
Abstract
Celiac disease (CD) is a chronic autoimmune condition with intestinal and extra-intestinal features. Extra intestinal features including hematological, neurological, and endocrine symptoms are seen more frequently in elder children. A 4 years 7 months old male child presented in clinic with history of abdominal pain and diarrhea on and off for 1 year. On examination, he was hemodynamically stable, pale, and malnourished with distended abdomen. He was investigated for CD, Anti TTG IgA <0.1 (positive >10), Anti TTG IgG 13 (positive >10). To confirm celiac disease, Esophagogastroduodenoscopy (EGD) was done which was consistent with diagnosis of Celiac disease (MARSH Type 3a). Gluten free diet was advised. Later, after 12 days he again presented with jaundice, fever, anorexia, and dark colored urine and irritability. He was admitted for fulminant hepatic failure, his workup revealed direct hyperbilirubenemia, ANA +ve, and hyper IgG. Liver biopsy confirmed autoimmune hepatitis. Further workup for anemia showed reticulocyte count 7.1, LDH 423, direct and indirect coombs test was positive confirming autoimmune hemolytic anemia. Child responded well to Azathioprine and prednisolone with clinical improvement. We report a rare presentation of celiac disease with polyautoimmunity in a young child. Case reports of autoimmune hepatitis with CD patients have been reported in adult patients. Association of celiac disease with autoimmune hemolytic anemia and autoimmune hepatitis is a distinct and rare condition.
Introduction
Celiac disease (CD) is a chronic autoimmune condition with intestinal and extra-intestinal features. 1 Genetically predisposed patients are prone to gluten mediated enteropathy presenting as chronic diarrhea and malabsorptive symptoms. 2 Extra intestinal features including hematological, neurological, and endocrine symptoms are seen more frequently in elder children. 3 It is estimated that 1% of the population suffers from celiac disease worldwide. 4 The true incidence of celiac disease in Pakistan is not known but the disease is increasingly being reported in both children and adults.
Diagnosis of CD is widely made using ESPGHAN (European Society of Pediatric gastroenterology and Hepatology Association Network) criterion. It states that if tissue transglutaminase (TTG) levels IgA levels are more than 10 times high, duodenal biopsy is not needed. Those with positive TTG-IgA but titers <10 times upper limit of normal should undergo duodenal biopsy to confirm the diagnosis. 5 CD is associated with other autoimmune conditions like type 1 Diabetes mellitus, autoimmune thyroid disease, Addison diseases, and autoimmune hepatitis.6,7 Likely mechanism is that CD associated HLA DQ2/DQ8 loci are shared by other autoimmune diseases. 8 Females and adolescents are more frequently affected with autoimmune associations. 9
We report a 4 year 7 months old boy with recently diagnosed celiac disease, presenting with autoimmune hemolytic anemia (AIHA) and autoimmune hepatitis (AIH) presenting as fulminant disease.
Case summary
A 4 years 7 months old boy presented in clinic with history of abdominal pain and diarrhea on and off for 1 year. There was also history of failure to thrive and pallor. He received treatment from many local doctor but symptoms did not improve. He also complained of body aches and distended abdomen for last 2 months. He was born full term with no postnatal issue. He was breastfed for first 6 months only followed by formula. Weaning was started at 6 months. He is partially vaccinated and developmentally normal. He has 2 other siblings who are healthy. His parents had a non-consanguineous marriage and there was no history of tuberculosis, malabsorption, or celiac disease in family.
On examination, he was hemodynamically stable, pale, and malnourished with distended abdomen. Height was 91 cm and weight was 12 kg (both less than fifth centile). There was no visceromegaly. Fluid thrill and shifting dullness were negative. Rest of systematic examination was also unremarkable.
Initial labs showed hemoglobin (Hb) 8.8 g/dl, white cell count (WBC) 9940/ul, platelets 551 000/ul, MCV 53.9, MCH 13.6, Ferritin 20.1, ESR 34, alanine aminotransferase (ALT) was 18 U/L. Electrolyte, renal, liver function test, stool examination, and culture were normal. He was investigated for CD, Anti TTG IgA <0.1 (positive >10), Anti TTG Ig G 13 (positive >10) and was also positive for deaminated gliadin peptide (DGP) IgA. To confirm the diagnosis esophagogastroduodenoscopy (EGD) was done which was consistent with diagnosis of Celiac disease (MARSH Type 3a) showing distorted villous architecture, increased intraepithelial lymphocytes (Figure 1a). He was advised to follow a gluten free diet along with iron supplements. HLA testing was not done due to non-affordability of patient.

