhemispheric inhibition and leads to functional reorganization of the lesional hemisphere.7-11 Moreover, randomized controlled trials of OT approaches, such as CIMT, have been shown to significantly improve motor function of the hemiparetic upper limb after stroke, which led to the development of a 2-week intervention program (NEURO®) that combines low-frequency rTMS and intensive OT.12,13 The program consists of a 2-h OTO daily training session with the unaffected upper limb restrained and 2 h of self-training to improve the feasibility of the intervention, which is a more feasible treatment schedule than that of traditional CIMT protocols. Low-frequency rTMS to the contralesional hemisphere was introduced to the OT protocol as an adjuvant therapy to facilitate or consolidate the effects of OT.
The high effectiveness of NEURO® among patients in the chronic phase of stroke has been reported in a randomized comparative study that used CIMT as a control. 14
However, to date, the effectiveness of rTMS in the clinical treatment package of NEURO® for improving upper limb function has not been explored. Therefore, our aim was to compare the effects of NEURO® (OT in combination with rTMS) and OT alone in stroke patients to understand the additional effects of combining rTMS with OT according to the NEURO® program. CIMT restrains the non-paralyzed upper limbs of stroke hemiplegic patients. Therefore, OT alone can be more pure control without restraint.
Methods
Study participants
Clinical characteristics of patients (n = 37).

Values represent numbers (%) or means ± standard deviations (SD).
Baseline participant characteristics of Groups A and B.
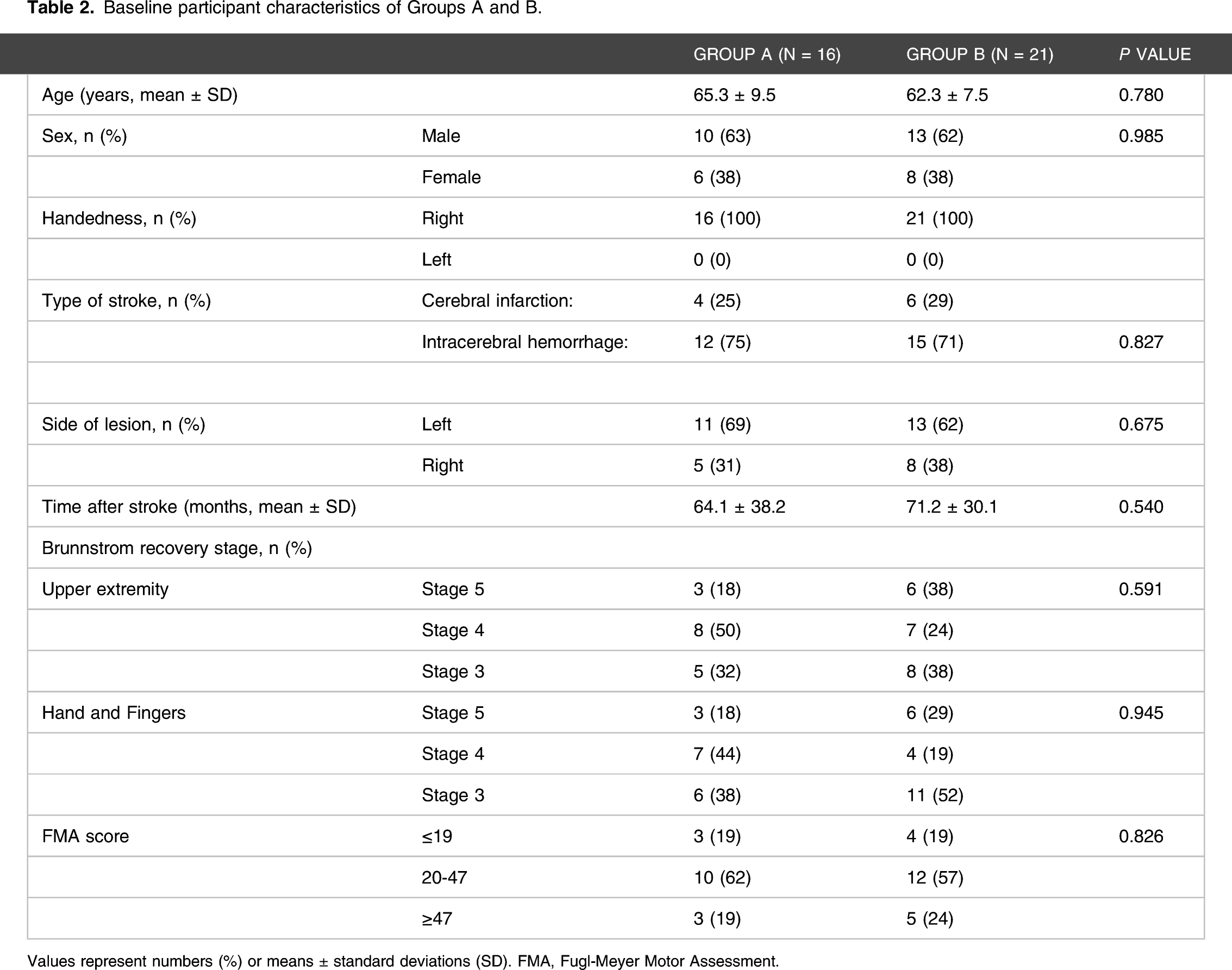
Values represent numbers (%) or means ± standard deviations (SD). FMA, Fugl-Meyer Motor Assessment.
