
Abstract
Background:
The pattern of paediatric kidney diseases across different regions is influenced by genetic, racial, and environmental differences.
Objectives:
The aim of this study was to review the current spectrum and outcome of childhood kidney diseases at Parirenyatwa Group of Hospitals and highlight the challenges of care.
Design:
Retrospective observational study.
Methods:
Data on all children below 16 years of age hospitalised for any kidney disease over an 8-month period (1 January-31 August 2022) were retrieved and retrospectively analysed. Kidney diseases were categorised as per standard definitions.
Results:
Kidney disease accounted for 2.2% (n = 50) of all 2264 admissions in the paediatric unit, with males constituting 60% (n = 30). Age ranged from 2 weeks to 13 years (mean 5.5 ± 3.5 years) with 58.0% being under 5 years. The commonest diagnoses in the unit were acute kidney injury (AKI) (n = 16, 32%) nephrotic syndrome (n = 16, 32%), hypertension (n = 12, 24%) and end stage kidney disease (ESKD) (n = 11, 22%) with some children presenting with more than 1 diagnosis. Only 3 out of 11 children with ESKD and 3 out of 8 children with AKI who required dialysis could be offered dialysis due to limited resources. Overall mortality rate was 32% (16/50): 5 children with AKI, 2 with nephrotic syndrome and normal kidney function, 8 with ESKD and 1 with Fanconi syndrome.
Conclusion:
Childhood kidney disease contributes significantly to hospitalisations at our institution with highest mortality among children with ESKD. The study highlighted the need for provision of essential drugs and kidney replacement therapy for children with kidney disease at our institution.
Introduction
Kidney disease in children constitutes an important cause of morbidity and mortality. There is increasing prevalence of chronic kidney disease (CKD) globally with an annual incidence rate of 8%.1-4 The pattern of paediatric kidney diseases across different regions is influenced by genetic, racial and environmental differences. 5 Acute kidney injury (AKI) and nephrotic syndrome are the most reported paediatric kidney diseases in Africa. 6 In contrast, the prevalence of chronic kidney disease and congenital anomalies of the kidneys and urinary tract remains low due to the unavailability of screening or antenatal ultrasound investigations resulting in underestimation. The absence of comprehensive National Renal Registries across the continent (except for South Africa/Egypt/Tunisia) means the true burden of end-stage kidney disease (ESKD) in children is largely unknown and infrequently reported. 6 As a result, there are insufficient data to guide resource allocation.
The proportion of kidney-related admissions to secondary and tertiary hospitals across Africa varies widely from 3.5% to 8.9%. 7 The most commonly documented kidney diseases are nephrotic syndrome, acute glomerulonephritis (AGN), AKI, urinary tract infection and congenital anomalies of the kidney and the urinary tract (CAKUT) with varying incidences.2,7-9 Reported risk factors for CKD among children in sub-Sahara Africa (SSA) include intrauterine injury to the developing kidney, malnutrition in childhood, parasitic infections, post infectious glomerulonephritis, HIV related nephropathy, sickle cell disease and AKI especially due to diarrhoeal diseases.10-14 Community-based studies have reported average proteinuria prevalence of 32.5% (2.2%-56.0%), average haematuria prevalence of 31.1% (0.6%-67%), and imaging abnormalities found in 14.8% (0.5%-38.0%) among children in SSA. 10
A few studies analysing paediatric kidney diseases have been conducted in Zimbabwe. An AKI prevalence of 33% among admitted term neonates has been reported at one tertiary hospital in the country. 15 Among anti-retroviral therapy (ART) naïve children living with HIV, the prevalence of urinary tract infection was 9.5%, persistent proteinuria of 5% and renal impairment in 34.6%. 16 Reduction in estimated glomerular filtration rate (eGFR) < 90 ml/min/1.73 m2 and proteinuria was evident in 35.9% and 32.8% of children, respectively for those on ART. 17 However, there is still paucity of local data on kidney diseases in admitted children in Zimbabwe. The aim of this study was to review the current spectrum and outcome of childhood kidney diseases in the Paediatric Unit of Parirenyatwa Group of Hospitals (PGH) and highlight the challenges of care.
Methodology
Study centre and population
The study was conducted at Parirenyatwa Group of Hospitals (PGH), a tertiary/quaternary hospital in the capital city of the country, Zimbabwe. It is a state-owned hospital which is one of the main referral hospitals in the country for all complex medical and surgical conditions. Majority of patients are from low- and middle-income classes of society. All paediatric kidney conditions which require a nephrologist are referred to the PGH paediatric renal unit. There are no user fees for children below 5 years of age for services rendered including investigations. There is currently no financial support for those above 5 years who are unable to afford care. Peritoneal and haemodialysis is available free of charge; however, the main challenge is availability of consumables such as catheters, dianeal solutions and paediatric haemodialysis blood lines and filtres necessary for these procedures. Haemodialysis is offered to children above 15 kg body weight while those below only receive peritoneal dialysis. The unit does not offer kidney transplant services.
