
Abstract
Objectives:
To determine incidence of bleeding in thrombocytopenic patients with cancer undergoing acute inpatient rehabilitation.
Design:
This is an observational cross-sectional retrospective study.
Setting:
Acute inpatient academic rehabilitation facility.
Participants:
Adult patients admitted to acute inpatient rehabilitation with functional impairments secondary to cancer.
Methods:
Electronic records were reviewed for thrombocytopenic patients with cancer to determine platelet counts, bleeding events during rehabilitation, and anticoagulant medications prescribed.
Main outcomes measurements:
Type and number of bleeding events, severity of bleeding by World Health Organization criteria.
Results:
Of the 278 patients with cancer admitted to acute rehabilitation over a 27-month time frame, 119 had at least one platelet count <150 000/µL. In all, 37 (31.1%) had a history of a bleeding event prior to the rehabilitation admission and 34 (28.6%) had at least one bleeding complication during their stay. Most events (87.5%) were of low grade (Grade 1 and 2 World Health Organization criteria). There was no association between platelet counts <11 000 or counts 11 000 to 20 000/µL and the occurrence of bleeding (P = .106 and P = .319, respectively). Although anticoagulants were common, there was no association found with a bleeding event and either anticoagulation status (receiving or not on such agents), specific anticoagulant or antiplatelet agents, or a combination.
Conclusions:
Bleeding events in patients with cancer with thrombocytopenia during acute rehabilitation stay are not uncommon but are typically mild in severity and not associated with the degree of thrombocytopenia. Patients taking anticoagulants when platelet levels rose did experience bleeding events, but not at a statistically greater rate than those not taking such medications.
Introduction
Data from the National Cancer Institute (NCI) 1 report that as of 2014, nearly 14.5 million persons in the United States were living beyond their diagnosis of cancer, with this number increasing to an estimated 19 million by 2024. In 2016, the NCI 1 estimated that about 1.6 million new cancer cases were identified. Patients with cancer may experience short- and long-term significant functional impairments as a result of their primary tumor or as a consequence of surgery, radiation, or chemotherapy treatments and thus require rehabilitation interventions to improve function.2–4 Hematologic abnormalities, including thrombocytopenia, are common during active cancer treatment. The presence of low platelet counts, however, has been an ongoing source of concern regarding exercise interventions in this patient population due to a perceived bleeding risk.
In 1986, The Physician and Sportsmedicine published exercise guidelines for patients with cancer, recommending caution with thrombocytopenia and exercise, citing a cutoff level of 50 000 platelets/µL. 5 Oncology texts continue to state that thrombocytopenia of less than 50 000 platelets/µL is a contraindication to resistive exercise. 6 Furthermore, if patients have platelet levels of less than 20 000, exercise should be limited to ambulation, and “no showering or high fall risk activities” are recommended. 6 Maltser et al 7 recommended the same in a review article in 2017.
Despite the acceptance of these recommendations, there have been no conclusive studies indicating an increased risk of complications associated with the exercise levels that patients with cancer with thrombocytopenia experience in acute rehabilitation. Patients with cancer may require transfer to acute inpatient rehabilitation due to significant functional loss and, during rehabilitation, receive physical and occupational therapy several hours per day. 4 However, hematologic abnormalities may be perceived as a reason to delay or stop therapy interventions or require transfer back to acute care, further compounding the weakness and decreased endurance already experienced by these patients due to inactivity from their disease process or treatments.8,9
Studies evaluating the interaction of platelet counts and bleeding during exercise therapy interventions are limited. Low platelet counts have been reported to be a risk factor for transfer from acute rehabilitation back to acute care in patients with leukemia or multiple myeloma. Whether resultant hemorrhagic complications contributed to the increased transfer rate in this prior report, however, is unclear.8,9
As more patients are surviving their initial diagnosis and may be participating in an acute rehabilitation program as their platelet levels diminish, it is important to establish whether exercise in this level of care contributes to complications in the setting of thrombocytopenia. The purpose of this study was to describe rates of bleeding events in patients with cancer undergoing acute inpatient rehabilitation and who had thrombocytopenia during their rehabilitation stay. The hypothesis was that thrombocytopenia would not be related to risk of bleeding events nor would bleeding events result in higher rates of transfers back to acute care.
Methods
This was a retrospective cross-sectional study in which the electronic medical records (EMRs) of all adult patients (18-89 years old) with a primary rehabilitation diagnosis of cancer and who were admitted to a freestanding acute inpatient rehabilitation facility from December 1, 2009, to February 29, 2012, were identified via the hospital’s service code designation, which identifies the primary rehabilitation diagnosis. The charts of all patients with this diagnosis code were initially reviewed for platelet levels, and patients found to have at least one platelet count of less than 150 000/µL at any time during their rehabilitation admission were included for further data review and analysis. Local university institutional review board approval was obtained for the record review required for this study.
