
Abstract
The use of chemotherapy in premenopausal cancer patients may lead to chemotherapy-induced premature ovarian failure. Pharmacological temporary ovarian suppression obtained with the gonadotropin-releasing hormone agonist (GnRHa) administered concomitantly with chemotherapy has been investigated as a technique capable to reduce the gonadotoxicity, reducing the risk of developing premature menopause. In recent years, important evidence has become available on the efficacy and safety of this strategy that should now be considered a standard option for ovarian function preservation in premenopausal breast cancer patients. However, in women interested in fertility preservation, this is not an alternative to cryopreservation strategies, which remains the first option to be proposed. The purpose of this review is to summarize the mechanisms of GnRHa in the preservation of fertility in premenopausal cancer patient candidates to receive chemotherapy, highlighting the areas of doubt that require further investigation.
Introduction
The increase in cancer incidence in premenopausal patients and the significant improvement in their prognosis have brought concerns about the possible consequences of the treatment on their reproductive life. 1 The most relevant side effect of chemotherapy for younger cancer survivors is the induced transient or permanent amenorrhea with resultant vasomotor symptoms and distress related to the concern about infertility. 2
In addition, many young women have not been mothers yet at the time of cancer diagnosis, but they wish to have children after the end of treatments. 3
Therefore, according to international guidelines, the risk of developing chemotherapy-induced premature ovarian insufficiency (POI) should be discussed after diagnosis with all young patients, before anticancer treatments.4,5 For young patients interested in preserving their fertility, the standard available strategies (ie, embryo and oocyte cryopreservation) should be primarily proposed, although these strategies cannot prevent the risk of iatrogen POI with its associated psychosocial and menopause-related concerns.
A pharmacological protection of the ovaries induced by the administration of gonadotropin-releasing hormone agonist (GnRHa) concomitantly with chemotherapy has been studied as a strategy able to reduce the gonadotoxicity of chemotherapy by reducing the likelihood of developing POI. Although this topic is still debated, recent research efforts have better clarified the efficacy and safety of temporary ovarian suppression with GnRHa during chemotherapy and this strategy is recommended for premenopausal breast cancer patients candidates to receive systemic anticancer therapies.4–6
The aim of the current review is to provide an overview on the protective mechanisms on ovaries induced by the administration of GnRHa concomitantly with chemotherapy, focusing on the biological rationale.
Biological Rationale
During the reproductive life, there is a balance between ovarian follicles in the quiescent and in the growing phase. After being in the preantral stage, the development of the follicle depends on the gonadotrophins (follicles-stimulating hormone [FSH] and luteinizing hormone [LH]) that stimulate the proliferation of granulosa cells, the differentiation of theca cells and steroidogenesis. 7
Ovarian toxicity caused by chemotherapy is exerted through different events, involving all follicular stages and cell types:
A direct ovarian tissue’s toxicity, primarily described for alkylating and platinum agents, may deplete the follicular pool with a dose-dose-dependent mechanism, revealed by the apoptosis of primordial follicles and of pregranulosa cells.
A vascular toxicity characterized by reduction in ovarian blood flow and disintegration of the vessel wall may mediate end-organ (ie, ovarian) damage. It has been reported only with anthracycline exposure.
Direct cellular effects on various components of the ovary have been shown for several classes of chemotherapies that differ on their specific cellular targets (eg, cytoskeleton for taxanes, DNA for anthracyclines and platinum compounds, antioxidant enzymes for alkylating agents, anthracyclines and platinum compounds).8,9
Therefore, pharmacological protection should reduce toxicity on ovaries at various levels.
The mechanisms used by GnRHa to protect the ovarian function by the damage of cytotoxic agents are not fully understood yet. To date, 5 different effects have been hypothesized, directly or indirectly (Figure 1).
