
Abstract
The workforce of the medical specialty of Rehabilitation Medicine (RM) in the UK is 10 times less than the European average for the specialty of Physical and Rehabilitation Medicine (PRM). This can be explained partly by the difference in the scope of practice within the specialty between the UK and other European countries and USA. This opinion paper aims to compare the rehabilitation needs in chronic medical conditions and compare the scope of practice between countries within Europe and other regions of the world. The potential advantages of a broader remit specialty to improve rehabilitation care for patients by involving rehabilitation physicians in various medical conditions is explored. Recommendations have been put forward in the Rehabilitation Medicine Expansion Proposal (RMEP), which is likely to make the medical specialty of RM/ PRM more satisfying for the doctors working in the specialty and a more attractive career choice for those entering training in the specialty. There is a need for an international universal framework for the scope of the specialty to have a greater impact on improving the lives of those with chronic medical conditions.
Keywords
Background
Rehabilitation Medicine (RM) is concerned with improving functioning through the diagnosis and treatment of health conditions, reducing impairments and preventing or treating complications. 1 The purpose of the medical specialty is defined as ‘the application of medical skill to the diagnosis and management of disabling disease and injury of whatever cause and affecting any system of the body’.
The common conditions causing disability in the UK are listed in Table 1. 2
Top 25 causes of YDL (years lived with disability) in the UK for both sexes and all ages in 2010 (in descending order).

The RM specialty training programme duration is 4 years to become a consultant/specialist. Trainees should have completed core training in medicine/surgery/general practice/psychiatry and obtained membership of Royal College prior to entering specialist training in RM. The training prepares them to acquire specialist medical skills in biopsychosocial assessment of complex disability, use of pharmacological and non-pharmacological interventions (such as anti-spasticity treatments), use technology for diagnosis and guiding management (such as 3D-motion analysis) and lead multidisciplinary rehabilitation teams. There are currently around 190 RM consultants in the UK. The current workforce practice predominantly in three areas of RM: Brain Injury Rehabilitation, Spinal Cord Injury Rehabilitation and Amputee Rehabilitation (in descending order of number of specialists). There are very few doctors in RM practicing in areas outside these three areas.
There are doctors currently practicing rehabilitation within the areas of clinical need not covered by RM, but they belong to other specialties such as Rheumatology, Anaesthesia, Cardiology, Neurophysiology, Paediatrics and Palliative Medicine. Also, some newer specialties have emerged to meet specific areas of unmet need such Sport and Exercise Medicine (SEM) and Stroke Medicine. Musculoskeletal (MSK) medicine is now predominantly practised by specialists in SEM or General Practitioners with a special interest (GPwSI) in MSK Medicine. Pain Medicine and Rehabilitation in the UK is mostly practiced by anaesthetists. Cardiac and Pulmonary rehabilitation services are predominantly run by specialist nurses under supervision from cardiologists and respiratory physicians (and GPwSIs in some places). Although an obvious need exists, Cancer Rehabilitation has very little medical oversight or involvement and pathways vary widely between different areas in the UK. Clinical Neurophysiology (Neuromuscular Medicine) is a small specialty with around 100 specialists in the country.
The workforce in RM (in the UK) has remained relatively static (compared with the expansion in numbers seen in other core medical subspecialties). It can be argued that the growth and expansion of the specialty of RM have been hampered by the emergence of multiple smaller specialties and the provision of rehabilitation services led by non-RM physicians in certain areas. It can be argued that these services might be better led by RM physicians whose practice is based on the WHO ICF biopsychosocial framework. 3
This opinion paper aimed to compare the scope of practice between UK and other regions of the world and make some recommendations for expanding the RM specialty.
Methods
We compared the workforce numbers between countries in Europe per unit population. The training requirements of different countries inside and outside Europe were compared to understand the variation in the scope of practice. The name of the specialty was also noted to help us understand the relationship between name and scope of practice. Based on our findings, in 2016, we have put forward recommendations for expanding the scope of the specialty and named it the Rehabilitation Medicine Expansion Proposal (RMEP). We put forward the merits of an expanded specialty to patients with rehabilitation needs, discuss the strategy for each subspecialist area expansion, debate the role of the name of the specialty and mention the potential barriers to RMEP.