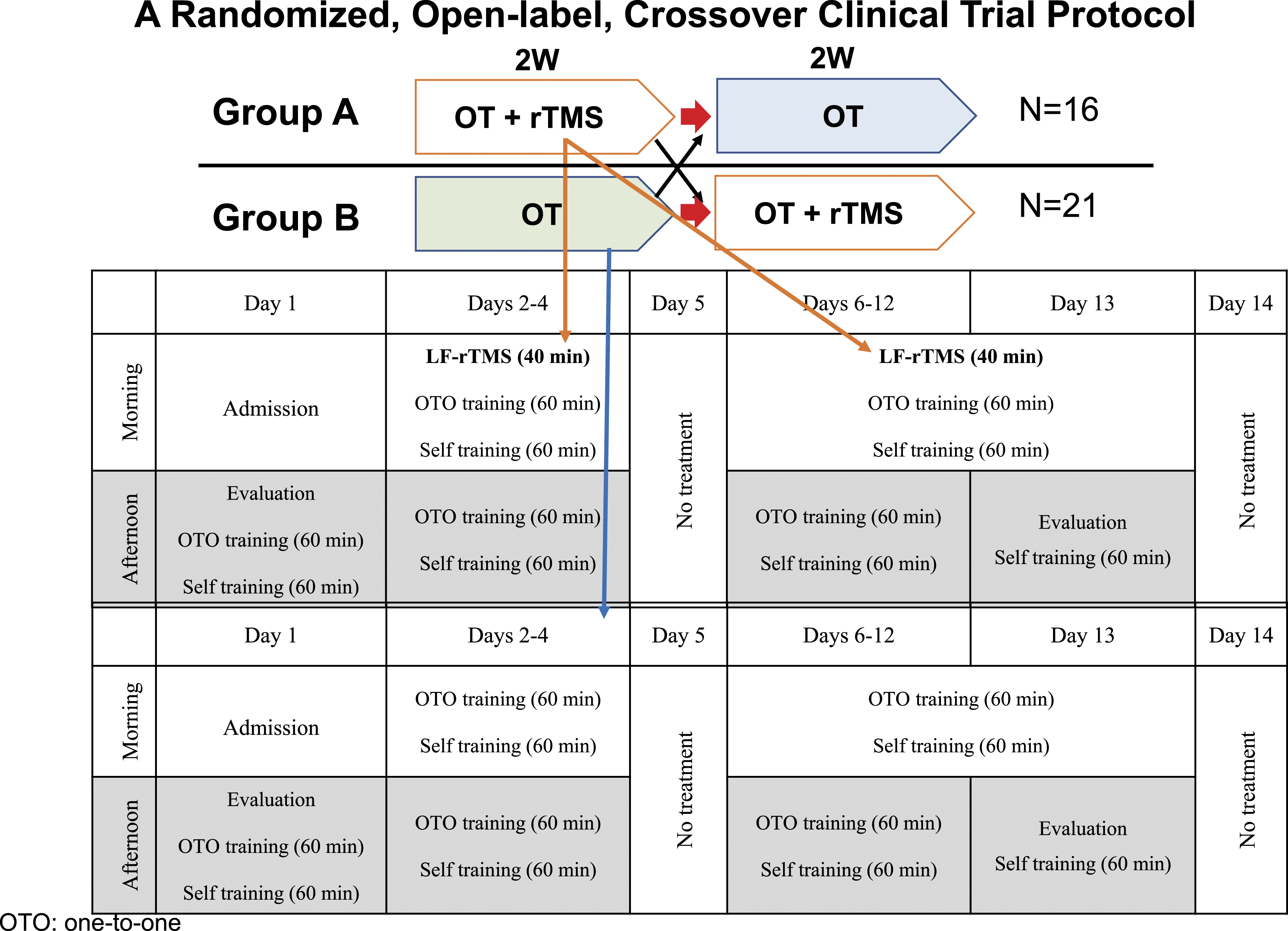
Clinical trial protocol and treatment schedule for the NEURO program. Sixteen patients (Group A) underwent the NEURO (OT + rTMS) treatment before OT-only for 2 weeks, and 21 patients (Group B) underwent NEURO (OT + rTMS) after OT-only for 2 weeks. LF, low frequency; OT, occupational therapy; rTMS, repetitive transcranial magnetic stimulation; OTO, one-to-one.