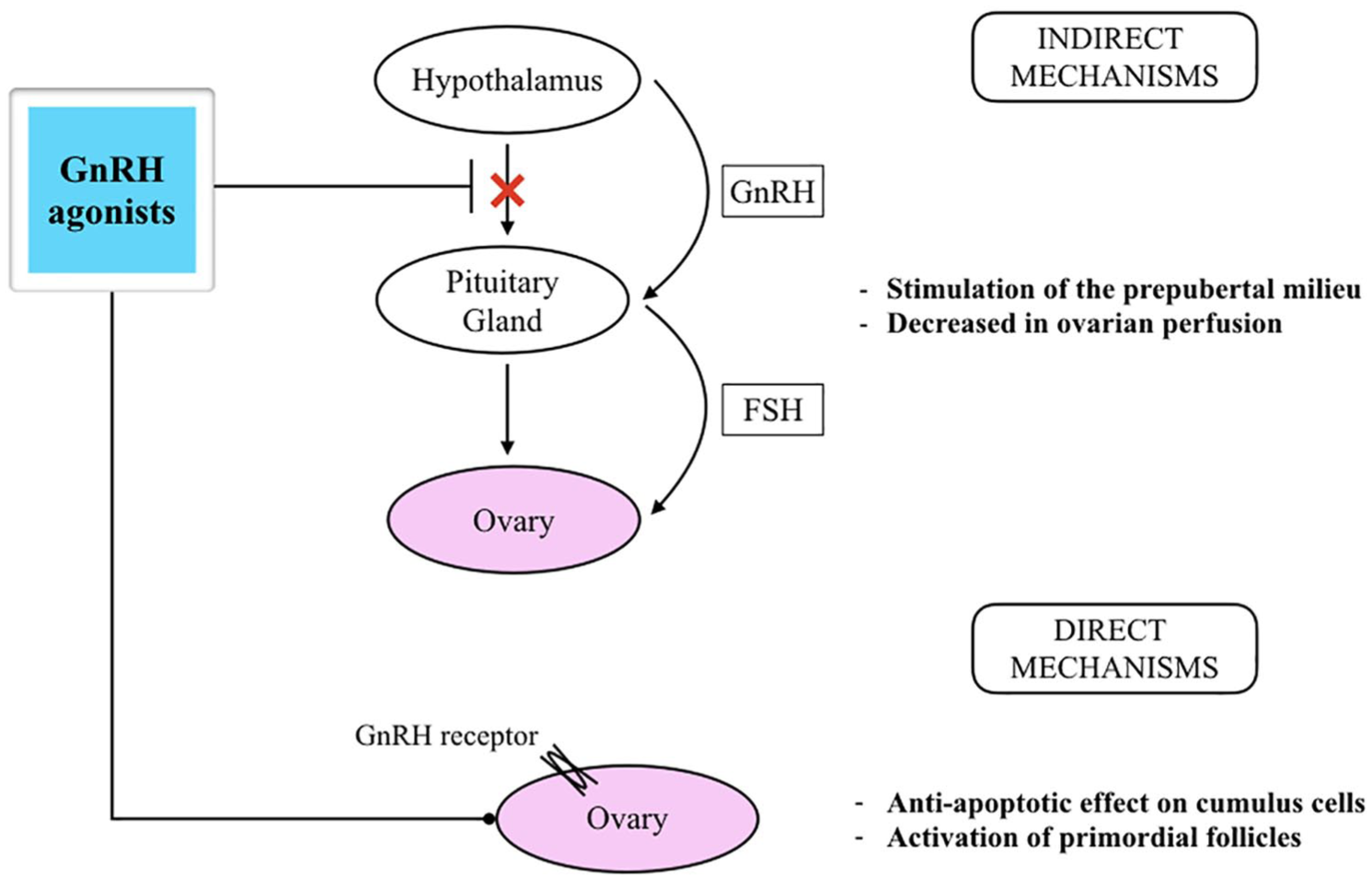
GnRHa administration concomitantly with chemotherapy: conceivable mechanisms of ovarian protection (modified from) 7 . FSH indicates follicles-stimulating hormone; GnRHa, gonadotropin-releasing hormone agonist.
