
Abstract
Background:
Splenic cysts are one of the relatively rare conditions in pediatric surgery practice. Primary non-parasitic splenic cysts are even more scarce.
Case presentation:
A 13-years-old female patient presented with chronic left hypochondrial pain of 2 months duration. Abdominal ultrasonography and computed tomography revealed huge 18 cm × 14 cm × 10 cm splenic cyst. Deroofing of the cyst was done which was complicated by secondary infection. Subsequently, the patient was re-operated on and partial splenectomy done with good outcome at 6 months follow up.
Conclusion:
Partial splenectomy is the best management strategy for huge non-parasitic splenic cysts in children. There is also less recurrence rate of splenic cysts with preservation of splenic functions.
Introduction
Splenic cysts are generally rare and are usually discovered accidentally during imaging studies.1,2 The first splenic cyst described in literature was discovered at autopsy by Andral in 1829. 3
Splenic cysts can be classified according to Martin’s classification into; Martin splenic cyst class 1 that mean a true (primary) cyst with existing lining epithelium,4,5 and Martin splenic cyst class 2 that indicates absence of lining epithelium and is always considered to be secondary to direct splenic/or abdominal wall trauma, splenic infarction or abscess.6-8
In 2007, Mirilas and coworkers, 9 critically reviewed literature for a valid classification of splenic cysts. They classified nonparasitic splenic cysts into primary and secondary cysts (Table 1). However, according to the International Society for the Study of Vascular Anomalies (ISSVA), splenic hemangioma, and lymphangioma are considered congenital malformations and not neoplastic lesions.10,11
Classification of non-parasitic splenic cysts. 7

Table reproduced with permission.
Permission license attached as Supplemental File.
For a long period of time; surgical management with removal of the spleen was the treatment of choice for splenic cysts and the first splenectomy for a cyst was done on 1867 by Splenotomy. 12
Nowadays, the conservative school is the most agreed for management of small and asymptomatic cysts. Total splenectomy conducts to infectious complications, that is why conservative management is preferred. Deroofing and partial splenectomy have their particular indications while total splenectomy is rarely needed.
We here in report the first case of primary huge mesothelial cyst in a child from Saudi Arabia and discus her management pitfalls.
Case Description
A 13 years old Saudi female presented to the pediatric emergency department with chronic left upper quadrant pain for 2 months. The patient was in her usual status of health until 2 months prior to presentation. The pain was localized in the left upper quadrant with no radiations, throbbing in nature, intermittent in course, aggravated by movement and relived by rest. Inspiratory movements also aggravated the pain.
There was no associated history of fever, yellowish discoloration of the skin & mucus membranes, weight loss, change in appetite, headache, blurred vision, chest pain, hemoptysis, vomiting, bowel habits changes, urinary symptoms, or any other symptom suggestive of any body system affection. There was no history of abdominal trauma.
At the meantime, there were neither history of contact with animals nor travel to endemic areas of infections or infestations. She had none significant family and surgical histories.
On examination, the patient looked clinically well and vitally stable with average anthropometric measurements. Her abdomen was soft, but with a left upper quadrant mass detected by deep palpation. The mass was immobile, hard, 18 cm × 14 cm × 10 cm in size, dull on percussion with no auscultatory findings. It was tender on palpation with pain score of 8 over 10.
Accordingly, the patient was admitted for workup. Basic laboratory testing including; complete blood picture, liver and kidney functions tests, C-reactive-protein, erythrocyte sedimentation rate and urine, and stool analyses were normal.
Her abdominal ultrasonography (US) showed huge splenic cyst which was hyper echoic with posterior enhancement. The study was completed by a computed tomography (CT) of the abdomen and pelvis which revealed large septate intra-splenic cyst with fluid collection measuring 18 cm × 14 cm × 10 cm, located at the upper pole of the spleen away from the hilum (Figure 1). Hydatid disease serology was performed to exclude parasitic splenic cyst (PSC) which came out to be negative.

Preoperative abdominal CT scan picture of the splenic cyst.
The diagnosis of non-parasitic splenic cyst (NPSC) was retained and the patient underwent laparoscopic unroofing dome cystectomy.
On the third day post operation; the patient developed high spikes of fever and follow up US showed recollection with turbid fluid inside with an estimated size of 10.1 cm × 8.3 cm × 7.6 cm suggesting recollection with secondary infection. CT abdomen and pelvis confirmed the US findings (Figure 2).