All information was recorded from the EMR of these subjects and included demographic information (age, sex) and medical information: primary cancer type, history of prior bleeding events, number and reason for transfers to acute care, prescription of anticoagulant and antiplatelet medications during rehabilitation, and number and severity of bleeding events during rehabilitation. These agents are routinely prescribed to those with moderately low or normal platelet counts without additional contraindications. Cancer type was categorized into 1 of 4 groups for the purpose of evaluating bleeding risk: primary central nervous system malignancy, secondary central nervous system malignancy, solid organ tumor (without brain metastases), and hematologic malignancy. Because of the concerns for intracranial hemorrhage potentially resulting in greater morbidity, primary and secondary brain tumors were classified separately. Hematologic malignancies were identified as a separate category because of the propensity for pancytopenia. As there was no standard protocol at the study institution outlining the frequency of assessing hematologic parameters in this patient population, and frequency of laboratory evaluation was based on individual clinical need, all platelet counts obtained during each subject’s rehabilitation stay were recorded. Counts were stratified into 6 levels: 5 levels of thrombocytopenia (less than 11 000, 11 000-20 000, 21 000-30 000, 31 000-50 000, 51 000 less than 150 000) and normal platelet level (greater than or equal to 150 000/µL). The level with 150 000/µL was chosen as the value for determining thrombocytopenia as this was the lower limit of normal at the study institution at the time of the study. Platelet grouping categories were chosen using the Memorial Sloan-Kettering Exercise Precautions for Cancer Patients with Thrombocytopenia guidelines, institutional guidelines regarding decisions to use or hold antiplatelet agents, and transfusion thresholds. 10
Subjects received 3 to 5 hours of therapy daily, including a combination of physical therapy, occupational therapy, and speech therapy, music/recreational therapy, focusing on improving endurance, independence with functional tasks and mobility. Of note, adjustments in the patient’s therapy program were not made based on platelet counts during the time course of this study regarding number of hours, intensity of therapy intervention, or types of exercises patients performed. Bleeding events occurring prior to admission were identified through review of the admission history and those during the stay through review of physician progress notes and transfer notes. All bleeding complications were rated for severity, based on the World Health Organization’s Bleeding Scale 11 :
Grade 1: “petechial bleeding” (ie, mild, no intervention required);
Grade 2: mild blood loss (clinically significant, but intervention excluding transfusion required);
Grade 3: gross blood loss, severe, requires transfusion (transfusion ± transfer to acute care);
Grade 4: Debilitating blood loss, retinal or cerebral, associated with fatality.
For patients with any bleeding event during the rehabilitation stay, platelet counts within (±) 1 day of this bleeding were identified. Any potential precipitants around the time of the bleeding complication, such as falls or bleeding occurring during therapy sessions, were noted. Additional information was also identified regarding any interventions required as the results of the bleeding event and whether transfer to an acute care hospital was required.
Statistical analyses
Descriptive statistics were computed to characterize the sample. Crosstabs with Pearson’s χ2 statistic and independent samples t tests for variables with normal distributions were used. For variables with non-normal distributions, independent samples Mann-Whitney U test was used. IBM SPSS version 22 was used for all statistical analyses.
Results
A total of 282 adult patients were initially identified as being admitted to the rehabilitation facility with rehabilitation needs due to a cancer diagnosis over the specified time frame. Four patients were omitted from further review as an alternative diagnosis leading to the rehabilitation admission was identified on initial chart screening. From the remaining 278 patients, 119 had at least one platelet count of <150 000/µL during their inpatient rehabilitation stay. Information on patients with readmissions over the study time frame was counted as one subject. There were slightly more male (52.9%, n = 63) than female patients identified meeting these criteria, and 86.6% (n = 103) were 51 years of age or older (see Table 1). Length of stay for these patients ranged from 2 to 111 days with a mean of 22.8 days. Cancer diagnosis type within this data set was broad as noted in Table 1.
Patient demographics and cancer characteristics.