Data collection
Data on all children admitted over an 8-month period (1 January - 31 August 2022) were retrospectively retrieved from the renal unit database and analysed. This included demographic data, clinical history, investigations, diagnosis, disease outcome and procedures such as dialysis. Inclusion criteria were age (birth to 16 years), and ward admission with diagnosis of a kidney disease. Children admitted with primary surgical diagnosis in the surgical wards were excluded from the study. Kidney Disease: Improving Global Outcomes (KIDGO) classification was used to define AKI, 18 Chronic kidney disease (CKD) 19 and Nephrotic syndrome. 20 Diagnosis was based on history, physical examination and laboratory investigations such as urinalysis, urine microscopy, blood chemistry and haematology. Results of imaging such as ultrasonography were recorded.
Data analysis
Data were analysed using Statistical Package for Social Sciences (SPSS). Continuous data were represented as mean (SD) or median (IQR) as appropriate while categorical data were presented as percentages. The incidence of childhood kidney disease was calculated as a proportion of the total number of paediatric admissions diagnosed with a kidney condition. Case fatality rate was calculated as a proportion of the total number of deaths in children with kidney disease over the study period.
Results
Of the 2264 children admitted during the study period, 50 had kidney disorders giving an incidence of 2.2% (22 per 1000 admitted children). Majority were male (n = 30, 60.0%). Age ranged from 2 weeks to 13 years (mean 5.5 ± 3.5 years) with 58.0% being under 5 years (Table 1). Overall, 123 children admitted in the paediatric unit died during the study period with 16 (13.0%) of these having kidney disease (case fatality rate of 32% (16/50). Of the 16 children with kidney who died 8 had ESKD, 5 had AKI, 2 with nephrotic syndrome and normal kidney function and 1 with Fanconi syndrome.
Age and gender distribution of children admitted with kidney disease.

The commonest diagnoses in the 50 children with kidney diseases in the unit were AKI (n = 16, 32%) nephrotic syndrome (n = 16, 32%), hypertension (n = 12, 24%) and ESKD (n = 11, 22%) (Figure 1). Hypertension was diagnosed in 1 child with neuroblastoma, 3 with nephrotic syndrome, 3 with ESKD and 5 with glomerulonephritis. Of the 5 cases of glomerulonephritis 2 had rapidly progressive disease. One 7-year-old boy had pyelonephritis with posterior urethral valves and ESKD while a 12 years old girl who presented with seizures, bi-cytopenia, skin rash and severe joint pains that had rendered her bed ridden for 2 months, had systemic lupus erythematosus (SLE) that was managed successfully with steroids and cycles of cyclophosphamide.

Indications for admission into the renal unit.*
Nephrotic syndrome
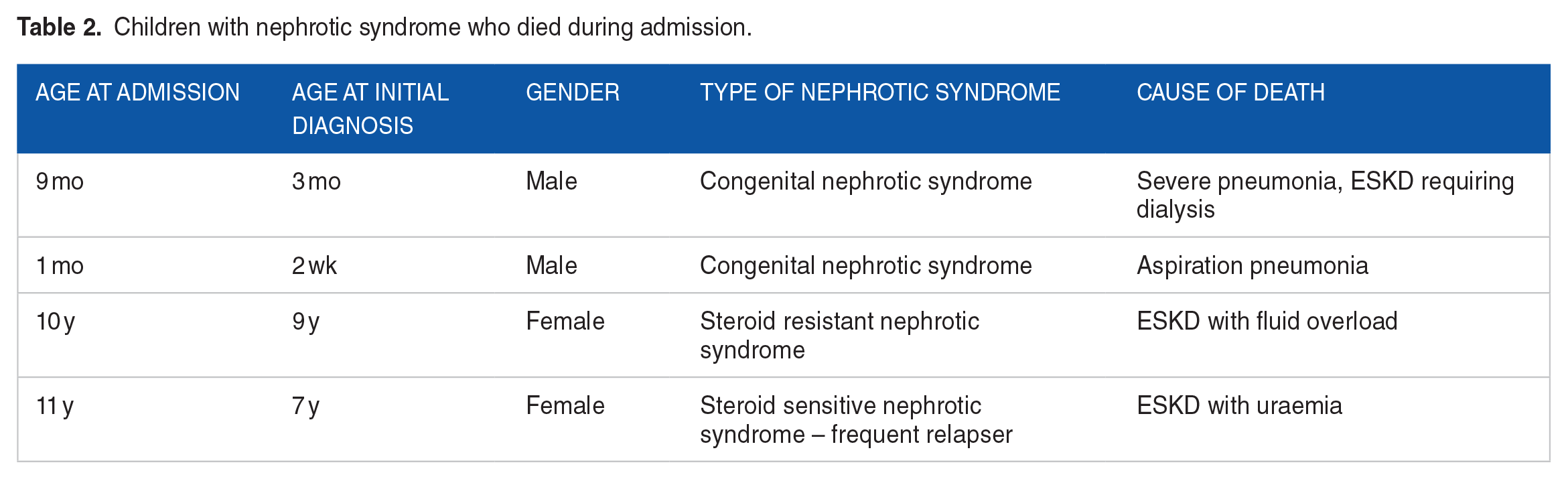
Of the 16 cases of nephrotic syndrome, 9 (56.3%) were newly diagnosed. Males constituted the majority, n = 9 (56.3%). Half of the children were under 5 years of age and age ranged from 1 month to 10 years (IQR 3-9, mean 6.3 years). Hypertension was reported in 3 (18.8%) of the newly diagnosed patients who all turned out to have steroid sensitive nephrotic syndrome and anti-hypertensives were stopped within a month of starting steroids. Both children with congenital nephrotic syndrome died on admission from ESKD and severe community acquired pneumonia in one, while the other had aspiration pneumonia. Those with indications for albumin received 20% albumin during the initial days of admission. All newly diagnosed patients screened negative for possible secondary causes of nephrotic syndrome such as HIV, hepatitis B and C. Prednisolone was given to all newly diagnosed patients except the 2 who had congenital nephrotic syndrome. Eleven children had steroid sensitive nephrotic syndrome and 3 with steroid resistant nephrotic syndrome. Children with steroid resistant nephrotic syndrome and frequently relapsing nephrotic syndrome did not have access to second line immunosuppressive drugs. These drugs are not stocked at the hospital and are very expensive in private pharmacies. Kidney biopsy was also not available for those with indications for biopsy. Four patients with nephrotic syndrome demised as shown in Table 2.