Postoperative abdominal CT scan showing recurrence of the splenic cyst.
Broad spectrum antibiotics were immediately started, and re-exploration laparoscopy was done. On laparoscopy, adhesions were found between the remnants of the cyst, the diaphragm and the great stomach curvature.
The surgeon decided to convert to open laparotomy due to the extensive adhesions to the diaphragm. Adhesions were cut, vessels were divided, and an upper pole partial splenectomy resecting the whole upper pole of the spleen including the entire cyst was done with hemostasis sutures sutured at the cut edge as shown in Figure 3. This was followed by smooth uneventful postoperative course.

Post recurrence surgical splenic picture with resection of the cyst and upper pole of the spleen.
Histopathological assessment of the removed part of the spleen with the cyst revealed primary non-parasitic splenic mesothelial in origin (arrows in Figure 4(A)), there was no squamous metaplasia, there was no evidence of clear septation or trabeculations (Figure 4(A)). Immunostaining with PanKeratin and Calratinin were positive supporting the primary mesothelial nature of the cyst (stained brown in Figure 4(B)). CEA staining was negative.

Histopathological picture of the resected cyst with mesothelial lining. (A) Hematoxylin and eosin. (B) PanKeratin and Calretinin immunostains.
Other differential diagnosis should be always kept in mind, including lymphangioma as well as hydatid cysts and pseudocysts.
The patient was discharged after completing the antibiotics course and is currently under regular follow up. Her 1, 3, 6-, and 12-months post-surgery follow up was uneventful with normal abdominal US with no recurrence.
Discussion
Splenic cysts are rare entity that is commonly coincidentally discovered in imaging studies specially during investigations for different gastrointestinal complaints, following abdominal trauma, during laparotomies or at autopsies.1,2 There are conflicting data about their incidence; in one report it was mentioned to be around 0.5% to 2.0% of the whole population 13 while in another report of 42 327 autopsies, splenic cysts were found in only 0.07% of the series.14,15 Up to our knowledge, there are only around 1000 reported cases of primary (1ry) splenic in literature.
As mentioned before; there are 2 main categories of splenic cysts according to presence or absence of a lining epithelium; true/primary splenic cysts (PSC) or secondary splenic cysts (SSC) respectively. 16 PSC can be further subdivided into; parasitic (PPSC) and non-parasitic (NPPSC). 17 In Europe and North America, it is common to see the NPPSC, while in Africa and Central America it is commonly to see the parasitic ones. 18 The NPPSC can be either congenital or neoplastic. The congenital cysts can be either epidermoid, endodermoid or dermoid cysts. 19
PSC accounts for 20% to 25% of all splenic cysts. 20 Among PSC, epidermoid cysts constitute around 25%. 21 The PSC were found to be most common in children, adolescents, and young adults. 1 On the other hand, females were found to be more affected by splenic cyst in general and congenital type in particular.22,23
Approximately 75% to 80% of total splenic cysts are SSC which can be either neoplastic (endothelial in origin like: hemangioma, lymphangioma) or even pseudocysts without any lining epithelium, which is can be a result of direct splenic/abdominal blunt trauma or splenic infarction, infection or abscess. 24
The post traumatic pseudocysts usually develop due to hematoma that failed to be collected under the splenic capsule or inside its parenchyma, and rarely can be as a result of splenic infection or ischemic lesion.6-8 A total of 30% to 60% of them are asymptomatic. 25