Results
There are over 13 000 PRM specialists in 30 countries of Europe, with an average of 3 PRM specialists/100 000 inhabitants (compared to less than 0.27 RM specialists/100 000 inhabitants in UK; Figure 1). 4 The structure of the specialty in the USA and Canada is broad-based with numerous subspecialties. The USA has more than 8000 physicians practicing in various fields under the equivalent umbrella specialty of Physical Medicine and Rehabilitation (PM&R).
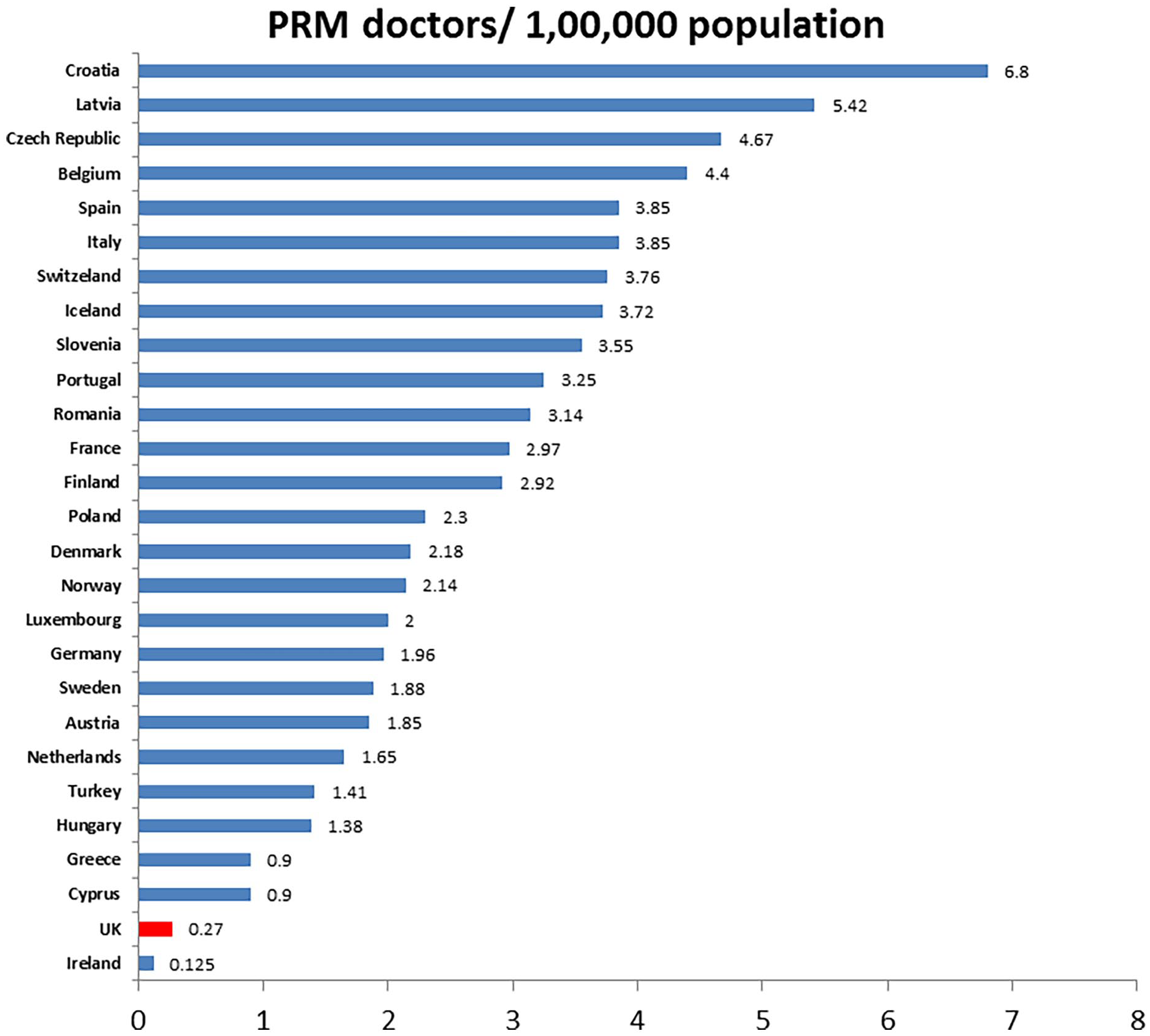
Number of PRM specialists in Europe.