NEURO® program and occupational therapy-only protocols
The NEURO® program comprised both rTMS and OT sessions on days 2–4 and 6–13, with OT also provided on day 1. For the OT-only protocol, patients received the same intensive OT program as that of the NEURO program without the rTMS sessions. For the delivery of low-frequency rTMS, we used the MagPro R30 stimulator (MagVenture Company, Farum, Denmark) equipped with a figure-of-eight coil (70-mm diameter). During each session, 2400 pulses at 1 Hz for 40 min were applied to the skull of the patient’s non-lesional hemisphere at a site that elicited the largest motor-evoked potentials in the first dorsal interosseous (FDI) muscle of the unaffected upper limb using surface electromyography. The stimulation intensity was set at 90% of the motor threshold of the FDI muscle, which was defined as the lowest stimulation intensity at which a motor-evoked potential could be elicited in the FDI muscle.
The 240-min intensive OT program comprised 120 min of OTO training (60 min each in the morning and afternoon) and 120 min of self-exercise (60 min each in the morning and afternoon), 6 days a week (excluding Sundays). 13 Between the OTO training and self-exercise sessions, patients were given 5 to 10 min of rest. The OTO training was provided by an occupational therapist and mainly involved shaping techniques (eg, wiping a table with a towel, writing letters with a pencil, and moving a cup from one place to another) and repetitive task practice (eg, gripping a small ball, picking up a small coin, and squeezing clay). The detailed content of this training was tailored to the motor function of the patients’ affected upper limb and lifestyle (eg, occupation, interests, and household chores). The program was modified to improve motor function of the affected upper limb during hospitalization.
The treatment strategy included the following: (1) incorporation of a fair amount of everyday physical activity in the training tasks; (2) individualized functional training to aimed at acquiring more movement and activity; (3) incorporation of elements involved in gross and fine motor functions and multitasking; (4) clear demonstration of the position of the upper limb during training; (5) enabling a specific staged intervention; (6) incorporation of content that can be continued at home following discharge in situations of ADLs and unsupervised training; (7) not restraining the unparalyzed upper limb, such as CIMT; and (8) provision of action feedback by passive intervention with verbal instructions.
Following the OTO training, self-exercise was encouraged in another quiet room without any supervision. Before each session, patients received written instructions for self-training that were prepared individually, which included tasks similar to those carried out during the OTO training. After each session, the performance of the tasks was checked and reviewed by the therapists by interviews. If needed, the intensity and duration of the self-exercise were modified after initiation of the protocol to ensure that the exercises could be completed efficiently. At discharge, patients were provided with instructions for daily home exercise based on their functional recovery. The treatment schedule of the NEURO program is illustrated in Figure 1.