Like in our patient, splenic cysts usually symptomatize when there is increase in size more than 8 cm 26 due to compression of nearby organs like stomach and kidney. 27 Our patient was symptomatic due to the huge cyst (18 cm × 14 cm × 10 cm) she had.
She presented with abdominal pain which agreed with other reports which stated that abdominal pain is the most important complaint in symptomatic cases. 28 Hypertension can occur in some patients due to renal artery compression.29,30
Most patients present at pubertal age as the cyst growth was found to be affected by hormonal changes during puberty, especially around the age of 11 to 12 years old, 31 which coincides with the presentation of our patient.
When it comes to diagnosis, ultrasound as initial step followed by computed tomography are the most used modalities, 32 and histopathology is the definitive diagnostic modality.25,33 We used the same strategy in our patient.
The management of NPSC remains controversial. Surgical resection is indicated for symptomatic or complicated forms, but no guidelines are available for asymptomatic NPSC. A recent report released in 2017 by Delforge and his colleague, suggested a practical logical management algorithm for NPPSC, Table 2 and Figure 5. 28 Different surgical techniques are used for symptomatic cases including unroofing marsupialization as we did initially in our patient or partial splenectomy as we did later after complications. 33 Previously, total splenectomy was the main management modality but after discovery of the crucial immunological functions of the spleen in opsonization of capsulated organism. This approach is only reserved to very limited indications to avoid overwhelming post-splenectomy which can be infections and fulminant. 34
Pediatric literature on the surgical outcome of non-parasitic splenic cysts. 25
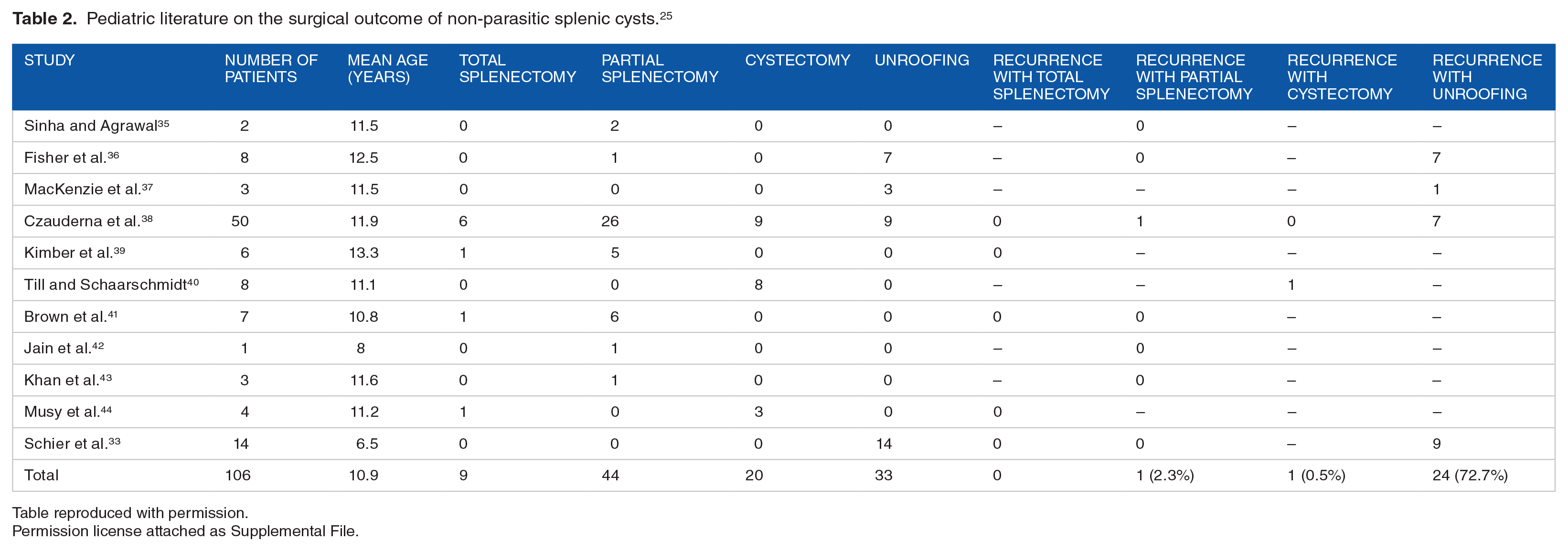
Table reproduced with permission.
Permission license attached as Supplemental File.

Suggested non-parasitic splenic cysts management protocol. 25
The patient’s clinical course was complicated by infection which necessitated a second surgery with partial splenectomy. Most recent literature reported high recurrence rate and post-operative infection and/or bleeding.33,45
We admit that with this huge size of the mass, the choice of the deroofing was not appropriate and that partial splenectomy should have been the initial treatment of choice. Partial splenectomy preserves good tissue of the spleen with low recurrence rate. 46
Conclusion
Partial splenectomy might be an excellent line of management of large splenic cysts to avoid recurrence and postoperative complications.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ Contributions
IK, KM, MK, UK, MK, RA: Diagnosed the patient, performed the surgical procedure, set the idea of the study and designed the study. HA, NK: collected data, reviewed literature, drafted the manuscript, critically analyzed the data. All authors reviewed and approved the manuscript for final publication
Availability of Data and Materials
All data and materials related to the study are included in the current manuscript.
Ethical Approval and Consent to Participate
The study was approved by the research and ethical committee of the participating hospitals. All parents of enrolled children signed written informed consents for participation of their children in the current study.
Consent for Publication
All parents of enrolled children signed written informed consents for publication the current study.