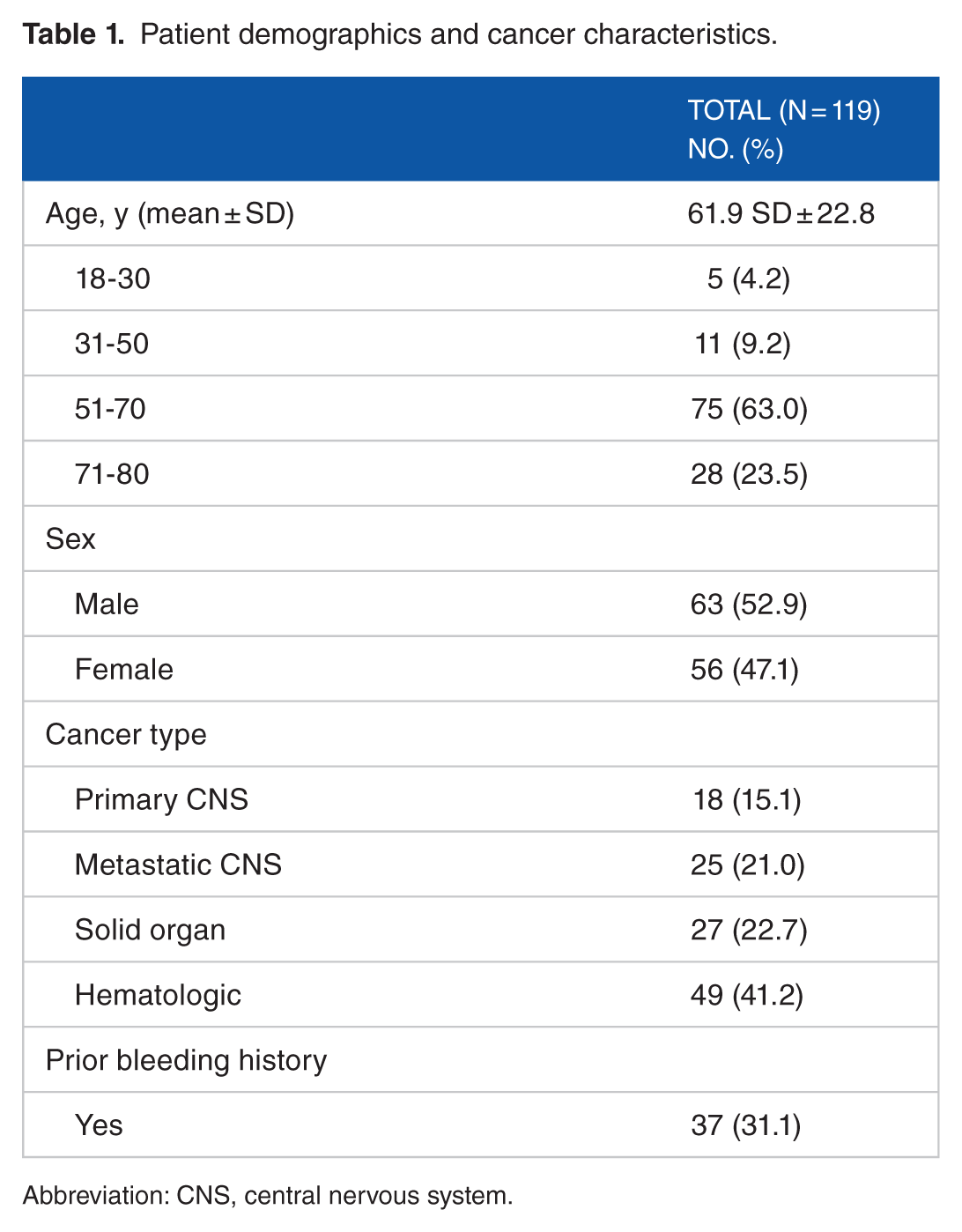
Abbreviation: CNS, central nervous system.
In all, 112 patients had undergone active treatment for their cancer within the past 6 months and 37 (31.1%) had a history of a bleeding event documented prior to the rehabilitation admission. In these 119 subjects, platelet counts were measured 1205 times. About 27.5% (n = 331) of the recorded platelet counts were 50 000/µL or less, and 0.7% (n = 9) were less than 11 000/µL (Figure 1).

Platelet recordings during rehabilitation.
Of the 119 subjects, 34 (28.6%) had at least one bleeding complication during their rehabilitation stay, with 12 having multiple for a total of 56 bleeding events occurring during admission. There was no statistical relationship found between bleeding event during rehabilitation and age or a prior bleeding history. Types or locations of these bleeds included superficial skin or subcutaneous tissue (n = 20), hematuria (n = 12), gastrointestinal/hemorrhoidal bleeding (n = 11), epistaxis (n = 10), other (n = 2), and intracranial (n = 1). Most events (87.5%, n = 49) were of mild severity, Grade 1 and 2 by World Health Organization criteria. About 5.8% (n = 7) of the bleeds were Grade 3. This information is presented in Table 2.