The USA specialty residency training programme is for 4 to 5 years after graduating from medical school. The first year involves working in General Internal Medicine (GIM) followed by 2 years of rotations in various mandatory areas listed above. Trainees then spend 1 to 2 years subspecialising in their area of interest. The specialty has ranked in the top 10 to 15 specialties (out of 60 odd specialties) in residency matches for the last few decades (its popularity being greater than specialties like Neurology, Internal Medicine and Family Medicine). The satisfaction rate in the specialty is also higher than many other core specialties. 5
The training structure in most European countries is similar (4 years) with board certification required (similar to the USA) to become a specialist. The entry requirement does not involve completing core medical or surgical training as in the UK. The areas of practice are also similar to those of the USA, with specialist areas of Neurological Rehabilitation, Musculoskeletal Medicine, Spine, Pain and Sports Injuries. It is our understanding that some European PRM specialists’ also practice in areas of Cardiac, Pulmonary or Cancer Rehabilitation.
The scope of practice in various countries is summarised in Table 2.
Curriculum comparison between countries.

Physical Medicine and Rehabilitation is a developing specialty in countries like India, China and Japan. In these countries, PM&R is based on the model from the USA, with fellowships in specialist areas, but the workforce is thought to be small by comparison to North America/Europe and the model is quite variable in different regions of these countries.
Rehabilitation Medicine in Australia, New Zealand and Singapore is based on the UK model, with practice predominantly focused on inpatient rehabilitation. However, RM in these countries has a broad remit, including the care of neurological conditions, orthopaedic post-surgical cases and systematic deconditioning. In contrast to the UK, many RM specialists in these countries practice in chronic pain.
There are various names for the specialty around the world:
Physical Medicine and Rehabilitation in USA, Canada, India and China.
Physical and Rehabilitation Medicine in most countries of Europe.
Rehabilitation Medicine in some countries of Europe, UK, Singapore and Australia.
Discussion
Currently, the UK NHS is under significant strain with increasing demands being placed on finite resources. Complex multimorbidity is increasingly seen as the norm in UK populations, and medical education, research and clinical services must adapt to meet this growing challenge. The increase in patients attending appointments and being admitted to hospital consists of those with chronic disabling health conditions and complex rehabilitation needs. Many rehabilitation services (eg, musculoskeletal services) are staffed exclusively by non-medically trained therapists and lack dedicated involvement of RM doctors. An expanded RM workforce with a broader skill base and scope would be ideally placed to manage such demand and improve the lives of such patients. In this regard, the Royal College of Physicians (RCP) places emphasis on improving the generalist ability of trainee physicians to meet the needs of the population and RM/ PRM is theoretically well placed in this regard, with the specialty accepting applicants from a broad range of backgrounds in Medicine, Surgery, Psychiatry and General Practice.
A RM/ PRM physician has a wide remit of skills to be a well-rounded physician, and provides holistic, person-centred rehabilitation. A training programme which includes adequate exposure and training opportunities in all subspecialist areas is likely to produce highly skilled RM/ PRM physicians, more attractive in terms of employment potential and able to work in a greater range of acute and community settings alike. Such a sought-after workforce is likely to be able to develop services and respond to variety of needs defined by CCGs.
Patients’ rehabilitation needs are generally complex and not confined to one subspecialty. For example, there is now increasing evidence that most of the benefits noted in patients undergoing neurological rehabilitation is from optimising their physical status. Improved fitness can translate into better cognitive and psychological improvement in these groups of patients. Hence skills in musculoskeletal and exercise medicine will be useful in improving the quality of many rehabilitation programmes and hence outcome for these patients.