Simulation of the prepubertal, hypogonadotropic milieu
The administration of GnRHa induces an initial release of gonadotropins (the “flare-up effect”) which desensitizes the gonadotropin-releasing hormone (GnRH) receptors on the pituitary gonadotropes, preventing from the pulsatile GnRH secretion to perform its physiological action. 10 This generates a hypogonadotropic, prepubertal milieu, in which the follicles are kept in the quiescent phase, and thus less vulnerable to chemotherapy-induced gonadotoxicity. 11 This mechanism has been considered controversial, because of the dogma that the primordial and primary follicles are not dependent on gonadotropin and without FSH receptors. However, the advanced antral follicles, which are gonadotropin-dependent, secrete many growth factors (such as the transforming growth factors superfamily, the bone morphogenic proteins, activin, and others), which enabled to the growing of primordial and primary follicles with a paracrine way. Therefore, cytotoxic agents promote the death of the follicles, with decreased levels of estrogen and inhibin, causing the increase of FSH, and consequently the unidirectional way of apoptosis (the so-called “burn-out effect of chemotherapy”). The concomitant administration of GnRHa and consequent decreasing of FSH levels lead to minimize the further recruitment of primordial follicles and their burn-out. 10 Moreover, growing follicles secrete also other factors including the antimullerian hormone (AMH), that can negatively regulate the primordial follicles pool. During chemotherapy, AMH levels decreased, promoting the burn-out effect of chemotherapy. Therefore, the administration of GnRHa prevents gonadotoxicity of chemotherapy on growing follicles producing AMH, limiting the burn-out effect. Preclinical studies conducted demonstrated that rats treated with GnRHa and cyclophosphamide have decreased levels of AMH, confirming the potential protective effect of GnRHa through the regulation of AMH levels during chemotherapy. 12
Decrease in ovarian perfusion
The presence of elevated levels of estrogens significantly increases ovarian perfusion and this mechanism is inhibited by administration of a GnRHa. The treatment with GnRHa decreased the ovarian perfusion, resulting in a lower total cumulative exposure of the ovaries to the antineoplastic drugs, and consequently less gonadotoxicity. 13
Direct effect mediated effect through the GnRH receptors on ovaries
This effect is poorly understood, nevertheless it has been observed that GnRH receptors are expressed on ovaries surface, and their activation may result in a reduction of apoptosis, by stimulating the oocyte maturation and follicular destruction.14,15
Possible up-regulation of an antiapoptotic molecule
The sphingosine-1-phosphate (S1P) is an antiapoptotic molecule that acts with the inhibition of the ceramide pathway implicated in chemotherapy-induced apoptosis in the ovaries; moreover, this molecule exerts also a protective effect of the primordial ovarian follicles, by improving neoangiogenesis. 16 It has been observed that S1P exposure prevents cyclophosphamide- and doxorubicin-induced oocyte death in vivo in different species, 17 and oocytes without expression of sphingomyelinase are resistant to doxorubicin-induced apoptosis in vitro. 18 Nevertheless, no experimental evidence supports fully whether the GnRHa treatment activates the receptors in the ovaries and possibly an intraovarian increase of S1P or other antiapoptotic factors.
Possible protection of the ovarian germinative stem cells
Johnson et al 19 demonstrated the presence in the ovary of germ line stem cells, with mitotical activity able to reconstitute the primordial follicle pool. This finding contradicted the fundament of reproductive human biology, based on the assumption of a fixed reserve of germ cell in the mammalian females, without the ability of renewal.
The administration of GnRHa may interact with these germ cells through some pathways essential for the cell growth and for the activation of primordial follicles after chemotherapy exposure.20,21
Antiapoptotic effect on cumulus cells
Recently, for the first time, a culture system of ex vivo human immature cumulus cell-oocyte complexes was used to investigate whether GnRHa administration was able to protect the oocytes from chemotherapy injuries become available. The human complexes were cultured with chemotherapy alone (ie, cyclophosphamide) or GnRHa alone or both. Effects of these treatments were evaluated on GnRH receptors, apoptosis pathways, ceramide pathway, and glutathione synthesis.
The authors showed that cyclophosphamide concentration was mainly detrimental to the cumulus cell compartment, and this effect was partially counteracted by GnRHa.
Furthermore, the co-administration of GnRHa and chemotherapy preserved the cumulus complex from a morphological point of view, without impact on the oocytes, thanks to the surrounding granulosa cells.