Number of bleeding events according to severity.

In all, 31 subjects had multiple admissions during the designated study time frame; however, most transfers from acute rehabilitation were not bleeding related. Three subjects (1 transfer each) returned to acute care due to bleeding events. Two patients were transferred with lower gastrointestinal bleeds, each receiving prophylactic low-molecular-weight heparin. One subject had a platelet count of 23 000/µL on the day of transfer and the other 101 000/µL. The third patient, also on a prophylactic dose low-molecular-weight heparin, was transferred to acute care for a retroperitoneal bleed with a platelet count of 130 000/µL on the day of transfer. Platelet counts recorded nearest to the time of bleeding and bleeding event by severity are presented in Figure 2.

Frequency of bleeding events according to severity and platelet level. WHO indicates World Health Organization.
There was no association found between platelet counts and bleeding event severity, including very low platelet counts (less than 11 000 or 11 000-20 000/µL (P = .106 and P = .319, respectively). Although a higher number of bleeding events occurred when platelet counts were 51 000/µL or greater (35/56 bleeding events), this was not statistically significant.
Patients were often on anticoagulants during their inpatient stay either for prevention or treatment of thromboembolic complications, except, as anticipated, those patients with very low platelet counts. In all, 26 (76.4%) patients with bleeding events received antiplatelet or anticoagulants within 2 days of bleeding. However, no specific anticoagulants or antiplatelet agents, combinations of these medications, or lack of anticoagulant/antiplatelet agent use around the time of the bleeding was statistically associated with a bleeding event (Figure 3). It was noted, however, that the patients who required transfer out to an acute care hospital due to bleeding were all receiving prophylaxis doses of low-molecular-weight heparin at the time of the bleeding event.

Anticoagulation status at the time of bleeding event. LMWH indicates low-molecular-weight heparin.
Discussion
This study is the first to describe the frequency and types of bleeding events in oncology patients with thrombocytopenia undergoing inpatient rehabilitation. Although bleeding events were not uncommon, with 28.6% (n = 34) of patients experiencing a bleeding event during rehabilitation, most were mild in severity. In addition, these bleeding events were not associated with very low platelet counts. Thus, additional information is provided in this study for health care providers assessing patients with cancer for appropriateness of admission to acute rehabilitation or those caring for this patient population in rehabilitation settings.
An early study of patients with cancer evaluating the association between thrombocytopenia and hemorrhage found increased intracranial hemorrhage rates with platelet counts of less than 20 000/µL. 12 This then became the de facto threshold for transfusion and limiting or excluding patients from exercise. 13 Although transfusion recommendations have been updated, the concern for hemorrhage due to exercise has persisted.6,13 Studies of patients with malignant neoplasms undergoing inpatient rehabilitation have consistently found increased rates of transfer out to acute care relative to other rehabilitation populations.4,14 A recent study found that the odds of transfer out was 2.5 times greater for this population. 14 Bleeding, however, has not been identified as the most common cause of transfer, even in the setting of thrombocytopenia.8,14 Fu and colleagues8,9 reported that platelet counts were one of the factors associated with transfer back in bone marrow transplant patients and patients with multiple myeloma but did not specifically cite bleeding as an associated complication. Indeed, infectious complications rather than bleeding have often been a common reason cited for transfer in this and other studies of cancer populations. 14
Chest Guidelines for Prevention of Venous Thromboembolism in Nonsurgical Patients summarized data from an ongoing registry entitled IMPROVE, regarding multiple independent risk factors for bleeding in 10 866 medical patients hospitalized in acute care, including patients with cancer and thrombocytopenia. 15 Concomitant exercise or rehabilitation interventions were not factored into their analysis. 16 This study found that 9.5% of patients with platelet counts of <50 000 at admission had at least one bleeding event within the first 14 days of acute care admission, and 3.7% of patients with cancer experienced at least one bleeding event. 16 Although the incidence of bleeding was lower for patients with cancer in that study compared with this study, they did not specifically evaluate incidence in patients with cancer who also had concomitant thrombocytopenia or other bleeding risk factors. 16 More importantly, that study evaluated patients for “major bleeding, or clinically relevant non-major bleeding” in contrast to this study which included all recorded bleeding events. When comparing levels of major bleeding events only (World Health Organization Grade 3), which is similar to the criteria used in the analysis of data from the IMPROVE database, the bleeding rate in this study was similar at 5.8%. No statistically significant association was found for bleeding events that occurred during rehabilitation in those with a history of prior bleeding events. These findings are contrary to findings from the IMPROVE database, where the odds ratio for new bleeding in patients with a history of prior bleeding in the past 3 months was 3.64. 16
It is unclear why the bulk of bleeding events in this study occurred in patients with higher platelet counts. Potentially, this finding was due to a key threshold in care change. At the study institution, unless there is a specific contraindication or concern, it has been standard practice to consider initiation of venous thromboembolic chemoprophylaxis once platelet levels reach 50 000 or above.