The RM workforce in the UK is likely to grow if smaller specialties are integrated back into RM training and service delivery in the future. With a bigger workforce, there will be more awareness of the specialty among medical students, colleagues in other specialties, commissioners and service managers. To match the European average of 3 PRM specialists/100 000 population, there would be a need for around 2000 specialists in the UK (around 10 times the current number). Although there are many physicians already practicing rehabilitation, they are either not RM trained, or are not working under the RM banner. Addressing this discrepancy has obvious advantages in clinical governance, education, quality control and the establishment of national standards. An integrated specialty with a wide variety of practice is likely to be more popular and attract a greater number of junior doctors to consider the specialty as a career. The national society of RM physicians has a key role to drive such an expansion strategy.
Most medical specialties in the UK have the required international equivalence that enables physicians trained here to relate to their peers outside UK, contribute to key developments in the specialty on an international stage and be employable abroad. As we have a relatively small workforce and a narrower scope of practice, we currently do not have the benefits of such equivalence. If we work towards an international model, this position will likely improve and lead to a greater involvement of UK RM physicians internationally which would be stimulating and helpful to all.
In the UK, there is a pressing need to re-vitalise academic RM again. Currently, there is considerable academic output from USA. In Europe, there are moves afoot to develop a Cochrane Collaboration focus group on PMR, and it is important that the UK is represented in this development. There are many areas of potential relevance to the specialty, such as correlating self-report and biomarkers in managing chronic pain and/or functional neurological disorders. Most interventions in RM are complex, involving multiple potential therapeutic contacts/inputs/providers, and using methods that account for this complexity are available. 6 RM is unique in this respect, in that such a research approach is possible within 1 specialty (if neurorehabilitation, neurophysiology and pain specialists were all colleagues working within the same umbrella specialty).
RM in the UK is currently in a disadvantaged position where many small specialties have already emerged that are essentially subspecialties of the specialty outside UK. It is thus important to work towards devising a framework for a wider-scope specialty, which includes multiple subspecialties, such as those listed below.
Musculoskeletal Medicine and Rehabilitation is the most popular subspecialty of PM&R/PRM in other countries. As already highlighted in a UK RM trainee survey in 2011, there is a need to increase training and career opportunities in MSK medicine for RM specialists. 7 Using SEM as an example, when a lack of specialists in this area was highlighted with the 2012 London Olympics on the horizon, creating the specialty of SEM became easier. However, SEM as a standalone specialty has since struggled to prove its returns to the NHS, with most specialists currently working with elite athletes and in the private sports arena. By building links with SEM, RM could put forward a case for merger of the specialties to their mutual benefit, providing a framework for shared training and skills development and producing high-quality specialists working in a single integrated, quality-controlled and clinically relevant specialty.
Clinical Exercise Medicine and Neuromuscular Medicine. Both branches of physiology are core elements that underpin the routine practice and RM would benefit from having expertise in these areas within the specialty. A separate specialty of Clinical Neurophysiology is quite unique in the UK; it is a subspecialty of PM&R/PRM elsewhere. RM/ PRM integration with Neurosciences is likely to become even stronger if core skills in Neurophysiology are made essential to any Neurological Rehabilitation service (including District General Hospital set-up). Physicians practising neurorehabilitation in the USA have these skills and are an integral part of hospital neurology services in the country. Again, a merger of Neurophysiology with RM can be explored to mutually benefit both specialties.
Cardiac and Pulmonary Rehabilitation is ideally delivered by multidisciplinary teams led by a RM/ PRM physician and a case for this has to be put forward with relevant bodies in Cardiology and Respiratory Medicine, and attract the physicians working in these areas to become members of the national RM society, to develop jobs that encompass rehabilitation and to facilitate training our future trainee workforce in these areas.
Cancer Rehabilitation needs to be formally recognised and accredited and develop as a subspecialty of RM/ PRM. RM society needs to encourage non-RM physicians already working in the area to join the national society and facilitate RM expansion.
Pain Medicine and Rehabilitation in the UK is almost restricted to physicians trained in Anaesthesia, whereas more than one-third of Pain physicians overseas are PRM/PM&R specialists. Recent research has proven the value of the bio-psychosocial model for chronic pain management. RM physicians are champions of this approach and are well placed to manage these patients. Managing chronic pain requires a good grounding in Neurology and MSK Medicine that is uniquely available to RM. The British Pain Society needs to facilitate the intake of RM trainees/ post-CCST fellows for Pain fellowships and for consultant positions to the benefit of people with chronic pain, Pain Medicine and RM specialty.