(a) Duodenal biopsy consistent with Marsh 3a—showing partial villous atrophy, intra epithelial lymphocytes, lamina propria inflammatory infiltrate. (b) Liver biopsy showing giant cell formation, interface hepatitis, and inflammatory infiltrate.
Later, after 2 weeks he presented with jaundice, fever, anorexia, dark colored urine, and irritability. He was deeply jaundice and had marked pallor on examination, his abdomen was soft with mild hepatomegaly but no splenomegaly. He was admitted for fulminant hepatic failure and investigations for anemia. Initial investigation showed hemoglobin 7.2 g/dl, WBC 10 260, platelet 186 000, total bilirubin 7.76 mg/dl, direct bilirubin 5.40 mg/dl, (ALT) 236, aspartate transaminase AST 439, gamma GT (GGT) 226, alkaline phosphatase ALP 387, serum ammonia 141, PT 12.50, INR 1.68 (0.8-1.3) APTT 45 seconds (24.8-36.2). Viral serology for hepatitis A and E were negative. Workup for Wilson disease was normal including serum ceruloplasmin 20.2 mg/dl (15-30 mg/dl), 24 hours urinary copper excretion was 16 ug/day (normal <60 ug/day), KF rings were not seen. Serial liver function tests are shown in Table 1. Further workup for anemia showed reticulocyte count 7.1, LDH 423, direct and indirect coombs test was positive suggestive of autoimmune hemolytic anemia for which steroids were started. Ultrasound abdomen showed mild hepatomegaly.
Liver function test.
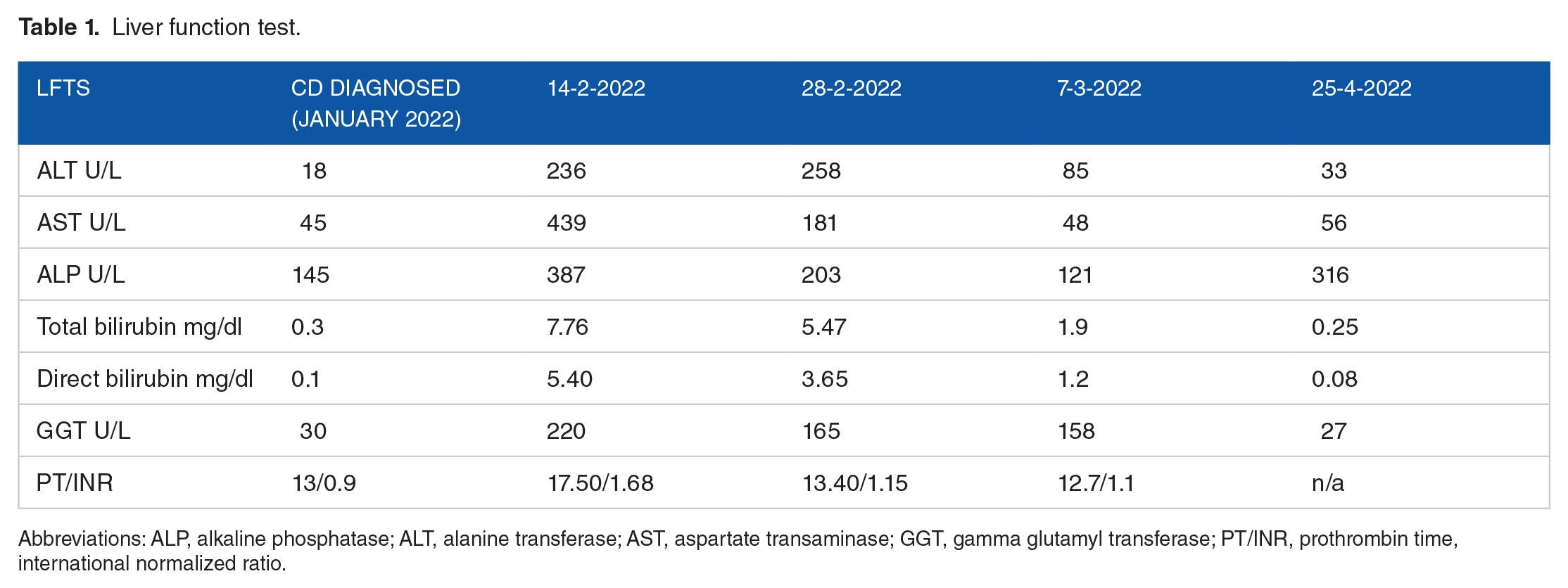
Abbreviations: ALP, alkaline phosphatase; ALT, alanine transferase; AST, aspartate transaminase; GGT, gamma glutamyl transferase; PT/INR, prothrombin time, international normalized ratio.