Children with nephrotic syndrome who died during admission.
Chronic kidney disease
Patients admitted with CKD presented late with almost all being admitted with stage 5 CKD (eGFR < 15) and many complications including severe anaemia (n = 8, 72.7%), fluid overload (n = 7, 63.6%) and uraemia (n = 3, 27.3%) (Table 3). Chronic peritoneal dialysis became unavailable during the course of the study period for both adult and paediatric patients due to unavailability of dianeal solutions which are usually supplied by the hospital pharmacy. Non availability of consumables for either peritoneal dialysis or haemodialysis and medications needed for medical management of CKD (erythropoietin, sodium bicarbonate, calcium carbonate, activated vitamin D) made management of these patients extremely difficult contributing to a case fatality rate of 72.7% (8 out of 11 patients). Only 3 children with ESKD received dialysis, 1 child initially received peritoneal dialysis but developed adhesions and was switched to HD, and 2 received HD as initial mode of dialysis. All these were children above 10 years of age who could use adult dialysers and haemodialysis lines. Main challenges encountered were septic exit site and limited dialysis time due to limited resources. However these 3 children were still alive and receiving dialysis at the time of submission of this manuscript.
Characteristics of children admitted with CKD.

Child initially started on PD but later switched to HD due to PD failure.
Children still alive at the end of the study period.
AKI
AKI was diagnosed in 16 children with an age range of 1 week to 12 years (mean 3.8 years) (Table 4). Of these children 8 required dialysis, however only 3 could be offered dialysis due to limited resources (HD and PD catheters, fluids, intensive care unit (ICU) facilities for the critically ill) and early death due to late presentation. The mode of dialysis used was peritoneal dialysis. Improvised PD using a paediatric central venous catheter in 1 and adult haemodialysis catheters in the other 2 were used. Fortified ringer lactate was used as dialysis fluid. Poor drains (n = 2) and leakage (n = 1) at the exit site were the complications encountered, with 1 case of staphylococcal peritonitis being reported. This was managed successfully. All patients who received PD had full recovery of their renal function and survived. The proportion of patients admitted with AKI who died was 31.3% (n = 5).
Demographics causes of AKI and indications for dialysis in the children studied.

Rhabdomyolysis, Diabetic keto acidosis, Nephrotoxic drugs.
Most children had more than 1 indication for initiation of dialysis.
There was no capacity to quantify acidosis.
Proportion of children who required dialysis and still alive at discharge after admission.
Several challenges were encountered during the study period as outlined in Table 5 below.
Challenges in managing children with kidney disease.

Discussion
Kidney disease was diagnosed in approximately 1 in every 50 children admitted at Parirenyatwa Hospital between 1 January and 31 August 2022. Majority of these children were under 5 years of age. The commonest diagnoses in the unit were AKI, nephrotic syndrome, hypertension and ESKD. A high case fatality rate of almost 1 in 3 children with kidney disease was reported.