Paediatric Rehabilitation in the UK is currently managed by Paediatricians, and the children are eventually being passed on to adult services, which may or may not be led by RM physicians. Transition to adult services can face multiple difficulties for patients and carers alike and an integrated approach is necessary. Other countries already have Paediatric Rehabilitation specialists’ who belong to the same specialty as those involved in adult rehabilitation. UK needs to encourage Paediatricians working in the area of Neurodisability to work collaboratively with RM to develop a dedicated and seamless Paediatric Rehabilitation service. This will help managing the needs of the paediatric population through transition into adult services and beyond. This is likely to benefit both patients and RM specialty in the long run.
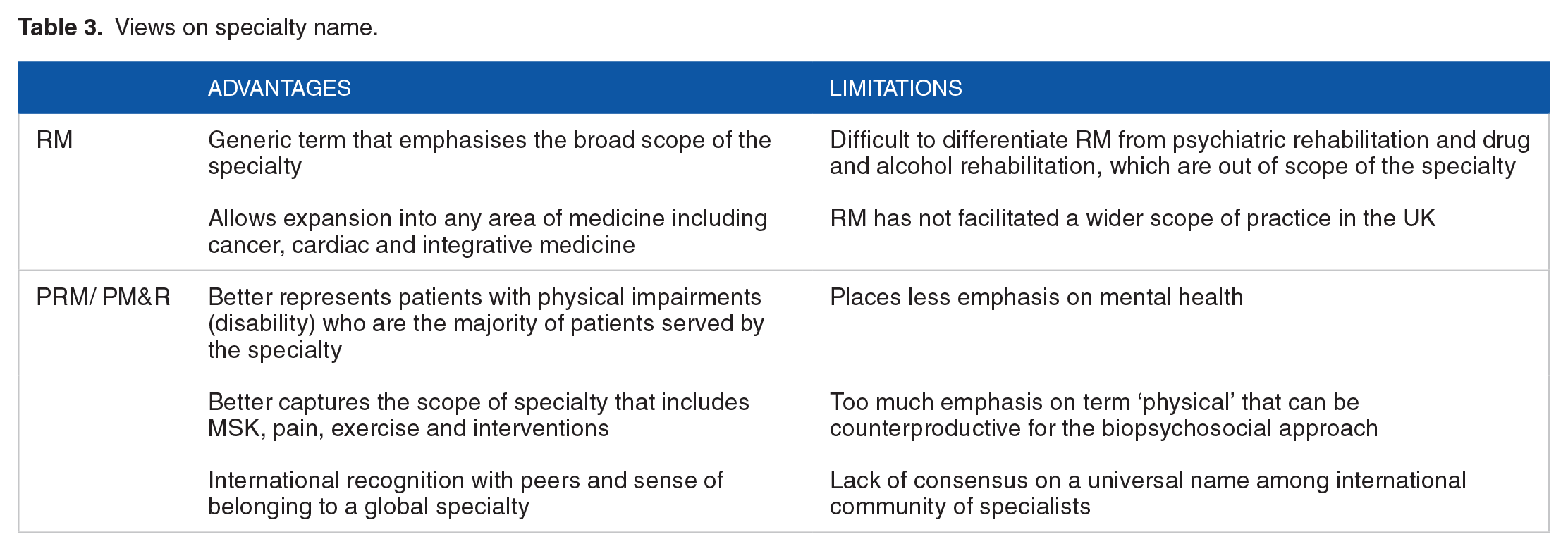
The specialty of RM in the UK needs to consider whether a change of name to PRM/ PM&R is needed to embark on the proposed expansion mission. The existing literature contains ideological debates on the name of the specialty.8,9,10 The views on the different names for the specialty are summarised in Table 3.
Views on specialty name.