Autoimmune liver profile showed ANA+ and was negative for AMA, ASMA, GPC, and LKM. However, patient had hyper immunoglobulin Ig G was 44.1 g/l (Normal for this age 5.04-14.65). Liver biopsy showed moderate portal inflammation with foci of interface hepatitis, parenchymal cholestasis, and giant cell changes along with fibrous portal expansion with short fibrous septae, all favoring autoimmune hepatitis type I (Figure 1b).
Prednisolone (2 mg/kg/day) and Azathioprine (2 mg/kg/day) were started. Steroids were gradually tapered over 4 weeks. Two months follow-up showed normalization of LFTs. His hemoglobin improved from 7.2 to 8.8 g/dl on follow-up. Gluten free diet is re-emphasized on each visit.
Pediatric hematologist, gastroenterologist, and dietician were involved and final diagnosis of celiac disease with autoimmune hemolytic anemia and giant cell autoimmune hepatitis was made. Written informed consent was taken from the parents.
Discussion
We report a rare presentation of celiac disease with polyautoimmunity in a young child. To the best of our knowledge this is the youngest age reported with multiple autoimmune associations of celiac disease.
Our patient had low titers of TTG IgA and IgA DGP necessitating duodenal biopsy which confirmed the diagnosis of CD. It is recommended that symptomatic children with high suspicion of CD must be offered biopsy regardless of antibodies titers. 10
Liver diseases associated with celiac disease include raised transaminases called celiac hepatitis, and autoimmune associations include autoimmune hepatitis (AIH), Primary biliary cholangitis, and Primary biliary cirrhosis. Patients with celiac hepatitis improve on institution of gluten free diet (GFD). 11 While patients with autoimmune hepatitis need long term immunosuppression and might need liver transplant. 12 Case reports of autoimmune hepatitis with CD patients have been reported mainly in adult patients at 50 and 60 year of age. 13 Two studies in adults report AIH patients have high prevalence of CD, from 4% to 6.4%. 14 In pediatric population the prevalence of CD in AIH is reported to be higher than adults ranging from 11.5% to 46%. 15 It is postulated that CD and AIH share same genetic loci for Human Leukocyte Antigen class II, explaining their coexistence. 16 It is recommended to test for AIH in CD patients with abnormal liver function tests. 17 Patients with AIH and CD have been reported to achieve treatment-free sustained remission in a significantly higher proportion of cases, when compared with patients with AIH without coeliac disease, suggesting a possible long-term adjuvant effect of the gluten-free diet.
Our patient presented acutely with fulminant liver disease, his antibodies were negative but had ANA positive and hypergammaglobulinemia, consistent with type 1 autoimmune hepatitis. 18 Histological findings on liver biopsy were consistent with autoimmune hepatitis. Up to 20% of patients might not have any autoantibodies but have disease pattern and histology findings consistent with disease. 19 Autoimmune hepatitis with negative antibodies presenting as fulminant hepatic failure has been reported in literature in an 8 year old girl. 20 Autoimmune hepatitis can be associated with latent celiac disease so all patients should be screened. 21 He was treated as per ESPGHAN guidelines on autoimmune hepatitis with steroid and azathioprine and achieved remission in 8 weeks. 22
Autoimmune hemolytic anemia has been reported in association with celiac disease. 23 However, the association of AIHA with autoimmune hepatitis is a distinct condition rarely reported in children. 24 Literature supports the fact that it needs aggressive therapy with immunosuppression with steroids and Azathioprine. 25 Literature shows that patient respond well to treatment with resolution of symptoms as seen in our case. Case reports of AIHA with CD are reported mainly in adult females. 26 Table 2 shows case reports of CD with AIH and AIHA reported in pediatric age group.
Association of celiac disease with AIH, AIHA reported in children.

The study highlights that all children with CD with abnormal liver function tests should be screened for AIH.
Conclusion
This is a rare presentation of celiac disease with autoimmune hemolytic anemia and autoimmune hepatitis, necessitating prompt therapy with immunosuppressant showing encouraging results.