(JMACCT; JMA-IIA00215)
Serial evaluation of motor function in the affected upper limb
Upper limb movements were evaluated using the Wolf Motor Function Test (WMFT) and the Fugl-Meyer Motor Assessment (FMA). We assessed improvements in the performance of these tests of the upper limbs in the two groups after 2 and 4 weeks. The WMFT contains 15 timed tasks and two strength tasks.16,17 Examples of the tasks include the following: 1. placing forearm on the desk by abducting the shoulder; 2. placing forearm on a box by abducting the shoulder; 3. extending the elbow to reach toward the other side of the desk; 4. extending the elbow to move a 450 g weight to the opposite side of the desk; 5. gripping and raising a pencil; 6. gripping and lifting a clip; 7. folding a towel. The performance time for each timed task was recorded for a single trial. When the task was not completed within 120 s, the performance time of the task was recorded as 120 s. The sum of the performance times for all 15 tasks was the total time. For the statistical analysis, the mean value of WMFT performance times of the 15 tasks was transformed into a natural logarithm to normalize the skewed distribution of the data, following the method applied by the EXCITE trial. 6 The FMA is a performance-based tool for the quantitative assessment of impairments in patients with hemiparesis following stroke. The FMA section that is associated with motor function of the upper limb consists of 33 items, and each item is rated on a 3-point ordinal scale (0–2) with a maximum motor performance score of 66 points.18,19 FMA scores were classified into three categories of severity according to the methods used by Woodbury et al 20 : mild (≥47 points), moderate (20–46 points), and severe (0–19 points). The trial was an open-label design and participation after explaining the treatment contents for 4 weeks. Therefore, sham stimulation was not used and blinding was not possible. However, the assessors were blinded to intervention to minimize bias.
Statistical analysis
We calculated WMFT log performance time values for Groups A and B at 2 weeks after admission and subtracted the corresponding values at admission to obtain ΔWMFT log performance times, which were used to evaluate the improvement in upper limb motor function. Similarly, the degree of FMA change (ΔFMA) between Groups A and B was also evaluated. Fisher’s exact probability test was used to analyze categorical variables (eg, severity based on FMA score and BRS for fingers). The Wilcoxon signed-rank test and an ANOVA were used to compare changes in FMA score and WMFT log performance time from baseline between the two groups. Data are expressed as means ± standard deviations (SD). A P-value < .05 was considered statistically significant. All statistical analyses were performed using the Statistical Package for Social Sciences, version 25.0 (SPSS Inc, Chicago, IL) and EZR (version 1.36; Saitama Medical Center, Jichi Medical University, Saitama, Japan).