We documented an incidence of 2.2% (22 renal cases per 1000 children seen) for kidney disease among paediatric hospital admissions over a period of 8 months. It was comparable with studies in India, 9 however lower incidence rate of 1.1% have been reported in South Nigeria 21 and high rate of 6.3% was documented in Nepal. 22 Burden of kidney disease differs among different countries due to differences in genetic predisposition, environmental factors, clinical and laboratory capacities to diagnose kidney diseases. Mean(SD) age of presentation in our study was 5.5 ± 3.5 years with a M:F ratio of 1.5:1 and most children were aged between 0 and 5 years as seen in other studies.9,23
As shown in other studies in Africa 6 and Bangladesh 23 the most common kidney diseases requiring admission in the unit were AKI, ESKD and nephrotic syndrome. Unlike in India, 24 another developing economy, where post infectious glomerulonephritis is still constituting a majority of admissions, our unit only encountered 5 children (10%) with this condition. This could be because our study did not cover a full year thus taking into account the seasonal variability of the condition.25,26 Only 1 child was admitted with a urinary tract infection (UTI) whereas this is one of the most common renal diagnosis in several studies.8,9,24,27 Prevalence studies have shown that UTI may often be missed on history and physical examination 28 with >50% of febrile UTIs being misdiagnosed in children under 3 years. 29 There is need to conduct further research to identify the reason for the low diagnosis of urinary tract infections in our centre.
Nephrotic syndrome usually presents in the first decade of life. In our study it presented at a mean age of 6.3 years which is similar to other studies. 30 Our results support that prognosis of congenital nephrotic syndrome is poor without early aggressive proteinuria control, dialysis and subsequent transplantation, with most children dying in the first year of life. 31 Steroid resistant nephrotic syndrome has a poor prognosis with approximately 20% of children with initial steroid-resistant nephrotic syndrome developing CKD in childhood. 32 Persistent proteinuria increases the risk of progression to ESKD in children with nephrotic syndrome 33 hence the need to provide them with second line immunosuppression drugs.
In the current study AKI was mainly due to sepsis which is in accordance with other studies in sub-Sahara Africa.2,34,35 AKI in sub-Sahara Africa tends to be severe with up to 66% of children requiring dialysis at presentation. 34 It has been well documented that access to Kidney Replacement Therapy (KRT) in sub-Sahara Africa is limited. 34 At our centre only 37.5% of children requiring dialysis accessed it. Major barriers to access to KRT reported are out-of-pocket costs, erratic hospital resources and late presentation.2,34 Our reported case fatality rate of more than 31.2% is comparable to that reported in sub-Sahara Africa. 2 This high case fatality rate in children presenting with AKI could be explained by many factors such as: severity of disease at presentation, limited resources for dialysis and critical care facilities.
An overall mortality rate of 32% reported in our study is higher than <1.0%, 3.4% and 17.7% reported in Libya, 36 India 9 and Nigeria 37 respectively. Highest mortality was among children with ESKD. Almost every child with CKD presented with stage 5 disease. This could be because of late presentation and/or late referral from peripheral health centres due to non-recognition or misdiagnosis. Almost all patients with CKD presented late with stage 5 disease requiring dialysis which could only be offered in 3 children out of 11. Half of the children with AKI did not require dialysis and survived. Of the 8 who required dialysis only 3 managed to receive it and those are the children who survived. This highlights the need for dialysis in management of these cases.
Recommendations to improve care of children with kidney disease in our centre would include:
Increasing awareness of kidney disease to caregivers and health care providers in order to reduce late presentation and referrals.
Improving diagnosis of conditions and complications by equipping the laboratory as well as providing kidney biopsies where needed.
Ensuring adequate drugs are available to manage AKI or CKD complications as well as treatment of nephrotic syndrome.
Providing dialysis to those who require this life saving treatment.
Limitations
The retrospective nature of this study is a limitation. However, data in the unit is carefully entered and stored, therefore we are confident that the data was adequate for analysis. Although the small number of participants in our study may limit power to detect true differences, it however will inform future studies and guide immediate reforms in resource allocation and awareness programmes.
Conclusion
Childhood kidney disease contributes significantly to hospitalisations at our institution, with AKI, nephrotic syndrome, hypertension and CKD being the leading kidney disorders. Case fatality rate was high, being highest among children with ESKD. Of the 4 children with nephrotic syndrome who died 2 had ESKD secondary to the condition. Provision of second line immunosuppression drugs for children with frequently relapsing or steroid resistant nephrotic syndrome is required. Children with CKD present late with majority presenting with ESKD. Kidney replacement therapy is not available for most children who need it. The study also highlighted the need for essential drugs required in the management of children with CKD. Further studies are needed to determine the reason for late presentation among children with ESKD as well as the low number of children diagnosed with UTIs.