Existing, well-established specialties might view the RM proposal as a threat to their expansion. However, we believe that the smaller specialties mentioned in this document may be better placed and prosper in a unified specialty. Reconfiguration and growth of the scope of RM may also positively impact on the acute specialties, allowing them to concentrate on providing the highest quality of acute care. For example, if RM physicians can manage stroke rehabilitation work, acute stroke physicians can focus on dealing with their heavy workload in acute stroke and internal medicine.
Some might view this proposal as moving away from traditional inpatient work involving managing patients with complex long-term neurological conditions. However, it is our view that RM specialists are also responsible for catering to the rehabilitation needs in other non-neurological conditions. The proposed expansion does not mean that every RM physician will have to practise in all subspecialist areas, but it gives them more choice. The proposal aims to promote the creation of a larger and unified specialty with different groups of specialists, driving the clinical and academic work in a wide variety of subspecialist areas. It is anticipated that such a move will also enable RM physicians in the UK to enjoy international equivalence, enhance their ability to interact with and relate to their professional peers elsewhere in the world and work elsewhere if they wish.
Conclusion
In summary, complex multimorbidity and long-term conditions are increasingly common in any population. The NHS in the UK needs to adapt to meet the complex needs of such patients, and RM is, in some ways, uniquely placed to do this. However, the current scope of practice and workforce in RM in the UK is limited compared to that in many other countries worldwide, and the specialty is not yet able to adequately respond to these needs. These limitations exist in a context where other specialties have stepped forward to meet rehabilitation needs in areas of practice outside the current remit of RM in the UK. Targeted expansion of RM, working collaboratively with other relevant specialties, facilitated by the national society, will help build a more robust specialty that can meet the variety of rehabilitation needs in the NHS. This is likely to lead to increased engagement with our colleagues in acute adult specialties, more seamless integration between paediatric and adult services, enhanced links with primary care and a more satisfying career pathway for the doctors working in the specialty of RM/ PRM.
Footnotes
Acknowledgements
The authors would like to thanks the following colleagues for fully supporting this proposal: Professor Mike Barnes (Professor RM Newscastle), Professor Anne Chamberlain (Professor RM Leeds), Professor Jai Kulkarni (Professor RM Greater Manchester), Dr Lloyd Bradley (Consultant RM Chichester), Dr Julian Harriss (Consultant RM London), Dr Tarek Gaber (Consultant RM Greater Manchester), Dr Rajiv Purkayastha (Consultant RM Aberdeen), Dr Ruth Kent (Consultant RM Pinderfields), Dr Ram Hariharan (Consultant in Spinal Injuries Sheffield), Dr Sajida Javaid (Consultant RM Neath), Dr Ashraf Azer (Consultant RM Wirral), Dr Martina Walsh (Consultant RM Birmingham), Dr Clive Bezzina (Consultant RM Stoke on Trent), Dr Zacc Falope (Consultant RM Birmingham), Dr Swaroop Shanbhag (Consultant RM Bristol), Dr Myint Myint Ku (Consultant Stroke and RM Halifax), Dr Moheb Gaid (Consultant RM Norwich), Dr Santanu Sarkar (Consultant RM Aberdeen), Dr Imad Sedki (Consultant RM Stanmore), Dr Kudret Yelden (Consultant RM London), Dr Barbara Chandler (Consultant RM Inverness), Dr Alison McKendrick (Consultant RM Dumfries), Dr Kanchana Devinuwara (Consultant RM Leeds), Dr Laura Smith (Specialist Trainee RM West Midlands), Dr Raef Dahab (Consultant RM Greater Manchester), Dr Anita Singh (Consultant RM Stoke on Trent), Dr Kay Mitton (Consultant RM Greater Manchester), Dr Nina Brixey (Specialty Doctor RM Hull), Dr Javvad Haider (Consultant RM Cardiff) and Dr Pradeep Thumbikat (Consultant in Spinal Injuries Sheffield). The networking and discussion among colleagues was facilitated by the national society of RM physicians (called BSRM when the proposal was originally written in 2016, now changed its name to BSPRM in 2022).
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
MS conceptualised the work. MS, MC, EO, AS, and RS gathered data from the literature and analysed the difference in the scope of practice between countries. All authors contributed to drafting the manuscript, critically revising the work for important intellectual content, approved the final version and agreed to be accountable for all aspects of the work.