The authors hypothesize that GnRHa directly acts on cumulus cells to protect the oocytes from chemotherapy by an antiapoptotic effect. This is in contrast with previous data that excluded a protective role of GnRHa against cyclophosphamide in ex vivo and in vitro models of human ovary and granulosa cell. 22 The difference may be due to the different timing of GnRHa administration: in fact, in the study conducted by Bildik, GnRHa was administered at the same time of chemotherapy, whereas in the study by Scaruffi et al, the incubation with GnRHa started 24 hours before the addiction of chemotherapy. Thus, a prior and longer exposure to GnRHa facilitate in the cumulus cells and indirectly in the oocytes the activation of the molecular pathways, leading to decrease ovaries toxicities and follicular apoptosis during chemotherapy.
In conclusion, these results supported the indirect protective gonadal effect of GnRHa treatment concomitantly with chemotherapy, mediated through the cumulus cells (P Scaruffi et al., personal data).
Clinical Evidence in Breast Cancer Patients
Most studies available on the role of GnRHa during chemotherapy as a strategy to preserve ovarian function and potential fertility have been conducted in premenopausal women with breast cancer23–38 (Table 1).
Main results of the randomized trials conducted to evaluate the efficacy of temporary ovarian suppression with GnRHa during chemotherapy in young breast cancer patients.

Abbreviations: CT, chemotherapy; E2, estradiol; FSH, follicle-stimulating hormone; POF, premature ovarian failure.
Of 14 randomized trials, 10 reported that temporary ovarian suppression with GnRHa concomitantly with chemotherapy significantly decreased the premature ovarian failure in premenopausal women with breast cancer. Notably, a large heterogeneity among these trials should be highlighted: the timing of the assessment of the premature ovarian failure rate ranged from a minimum of 6 to 72 months, only few trials used the composite end point (amenorrhea and postmenopausal levels of FSH and estradiol) to define the premature ovarian failure.
Furthermore, a recent meta-analysis of individual data of the major 5 randomized trials showed a significant reduction in the risk of developing POI (adjusted odds ratio = 0.38; 95% confidence interval [CI] = 0.26-0.57) and significant higher chances to be pregnant after treatments (incidence rate ratio = 1.83; 95% CI = 1.06-3.15) in young breast cancer patients treated with GnRHa during chemotherapy, without impact on long-term outcomes. 39 These results provided a substantial clinical evidence on the efficacy and safety of this strategy to improve both ovarian preservation and fertility.
Conclusions
Several efforts of research in this field were conducted through the last years, but the mechanism of action of GnRHa to induce temporary ovarian suppression is not still clearly identified. Nevertheless, recently updated guidelines on this topic strongly recommend the use of temporary ovarian suppression with GnRHa in premenopausal breast cancer patient candidates to receive chemotherapy.1,4,5
This technique has some advantages: the easy and not invasive administration, the possibility to preserve not only the fertility but the whole ovarian function, and finally this technique is not mutually exclusive with the other strategies (ie, cryopreservation strategies).
The administration of GnRHa should be proposed to all premenopausal cancer patients interested to preserve their ovarian function and reduce the risk of developing chemotherapy-induced premature ovarian failure, irrespectively of their motherhood desire. This technique should be performed at least 1 week before chemotherapy, and it has the potential to avoid the menopausal signs and symptoms, and the detrimental long-term consequences.
However, the role of the temporary ovarian suppression obtained with GnRHa in the fertility preservation may be considered cautionally. Moreover, the standard cryopreservation strategies should be proposed for the first, and temporary ovarian suppression with GnRHa should also be proposed after these surgical techniques.
Considering that the mechanisms of action of GnRHa to protect ovaries during chemotherapy are still unclear, further research efforts are needed to better clarify this topic.
Footnotes
Acknowledgements
Matteo Lambertini acknowledges the support from the European Society for Medical Oncology (ESMO) for a Translational Research Fellowship at the Institut Jules Bordet in Brussels (Belgium).
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by AIRC (Associazione Italiana per la Ricerca sul Cancro) [grant number IG 2013-14272].
Declaration of Conflicting Interests:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Lucia Del Mastro received honoraria from Takeda and personal fees from Ipsen and Takeda outside the submitted work. Matteo Lambertini served as a consultant for Teva and received honoraria from Theramex outside the submitted work. All other authors declare no conflicts of interest.
Author Contributions
All the authors contributed equally to the work.