It is important to note that the patients included in this study were often on agents to prevent or treat thromboembolic events at some point in their rehabilitation stay. The use of anticoagulants in patients with cancer with thrombocytopenia, either for treatment of venous thromboembolism or for prophylaxis, is not well-studied. Indeed, a recent review of the use of anticoagulants in adult patients with cancer found that firm conclusions regarding the use of such agents were difficult to determine due to the lack of critical information in the literature. 17 Analogous findings are described in the International Clinical Practice Guidelines for the Treatment and Prophylaxis of Venous Thromboembolism in Patients with Cancer. These guidelines also reported limited evidence in the literature related to bleeding risk in patients with cancer with thrombocytopenia, particularly regarding anticoagulation use. 18 This international consensus working group of experts in their recent systematic review found no study evaluating the pharmacologic of prophylaxis of venous thromboembolism in patients with cancer with thrombocytopenia, concluding that bleeding risk with administration of these agents in this specific patient population overall is unknown. 18
A study evaluating subjects continuing venous thromboembolism prophylaxis following acute care, some with a diagnosis of cancer, found that 3.9% of subjects prescribed anticoagulants experienced a major bleeding event compared with 1.9% of subjects who were not taking anticoagulants. 19 Rehabilitation or exercise was not mentioned as a cofactor analyzed. 19 Furthermore, a critical evaluation of bleeding risk in rehabilitation patients with these clinical findings has also not been done. Although bleeding incidence in this study in this higher risk group of patients with cancer was not independently associated with anticoagulant use, it is notable that all 3 of the patients who were transferred out in this study were on low-molecular-weight heparin at the time of transfer.
Findings of limited severe bleeding complications are similar to those of a recent Cochrane review evaluating patients with cancer with hematologic malignancies participating in aerobic exercise compared with standard care. 20 This Cochrane review did not find an increase in serious adverse events. However, their patient population for study was limited to those with hematologic malignancy, exercise was limited primarily to aerobic intervention, and severity of thrombocytopenia was not taken into account. 20 It is also important that acute inpatient rehabilitation therapy provides more than aerobic exercise instead including a variety of exercise interventions, including resistive as well as stretching and training in functional tasks. This study also includes those with intracranial tumors for which any interventions which increase bleeding may be particularly concerning.
Findings in this study support the hypothesis that patients with cancer as their primary impairment can safely undergo inpatient rehabilitation even with low platelet counts. Safety with the use of venous thromboembolism prophylaxis in patients with cancer undergoing inpatient rehabilitation in the setting of mild or moderate low platelet levels is less clear however. Although there was no association found for bleeding risk with the use of venous thromboembolism prophylaxis in those individuals with mild or moderate low platelet levels, further study appears to be warranted. This study supports that platelet parameters with anticoagulant use for venous thromboembolism prevention need to be studied in combination, including in the rehabilitation of patients with cancer.
Limitations
This study is limited by the retrospective design. Lab monitoring was not performed at specific intervals across all patients, and thus there was some variability on the timing of the platelet levels in relation to the bleeding event. In addition, this was a single-center study of patients in inpatient rehabilitation, so findings may not be generalizable to acute care settings where therapy is performed and should be confirmed in other rehabilitation units or hospitals in this population.
Conclusions
Bleeding events in thrombocytopenic patients with cancer undergoing inpatient rehabilitation are common but typically mild based on established criteria. Bleeding events and severity did not differ by platelet levels, age, cancer type, or anticoagulation status. Future research evaluating oncology patients in rehabilitation at risk for these events is needed, which should include a more standardized protocol of monitoring platelet levels. Comparing rates of bleeding complications with other populations undergoing inpatient rehabilitation would also be of interest.
Footnotes
Acknowledgements
This project was presented in abstract form at the American Academy of Physical Medicine and Rehabilitation Annual Assembly, 2011, in Kissimmee, Florida.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, and/or analysis and interpretation of data. All authors participated in drafting the article or revising it critically for important intellectual content. And, all authors gave final approval of the submitted and revised versions of this manuscript.