Results
The age at treatment ranged from 37 to 65 years, and the types of stroke among patients were cerebral cortical infarction (n = 12) and intracerebral hemorrhage (n = 25). The right upper limb was affected in 13 patients and the left in 24 patients. The severity of motor deficits in the fingers before treatment was BRS 3–5. There were no significant differences in baseline measures between the two groups (Table 2). All patients completed the full 4-week protocol. None of the patients experienced any pathological symptoms or deterioration of motor function in the upper limb during hospitalization. After 4 weeks of therapy, none of the patients exhibited any abnormal findings.
Efficacy of the protocol
The median ΔWMFT log performance time values of Groups A and B at 2 weeks were −.261 and −.0005, respectively. There were significant differences in WMFT log performance time values between Groups A and B from baseline to both 2 and 4 weeks (P < .01). The decrease in ΔWMFT log performance time values from baseline to 2 weeks of Group A was significantly larger than that of Group B (P = .034). The median ΔWMFT log performance time values of Groups A and B were −.293 and −.01, respectively The comparison of the ΔWMFT log performance time values from baseline to 4 weeks between Groups A and B showed that the decrease of Group A was significantly greater than that of Group B (P = .011; Figure 2). Comparison of WMFT changes between Groups A and B **P < .01. WMFT, Wolf Motor Function Test.
There were significant differences in ΔFMA between Groups A and B from baseline to both 2 and 4 weeks. The ΔFMA (median ±SD) from baseline to week 2 for Groups A and B were 4.63 ± 3.26 and 2.19 ± 3.27 (P < .001), respectively, and that from baseline to week 4 for Groups A and B were 7.25 ± 3.84 and 4.00 ± 3.37 (P = .005), respectively. The increases in FMA from baseline to 2 and 4 weeks of Group A were significantly greater than those of Group B (Figure 3). Comparison of FMA changes between Groups A and B *P < .05. FMA, Fugl-Meyer Motor Assessment.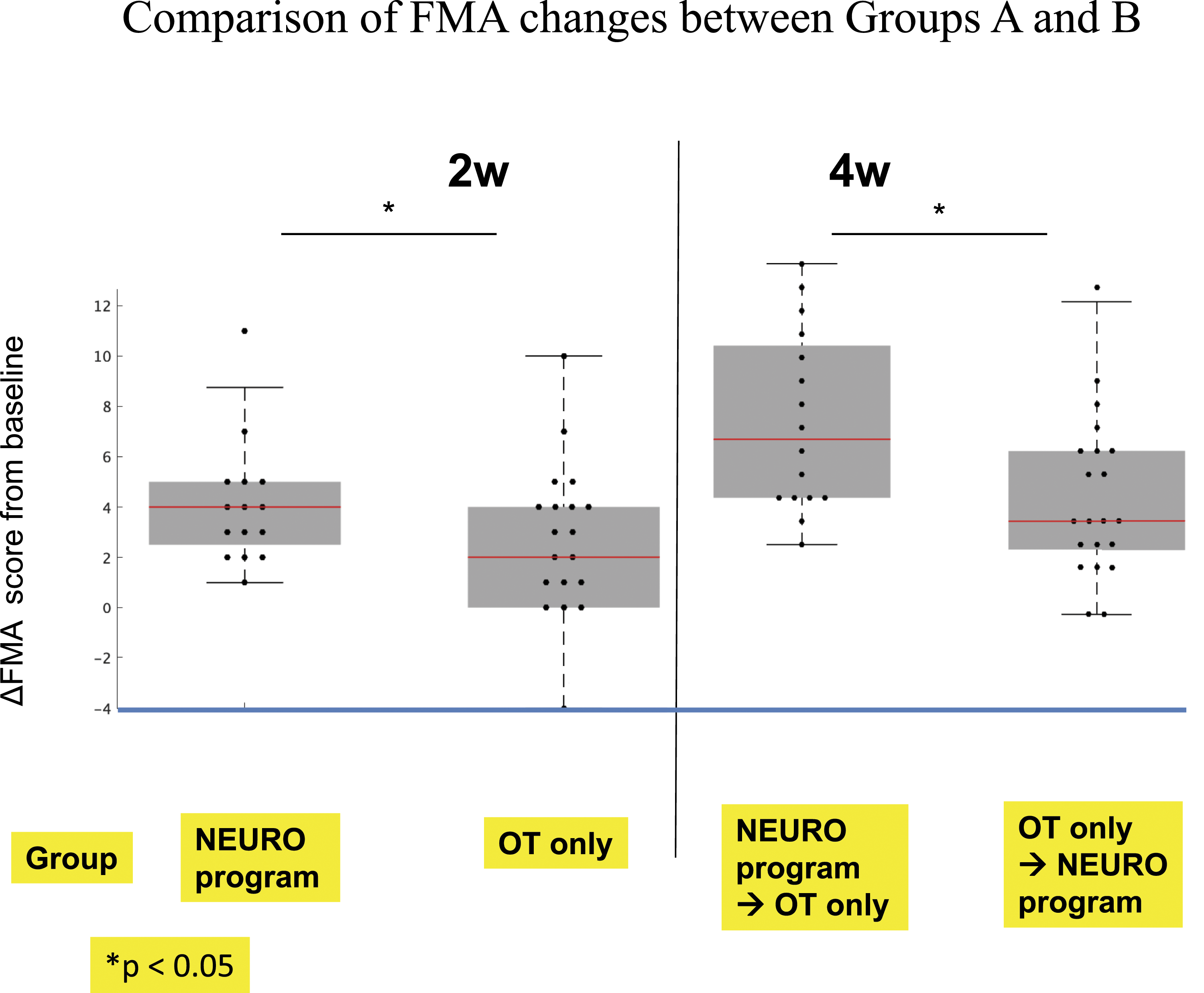
Discussion
Based on data of more than 1700 post-stroke patients, a combined protocol of low-frequency rTMS and intensive OT (NEURO®) has been shown to safely improve the motor function of the affected upper limb. 20 Moreover, the therapeutic efficacy of this treatment was shown to persist for at least 1 month. 20 In the current study, at 2 and 4 weeks following admission, post-stroke patients in Group A showed significantly greater improvements in FMA score and WMFT log performance time than those in post-stroke patients in Group B. This indicated that treatment of Group A was more effective than that of Group B for recovery of upper limb motor function.
Studies using a stroke model in rats have revealed that enhancing the activation of the motor cortex of the affected cerebral hemisphere is crucial for improving motor paralysis.21,22 Several randomized controlled trials have recently confirmed that low-frequency rTMS applied to the non-lesional hemisphere of post-stroke patients can significantly improve motor function of the affected upper limb.8-10 The underlying mechanism of the beneficial effects of rTMS is thought to be the reduction in interhemispheric inhibition of the non-lesional hemisphere to the lesional hemisphere following low-frequency rTMS, which facilitates beneficial functional reorganization of the lesional hemisphere.23-25 Subsequent intensive OT may promote functional remodeling of the cerebrum when the peri-lesional area is released from neural inhibition by rTMS. Patients who received intensive OT first were able to move both their paralyzed and non-paralyzed upper limbs, which may have affected the interhemispheric inhibition of the cerebral hemispheres, where suppression of the hyperexcitability of the non-affected cerebrum by rTMS may not have been sufficiently exerted. As a result, the effect of improving motor function of the paralyzed upper limb may have been weakened. In non-severely paralyzed patients, greater interhemispheric inhibition results in poor improvement of upper limb motor function on the paralyzed side, whereas, in patients with severe paralysis, a compensatory improvement in motor function occurs because of the nerve fibers in the injured cerebral hemisphere.26,27 We presumed that the patients in our study were not severely paralyzed because of the therapeutic effect observed following rTMS. By first examining the degree of post-stroke hemiplegia, whether rTMS should be used first or later in combination with OT may be determined.
WMFT quantifies upper-extremity movement ability using timed single- or multiple-joint motions and functional tasks. The tasks are arranged in order of complexity, with progression from proximal to distal joint involvement, and tests total extremity movement and movement speed; moreover, the test requires few tools and minimal training to implement.16,17 In Group A, but not in Group B, WMFT log performance time values decreased significantly from baseline to 2 and 4 weeks, which indicated an improvement in upper limb motor function. This reflected a significant reduction in the WMFT log performance time value in patients with a BRS of 3 or 4 for fingers (the subjective ability to flex all fingers of the affected upper limb in the full range of motion). In hemiplegic patients with a BRS of 3 or 4 for fingers, spasticity strongly affects peripheral voluntary movements during the recovery process. 28 Kakuda et al evaluated the degree of upper limb spasticity before and after NEURO® in patients who had a stroke resulting in upper limb paralysis and spasticity and reported an improvement in the modified Ashworth scale and a decrease in the muscle tone of the paralyzed upper limb flexor muscle group.29,30 In addition, Kondo et al performed a nerve conduction velocity test before and after NEURO® and showed that the improvement in upper limb function was accompanied by a decrease in spasticity. 31 RTMS decreases the excitability of the anterior horn cells on the affected side of the brain to relieve spasticity, which is consistent with the improvement in spasticity of the paralyzed upper limbs and restoration of voluntary movement in patients with BRS 3 (almost 4) or 4 that we observed following the NEURO® intervention.
In this study, the FMA score showed a statistically significant improvement in either Group A or B. This may be because of the difference in evaluation factors. In the field of stroke rehabilitation, FMA is considered one of the most comprehensive quantitative measures of motor impairment following stroke. 19 Unlike FMA, WMFT includes numerous items for evaluating peripheral voluntary movements, such as article operation tasks. In contrast to Group B, many patients in Group A showed improvements in upper limb motor function, such as article manipulation, which appeared to be due to rTMS treatment.
There are several limitations to the present study. First, this study did not explore the functional changes in the brain following the NEURO® intervention. However, previous reports have shown that the reduction of spasticity on the paralyzed side and improvement in limb dysfunction following rTMS30,31 are reflected in neuromodulation in predominantly the disabled side based on functional magnetic resonance imaging 32 and single-photon emission computed tomography. 33 Moreover, changes in brain-derived neurotrophic factor have also been demonstrated following rTMS. 34 Thus, we speculate that in the current study, the functional changes in the brain were caused by the rTMS treatment. Second, it has been reported that long-term motor function improvement following NEURO® lasts for at least 1 month; however, establishing longer-term effects at 6 months and later is required in the future. Third, as suggested by this study, the function and degree of improvement in upper limb paralysis after stroke vary depending on the intensity of spasticity. Therefore, it is necessary to conduct large-scale clinical trials in patients with different levels of motor dysfunction severity to gain a complete understanding of the degree of paralysis and characteristics of each patient. Fourth, we should consider OT contents. Occupational therapists use a wide variety of intervention methods, and effects likely differ depending on the intervention method. Finally, the crossover design may have introduced carryover effects. However, the main purpose of the study was to compare the effects of the intervention at 2 weeks, for which we observed a significant difference. In future studies, further factors should be considered, such as intervention frequency, method, trial design, and evaluation of functional improvement by incorporating neuroimaging, to develop more effective intervention methods for occupational therapists to treat post-stroke hemiplegic patients.
Footnotes
Acknowledgments
The authors gratefully acknowledge the participation of the patients in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by a Grant-in-Aid for Scientific Research from the Japan Society for the Promotion of Science.